DiAngelis AJ, Andreasen JO, Ebeleseder KA, Kenny DJ, Trope M, Sigurdsson A International Association of Dental Traumatolology guidelines for the management of dental injuries: 1. Fractures and luxations of permanent teeth. Dent Traumatol. 2012; 28:2-12
Glendor U. Epidemiology of traumatic dental injuries – a 12 year review of the literature. Dent Traumatol. 2008; 24:603-611
Andreasen JO, Andreasen FM.Oxford: Blackwell Munkgaard; 2000
Cvek M. A clinical report on partial pulpotomy and capping with calcium hydroxide in permanent incisors with complicated crown fractures. J Endod. 1978; 4:232-237
Murchison DF, Burke FJT, Worthington RB. Incisal edge reattachment: indications for use and clinical technique. Br Dent J. 1999; 186:614-619
Andreasen FM, Noren JG, Andreasen JO, Engelhardtsen S, Lindh-Stromberg U. Long term survival of fragment bonding in the treatment of fractured crowns: a multicenter clinical study. Quintessence Int. 1995; 26:669-681
Mazumdar P, Maiti A, Maity I, Das UK. A case report on management of complex crown fracture by non surgical endodontic treatment and fragment reattachment – a novel approach. Int J Adv Res. 2016; 4:1370-1375
Traumatic injuries to teeth are commonplace and can result in significant morbidity and aesthetic disfigurement. If the patient has not reached maturity at the time of the injury, efforts should be made to delay the provision of definitive indirect restorations until adulthood and the orofacial development is completed.
CPD/Clinical Relevance: This paper describes a trauma injury and how definitive indirect treatment was delayed for almost ten years, by employing adhesive techniques and retaining the fractured crown of the patient by re-attachment.
Article
Five per cent of all injuries for which treatment is sought are related to dental trauma in children and young adults.1 In a 12-year literature review, undertaken in 2008, it was shown that 25% of all school children experience dental trauma and that 33% of adults have suffered damage to the permanent dentition, the majority of which occurred before reaching 19 years old.2 In the primary dentition, the most common injuries are luxation injuries, whereas crown fractures predominate in the permanent dentition.1
This paper describes the treatment and care offered, over a period of almost ten years, to a 16-year-old young man who suffered a traumatic dental injury to his upper left central incisor. A minimally invasive approach to dental treatment is just as appropriate when dealing with trauma cases as when dealing with ‘routine’ restorative dental care and the approach taken in this case was to minimize the amount of initial treatment needed and to preserve as much natural tissue as possible.
Case report
A phone call was received, one Sunday morning in January 2007, from a patient whose son, also a patient, had run into a tree late the previous evening. He was aware that he had damaged and possibly broken a front tooth and lacerated his upper lip.
The surgery was opened and, on arrival, clinical examination indicated that he had sustained minor soft tissue damage to the upper lip (Figure 1) and that he had sustained a traumatic injury to his upper left central incisor (Figure 2).
Figure 1. Soft tissue damage on presentation.Figure 2. Fractured UL1 on presentation.
An enquiry was made as to whether he had lost consciousness and if any tooth fragments had been lost, the answer to both questions being ‘No’.
In all dental trauma cases a thorough history needs to be undertaken which will include:3
When it happened;
Where it happened;
What happened;
Any loss of consciousness;
Any emergency treatment;
Medical history;
Disturbances in the occlusion.
In this case, the injury was sustained late the previous evening when he accidentally ran into a tree. He was not rendered unconscious and his medical history was uncomplicated. He was unaware of his tetanus status and was advised to seek the advice of his GMP as soon as possible.
An extra-oral examination was undertaken. This excluded any foreign bodies in the contusions and no evidence of any facial bone fractures. The patient was unable to achieve his normal intercuspal position due to slight palatal displacement of the tooth. A complete oblique crown fracture was evident, with the fractured portion only attached by the palatal gingival tissues. Local anaesthetic was administered and a long cone periapical radiograph taken. No root fractures were seen (Figure 3). The patient was advised that the fractured portion of the tooth would have to be removed, but that it might be possible to re-attach it using adhesive technology, although no guarantee could be given. He was also advised that root canal treatment might be necessary if there was pulpal involvement.
Figure 3. Long cone PA radiograph taken on presentation. No root damage noted but possibly some minor evidence of subluxation apically.
Consent to treatment was obtained and the fractured portion was removed. The palatal fracture line was found to be approximately 3 mm subgingival on the palatal aspect, and a large pulpal exposure was noted. The exposure was deemed too large for a Cvek (partial) pulpotomy,4 along with the fact that the injury was sustained the previous day, suggesting that there would have been significant bacterial contamination of the pulp complex. The patient was advised that the tooth would have to be devitalized and root treated.
The tooth was isolated and the pulp was extirpated, followed by thorough irrigation with sodium hypochlorite and water. The canal was dried and dressed with non-setting calcium hydroxide and sealed with a plug of white gutta-percha (GP), making sure that the GP would not prevent seating of the fractured portion of the tooth.
The intention was to re-attach the broken portion of the tooth. Accordingly, an access cavity for the continuation of the endodontic treatment was cut into the broken tooth fragment prior to bonding it back into place (Figure 4). It was considered that this would minimize the potential disruption to the bond once the fragment was re-attached and the endodontic treatment continued.
Figure 4. Fractured portion with a palatal access cavity prepared prior to re-attachment.
Both portions of the tooth were etched with 35% phosphoric acid. Optibond™ FL and flowable composite were used to re-attach the broken portion (Figures 5 and 6).
Figure 5. Palatal view of the re-attached portion of the tooth.Figure 6. Labial view of the re-attached portion of the tooth.
Endodontic treatment was completed a week later (Figure 7). Access was achieved through the thin layer of flowable composite sealing the access cavity made prior to recementation of the broken tooth fragment the previous week. It was felt that this was likely to cause less stress on the bonded fragment of tooth. (This is a personal view and not based on any known evidence).
Figure 7. Completed endodontic treatment of UL1 one week after the accident
The patient was advised that, due to the configuration of the fracture, the broken fragment may debond and that the subgingival nature of the palatal fracture line made moisture control difficult and potentially compromised.
At the six month review, the repair had remained in place, the tooth was a good colour and was totally symptom-free (Figure 8).
Figure 8. Six month review after re-attachment.
After 18 months it was noted that the tooth was beginning to discolour slightly and the fracture line was a little more apparent. However, the tooth remained symptom-free and there was no indication for any further intervention (Figures 9 and 10).
Figure 9. Eighteen month review after re-attachment.Figure 10. Close up of the UL1 at 18 month follow-up.
As may often be the case when young people reach adulthood, the patient's attendance became more sporadic when he ‘disappeared’ off to University. Upon completion of his studies, he called requesting an appointment as he was no longer happy with the appearance of the tooth that he had fractured in the index accident (Figure 11).
Figure 11. Nine and a half years after re-attachment.
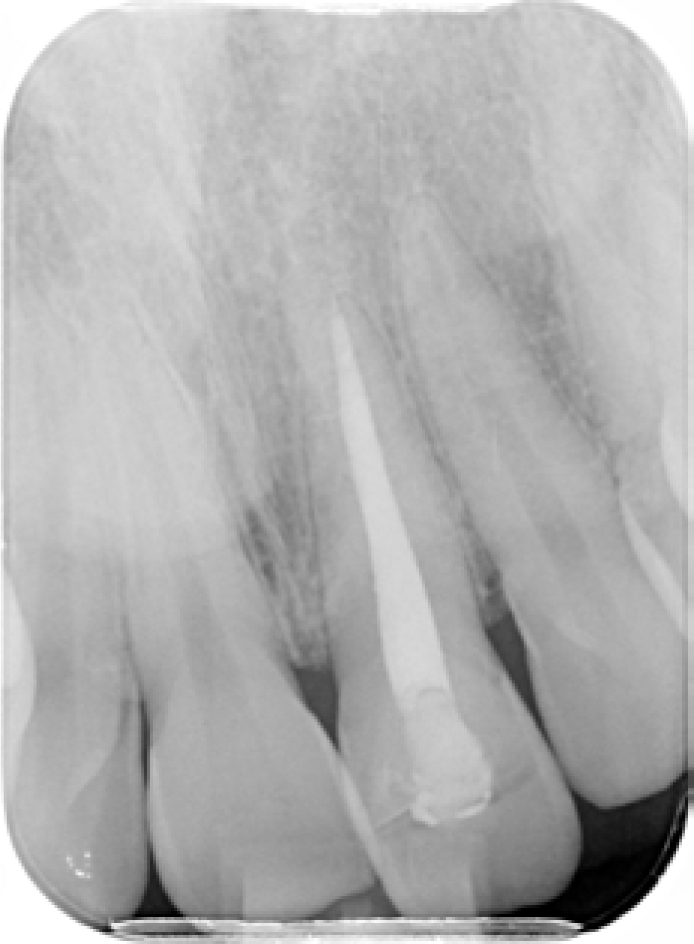
After nine and a half years, the discoloration of the tooth was much more apparent, as was the fracture line. Concern was expressed about potential microleakage which could compromise the endodontic status of the tooth. A periapical radiograph was taken to assess the periapical status of the tooth and this was shown to be healthy (Figure 12).
Figure 12. Long cone PA radiograph nine and a half years after endodontic treatment.
Various treatment options were discussed and, in consultation with his father, the patient decided that he would like to go ahead with a ceramic crown.
Upon removal of the fractured portion, a decision was made to bond a tooth-coloured fibre post into the root and to build-up a dentine-bonded composite core.
Under local anaesthesia, gingival electrosurgery was undertaken on the palatal aspect of the tooth in order to make the fracture line supragingival (Figure 13). The margin was only just supra-crestal, and the author had some concern about encroaching upon the biologic width. However, the patient did not want to undergo conventional crown lengthening with bone removal and so the electrosurgery was considered a good compromise, especially as he had a relatively thick gingival biotype. A provisional crown was made from a putty index taken prior to removal of the fractured piece of tooth, adjusted and polished (Figure 14).
Figure 13. Palatal view of the UL1 following removal of the fractured portion and gingival electrosurgery to expose palatal fracture line.Figure 14. Provisional crown after core build-up.
After a period of healing, the provisional crown was removed and the preparation refined for an IPS e.max (Ivoclar Vivadent) crown.
Unfortunately, there was a misunderstanding with the laboratory and they presumed the author wanted to bring the tooth into alignment with the UR1. However, it was the UR1 which was retroclined and the UL1 which was in the correct place. Consequently, considering there wasn't enough room for the ceramic, a reduction coping was produced (Figure 15) with a request that more tooth substance be removed in order to fit the new crown which had been made in alignment with the UR1. It was considered completely inappropriate to remove further tooth tissue and therefore a new impression was taken with instructions to make a new crown in the original position. If, in future, the patient had wanted to improve the alignment of his teeth, then orthodontic treatment might have been feasible, or a composite or ceramic labial veneer could have been constructed, in order to bring the labial face of the UR1 into alignment with the crown.
Figure 15. Lab made reduction coping in place demonstrating the extent to which it would have been necessary to remove further tissue to seat the definitive crown. Not undertaken.
The new crown was made and cemented with G-Cem LinkForce™ resin cement (Figures 16 and 17).
Figure 16. Labial view of the completed restoration of the UL1.Figure 17. On completion of the definitive restoration almost 10 years after the original accident.
Discussion
This case illustrates how, by re-attaching the broken portion of the tooth, the patient was able to reach maturity before further intervention was necessary. This allowed complete maturation of the gingival tissues before making an indirect restoration, and also deferred more invasive treatment until he was older, more able to accept dental treatment and less likely to experience further trauma.
Whilst there are a number of papers describing the technique of crown re-attachment,5 few papers describe the potential for success of the procedure which has been described. However, the results from a multicentre trial by Andreasen and colleagues indicates a survival rate of 25% after 10 years, with the rider that most failures came from a new traumatic incident.6 The authors added that, while the success rate that they reported was low in comparison to survival rates of resin composite restorations, fragment loss was an absolute, while restorations may discolour, suffer substance loss or caries and be unsatisfactory over a prolonged period. In addition, it has been considered that rebonding of a lost incisor fragment provides a positive psychological response in the patient, although patient understanding of the limitations of the treatment is important.7 Having both bonded fractured tooth fragments and undertaken large composite build-ups when fragments have been lost, this author finds the rebonding of the tooth fragment both quicker and easier. In a laboratory experiment carried out by Farik and co-workers on 200 extracted sheep's teeth, which they transversely fractured using two microtomes, the results indicated that the strength of intact teeth was not significantly different from teeth rebonded using three bonding agents, but was significantly greater than teeth rebonded using five other dentine-bonding agents, indicating a variability in the effectiveness of different bonding agents.8 Nevertheless, it may be considered that, despite the lack of strong clinical evidence, the technique described is one that is worth attempting, as in this case, the delay in crowning the tooth bought time and allowed the patient's mouth to mature.
Readers are also directed to the paper by Djemal et al,9 recently published in Dental Update, for a further description of the Cvek pulpotomy technique and a further case of fragment re-attachment.
Finally, with the benefit of hindsight, there are a few things which perhaps this author may have changed:
In spite of the exposure and the potential leakage prior to treatment, it might have been worth trying a Cvek pulpotomy. If this was unsuccessful, endodontic treatment could have been carried out later.
It might have also worth placing a composite ‘bandage’ over the fracture line to give the fractured portion a little more ‘support’.
A conventional crown lengthening procedure, including some bone removal on the palatal aspect, would have also prevented the possible problems of encroaching upon the biologic width.
The tooth could have been extruded orthodontically, in effect making the fracture line supragingival.