
References
Diabetes mellitus: an update for the general dental practitioner
From Volume 45, Issue 8, September 2018 | Pages 750-759
Article

Diabetes is a chronic syndrome of hyperglycemia with anomalies in carbohydrate, fat and protein metabolism due to lack of insulin production, decreased cellular sensitivity to insulin or both.1,2,3 Most cases of diabetes fall within two main categories:
Diabetes is a major cause of multi-organ failure, heart attacks, blindness and nephropathy. It is an increasing public health concern and has been declared a pandemic.4 The incidence of diabetes is approximately 422 million worldwide, with 1.5 million deaths attributed to it in 2012.5
Aetiology
Genetic factors
Twin studies have demonstrated that genetic susceptibility plays a vital role in the aetiology of Type II diabetes. An increased susceptibility can also be inherited in Type I diabetes, but to a lesser extent than in Type II.6 An early study found impaired glucose tolerance in 30% of subjects who were close relatives of diabetics, as opposed to 6% of subjects who had no diabetic relatives.7 The HLA-DR3 and DR4 serotypes increase an individual's susceptibility to diabetes 14-fold.8 Difference in glucose metabolism is a key factor in Type II diabetes and studies show differences amongst different races. β-cell function is thought to be inheritable.9 However, the precise role of genetics in diabetes remains indeterminate as environmental factors also play a modifying role.6
Environmental influences
Environmental factors have a role to play in onset and outcome of the disease. This is evidenced by the marked geographical difference in its incidence. Nordic countries have the highest incidence and Asian counties, the lowest. Differences were also seen in different parts of the Caribbean, and rural and urban Malaysia.6
Gender
A study in 1993 showed a higher rate amongst males, suggesting the influence of testosterone.10 However, studies conducted in Canada and Italy did not concur.6
Nutritional factors
Verge postulated that early exposure to dairy milk could increase the diabetic risk in infants.11
Viruses and infection
A study revealed about 20% of new cases were positive for coxsackie antibodies.12 Twenty percent of children with congenital rubella had later developed diabetes.13
Immunological aspects
Autoimmune diseases rarely occur in isolation; patients with Type I diabetes often suffer from conditions like pernicious anaemia or autoimmune thyroid diseases. Over 70% of Type I diabetics suffer from islet cell antibodies.6 Insulin resistance is seen in late pregnancy.
Physical activity
Physical activity diminishes risk of Type II diabetes by increasing sensitivity to insulin and glucose metabolism. A study in Mauritius showed positive association between physical inactivity and diabetes. These findings were across all ethnic groups, which further supported the theory.14
Pathophysiology
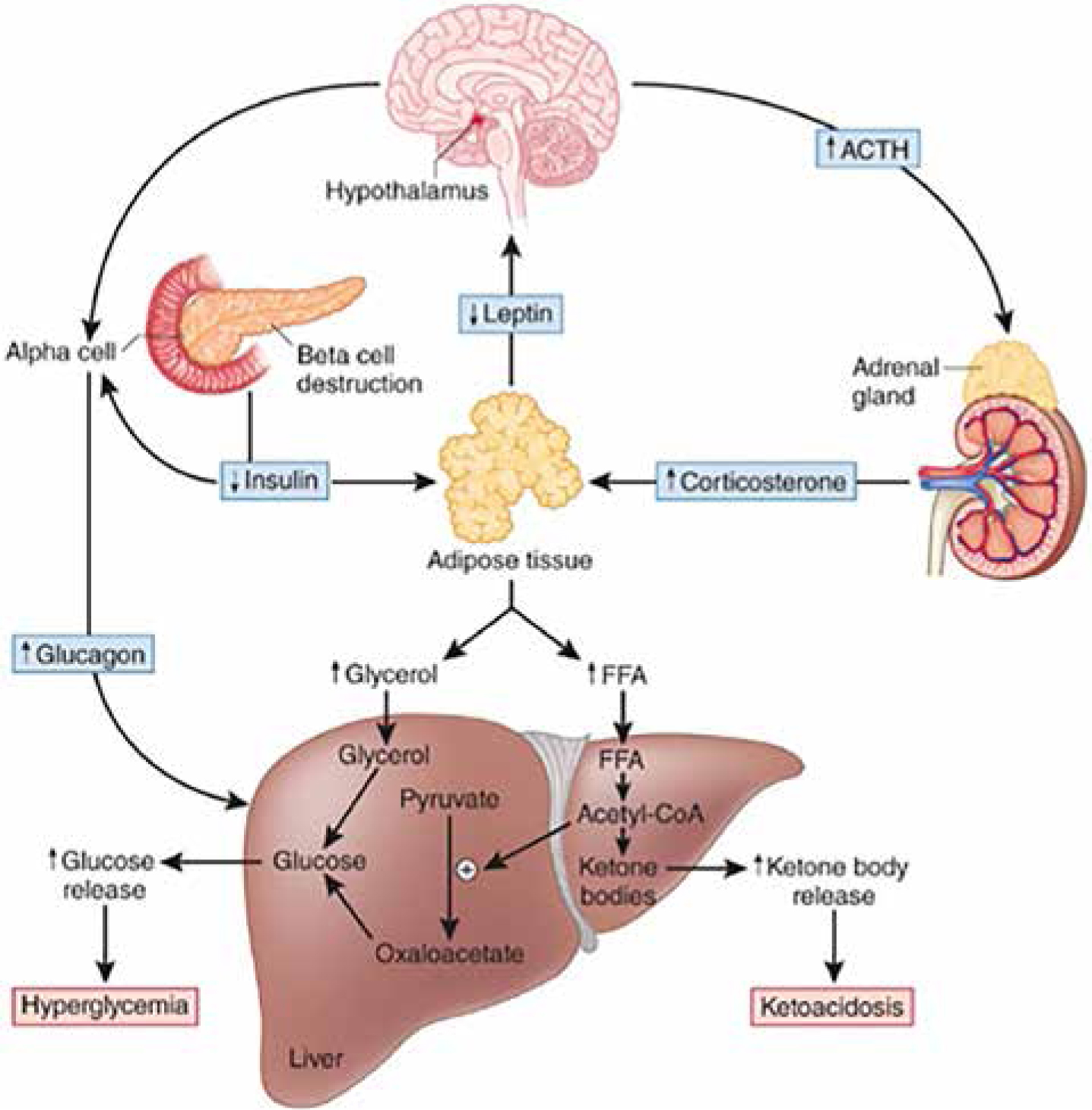
Type I diabetes is characterized by autoimmune destruction of β-cells that secrete insulin in the pancreas. The basis for autoimmune theory comes from inflammation within the islet of Langerhans. As diabetes progresses, β-cells decrease in number and so do their ability to regenerate.15 Cadaveric investigations of Type I diabetics revealed 70% with complete β-cell deficiency; 1% of those displaying inflammation. There was selective loss of β-cells with normal count of other Langerhans cells such as glucagon secreting α-cells, somatostatin secreting δ-cells and pancreatic polypeptide secreting PP cells. More than 90% of Type I diabetics have autoantibodies against β-cells. Autoantibodies include islet cell antibody, glutamic acid decarboxylase, and zinc transporter 8. Serological testing for those autoantibodies can identify at-risk individuals. Several studies have postulated proinsulin to be an important autoantigen in diabetes; which could explain the selective destruction of β-cells. Genetic susceptibility to diabetes comes from the human leucocyte antigen (HLA) genes; HLA-DR3 and DR4 showing the strongest association.15 T lymphocytes are most abundant in islet lesions, followed by macrophages, lymphocytes and plasma cells. These features, combined with the presence of autoantibodies against islet cells, show both humoral and cellular immunity involvement in the pathogenesis of diabetes.16
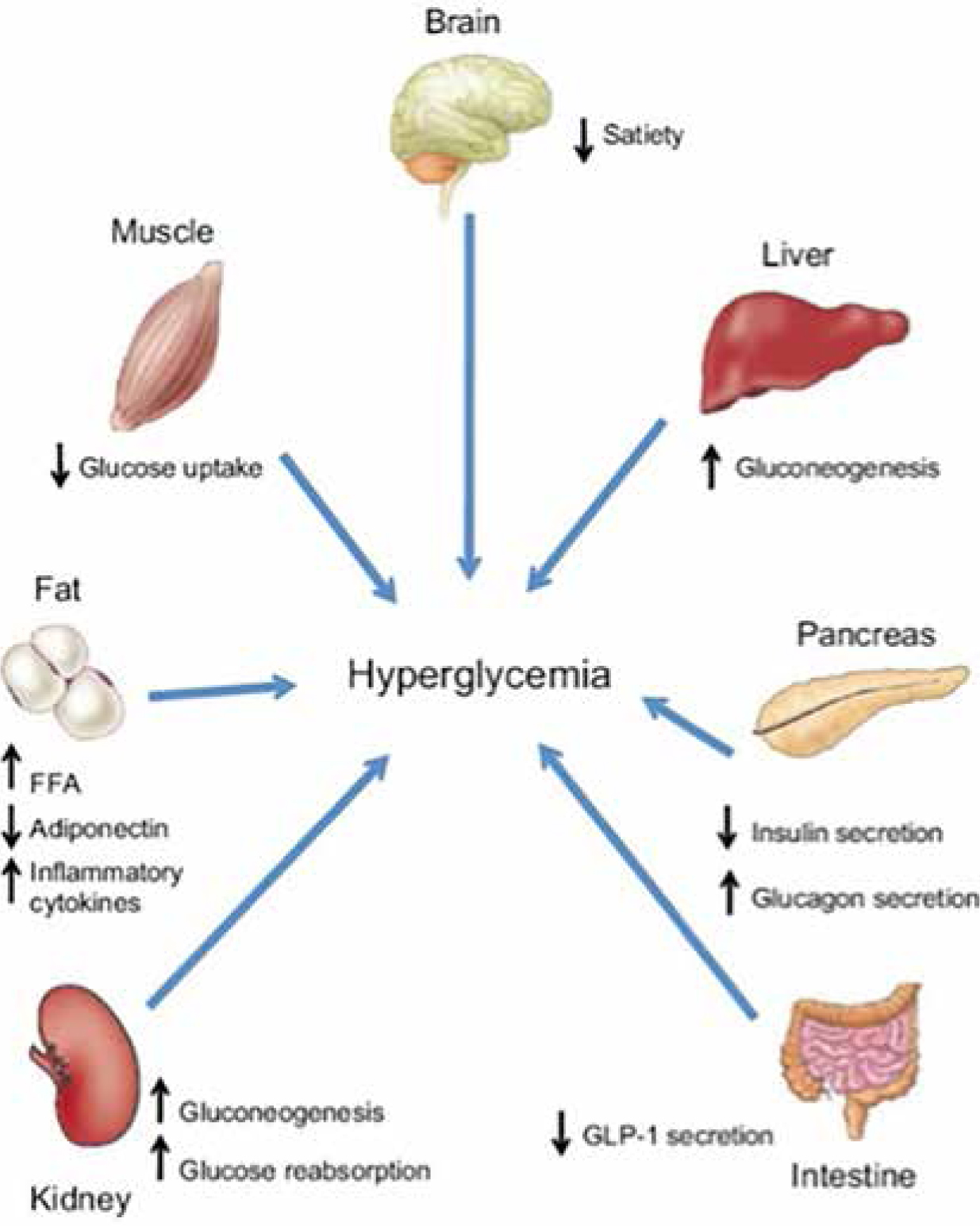
Pathophysiology of Type II diabetes has been extensively investigated. The advent of radioimmunoassay differentiated between ‘insulin-sensitive’ and ‘insulin-insensitive’ individuals.16 Kahn et al determined that the association between β-cell function and insulin sensitivity was better explained by a regulated feedback control system that maintains glucose homeostasis.17 Insulin is secreted in answer to β-cell stimulation and acts in the liver to stop glycogen being converted to glucose. Insulin also acts on insulin-sensitive tissues such as adipose and muscle to encourage glucose uptake. In turn, the insulin-sensitive cells respond via humoral mechanisms to the β-cells and determine the need for insulin. As insulin resistance develops, β-cells increase insulin manufacture to preserve normal glucose tolerance. When β-cells fail to keep up, blood glucose rises. Initial manifestation of impaired glucose tolerance eventually results in diabetes as sustained elevations in blood glucose occur. Progression to diabetes is a continuum where there is steady decline in β-cell function. Reduction of β-cells seen in Type II diabetes is due to elevated glucose, fatty acid and amyloid deposition that causes β-cell apoptosis. β-cell loss is amplified by the fact that the pancreas is incapable of regenerating β-cells beyond the third decade. Glucagon-like-peptide-1 is released by the digestive tract and acts on β-cells to enhance insulin production and on α-cells to suppress glucagon production. While glucagon-like-peptide-1 levels remain alike in diabetics and non-diabetics and act directly on α-cells, glucagon suppression is insufficient in Type II diabetics during meal times. It is thought that β-cells influence this glucagon suppression, but the exact mechanism remains to be elucidated. Bile acids instigate release of fibroblast-growth-factor-19 which induces glycogen and reduces glucose production; thereby contributing to glucose homeostasis.9 Studies have suggested that alterations in intestinal microbiome may be associated with progression of Type II diabetes.18 The central nervous system controls glucose metabolism by adapting insulin and glucagon production. The hypothalamus regulates liver glucose.
Hypothalamic inflammation caused by a fatty diet leads to reduced insulin sensitivity and dysregulation of body weight.9 High-fat diet and physical inactivity results in a positive energy balance, which firstly fills the adipose cells under the skin. As fat accumulates, it is stored in muscle, liver, pancreas, blood vessels and pericardial tissue. The adiposity, especially within the intra-abdominal cavity, results in impaired glucose uptake due to intracellular impairment of insulin signalling.16Figures 1 and 2 highlight the pathophysiology of Type I and Type II diabetes mellitus, respectively.19,20
Diagnosis
The WHO published guidelines in 2006 on the diagnosis of diabetes.21 There are several ways to test for diabetes:
Table 1 highlights how diabetes is diagnosed as per the American Diabetes Association.20
| A1C ≥6.5% The test should be performed in a laboratory using a method that is NGSP certified and standardized to the DCCT assay.* |
| OR |
| FPG ≥126 mg/dl (7.0 mmol/l). Fasting is defined as no caloric intake for at least 8 h.* |
| OR |
| 2-h plasma glucose ≥200 mg/dl (11.1 mmol/l) during an OGTT. The test should be performed as described by the World Health Organization, using a glucose load containing the equivalent of 75 g anhydrous glucose dissolved in water.* |
| OR |
| In a patient with classic symptoms of hyperglycemia or hyperglycemic crisis, a random plasma glucose ≥200 mg/dl (11.1 mmol/l). |
The association between FPG and retinopathy was used to identify threshold glucose level in 1997. These analyses were used to define cut-off points as 126 mg/dl for FPG and 200 mg/dl for OGTT. HbA1C is useful in assessing adequacy of glycemic control, reflecting the mean plasma glucose level over the previous 2 months. HbA1C is unsuitable for diagnosing patients with haemoglobinopathies such as sickle cell anaemia or thalassaemia, children, acutely ill patients and patients on steroids. There is a category of patients whose glucose levels are not elevated enough to be classified under diabetes but are greater than normally considered. These patients were classified as having impaired fasting glucose (IFG) or impaired glucose tolerance (IGT) and termed as pre-diabetes. The American Diabetes Association endorses that pregnant women, who are not known diabetics, have an OGTT at between 24 and 28 weeks of gestation, as shown in Table 2.22
| Perform a 75–g OGTT, with plasma glucose measurement fasting at 1 and 2 h, at 24–28 of weeks gestation in women not previously diagnosed with overt diabetes. |
Early discovery and treatment of diabetes is recommended to minimize the burden of the disease (Table 3).
| Age > 45, particularly in those who are overweight (BMI > 25kg/m2) |
| Age < 45, particularly in those who are overweight (BMI > 25kg/m2) and have additional risk factors |
| First degree relatives with diabetes mellitus |
| Sedentary lifestyle |
| Delivered a baby weighing >9lb or have been diagnosed with gestational DM |
| Hypertension (BP > 140/90 mm) |
| HDL < 35 mg/dl and/or triglycerides > 250 mg/dl |
| On previous testing, had impaired glucose tolerance or impaired fasting glucose |
| History of vascular disease |
Systemic manifestations
Systemic manifestations of both Type I and Type II diabetes are numerous and may have devastating long-term consequences. These can be divided into microvascular and macrovascular. Microvascular complications are first to occur and include retinopathy, neuropathy and nephropathy. Macrovascular complications present at a later stage and can be in the form of cardiovascular disease and cerebrovascular accidents. Diabetes can also be associated with acute complications, potentially fatal, such as diabetic ketoacidosis in the event of hyperglycemia or diabetic coma in the event of hypoglycemia.
Nephropathy
In diabetics, continued hyperglycemia is acknowledged to be a profound risk factor for the initiation and progression of diabetic nephropathy. Hyperglycemia causes expansion and injury of mesangial cells by an increase in the mesangial cell glucose concentration. Initial glomerular mesangium expansion occurs by cell proliferation and subsequent cell hypertrophy, causing increased reabsorption and in turn contributes to hyperfiltration. Proteinurea is the presence of excess protein in the urine and is an indicator and potential contributor to renal damage. An increase in glomerular permeability allows plasma proteins to enter the urine. Some of these proteins will be absorbed by the proximal tubules, thereby propagating an inflammatory mechanism resulting in interstitial scarring and subsequent fibrosis. Tubular interstitial fibrosis is an indicator of an advanced stage of diabetic nephropathy and is a more accurate indicator of renal failure than glomerular sclerosis. Nephropathy affects all kidney functions including erythropoietin release, activation of vitamin D and re-uptake of water.23
Retinopathy
Diabetic retinopathy causes blindness through longstanding microvascular damage within the retina.21 Vascular damage encompasses increased vessel permeability and degeneration, micro-aneurysms and disproportionate angiogenesis. Cellular death alters colour perception. Retinopathy is separated into two stages; non-proliferative and proliferative. Patients are usually asymptomatic in early disease. Degeneration of the condition ends in retinal detachment.23
Neuropathy
Neuropathy occurs in the majority of diabetics, with 15% having amputation of the lower extremities.23 It affects both the autonomic and somatic nervous system. Pathological changes include endothelial thickening and subsequent hypoxia. Disease progression leads to loss of sensation to thermal/physical stimuli. Patients can experience allodynia or hyperesthesia. Recent studies suggest autonomic and sensory neurones are affected more than motor neurones. Longer nerve fibres first exhibit signs of degeneration, clinically manifested in the feet as paraesthesia, anaesthesia and loss of reflexes. Similar symptoms follow in the hands; termed as ‘glove and stocking’ distribution. As anaesthesia sets in, diabetics do not respond to lower limb injuries, elevating the risk of ulcers, leading to amputation. Patients also suffer from numerous bony foot fractures, leading to permanent deformation. Effect on the autonomic nervous system may manifest as orthostatic hypotension, diarrhoea and urinary incontinence.23
Cardiovascular disease
Diabetics are at increased risk of cardiac diseases such as myocardial infarction, atherosclerotic plaques, impaired diastolic function and cerebrovascular accidents. Atherosclerosis begins with endothelial damage. As low density lipoproteins accumulate in the endothelium, macrophages and T-cells attempt at digesting them. With years, these cells form atheromas which solidify to form atherosclerotic plaques, narrowing the lumen, reducing arterial blood flow. The atherosclerotic process is accelerated in diabetics, particularly if poorly controlled. This manifests as claudication or angina. Plaque rupture leads to strokes or myocardial infarction. Diabetic cardiomyopathy describes injury to the cardiac muscle cells and their performance, non-attributable to hypertension or coronary artery disease in diabetics. Changes in myocardial structure, calcium signalling and uptake are primary signs of cardiomyopathy. Diabetics present with co-morbidities augmenting risk of left ventricular hypertrophy and heart failure.24 Cellular behaviour within vessels are affected by oxidative stress and longstanding inflammation and favour thrombosis. Poor healing ability coupled with low endothelial progenitor cells contribute to multi-organ failure and substantial morbidity.23
Oral manifestations
Diabetes is associated with several oral health complications. Dentists are at the forefront of management of such patients (Table 4).
| Burning Mouth Syndrome |
| Candidiasis |
| Dental Caries |
| Gingivitis |
| Glossodynia |
| Lichen Planus |
| Neurosensory Dysethesias |
| Periodontitis |
| Salivary Dysfunction |
| Taste Dysfunction |
| Xerostomia |
Gingivitis and periodontitis
Poorly controlled diabetics show higher incidence of gingivitis, periodontitis and periradicular bone loss. Glycemic control is proportional to the severity of periodontal disease and is also bi-directional; meaning that poor periodontal health worsens diabetes. A recent meta-analysis supported this statement.25 A few theories have been postulated; including change in bacterial composition of subgingival plaque, weakened immune defence impairing leucocyte action and release of tumour necrosis factor (TNF). Increase in collagen breakdown and decrease in synthesis result in destruction of the periodontium.3,4
Dental caries
Diabetes is not directly responsible for causing caries. Increased susceptibility to dental caries stems from reduction in salivary production and periodontal destruction. Decreased saliva implies reduction in acid buffering capacity, in turn aiding Streptococcus mutans in rapidly destroying tooth structure.2
Salivary and taste dysfunction
Saliva functions include lubrication, taste, antibacterial effect and buffering capacity. Studies report salivary dysfunction in diabetics, especially those with neuropathy. Salivary flow rate from the parotids after stimulation was lower in patients with poor glycemic control. Resultant xerostomia may lead to soft tissue irritation and causes chronic inflammation and discomfort. Diabetic medications also contribute to xerostomia which can present first with polydipsia. The reasons for salivary hypofunction in diabetes are unknown but could be due to alteration in basement membrane of salivary glands. Diabetics also suffer from altered taste with reduced saliva as a contributing factor. Again, taste dysfunction is worse in poorly controlled diabetes. Poor glycemic control succeeds poor eating habits.1,2,4
Oral infections
Immunosuppression of diabetics predisposes them to opportunistic infections like candidiasis. Fungal infections are more common in poorly controlled diabetics who are also smokers, denture wearers or long-term steroid users. Low saliva flow plays a role in overpopulation of fungi. Diabetics are also predisposed to spreading and recurrent bacterial infections; which are more severe compared to healthy individuals, because they have an impaired defence mechanism hence are considered to be immunocompromised. Streptococcal bacteria are more common and infections easily spread in the submandibular regions. Diabetics with dental and facial abscesses need to be treated with urgency to avoid spread to deep fascial spaces.2,4
Oral mucosal diseases
Oral lichen planus and recurrent apthous ulceration have been described in diabetics. Oral lichen planus, which is considered to have an autoimmune aetiology, is more frequently seen in Type I diabetes.3,4 Consensus for diagnosis of oral lichen planus is histopathological, which may require the general dental practitioner to refer patients to an oral and maxillofacial or oral medicine department.
Neurosensory disorders
Neuropathy increases the risk of oral neurosensory disorders, such as burning mouth syndrome, because the reduced density of epithelial nerve fibres with axonal degeneration results in this persistent painful condition.26 Burning mouth syndrome has an adverse effect on quality of life of patients and may affect food intake and oral hygiene practices. This in turn affects diet control of glycemia and periodontal health. Increase in Langerhans cells is associated with immune dysfunction and has been seen in cases of neuropathy.2,4
Treatment of diabetes
Diet and lifestyle
Diet and lifestyle modification are central to diabetic management. Changes in diet have shown to improve HbA1c. To improve sensitivity to insulin, diabetic patients should aim at an intake of about 1000 kilocalories under their energy needs. Limiting carbohydrate intake is beneficial in patients on insulin. A high fibre diet improves cardiovascular health and glycemic control. Sucrose intake that contributes to energy expenditure does not adversely affect glycemic control, but care should be taken to avoid excessive consumption as it increases overall calorie intake. Exercise is recommended in diabetics and helps reduce abdominal fat, improving circulation, decreasing blood pressure and increasing insulin sensitivity of tissues.27,28
Pharmacological management
The goal of pharmacotherapy is to maintain rigid control of blood glucose. Drug management of diabetes can be oral or injectable.
Insulin therapy
Insulin therapy is the main drug used for treating Type I diabetics. They can be rapid-acting or long-acting. They mimic endogenous insulin production; basal and postprandial. During fasting, a long-acting insulin is used, which is then supplemented by a rapid-acting insulin to cover meal times. Continuous subcutaneous insulin in the form of a pump can also be used in Type I diabetics.
Oral hypoglycemic agents
Oral hypoglycemics are the first line of treatment in Type II diabetics. They either increase release of insulin or increase tissue sensitivity to insulin. Sulphonylureas and meglitinides work on sulphonylurea receptors to release insulin. These drugs are effective in patients with a functioning pancreas. Hypoglycemics that increase the action of insulin include bisguanide, thiazolidinediones and α-glucosidase. Bisguanides, for example metformin, increases muscles’ sensitivity to glucose and decreases the liver's production of glucose. Thiazolidinediones, such as pioglitazone, improve insulin's sensitivity in fat and muscle. α-glucosidase inhibitors, like acarbose, prevents digestion of carbohydrates (Table 5).3,9,27
| AGENT | MODE OF ACTION | ADVERSE EFFECT |
|---|---|---|
| Insulin Secretagogues | ||
| Sulfonylureas (currently third generation – glipizide, glimepiride, etc) | Bind to sulfonylurea receptors on the beta cells triggering release of insulin |
Hypoglycemia |
| Meglitinides (repaglinide, nateglinide) | Bind to sulfonylurea receptors |
Generally none, but possible hypoglycemia |
| Insulin Sensitizers | ||
| Biguanides (metformin) | Decrease hepatic gluconeogenesis and increase peripheral glucose uptake |
Diarrhoea, abdominal pains |
| Thiazolidinediones (rosiglitazone, pioglitazone) | Activate peroxisome proliferator-activated receptor γ to affect glucose and lipid metabolism |
Weight gain |
| α-Glucosidase Inhibitors | ||
| Acarbose Miglitol | Inhibit α-glucosidase in the gut and, thus, prevent breakdown of some complex carbohydrates into simple sugars that then cannot be absorbed |
Bloating, diarrhoea and flatulence due to action of colonic bacteria on undigested carbohydrates |
Effect on oral wound healing
Diabetics suffer from delayed wound healing due to poor soft tissue repair and osseous restoration. Various mechanisms have been postulated to explain this, such as decreased vascularity, diminished growth factor production, weakened humoral immunity or psychological pressure.4
Factors affecting would healing
The sequence of wound healing includes haemostatic and inflammatory phase, cell proliferation and healing. Local and systemic factors can interfere with healing, like smoking, alcohol, age and diabetes.29
Circulation and vascularization
Decreased vascularity in diabetics potentially encourages hypoxia. Hypoxia delays wound healing by increasing inflammation and free radical release. Hyperglycemia increases free radical production and advanced glycation end products (AGE) inhibit vascular proliferation. Gap junctions, which are composed of proteins, are expressed in the vasculature. Hyperglycemia prevents gap junction formation and encourages TNF-α production, which synergistically inhibits angiogenesis; these factors impairing vascularization and contributing to protracted wound healing.29
Immune responses
Suppression of innate immunity, seen in diabetics, causes predisposition to infection. AGE products decrease the neutrophil and monocyte count in circulation. Inactivation of these cells can account for immune suppression. A decrease in blood glucose would remedy this. Oral epithelial cells produce antimicrobial proteins like beta-defensins, cathelicidin and psoraisin. These peptides decrease as levels of blood glucose rises, impairing wound healing. Saliva contains antimicrobials and has buffering capacity. In diabetics with hyposalivation, healing is slower. Inflammatory cytokines, interleukin-6 and TNF-α are seen in obese subjects and Type II diabetics. TNF-α inhibits the inflammation cascade; the first stage of healing.29
Growth factors
Many growth factors at the wound promote healing, such as epidermal growth factor (EGF), insulin-like growth factor (IGF) or nerve growth factor (NGF). Lower levels of these growth factors, as seen in diabetics, extend healing time. In foot ulcers of diabetic patients, decreased expression of IGF was seen. NGF was also low on the skin of diabetic patients and laboratory rats. NGF encourages proliferation of keratinocytes and endothelial cells. The reduction in all these growth factors inevitably delays oral wound healing.29
Psychological stresses
Patients with chronic conditions are often under psychological stress and this is no different in diabetics. Mechanisms have been postulated explaining psychological stress and protracted healing. Suppression of the hypothalamus-pituitary-adrenal axis through stress predisposes patients to infection and delayed healing. Prolonged stress leads to long-term alteration of emotional states, which negatively affect both immune and endocrine functioning.29 Poor mental wellbeing leads to unhealthy lifestyles such as smoking/alcohol. Unhealthy lifestyles undesirably affect healing at a local level. Poor lifestyle habits affect glycemic control, which further worsens the situation.
Conclusion
Diabetes, although a common disease, has a complex multifactorial aetiology and has a profound systemic effect on the body. Diabetes also has grave oral implications. In fact, the diagnosis of certain oral conditions can even precede the diagnosis of diabetes mellitus. As such, as front line clinicians, dentists must remain ever vigilant of its signs and symptoms.