The surgical removal of an impacted canine: diagnosis, investigations and technique Zarish Rahman Hamnah Azam Bilal Ahmed Dental Update 2024 45:8, 707-709.
Authors
ZarishRahman
BDS(Hons), MFDS, PGCert(Dent Ed)
Orthodontic Specialty Registrar, Birmingham Dental Hospital, 5 Mill Pool Way, Birmingham B5 7EG, UK
Impacted canines occur in 1.7% of the population. These cases may be seen in general practice for further referral to an orthodontist or oral surgeon. Diagnosis often involves clinical examination, palpation and radiographic imaging to ascertain the location and association with anatomical structures. By using a clinical case, this paper aims to demonstrate one conservative way of managing the removal of impacted maxillary canines.
CPD/Clinical Relevance: Canine impactions can cause resorption to adjacent teeth. They may require orthodontic traction to be brought into alignment but in some cases surgical removal is necessary.
Article
The surgical removal of impacted maxillary canines is a commonly performed procedure in oral surgery. Indications for this procedure include impacted canines causing root resorption or hindrance of eruption of other teeth and canines undergoing cystic change.1,2 During this process, diagnosis and investigation are achieved through clinical examination, palpation and radiographic imaging. Clinicians routinely use the horizontal or vertical parallax technique which involves using radiographic images taken at different angulations. This is usually performed to help determine the location of the impacted tooth. High quality radiographic imaging in the maxillary incisal region may also help identify local anatomical features, such as the nasopalatine foramen. It is important to identify such features during the surgical treatment planning stages.
History
A 19-year-old female was referred to the oral surgery department for the orthodontic extractions of her retained URC and ULC to aid management of her impacted canines.3 Upon clinical and radiographic investigations, it was determined that the maxillary canines were positioned unfavourably and would not be suitable for orthodontic extrusion; thus needing to be surgically removed.4 The patient had an underlying skeletal malocclusion that required a bimaxillary osteotomy. However, the patient was not keen on orthognathic surgery. Thus it was agreed by the orthodontist and patient to mask her bimaxillary proclination with orthodontic camouflage, by removing her impacted canines and bringing her maxillary first premolars anteriorly to mimic canines.
Investigations
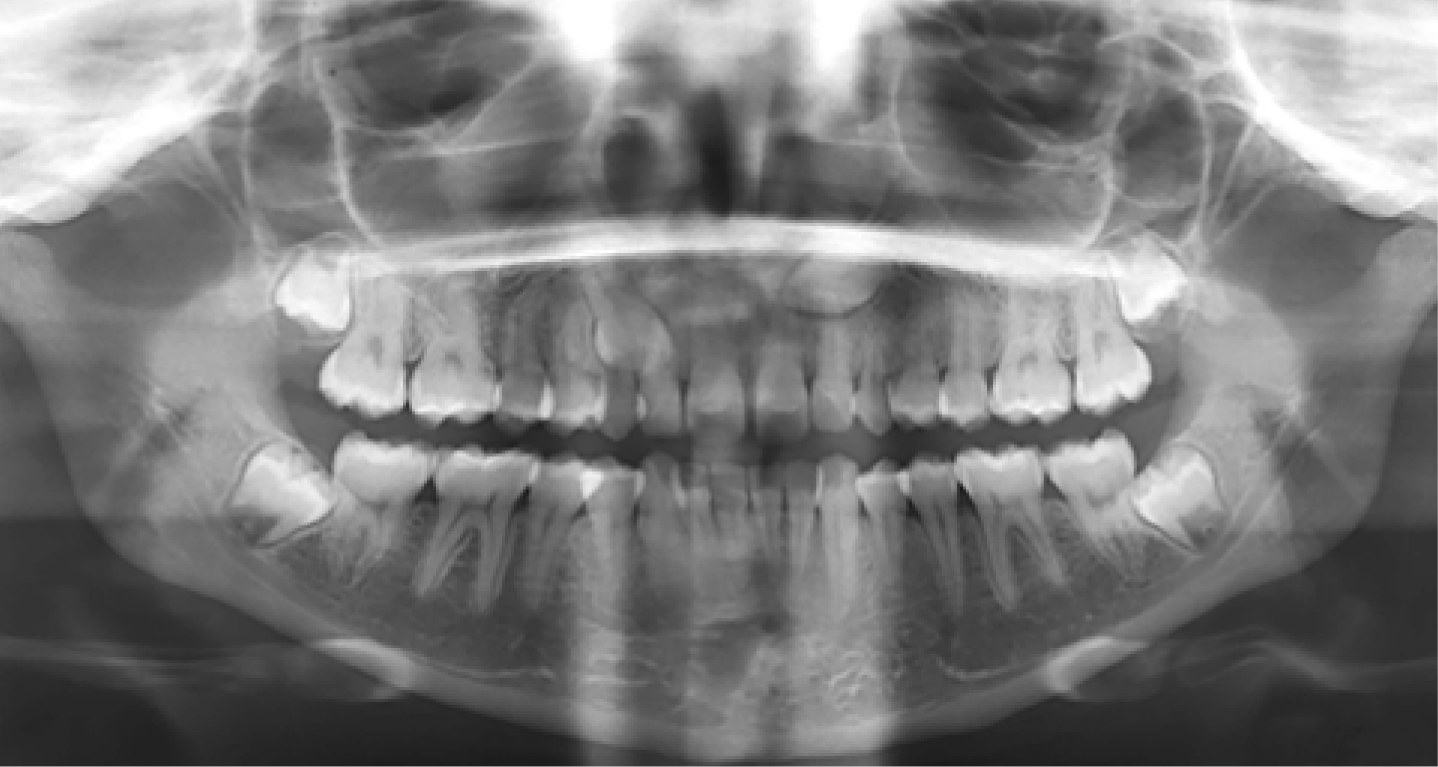
A lateral cephalometric reading, an anterior maxillary occlusal and an orthopantomogram were used initially. A cone beam CT was required to investigate the close proximity to the adjacent maxillary lateral incisors as well as potential resorption. Figure 1 shows a lateral cephalogram of the patient, with an arrow to indicate an underlying Class III skeletal malocclusion and bimaxillary proclination; the patient's full dentition is shown in Figure 2 via OPG.
Figure 1. Lateral cephalogram of the patient showing an underlying Class III skeletal malocclusion and bimaxillary proclination.Figure 2. Orthopantogram of the patient's dentition.
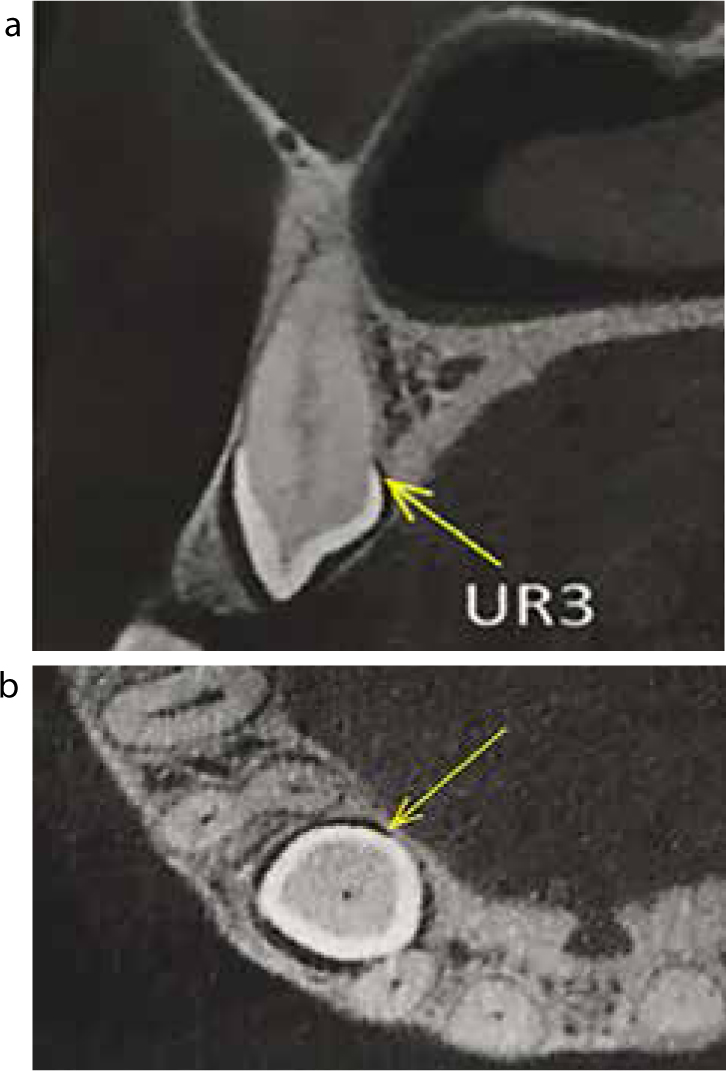
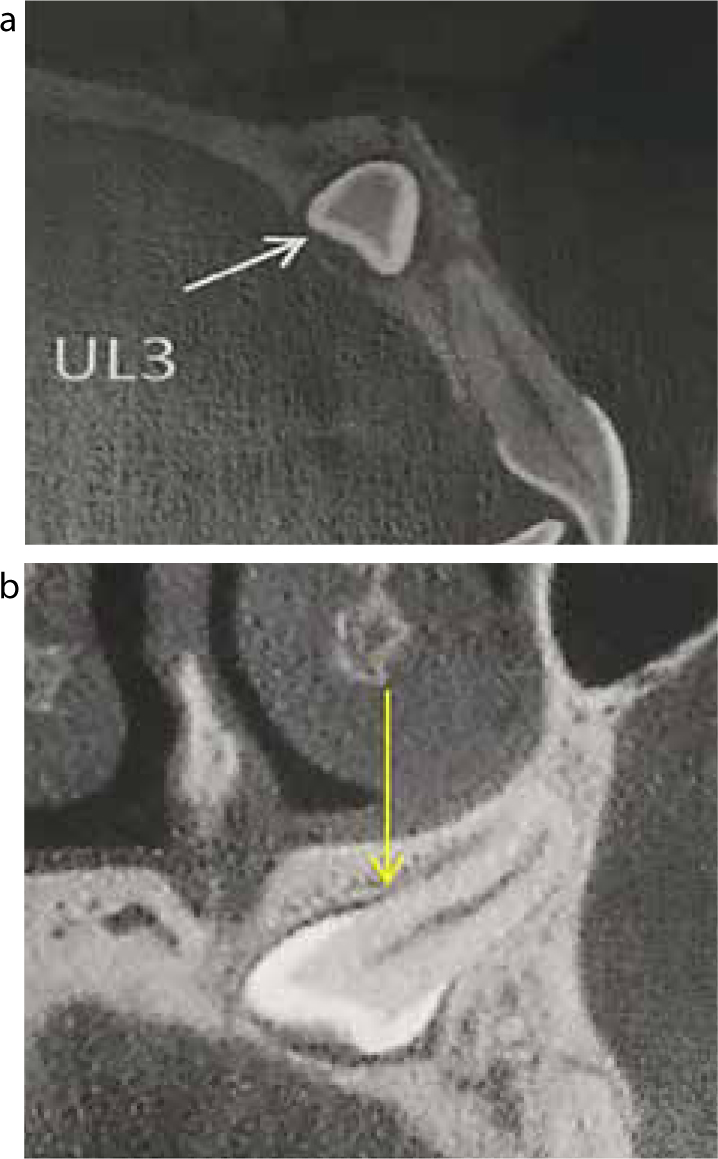
The OPG (Figure 2) and anterior maxillary occlusal radiograph (Figure 3) illustrate palatally impacted and unfavourably positioned maxillary canines (indicated by arrows). The maxillary CBCT in Figure 4 shows the UR3 (indicated by an arrow), whilst Figure 5 shows the UL3 (indicated by an arrow). The images shown in Figures 4 and 5 helped to determine the angulation and degree of impaction of the maxillary canines.
Figure 3. Anterior maxillary occlusal radiograph of the patient.Figure 4.
(a, b) Maxillary CBCT of the patient showing the UR3 (indicated by arrows).Figure 5.
(a, b) Maxillary CBCT of the patient showing the UL3 (indicated by arrows).
Surgical technique
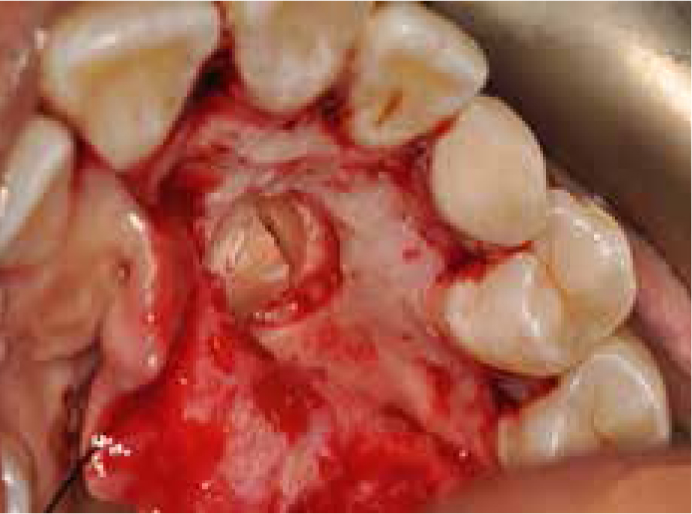
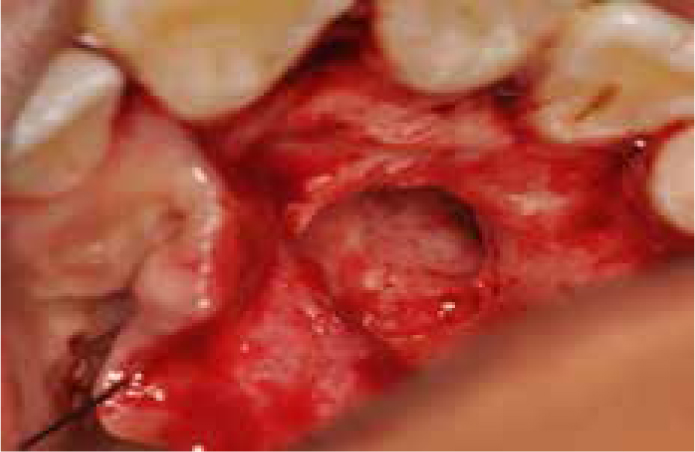
The procedure for the surgical removal of the upper left canine was carried out under Midazolam IV sedation together with local infiltrations of lignocaine and articaine by one of the authors (BA). A pre-operative image of the maxillary arch can be seen in Figure 6. A full mucoperiosteal flap extending from the UR1 to UL6 was raised using a curved Warwick James to reflect the papilla. This was then followed by the use of a Howarth's periosteal elevator further to reflect the flap shown in Figure 7.5 A black silk retraction suture was used to retract the flap to ensure good visual access without impinging on the nasopalatine nerve (Figure 8). Bone removal was necessary to expose the crown of the tooth. Using the CBCT to help locate the crown (Figures 4 and 5), a round stainless steel bur was used to remove bone carefully whilst making sure to stay clear of adjacent teeth; the follicular tissue was removed as it may prevent bony healing. The crown head of the impacted canine can be seen in Figure 9. As seen in Figure 10, the crown was sectioned using a Toller fissure bur. A luxator was then used to free the periodontal ligament and mobilize the root (Figure 11), whereas a Coupland's I was used to elevate the root (Figures 12 and 13). Figure 14 shows the remaining socket which was curetted and irrigated before closure. The flap was then closed with interrupted sutures with the knots lying buccally to limit patient discomfort (Figure 15). Figure 16 shows the extracted crown and root.
Figure 6. Pre-operative image of the maxillary arch.Figure 7. A full mucoperiosteal flap extending from UR1 to UL6 was raised using a curved Warwick James.Figure 8. A black silk suture was tied to the flap as a useful retraction technique.Figure 9. The crown head of the impacted canine.Figure 10. The crown was horizontally sectioned using a Toller fissure bur.Figure 11. A luxator was used to break the periodontal ligament and mobilize the root.Figure 12. A Coupland's II elevator was used to elevate the root.Figure 13. The root was elevated intact.Figure 14. The remaining socket.Figure 15. Flap closure with interrupted sutures.Figure 16. Image of the extracted crown and root.
Conclusion
This case describes the conservative technique used for the surgical removal of a palatally impacted maxillary canine. Careful patient selection ensured a successful procedure under intravenous sedation, thus eliminating the need for a GA. Good surgical retraction ensured adequate visual access without compromising the neurovascular bundle.