Scott J, Burke FJ, Watts DC. A review of dental injuries and the use of mouthguards in contact team sports. Br Dent J. 1994; 176:310-314
Foster M, Readman P. Sports dentistry – what's it all about?. Dent Update. 2009; 36:135-144
Bastone EB, Freer TJ, McNamara JR. Epidemiology of dental trauma: a review of the literature. Aust Dent J. 2000; 45:2-9
Nguyen Q, Bezemer P, Habets L, Prahl-Andersen B. A systematic review of the relationship between overjet size and traumatic dental injuries. Eur J Orthod. 1999; 21:503-515
Francisco SS, de Souza Filho FJ, Pinheiro ET, Murrer RD, de Jesus Soares A. Prevalence of traumatic dental injuries and associated factors among Brazilian schoolchildren. Oral Health Prev Dent. 2013; 11:31-38
Schatz JP, Hakeberg M, Ostini E, Kiliaridis S. Prevalence of traumatic injuries to permanent dentition and its association with overjet in a Swiss child population. Dent Traumatol. 2013; 29:110-114
O'Malley M, Evans DS, Hewson A, Owens J. Mouthguard use and dental injury in sport: a questionnaire study of national school children in the west of Ireland. J Ir Dent Assoc. 2012; 58:205-211
Newsome PR, Tran DC, Cooke MS. The role of the mouthguard in the prevention of sports-related dental injuries: a review. Int J Paediatr Dent. 2001; 11:396-404
McClelland C, Kinirons M, Geary L. A preliminary study of patient comfort associated with customised mouthguards. Br J Sports Med. 1999; 33:186-189
Fayle S. Mouthguards for sporting activities – do they offer protection?.: Royal College of Surgeons; 2014
Salam S, Caldwell S. Mouthguards and orthodontic patients. J Orthod. 2008; 35:270-275
Parker K, Marlow B, Patel N, Gill DS. A review of mouthguards: effectiveness, types, characteristics and indications for use. Br Dent J. 2017; 222:629-633
Tiryaki M, Saygi G, Ozel Yildiz S, Yildirim Z, Erdemir U, Yucel T. Prevalence of dental injuries and awareness regarding mouthguards among basketball players and coaches. J Sports Med Phys Fitness. 2017; 57:1541-1547
Bergman L, Milardovic Ortolan S, Zarkovic D, Viskic J, Jokic D, Mehulic K. Prevalence of dental trauma and use of mouthguards in professional handball players. Dent Traumatol. 2017; 33:199-204
Rodd HD, Chesham DJ. Sports-related oral injury and mouthguard use among Sheffield school children. Community Dent Health. 1997; 14:25-30
Gould TE, Piland SG, Caswell SV, Ranalli D, Mills S, Ferrara MS National Athletic Trainers' Association Position Statement: Preventing and Managing Sport Related Dental and Oral Injuries. J Athl Train. 2016; 51:821-839
Vucic S, Drost RW, Ongkosuwito EM, Wolvius EB. Dentofacial trauma and players' attitude towards mouthguard use in field hockey: a systematic review and meta-analysis. Br J Sports Med. 2016; 50:298-304
Dhillon BS, Sood N, Sood N, Sah N, Arora D, Mahendra A. Guarding the precious smile: incidence and prevention of injury in sports: a review. J Int Oral Health. 2014; 6:104-107
Pacheco G, Clemente MP, Vasconcelos M, Ferreira AP. The orthodontic sports protection appliance. J Clin Orthod. 2010; 44:41-44
Hickey JC, Morris AL, Carlson LD, Seward TE. The relation of mouth protectors to cranial pressure and deformation. J Am Dent Assoc. 1967; 74:735-740
Labella CR, Smith BW, Sigurdsson A. Effect of mouthguards on dental injuries and concussions in college basketball. Med Sci Sports Exerc. 2002; 34:41-44
Maeda Y, Kumamoto D, Yagi K, Ikebe K. Effectiveness and fabrication of mouthguards. Dent Traumatol. 2009; 25:556-564
Cohenca N, Roges RA, Roges R. The incidence and severity of dental trauma in intercollegiate athletes. J Am Dent Assoc. 2007; 138:1121-1126
Finch C, Braham R, McIntosh A, McCrory P, Wolfe R. Should football players wear custom fitted mouthguards? Results from a group randomised controlled trial. Inj Prev. 2005; 11:242-246
Knapik JJ, Marshall SW, Lee RB, Darakjy SS, Jones SB, Mitchener TA Mouthguards in sport activities: history, physical properties and injury prevention effectiveness. Sports Med. 2007; 37:117-144
Azeredo FN, Maia DW, Pomarico L, Antunes LA, Antunes LA. Perceptions regarding the occurrence and prevention of orofacial injuries during general anesthesia. J Oral Sci. 2015; 57:263-267
, 3rd edn. St Leonards, Sydney: ADA; 2016
Chapman PJ. The bimaxillary mouthguard: a preliminary report of use in contact sports. Aust Dent J. 1986; 31:200-206
Milward PJ, Jagger RG. A bimaxillary sports mouthguard: a modified technique. J Prosthodont. 1997; 6:292-295
Jagger RG, Milward PJ. The bimaxillary mouthguard. Br Dent J. 1995; 178:31-32
Patrick D, Van Noort R, Found M. Scale of protection and the various types of sports mouthguard. Br J Sports Med. 2005; 39:278-281
Fakhruddin KS, Lawrence HP, Kenny DJ, Locker D. Use of mouthguards among 12-to 14-year-old Ontario schoolchildren. J Can Dent Assoc. 2007; 73
Mizuhashi F, Koide K. Formation of vacuum-formed and pressure-formed mouthguards. Dent Traumatol. 2017; 33:295-299
Guerard S, Barou JL, Petit J, Poisson P. Characterization of mouthguards: impact performance. Dent Traumatol. 2017; 33:281-287
Del Rossi G, Lisman P, Signorile J. Fabricating a better mouthguard. Part II: the effect of color on adaptation and fit. Dent Traumatol. 2008; 24:197-200
Verissimo C, Costa PV, Santos-Filho PC, Tantbirojn D, Versluis A, Soares CJ. Custom-fitted EVA mouthguards: what is the ideal thickness? A dynamic finite element impact study. Dent Traumatol. 2016; 32:95-102
Yonehata Y, Maeda Y, Machi H, Sakaguchi RL. The influence of working cast residual moisture and temperature on the fit of vacuum-forming athletic mouth guards. J Prosthet Dent. 2003; 89:23-27
Mizuhashi F, Koide K, Mizuhashi R. Influence of working model position on the formation of a pressure-formed mouthguard. Dent Traumatol. 2016; 32:469-473
Mizuhashi F, Koide K. Appropriate fabrication method for vacuum-formed mouthguards. Dent Traumatol. 2017; 33:110-113
Takahashi M, Koide K, Suzuki H, Iwasaki S. Optimal heating condition of ethylenevinyl acetate co-polymer mouthguard sheet in vacuum-pressure formation. Dent Traumatol. 2016; 32:311-315
Chaconas SJ, Caputo AA, Bakke NK. A comparison of athletic mouthguard materials. Am J Sports Med. 1985; 13:193-197
Kenyon BJ, Loos LG. Comparing comfort and wearability between Type III single-layered and double-layered EVA mouthguards. Gen Dent. 2005; 53:261-264
Bourdin M, Brunet-Patru I, Hager PE Influence of maxillary mouthguards on physiological parameters. Med Sci Sports Exerc. 2006; 38:1500-1504
Love RM, Carman N, Carmichael S, MacFadyen E. Sport-related dental injury claims to the New Zealand accidental rehabilitation and compensation insurance corporation 1993–96. N Z Dent J. 1998; 94:146-149
Maeda Y, Matsuda S, Tsugawa T, Maeda S. A modified method of mouthguard fabrication for orthodontic patients. Dent Traumatol. 2008; 24:475-478
Bussell MA, Barreto LS. The recommendation and provision of mouthguards: a survey of consultant orthodontists in the UK. J Orthod. 2014; 41:141-146
Croll TP, Castaldi CR. Custom sports mouthguard modified for orthodontic patients and children in the transitional dentition. Pediatr Dent. 2004; 26:417-420
It is recommended that all those participating in sports involving physical contact wear a sports mouthguard (MG) to prevent or reduce the severity of dental trauma. Fixed orthodontic appliances are potentially an additional risk factor for traumatic dental injuries during sports participation. Non-custom-made MGs may be ill-fitting, poorly retentive and ineffective in minimizing injury to the teeth and associated structures compared with custom-made MGs. The presence of fixed orthodontic appliances and prospective tooth movement, however, present a challenge in the provision of custom-made MGs for the orthodontic patient.
CPD/Clinical Relevance: Most orthodontic treatment is carried out in the age group of patients where there is a reported peak in the incidence of dental injury during sports activity. Oral health professionals need to be aware of the role MGs play in minimizing injury to the teeth and associated structures.
Article
Participants in contact sports have been shown to be more prone to orofacial injury with dental injury being most common.1,2-3 In addition, participants with an increased overjet may be at greater risk of dental trauma.4,5-6 Dental injuries can have a significant social, psychological and economic impact on patients and their parents.7 A sports mouthguard (MG) is a resilient appliance placed inside the mouth to prevent or minimize injury to the teeth and associated structures during participation in sporting activity. It works by absorbing some of the energy from a direct blow at the site of impact, and dissipating the remaining energy by cushioning and redistributing the force.8,9
MG wear is recommended for those participating in sports involving physical contact and/or moving objects – essentially any sporting activity where a blow to the jaws or teeth may occur.10,11 This includes all codes of football, rugby, cricket, lacrosse, hockey, ice hockey and boxing, in addition to martial arts and sporting activity where close physical contact can be expected, such as water polo, basketball and netball.11,12 Although wear is widely recommended in the UK, compulsory or mandatory MG wear occurs in only a few sporting activities, such as rugby in older age groups in addition to amateur and professional boxing.13,14-15 Their use appears to be limited in sports where wear is not mandatory and current evidence suggests that there is a lack of awareness among coaches, parents and participants regarding the risk of dental injury in sports and the role of MGs in its prevention.7,16,17,18,19,20-21
The proposed benefits of MG wear during participation in sporting activity include reduction of:
The risk of injury to the maxillary anterior teeth;
Damage to the posterior teeth of either jaw following traumatic closure of the mandible;
Soft tissue lacerations;
Tongue damage at impact;
Fracture of the body of the mandible and damage to the temporomandibular joint.12,22
In addition, MG wear may provide some protection against mild traumatic brain injury (concussion).23,24-25 The evidence for this, however, is weak.
Conclusive high level evidence that MGs reduce the risk and severity of orofacial injury is lacking. In part, this is due to the ethical issues surrounding individuals participating in randomized controlled trials (RCTs) of ‘protection’ vs ‘non-protection’ in potentially risky activity.25 Although the evidence base is not strong, a number of studies indicate that wearing a MG may reduce the risk of dental injury. One, conducted among American basketball players, showed that significantly fewer dental injuries occurred in the (custom-fitted) MG user group compared to those not wearing a MG (0.12% vs 0.67%).24 In another study, basketball players at an American University were five times more likely to report dental injury than American footballers at the same University.26 MG wear was mandatory for the American footballers whereas it wasn't for the basketballers. In a cluster RCT, a significantly lower rate of head and orofacial injuries was reported in those wearing a custom-fitted MG in Australian rules football compared to those wearing a non-custom-fitted MG.27 A meta-analysis has found that the overall risk of dental injuries was 1.6 to 1.9 times less when a MG was worn, compared to when a MG was not worn during athletic activity.28
MGs are generally fabricated for sporting activities, although they have been shown to be useful in other situations, such as dental protection during intubation for a general anaesthetic.29
The purpose of this article is to provide an overview of MG characteristics, outline the orthodontic considerations of MG wear and describe MG fabrication for a patient wearing fixed orthodontic appliances.
Characteristics of MGs
MG materials and types
The properties of an ideal MG material are shown in Table 1.30
Biocompatible
Ease of pre-fabrication manipulation
Resistance to damage from water absorption
Sufficient elastic modulus to reduce stress beneath material at point of impact
Sufficient rigidity to distribute forces over a large area of the dentition
Sufficient toughness to resist cutting by biting
Resistance to fracture under sudden impact
Able to withstand normal cleaning compounds
Resistance to low pH
Tasteless and odourless
Inexpensive
Common materials used in MG fabrication have included:
Polyvinylacetate-polyethylene or ethylene vinyl acetate (EVA) copolymer;
MGs may be single jaw or bimaxillary.13 Bimaxillary MGs may provide improved protection from lateral and frontal impact to the mandible by covering both arches.31,32-33 Their increased bulk, however, may affect speech and make them difficult to tolerate.13
Three MG types are generally available:
1. Stock MGs
Stock MGs are bought ‘over the counter’ and have no capability to adjust to an individual's dental morphological characteristics and are consequently worn without modification.2 They come in different sizes and are mostly made from polyurethane, or a co-polymer of vinyl acetate or ethylene. Although inexpensive, stock MGs are thought to be the least favourable as they fit poorly, are difficult to wear and offer minimum protection. Their poor fit may cause dislodgement during use with the consequent risk of airway obstruction (Figure 1).34
Figure 1. A stock MG. (This MG incorporates a ‘cut out channel’ for the patient's fixed orthodontic attachments.)
2. Mouth formed/‘boil and bite’ MGs
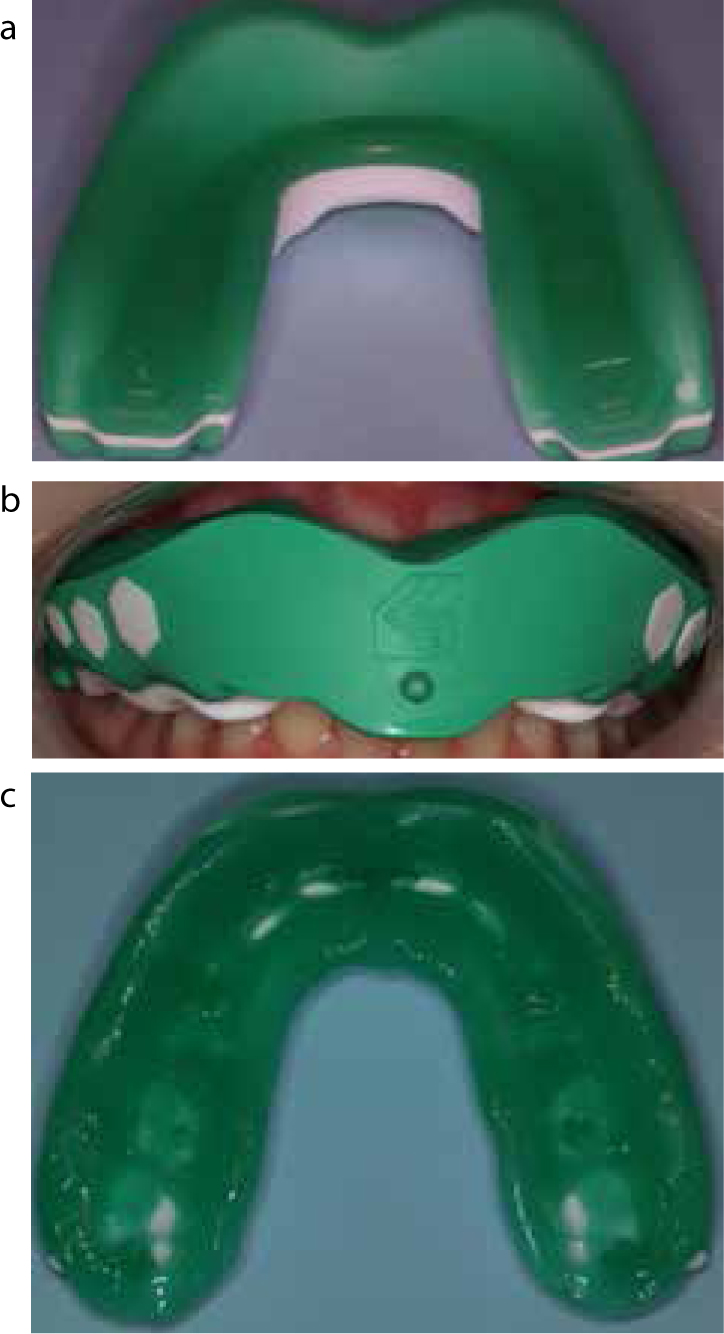
‘Boil and bite’ MGs are widely available at pharmacies and sport stores. They appear to be the most commonly used MG type.7,35 They are made of a thermoplastic material which is heated in hot water and the athlete moulds the MG to his/her mouth by biting, sucking and using finger pressure. Some require constant biting to hold them in place which can affect speech and breathing.12 Owing to their low temperature of formation, they continue to deform so that retention and occlusal thickness reduces. The protection offered, therefore, may be limited (Figures 2 and 3).2,34
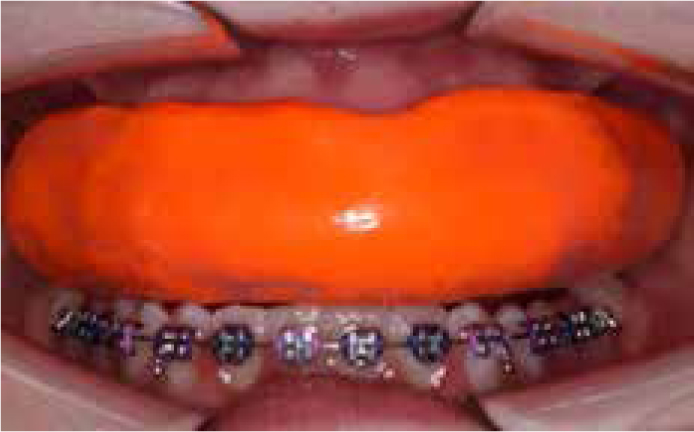
Figure 2. A ‘boil and bite’ MG.Figure 3.
(a) A ‘boil and bite’ MG prior to use in a 10-year-old patient with a 7.5 mm overjet. (b) The ‘boil and bite’ MG from (a) in the patient's mouth after heating the MG in hot water and moulding by the patient. (c) Occlusal view of the fitting surface of the ‘boil and bite’ MG from (a) subsequent to heating the MG in hot water and moulding by the patient.
3. Custom-made MGs
These are specially made from a cast of a dental impression of a jaw taken by an oral health professional and are generally more expensive than stock and ‘boil and bite’ MGs.7 They are considered to be more effective in preventing and reducing the severity of dental trauma, more retentive and offer a better fit compared with other MG types.13,21,25 In addition, patient acceptability appears to be greater.21
Fabrication
Ethylene vinyl acetate (EVA) has been the predominant material of choice for custom-made MG fabrication due to its availability, formability and ease of manipulation, though it may have limitations in terms of shock absorption capability and rigidity.28
Fabrication involves a thermoforming process which involves heating an EVA ‘blank’ in a pressure or vacuum-thermoforming machine above the cast (Figures 4, 5). When the ‘blank’ is soft enough, air pressure or a vacuum is applied which closely moulds the soft material to the cast.36
The thermoplastic material ‘thins’ during the fabrication process and this may influence the effectiveness of MGs, particularly when it occurs in the area where the external impact is generally exerted, usually the upper anterior region.24,28 Studies have shown that, during fabrication, thicknesses decreased from 25% to 50% for the custom-made MGs and 70–99% for mouth-formed/’boil and bite’ MGs. This suggests greater effectiveness with custom-made MGs.37 Thickness and impact performance, however, may not be sufficient criteria to characterize efficiency performance of MGs.38 Interestingly, incorporation of colour pigments into the thermoplastic material may provide superior adaptation and more firmly fitting MGs than clear material.39
Pre-fabrication EVA ‘blank’ (Figure 6) thicknesses of 3–6 mm have been recommended as a balance between sufficient energy absorption and minimal deformation, and wearer comfort and acceptance.25,28,40
Figure 6. A selection of EVA ‘blanks’ prior to MG fabrication.
Table 2 outlines the general design features of MGs.1,12,14,30,34 Careful attention to the thermoforming process may ensure superior fit and minimal thinning of the thermoplastic material. Recent in vitro evidence suggests that the ‘thoroughly dried’ working model should be positioned 15 mm posteriorly from the centre of the pressure former during pressure forming and the model should be inclined to where the labial surface of anterior teeth can make a ‘sharp angle’ to the sheet surface.41,42 During vacuum-forming, heating of the thermoplastic sheet to 120°C and a ‘sagging distance’ of 15 mm may provide the most suitable forming process.43,44
The approximate material thickness should be 2–3 mm on the labial aspect, 3 mm on the occlusal aspect and 2 mm on the palatal aspect
The labial flange should extend to within 2 mm of the vestibular reflection
The palatal flange should extend about 10 mm above the gingival margin
The edge of the labial flange should be rounded in cross-section
The edge of the palatal flange should be tapered in cross-section
All teeth to the distal of the maxillary second molars should be incorporated
In the mixed dentition, the MG should extend to the distal surface of the maxillary first molars
On closing the mouth, there should be even contact between the MG's occlusal surface and the lower teeth
The thermoforming process facilitates ‘lamination’. This is the fabrication of ‘multiple layered’ MGs since heated EVA sheets can be fused to each other firmly and allow better thickness control. Consequently, logos and different colour combinations can be incorporated.2 ‘Laminated’ MGs may also be more dimensionally stable than other custommade MG types.45
There appears to be little robust evidence to indicate which thermoforming process is more effective, although it is suggested that ‘pressure-formed laminated’ MGs may be superior.8,13,46 A recent in vitro study has shown that the vacuum-forming method maintained the MG thickness while the pressure-forming method obtained better fit.36 Further research, however, is required to establish whether this has clinical significance. Another study reported that patient acceptability for the double-layered, heat- and pressure-laminated MG was greater compared to the single-layered, vacuum-thermoformed EVA MG.36,47
Current research appears to indicate that fitted, custom-made mouthguards result in fewer problems, such as difficulty in breathing and speaking.13,25 In addition, MGs do not appear to impact on physiological measurements relevant to athletic performance.48
Orthodontic considerations
Most orthodontic treatment is carried out before or during adolescent years. It is during this time when there is a reported peak in the incidence of dental injury while participating in contact sports.49 Many patients undergoing orthodontic treatment do not wear MGs while participating in contact sports.50 Orthodontic patients wearing removable appliances are advised to remove their appliances and use MGs for contact sports.14
Fixed orthodontic appliances are an additional risk factor for traumatic injuries in the maxillofacial region during sports events.51 A potential orofacial injury may occur more easily because of increased tooth mobility and the presence of orthodontic appliances.8 This may result in additional damage to soft tissues, loosening of brackets and bending of archwires.2,12,52
Non-customized MGs (such as Orthoguard™), which incorporate a channel to accommodate fixed orthodontic appliances (such as orthodontic brackets, tubes, molar bands and archwires) and planned orthodontic movement of teeth have been described (Figures 1, 7–9).12,13-14 Although less expensive, they may be poorly retentive, offer less protection against dental injury and require more frequent replacement.
Figure 7. A stock orthodontic MG incorporating a hinge to keep the MG in place in the mouth (Masel Doubleguard Mouthguards, 1822 Aston Ave, Carlsbad, CA 92008-7306, USA).Figure 8. The stock orthodontic MG shown in Figure 7 in the patient's mouth.Figure 9. A ‘boil and bite’ MG (incorporating a ‘cut out channel’ for the patient's fixed orthodontic attachments).
Custom-made MGs (modified to facilitate the presence of fixed orthodontic appliances, prospective tooth movement and passive/active eruption of teeth) are considered, therefore, to offer superior protection from dental injury, greater fit and patient comfort.2,12,22,50,51-52
Fabrication of a MG for a patient wearing fixed appliances
Figures 10–13 outline the steps involved in the fabrication of a MG for a 13-year-old patient wearing fixed orthodontic appliances. This is a variation of previous descriptions of modified custom-made MGs fabricated by the vacuum-thermoforming technique.22,50,51 This simple method uses dental plaster for ‘blocking out’ on the cast and fabrication is via the pressure-forming technique.
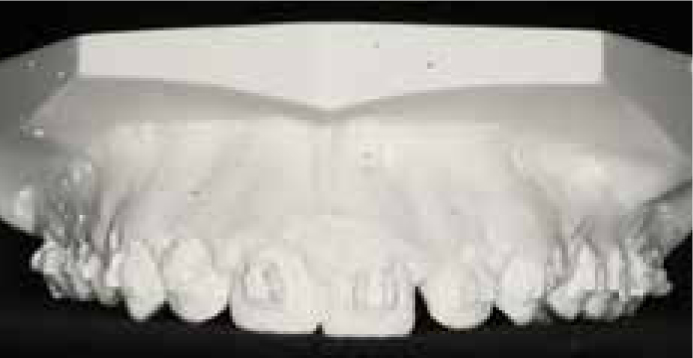
Figure 10. Occlusal view of a poured and trimmed ‘dental cast’ from an alginate impression of a 13-year-old patient.Figure 11. Frontal view of the ‘dental cast’ shown in Figure 9.Figure 12. Dental plaster placed over fixed attachments and in areas of prospective tooth movements.Figure 13. The heat-softened EVA ‘blank’ has been ‘forced’ over the dental cast with positive pressure.
The patient's archwire is removed and an alginate impression (Orthotrace®, Cavex Holland BV, Haarlem, The Netherlands) is taken of the patient's upper jaw to the full depth of the sulcus. In the author's experience, minimal tearing occurs when an ‘automatic’ mixing technique is used. A thin veneer of utility wax, however, may be placed over ‘bulkier’ attachments such as orthodontic bands.
The dental cast model (Super-White Dental Plaster, Whip Mix Corp, 361 Farmington Ave, Louisville, KY 40209) is poured and trimmed (Figures 10 and 11). Once the model is thoroughly dried, ‘runny’ dental plaster is applied over the areas of the fixed attachments and prospective tooth movements (Figure 12). The model is covered with a water-based separator or a polyethylene high-shine foil once the plaster is set.
The model is then placed in the pressure-forming machine. Following the manufacturer's instructions, a heat-softened 3 mm thick EVA ‘blank’ (Erkodent® Erich Kopp GmbH, Siemensstr 3 D-72285, Germany) is ‘forced’ over the plaster cast model with positive pressure (Figure 13).
On removal from the pressure-forming machine, the MG is allowed to cool (usually 20 minutes) and the periphery trimmed to the desired outline using a hot scalpel or special scissors.
For lamination of the second ‘blank’, the base and model side of the ‘blank’ is degreased with an isopropyl alcohol solution and/or the bonding surface of the first EVA blank is roughened with trimming wheels.
The blank is heated using a machine with infra-red heating that allows full thermoforming power before the end of the heating cycle. The manufacturer's instructions are followed for thermoforming the second (2 mm) EVA blank.
This is allowed to cool before trimming and polishing with scissors, tungsten carbide bur in a straight handpiece and silicone-impregnated discs. Final polishing and ‘glossing’ can be achieved with careful use of the flame from a hand-held torch (Figure 14). Careful use of the flame is required to avoid burning and distorting the MG.
The MG is then adjusted to provide even contact between its occlusal surface and the lower teeth on mandibular closure. This can be made in the mouth after first softening the occlusal surface with the flame from a hand-held torch. Caution must be exercised to avoid burning the patient.
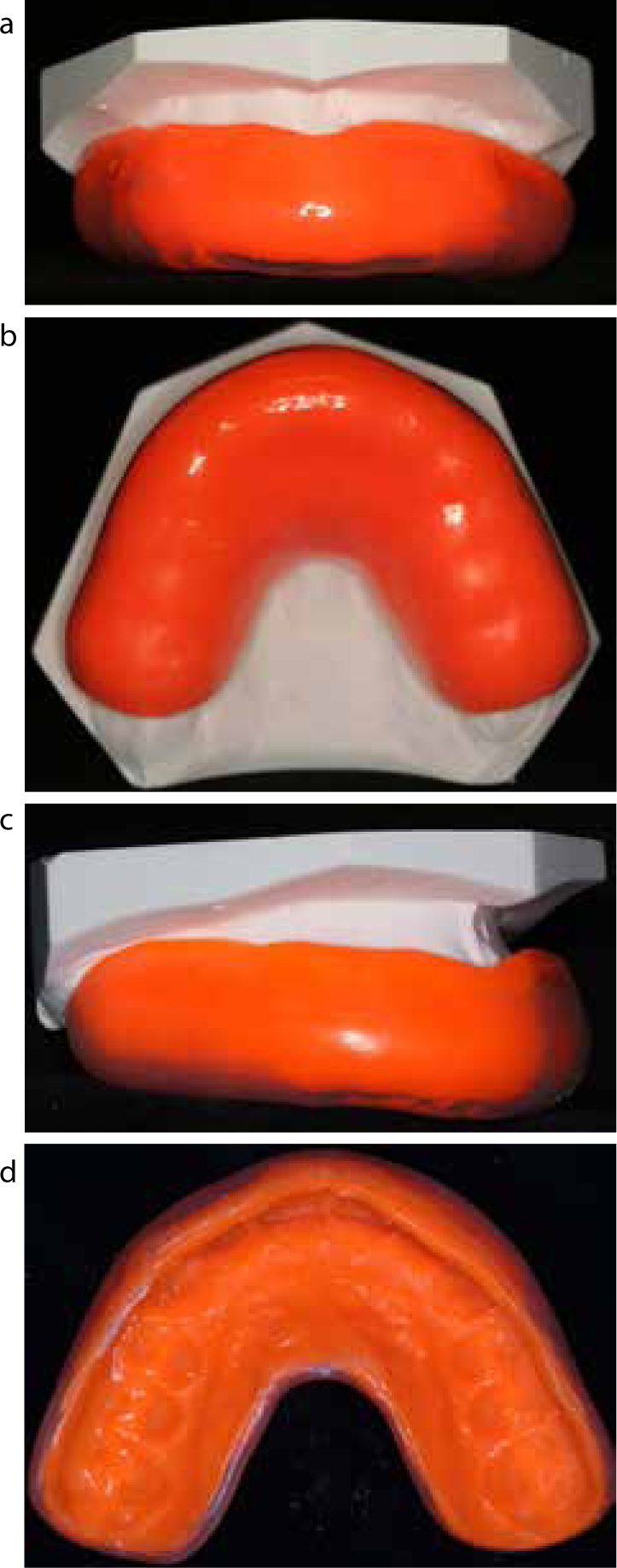
The completed MG is checked for comfort and fit (Figures 15, 16). All patients issued with a MG should be issued with instructions regarding its wear and care (Table 3).30
Figure 14. Final polishing and ‘glossing’ with the flame from a hand-held torch.Figure 15.
(a) Frontal view of the completed MG on the dental cast. (b) Occlusal view of the completed MG on the dental cast. (c) Lateral view of the completed MG on the dental cast. (d) Occlusal view of the fitting surface of the completed MG.Figure 16. Frontal view of the completed MG in the patient's mouth.
Wear only a custom-made MG with balanced occlusion
Wear your MG during practice and during the game
Rinse your MG before and after use
Wash your MG only with soap and in cold water
Clean surfaces with a soft toothbrush or nailbrush after wearing
Do not let others use your MG; it is custom-made for your use only
Store your MG in a clean, rigid and ventilated plastic container
Keep your MG away from sunlight, hot water and heat – it may cause your MG to distort
Check your MG regularly for signs of deterioration, and replace if it is cracking, splitting or the bite is changing
Have your MG checked as part of your routine dental review, or at least annually, by your oral health professional
Contact your oral health professional if your MG becomes loose, too tight or uncomfortable
Consider regular replacement of MGs in children whose mouths are growing, and where baby teeth are being lost and replaced by permanent teeth
This method can be modified further to facilitate patients in the transitional/mixed dentition and for patients wearing fixed slow and rapid maxillary expansion appliances.53
Discussion
The risk of dental injury appears to be greater in those who participate in sporting activity and do not wear a MG compared with those who participate in sporting activity and wear a MG. The risk may be even greater in those with an increased overjet. In addition to superior protection, fitted custom-made MGs appear to result in fewer breathing and speaking problems during wear and do not seem to impact on physiological measurements relevant to athletic performance.48 Further research, however, is still required to establish the optimal design, material and mode of fabrication of MGs.
Additional MG considerations for orthodontic patients include minimal bulk, maximum retention and space requirements for planned tooth movements. To achieve these considerations, a method of fabrication using dental plaster, which is a comparatively inexpensive, readily available and a dimensionally stable material, as the ‘block-out material’ for maintaining the space for fixed orthodontic appliances and planned tooth movements has been described in the article presented here. To decrease bulk and increase MG rigidity, a lamination technique was applied. A pressure-forming technique was employed which may provide superior protection from dental injury, greater fit and patient comfort. The described method may be modified for those in the transitional/mixed dentition and for patients wearing fixed slow and rapid maxillary expansion appliances.
Conclusions
All patients, including those wearing fixed orthodontic appliances, participating in contact sports should wear a fitted custommade MG to protect against dental injury.
Further research is required to establish the optimal design, material and mode of fabrication of MGs.
A fitted custom-made MG with minimal bulk and maximum retention, with areas blocked out on the plaster cast to allow for fixed orthodontic appliances and planned tooth movements, appears to be the design of choice for orthodontic patients.