Edwards A, Elwyn G, Mulley A. Explaining risks: turning data into meaningful pictures. Br Med J. 2002; 324:827-830
: GDC; 2013
The World Health Report: Defining and Assessing Risks to Health. 2002;
Lang N, Suvan J, Tonetti M. Risk factor assessment tools for the prevention of periodontitis progression: a systematic review. J Clin Periodontol. 2014; 42:S59-S70
Cardiovascular disease: risk assessment and reduction, including lipid modification. 2014;
Jackson R, Wells S. Prediction is difficult, particularly about the future. Arch Intern Med. 2007; 167:(21)2286-2287
Persson R, Attstrom R, Lang NP, Page RC. Perceived risk of deteriorating periodontal conditions. J Clin Periodontol. 2003; 30:982-989
Persson R, Mancl L, Martin J, Page RC. Assessing periodontal disease risk: a comparison of clinicians' assessment versus a computerized tool. J Am Dent Assoc. 2003; 134:575-582
Page RC, Martin J, Krall EA, Mancl L, Garcia R. Longitudinal validation of a risk calculator for periodontal disease. J Clin Periodontol. 2003; 30:819-827
Lang NP, Tonetti MS. Periodontal risk assessment (PRA) for patients in supportive periodontal therapy (SPT). Oral Health Prevent Dent. 2003; 1:7-16
Gonzalez-Cabezas Fontana M Minimal intervention dentistry: part 2. Caries risk assessment in adults. Br Dent J. 2012; 213:447-451
Busby M, Martin JA, Matthews R, Burke FJ, Chapple I. The relationship between oral health risk and disease status and age, and the significance for general dental practice funding by capitation. Br Dent J. 2014; 217
Axelsson P. Periodontitis is preventable. J Periodontol. 2014; 85::1303-1307
Weinstein N. Unrealistic optimism about susceptibility to health problems: conclusions from a community–wide sample. J Behav Med. 1986; 10:481-500
Edwards AGK, Hood K, Matthews EJ The effectiveness of one to one risk communication interventions in health care: a systematic review. Med Decis Making. 2000; 20:290-297
Misra S, Daly B, Dunne S Dentist-patient communication: what do dentists and patients remember following a consultation. Implications for patient compliance. Patient Prefer Adherence. 2013; 7:543-549
Newton T, Asimakopoulou K. Managing oral hygiene as a risk factor for periodontal disease: a systematic review of psychological approaches to behaviour change for improved plaque control in periodontal management. J Clin Periodontol. 2015; 42:S36-S46
Asimakopoulou K, Newton T, Daly B, Kutzer Y, Ide M. The effects of providing periodontal disease risk information on psychological and clinical outcomes: a randomized controlled trial. J Clin Periodontol. 2015; 42:350-355
Asimakopoulou K, Nolan M, McCarthy C, Newton T. The effects of goal-setting, planning and self-monitoring (GPS) on behavioural and periodontal outcomes: a randomised controlled trial (RCT). 2017;
Evidence shows that the use of validated risk assessment tools helps healthcare professionals to predict patients' likelihood of developing a disease with greater accuracy. Risk assessment tools have been shown to be beneficial in assisting professionals to communicate findings to patients. The psychological benefits of risk assessment tools have also been demonstrated in terms of positive behavioural change.
CPD/Clinical Relevance: With the current shift towards preventive approaches to healthcare, risk assessment can assist in directing resources and prevention programmes to those patients most in need.
Article
Oral health risk assessment involves the comprehensive assessment of hereditary, clinical and lifestyle factors which impact upon the likelihood of developing oral disease, the findings of which are used to support decision-making in planning preventive care for the patient. Edwards et al described the most effective ways of communicating risk messages to patients.1 Of primary importance is the discussion of those factors with the patient, a conversation which is facilitated through a risk-targeted questionnaire. At the end of the assessment patients should be sufficiently informed such that the derived risk banding does not come as a surprise to them. To have any credibility, risk assessment must use the best available research and evidence base to categorize that patient into risk bands (either numerical or on a traffic light scale). These bandings should enable patients to understand how their risk compares with that of the rest of the population. To carry impact, risk assessment should also encompass providing patients with personalized written reports which document their individualized risk and what they can do about it. Most importantly, the process transfers to patients the knowledge and responsibility for securing their future health.
The GDC,2 WHO,3 EFP,4 NICE5 and similar competent authorities are strong advocates of risk assessment and promulgate it as the keystone of a preventive approach to modern day dentistry. Risk assessment forms the basis of preventive medical care. It also forms part of the requirements for training dental students,6 which means those newly qualified are well versed in the need. But this was not always the case: for the majority of dentists now practising, it was simply not part of their dental school education.
Aims
This paper aims to explain why risk assessment matters. Additionally, it addresses:
How risk is unequally distributed in the population and changes over time;
How targeting those at risk is the best use of resources;
How it helps define your patient care plans;
Why population or practice level risk reduction strategies are essential but not good enough;
Why, importantly, it is not about the number, the risk level, and the precision that can be achieved, but ultimately about the process of communication that addresses the only person who can make that choice to put prevention into practice: the patient; and, of course
Why it works.
About risk
Risk in medicine and dentistry is the probability of developing disease over a specific period of time and has multiple triggers and causes. Lifestyle choices such as smoking and alcohol are factors which contribute to a host of common inflammatory diseases, and public health campaigns which address these are essential to promote healthy behaviour as a social norm and in a cost-effective way. In a dental practice, all patients will benefit from generalized preventive advice and support but, to maximize efficacy, this needs to be run alongside targeted approaches. We all know for example that we should eat healthily, exercise, not smoke and limit alcohol consumption; we do not all comply. However, if your clinician tells you that you personally are at high risk for cardiovascular disease, and part of just say 10% of the population who share those risk factors, how much more seriously are you likely to take his/her recommendations on board?
For any disease, risk is a continuum and people vary in the extent to which they have, and react to, known risk factors. Our response to risk may also change over time. A chocolate-based diet consumed at frequent intervals may result in multiple caries lesions and obesity in one person, whilst the next may remain slim and caries free. This may change as the person ages. With periodontal disease, 10% of the population are disease resistant and therefore plaque for them, in this context, is an irrelevance. At the other end of the spectrum, the 11–15% who are high risk need to invest heavily in supportive periodontal therapy (SPT), which requires a long-term commitment from the patient and an intensive level of support, monitoring and care from the dental team. The impact of this behaviour change and its lifelong support by the dental team is very significant to a patient's quality of life and may impact upon his/her general health. Individualized risk assessment is essential to highlight those differences, to explain to patients what care plan is appropriate for them, and on which areas they personally need to focus.
Risk assessment in medicine
The risk assessment approach is one which has been adopted by the medical profession: NICE guidelines state that patients should be assessed for Type II diabetes using a validated computer-based risk assessment tool, such as the Leicester University tool available from Diabetes UK, as a precursor to HbA1c testing for patients assessed to be medium to high risk.7 A dental practice considering HbA1c testing for diabetes would be advised first to consider the Leicester protocol,8 which also incorporates referral letters detailing the output of the risk assessment to the GMP.
QRISK2 is the NICE-recommended online risk assessment to assess a patient's 10-year risk of having a cardiovascular event for those who are deemed to have an elevated risk.9 Care pathways result: where patients are assessed to have a 10+% risk of developing CVD; serious consideration is given to placing them on statins. Below this level they are simply given lifestyle advice. Patients know the risk level, they know where they sit in the population in terms of risk of a cardiovascular event, are informed of their choices and are encouraged to take personal responsibility for their lifestyle in order to reduce their risk.
Oral disease risk
The causes of oral diseases are complex. Multiple factors influence a patient's risk of developing disease and the progression of existing disease. These include factors that cannot be controlled, so-called non-modifiable risk factors (eg age, gender, genetics), and modifiable risk factors, including lifestyle choices (eg alcohol, smoking, frequency of carbohydrate consumption), together with local plaque retention factors. In isolation, such risk factors may be insufficient to push a particular patient from health to disease, but in combination, they may trip the bacterial or inflammatory load towards disease initiation and/or progression. Historic disease experience is also an important indicator. If the weight of the respective risk factors on a patient's mouth has resulted in disease previously, then minimizing those risks going forward is a prerequisite for a successful preventive plan.
But can we accurately predict oral disease risk? As Jackson and Wells have stated, ‘Risk prediction is not rocket science, but similar to a tax return, most of us cannot do it in our heads’.10 Persson et al11 demonstrated that periodontists base their assessment of periodontal disease almost exclusively on measures of existing disease severity, excluding most known risk factors. A further study, that looked at GDP and expert assessment of the risk of periodontal disease by examining 107 patient records, demonstrated a paucity of agreement in assignment of risk level.12
Computerized tools incorporating validated algorithms and/or the latest evidence base provide consistent and reproducible assessment of risk to support clinical judgement.
There are two systems, PreViser™13 and the PRA14 (Periodontal Risk Assessment) that have been validated in longitudinal trials for assessing risk of periodontal disease. Multiple systems (eg CAMBRA, Cariogram, PreViser™) have been established for caries risk assessment,15 although no predictive algorithm has been validated. Similarly, there is good knowledge of the risk factors for tooth wear or oral cancer, although no algorithm that combines these factors has been shown in clinical trials to predict disease accurately. It would, however, be wrong to take this as a reason not to assess risk and simply focus on fixing disease. In the words of the WHO,3 ‘Estimation of the potential impact of a health hazard can never wait until perfect data are available since that is unlikely to occur’ and ‘Considerable gains can be achieved by reducing the risks of factors that are already known’.
Targeting care with risk assessment
Public Health England's ‘Delivering better oral health: an evidence-based toolkit for prevention’16 states that all patients should receive preventive advice and support and that those deemed to be at increased risk should receive advanced intervention. Risk assessment of each patient determines this requirement and provides measurable outcomes which can be used to monitor success at a population and individual level.
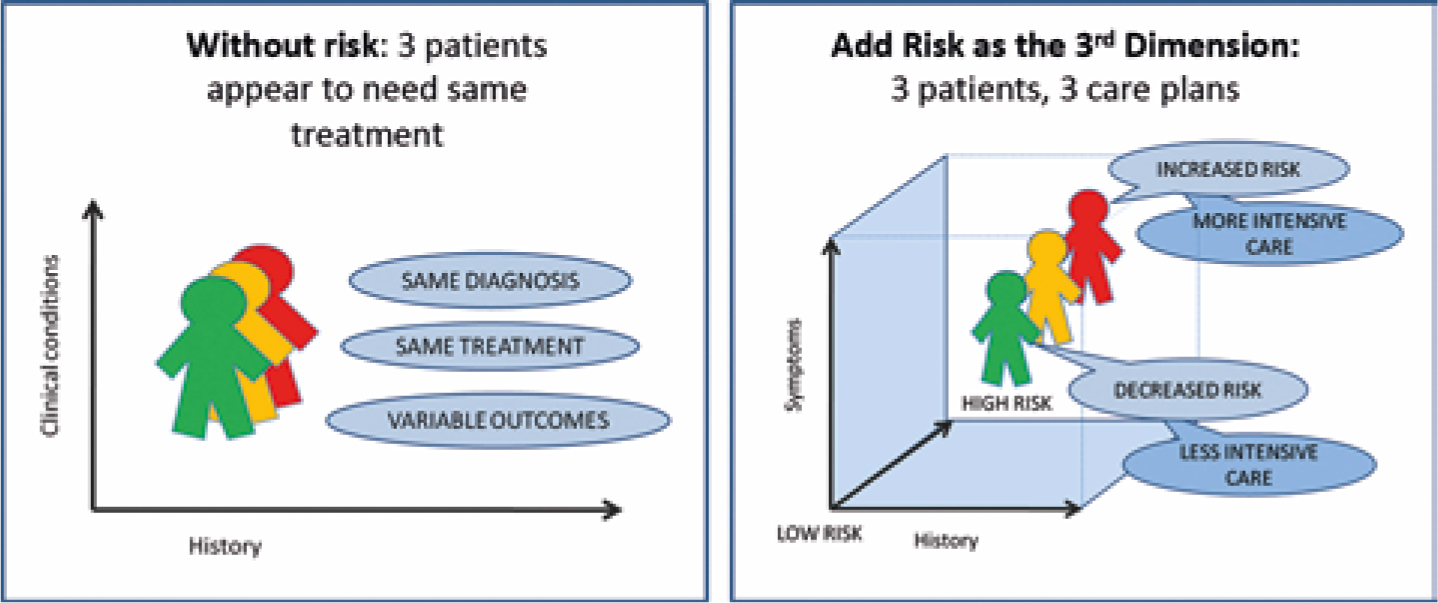
Figure 1 shows the premise of risk assessment from the point of view of the healthcare provider: how, if three patients come into the surgery who have the same diagnosis and are given the same care plan, there can be three different outcomes. Stratifying by risk, ie giving the high risk patient more intensive care and instruction and the low risk, less, will optimize outcomes and target resources most effectively.
Figure 1. Risk as the third dimension.
We know that, in terms of resources, both over and under treatment are consequences of dental healthcare models. Patients who are healthy receive a disproportionate share of clinical time in terms of frequent check-ups and prophylaxis and yet failure to diagnose periodontal disease is a major source of medicolegal claims.
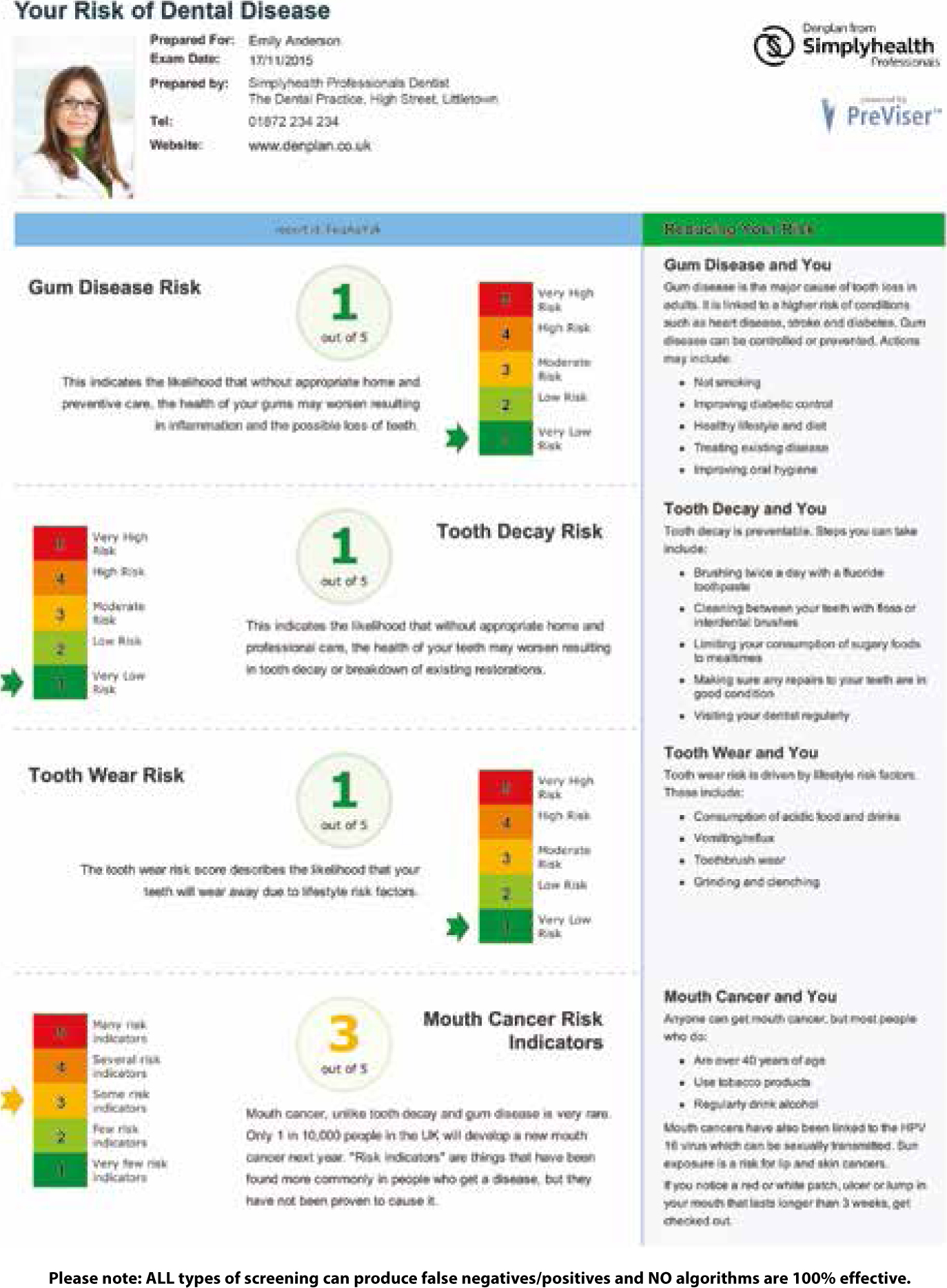
In 2012, NHS pilots were initiated which tried to redress this balance, moving the focus to prevention and away from targets on treatment and access. The NHS pilots start with a comprehensive oral health assessment which categorizes patients into red, amber or green for each of the oral diseases. The protocol restricts advanced NHS-funded treatment until health/improvements are achieved, because otherwise the likelihood of failure is high. This puts the emphasis for both patient and clinician firmly on prevention. A pilot for Medicaid use PreViser™ scores for a similar purpose in the USA. Another innovative programme provided by North East Delta Dental (NEDD) in the USA uses PreViser™ risk assessment to provide enhanced benefits (fluoride varnish, additional hygiene appointments, etc). to insured patients who are assessed at high risk of caries or periodontal disease, with the expectation that overall costs will reduce as preventive strategies take hold. In the UK, the Denplan PreViser™ Patient Assessment ‘DEPPA’ (Figure 2) incorporates the risk assessment findings into A–E capitation bandings to ensure that the recommended patient charge fully reflects the anticipated cost of care.17
Figure 2. DEPPA risk report.
Cure thyself
The most significant impact on outcomes comes from the patients themselves: their oral hygiene, their management of their risk factors and their willingness to engage with the dental professional to accept the help they require to improve or maintain their health. Per Axelsson successfully demonstrated the efficacy of a risk-based preventive approach in a Swedish study that spanned over 30 years.18 His aim was to determine whether caries and periodontitis could be prevented in adults using regular repeated self-care education and professional cleaning with the frequency and approach based on a patient level, tooth and surface level risk assessment. A control group which received standard care had to be abandoned after 6 years because, whilst the intervention group had only 0.2 new carious surfaces per patient, the control group had 14.0. Patients in the control group lost on average 1 mm of periodontal attachment vs a 0.2 mm gain in the intervention group. It was therefore unethical to continue with standard practice. Although the control group was disbanded, the protocol of the intervention group continued and the results were monitored and reported at 15 and 30 years. Over the 15-year period only 0.2 teeth were lost per patient. At 30 years, there was an overall gain of attachment; 92% of patients were brushing twice or more daily. In his 2014 paper in the Journal of Periodontology, ‘Periodontitis is preventable’,18 Professor Axelsson concluded: ‘The profession must move to providing preventive care on an individualised basis’. Whilst data on Swedish people may not be generalizable across other parts of Europe and the world, the message is a powerful one and not one that a responsible and ethical profession can ignore.
Behavioural science and risk assessment
‘It is not sufficient that the public knows what the major risk factors are. Health promotion programs need to go further. They must try to make certain that people actually apply this risk factor information to themselves and form personal risk perceptions that reflect their standing on these risk factors. People often seem quite ingenious in finding reasons for believing that their own risk is less than the risk faced by their peers’. Weinstein termed this behaviour ‘Unrealistic optimism’.19 If we are going to ensure that our patients engage with health promotion, we will need to ensure that we deliver an individualized message and find novel ways of getting this through to our patients.
So what does the literature tell us about how the risk assessment should be conducted in order to minimize ‘unrealistic optimism’?:
‘Individually calculated risk estimates based on personal risk factors were most effective in achieving improved patient outcomes’.20
An interactive process is important:1 the patient should be fully involved in the discussion of risk factors and what their scores mean for them. This is not just a clinical exercise.
Patients need support in making decisions by turning raw data into information that can facilitate the discussions. Simple language should be used. Pictorial presentation: traffic light colours or a simple numerical scale, are important to support the verbal discussions.1
Patients need to know how their risk compares with that of the rest of the population so that they can understand the relevance of the information to them.1
Patients' memory for the content of consultations is poor21 and it is therefore essential to give patients personalized information to take away and digest.
Goal-setting, planning and monitoring, as described by Newton et al, can impact behaviour change by giving the patient a specific measurable target between assessments.22
But does risk assessment change patient behaviour?
The Axelsson study (summarized above) gives a powerful example of the potential of an individualized risk-based approach. A recent European consensus based on systematic reviews of the scientific literature concluded that brief interventions on risk factor control were beneficial in the primary and secondary prevention of diseases.18 In research conducted at KCL, the PreViser™ system has been shown to improve psychological parameters associated with positive cognitive behaviours and self-efficacy in adult patients.23 More recently, biofeedback from PreViser™ was reported to improve oral hygiene behaviours of adults significantly and, for the first time, to improve clinical outcomes significantly by reducing plaque and gingival inflammation scores.24
Conclusion
Oral disease is preventable. Success in healthcare should no longer be measured by the provision of treatment for disease but by the efficacy of a preventive approach. Risk assessment facilitates that process by enabling and supporting the conversation with patients on what their personal combination of risk factors indicates for their future outturn of health and what steps can be put in place, both inside and outside the dental surgery, to achieve optimum outcomes. In the words of the GDC Standard 2.3,2 it provides the information patients need in a way they can understand so that they can make informed decisions. And in doing so, the evidence supports their successful achievement of positive psychological and clinical improvements.