Hex N, Bartlett C, Wright D, Taylor M, Varley D. Estimating the current and future costs of Type 1 and Type 2 diabetes in the UK, including direct health costs and indirect societal and productivity costs. Diabet Med. 2012; 29:855-862
Tuomi T, Santoro N, Caprio S, Cai M, Weng J, Groop L The many faces of diabetes: a disease with increasing heterogeneity. Lancet. 2014; 383:1084-1094
Rewers A, Chase HP, Mackenzie T, Walravens P, Roback M, Rewers M Predictors of acute complications in children with type 1 diabetes. JAMA. 2002; 287
Roche EF, Menon A, Gill D, Hoey H. Clinical presentation of type 1 diabetes. Pediatr Diabetes. 2005; 6:75-78
Gianani R, Campbell-Thompson M, Sarkar SA, Wasserfall C, Pugliese A, Solis JM Dimorphic histopathology of long-standing childhood-onset diabetes. Diabetologia. 2010; 53:690-698
Defronza RA. Pathogenesis of Type 2 diabetes: metabolic and molecular implications for identifying diabetes genes. Diabet Rev. 1997; 5:177-269
Ley SH, Hamdy O, Mohan V, Hu FB. Prevention and management of type 2 diabetes: dietary components and nutritional strategies. Lancet. 2014; 383:1999-2007
Forouzanfar MH, Alexander L, Anderson HR, Bachman VF, Biryukov S Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015; 386:2287-2323
Willi C, Bodenmann P, Ghali WA, Faris PD, Cornuz J. Active smoking and the risk of type 2 diabetes: a systematic review and meta-analysis. JAMA. 2007; 298:2654-2664
Buckley BS, Harreiter J, Damm P, Corcoy R, Chico A, Simmons D Gestational diabetes mellitus in Europe: prevalence, current screening practice and barriers to screening. A review. Diabet Med. 2012; 29:844-854
Bellamy L, Casas J-P, Hingorani AD, Williams D. Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysis. Lancet. 2009; 373:1773-1779
Kühl C, Hornnes PJ, Andersen O. Etiology and pathophysiology of gestational diabetes mellitus. Diabetes. 1985; 34:66-70
Poulakos P, Mintziori G, Tsirou E, Taousani E, Savvaki D, Harizopoulou V Comments on gestational diabetes mellitus: from pathophysiology to clinical practice. Hormones. 2015; 14:335-344
Nathan D. Diabetes Control and Complications Trial (DCCT): results of feasibility study. The DCCT Research Group. Diabetes Care. 10:1-19
Epidemiology of Diabetes Interventions and Complications (EDIC). Design, implementation, and preliminary results of a long-term follow-up of the Diabetes Control and Complications Trial cohort. Diabetes Care. 1999; 22:99-111
Jacobs J, Sena M, Fox N. The cost of hospitalization for the late complications of diabetes in the United States. Diabet Med. 1991; 8:S23-29
Chawla A, Chawla R, Jaggi S. Microvasular and macrovascular complications in diabetes mellitus: distinct or continuum?. Indian J Endocrinol Metab. 2016; 20:546-551
Gärtner V, Eigentler TK. Pathogenesis of diabetic macro- and microangiopathy. Clin Nephrol. 2008; 70:1-9
Dahl-Jørgensen K. Diabetic microangiopathy. Acta Paediatr Suppl. 1998; 425:31-34
Fowler MJ. Microvascular and macrovascular complications of diabetes. Clin Diabetes. 2008; 26:77-82
Goldney RD, Phillips PJ, Fisher LJ, Wilson DH. Diabetes, depression, and quality of life. Diabetes Care. 2004; 27:1066-1070
Manouchehr-Pour M, Spagnuolo PJ, Rodman HM, Bissada NF. Comparison of neutrophil chemotactic response in diabetic patients with mild and severe periodontal disease. J Periodontol. 1981; 52:410-415
Mowat AG, Baum J. Chemotaxis of polymorphonuclear leukocytes from patients with diabetes mellitus. N Engl J Med. 1971; 284:621-627
Geerlings SE, Hoepelman AI. Immune dysfunction in patients with diabetes mellitus (DM). FEMS Immunol Med Microbiol. 1999; 26:259-265
Delamaire M, Maugendre D, Moreno M, Le Goff M-C, Allannic H, Genetet B. Impaired leucocyte functions in diabetic patients. Diabet Med. 1997; 14:29-34
Iacopino AM. Periodontitis and diabetes interrelationships: role of inflammation. Ann Periodontol. 2001; 6:125-137
Bender IB, Bender AB, Yoon J, Tennenberg S, Finkenauer R, Dwivedi A Diabetes mellitus and the dental pulp. J Endod. 2003; 29:383-389
Lin BP-J, Taylor GW, Allen DJ, Ship JA. Dental caries in older adults with diabetes mellitus. Spec Care Dent. 1999; 19:8-14
Hintao J, Teanpaisan R, Chongsuvivatwong V, Dahlen G, Rattarasarn C. Root surface and coronal caries in adults with type 2 diabetes mellitus. Community Dent Oral Epidemiol. 2007; 35:302-309
Leone CW, Oppenheim FG. Physical and chemical aspects of saliva as indicators of risk for dental caries in humans. J Dent Educ. 2001; 65:1054-1062
Ben-Aryeh H, Cohen M, Kanter Y, Szargel R, Laufer D. Salivary composition in diabetic patients. J Diabet Complications. 1988; 2:96-99
Sandberg GE, Sundberg HE, Fjellstrom CA, Wikblad KF. Type 2 diabetes and oral health: a comparison between diabetic and non-diabetic subjects. Diabetes Res Clin Pract. 2000; 50:27-34
Khader YS, Dauod AS, El-Qaderi SS, Alkafajei A, Batayha WQ. Periodontal status of diabetics compared with nondiabetics: a meta-analysis. J Diabetes Complications. 2006; 20:59-68
Salvi GE, Carollo-Bittel B, Lang NP. Effects of diabetes mellitus on periodontal and peri-implant conditions: update on associations and risks. J Clin Periodontol. 2008; 35:398-409
Taylor GW, Burt BA, Becker MP, Genco RJ, Shlossman M. Glycemic control and alveolar bone loss progression in type 2 diabetes. Ann Periodontol. 1998; 3:30-39
Mealey BL, Rose LF. Diabetes mellitus and inflammatory periodontal diseases. Curr Opin Endocrinol Diabetes Obes. 2008; 15:135-141
Stanko P, Izakovicova Holla L. Bidirectional association between diabetes mellitus and inflammatory periodontal disease. A review. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2014; 158:35-38
Darby IA, Bisucci T, Hewitson TD, MacLellan DG. Apoptosis is increased in a model of diabetes-impaired wound healing in genetically diabetic mice. Int J Biochem Cell Biol. 1997; 29:191-200
Nassar H, Kantarci A, Van Dyke TE. Diabetic periodontitis: a model for activated innate immunity and impaired resolution of inflammation. Periodontol 2000. 2007; 43:233-244
Taylor JJ, Preshaw PM, Lalla E. A review of the evidence for pathogenic mechanisms that may link periodontitis and diabetes. J Clin Periodontol. 2013; 40:S113-S134
DeWitt GV, Cobb CM, Killoy WJ. The acute periodontal abscess: microbial penetration of the soft tissue wall. Int J Periodontics Restorative Dent. 1985; 5:38-51
Christgau M, Palitzsch KD, Schmalz G, Kreiner U, Frenzel S. Healing response to non-surgical periodontal therapy in patients with diabetes mellitus: clinical, microbiological, and immunologic results. J Clin Periodontol. 1998; 25:112-124
Santos VR, Lima JA, De Mendonça AC, Braz Maximo MB, Faveri M, Duarte PM. Effectiveness of full-mouth and partial-mouth scaling and root planing in treating chronic periodontitis in subjects with type 2 diabetes. J Periodontol. 2009; 80:1237-1245
Segura-Egea JJ, Castellanos-Cosano L, Machuca G, López-López J, Martín-González J, Velasco-Ortega E Diabetes mellitus, periapical inflammation and endodontic treatment outcome. Med Oral Patol Oral Cir Bucal. 2012; 17:356-361
Tenovuo J, Alanen P, Larjava H, Viikari J, Lehtonen OP. Oral health of patients with insulin-dependent diabetes mellitus. Scand J Dent Res. 1986; 94:338-346
Bender IB, Seltzer S, Freedland J. The relationship of systemic diseases to endodontic failures and treatment procedures. Oral Surg Oral Med Oral Pathol. 1963; 16:1102-1115
Tennenberg SD, Finkenauer R, Dwivedi A. Absence of lipopolysaccharide-induced inhibition of neutrophil apoptosis in patients with diabetes. Arch Surg. 1999; 134:1229-1233
Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J. 2006; 39:921-930
Brownlee M. The pathobiology of diabetic complications. Diabetes. 2005; 54:1615-1625
Forslund JM, Archdeacon MT. The pathobiology of diabetes mellitus in bone metabolism, fracture healing, and complications. Am J Orthop (Belle Mead NJ). 2015; 44:453-457
Caimi G, Montana M, Citarrella R, Porretto F, Catania A, Lo Presti R. Polymorphonuclear leukocyte integrin profile in diabetes mellitus. Clin Hemorheol Microcirc. 2002; 27:83-89
Wilgus TA, Roy S, McDaniel JC. Neutrophils and wound repair: positive actions and negative reactions. Adv Wound Care. 2013; 2:379-388
Miao M, Niu Y, Xie T, Yuan B, Qing C, Lu S. Diabetes-impaired wound healing and altered macrophage activation: a possible pathophysiologic correlation. Wound Repair Regen. 2012; 20:203-213
Liu BF, Miyata S, Kojima H, Uriuhara A, Kusunoki H, Suzuki K Low phagocytic activity of resident peritoneal macrophages in diabetic mice: relevance to the formation of advanced glycation end products. Diabetes. 1999; 48:2074-2082
Gary Sibbald R, Woo KY. The biology of chronic foot ulcers in persons with diabetes. Diabetes Metab Res Rev. 2008; 24:S25-S30
Botusan IR, Sunkari VG, Savu O, Catrina AI, Grünler J, Lindberg S Stabilization of HIF-1alpha is critical to improve wound healing in diabetic mice. Proc Natl Acad Sci U S A. 2008; 105:19426-19431
Rodriguez PG, Felix FN, Woodley DT, Shim EK. The role of oxygen in wound healing: a review of the literature. Dermatologic Surg. 2008; 34:1159-1169
Mehta SK, Breitbart EA, Berberian WS, Liporace FA, Lin SS Bone and wound healing in the diabetic patient. Foot Ankle Clin. 2010; 15:411-437
Vincent AM, Russell JW, Low P, Feldman EL. Oxidative stress in the pathogenesis of diabetic neuropathy. Endocr Rev. 2004; 25:612-628
Vlassara H, Palace MR. Diabetes and advanced glycation endproducts. J Intern Med. 2002; 251:87-101
Fong Y, Edelstein D, Wang EA, Brownlee M. Inhibition of matrix-induced bone differentiation by advanced glycation end-products in rats. Diabetologia. 1993; 36:802-807
Zhang S, Wang S, Wei H, Li D, Song Y. Post-extraction socket changes in diabetic patients – a retrospective study. Int J Clin Exp Med. 2016; 9:14077-14086
Fiorellini JP, Chen PK, Nevins M, Nevins ML. A retrospective study of dental implants in diabetic patients. Int J Periodontics Restorative Dent. 2000; 20:366-373
Renton T, Woolcombe S, Taylor T, Hill CM. Oral surgery: part 1. Introduction and the management of the medically compromised patient. BDJ. 2013; 215:213-223
Naujokat H, Kunzendorf B, Wiltfang J. Dental implants and diabetes mellitus – a systematic review. Int J Implant Dent. 2017; 2
Hill LV, Tan MH, Pereira LH, Embil JA. Association of oral candidiasis with diabetic control. J Clin Pathol. 1989; 42:502-505
Branco-de-Almeida LS, Alves CMC, Lopes FF, Pereira A, de FV, Guerra RNM, Pereira ALA. Salivary IgA and periodontal treatment needs in diabetic patients. Braz Oral Res. 2011; 25:550-555
Moore PA, Guggenheimer J, Orchard T. Burning mouth syndrome and peripheral neuropathy in patients with type 1 diabetes mellitus. J Diabetes Complications. 2007; 21:397-402
Diabetes is a chronic disease currently known to affect at least 5% of the UK's population and is expected to continue to increase in prevalence. The disease has significant effects on the immune system and increases inflammatory responses.
Diabetes affects various parts of everyday general dental practice including: the altered host-pathogen relationship on periodontal disease and its management; the dental pulp and, therefore, endodontics; and both wound and bony healing, thereby impacting surgical procedures.
Educating diabetes patients about the effects of the disease and associated risks to their treatment is important in patient management.
CPD/Clinical Relevance: Diabetes is a prevalent chronic disease in the UK and can adversely affect oral health and dental treatment outcome.
Article
Vinson Yeung Joht Chandan
The first World Health Organization global report on diabetes released this year indicated that 422 million adults worldwide were living with diabetes in 2014.1 In 2011, there were 2.9 million people diagnosed with diabetes in the UK. This equated to a cost to the NHS of approximately £24bn to manage diabetes. As it is estimated that, by 2025, five million people will have diabetes in the UK,2 the bill to the NHS will increase still further.3
Diabetes mellitus is a chronic, non-communicable disease and arises from either lack of insulin produced by the pancreas (Type 1 diabetes), or when the body cannot effectively utilize the insulin produced (Type 2 diabetes). The third most common type is Gestational Diabetes Mellitus (GDM), where the physiological processes associated with pregnancy can increase the risk of insulin resistance.
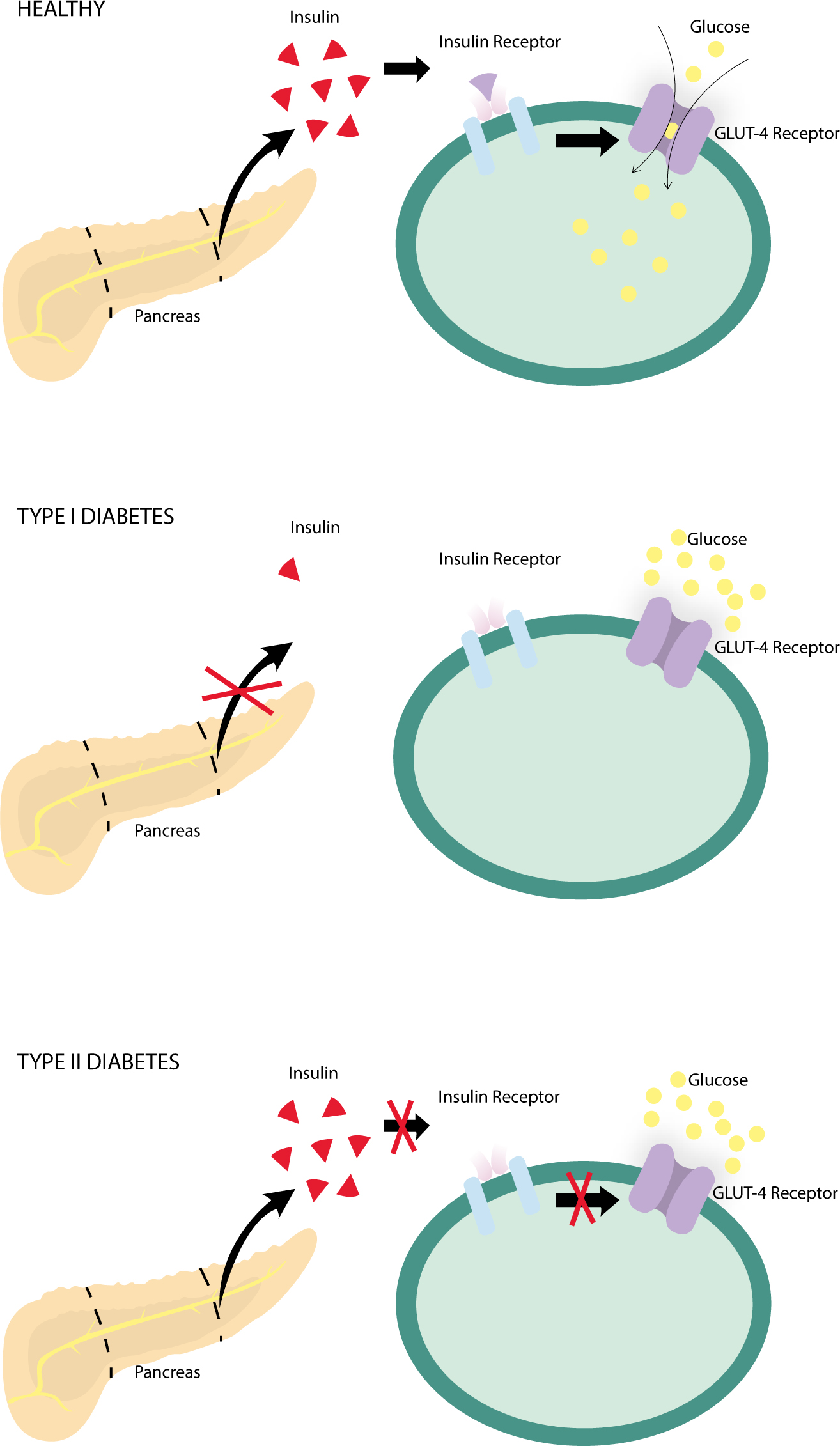
Insulin is a hormone produced by the pancreas allowing cells to store glucose from the bloodstream for future use. Glucose is utilized by cells as an energy source and is the preferred source of the energy by the brain. If insulin cannot be produced, or insulin receptors on cell surfaces become desensitized to the effect of the hormone, then cellular glucose storage becomes inadequate (Figure 1). This results in too little glucose being stored in cells for periods of fasting, or excess glucose not being stored during mealtimes. This can lead to hypoglycaemic episodes, with both short- and long-term complications.
Figure 1. Diagram demonstrating the role of insulin and its receptors.
It used to be assumed that Type 1 and Type 2 diabetes were, respectively, illnesses of the extremes of age, however, recent work has established diabetes as a far more heterogeneous disease than the current classification system assumes.4
Aetiology and presentation
Although the exact cause of diabetes is unknown, there are defined risk factors, depending on the type of diabetes, which can, in different combinations, lead to development of the condition.
Type 1 diabetes (previously known as insulin-dependent, juvenile or childhood-onset diabetes) is characterized by deficient insulin production in the body. Therefore, patients with the condition must administer insulin daily to regulate blood glucose (glycaemic) levels. Missed doses can lead to severe complications and ultimately death.5 Polyuria, polydipsia, polyphagia, along with hypoglycaemic episodes are the most common presentations of the disease.6 Most cases of Type 1 diabetes arise as part of an immune or auto-immune mediated disorder, however, not all Type 1 patients fall into this category and they can be broadly subdivided into Type 1A (autoimmune) and Type 1B (idiopathic) diabetes.7
In comparison, Type 2 diabetes accounts for over 85% of diabetes patients in the UK.2 Type 2 (previously known as non-insulin dependent or adult onset diabetes) results from the body's ineffective utilization of insulin. Symptoms may be similar to those of Type 1 diabetes, although the degree of insulin resistance varies in Type 2 diabetics, depending upon disease progression. This means that cases may progress undiagnosed for several years, accounting for around 1 in 16 people in the UK being currently undiagnosed.8
Genetics play a significant role in the development of Type 2 diabetes – some individuals inherit genes making tissues resistant to insulin.9 Combining genetic along with environmental and metabolic risk factors creates a complex picture of overall diabetic risk. Excess body fat due to dietary factors10 and physical inactivity are the biggest risk factors for diabetes development in any age group.11 Although it is common knowledge that higher waist circumference and BMI are associated with an increased risk of diabetes, practitioners should be aware that this varies according to ethnic group. Apart from diet and exercise, smoking also increases the risk of Type 2 diabetes, with the highest risk among heavy smokers.12
Gestational diabetes is a condition that occurs temporarily during pregnancy. It is a condition affecting between 2–6% of all pregnancies.13 Even though the condition is temporary, it can lead to an increased risk in the development of Type 2 diabetes.14 The pathophysiology of GDM is similar to Type 2 diabetes as both conditions arise from insulin resistance.15 The exact cause is not yet known, however, there is some indication as to the aetiology. During pregnancy, insulin resistance appears to be increased due to the production of placental hormones from the baby that antagonize the mother's usual insulin action.16 Risk factors for development appear to be age, family history of diabetes, GDM during previous pregnancy, excessive weight gain during pregnancy or a history of stillbirth or giving birth to children with congenital abnormalities.1
Complications of diabetes
The Diabetes Control and Complication Trial (DCCT)17 and subsequent Epidemiology of Diabetes Interventions and Complications (EDIC) Trial18 have identified short- and long-term complications of diabetes. Complications can be microvascular (small vessels), macrovascular (large vessels) and psychological. Microvascular complications include retinopathy, nephropathy and neuropathy, which usually occur after 10–15 years from diagnosis.19 Meticulous glucose intake control can reduce the risk of developing these conditions by 62%, 56% and 60%, respectively.17
The pathogenesis behind the risk to micro-vessels (ie in the eye, kidney and surrounding the nerves) due to the micro-angiopathic state present in diabetes is complex. High blood glucose levels in diabetes induce changes in the microvasculature, affecting the capillary basement membrane.20 Endothelial cells take in more glucose than normal, increasing surface glycoprotein formation and, therefore, increasing basement membrane thickness (causing glomerulosclerosis, arteriosclerosis and interstitial fibrosis hyperglycemia).21 This affects vessel function by increasing their risk of bleeding, leaking of proteins and reducing flow of blood carrying oxygen and nutrients.22
Macrovascular disease progression stems from the link between atherosclerosis and diabetes. Atherosclerosis develops as a response to chronic inflammation and injury to arterial walls. In response to endothelial dysfunction and injury, lipids and lipoproteins accumulate in the endothelial walls, causing a narrowing of blood vessel lumen23 and ischaemia of the tissues supplied by those vessels. The chronic inflammatory state arising from diabetes can lead to atheroma formation; there is evidence showing increased platelet adhesion and hyper-coagulability in Type 2 diabetes. Alongside these physiological complications, a diagnosis of diabetes can place patients at risk of depression and is often underdiagnosed in this population.24
Diabetes and the immune system
Diabetes is known to have significant effects on the body's immune response to infection, leading to changes in inflammatory pathways. The function of neutrophils, monocytes and macrophages are altered by the disease.25
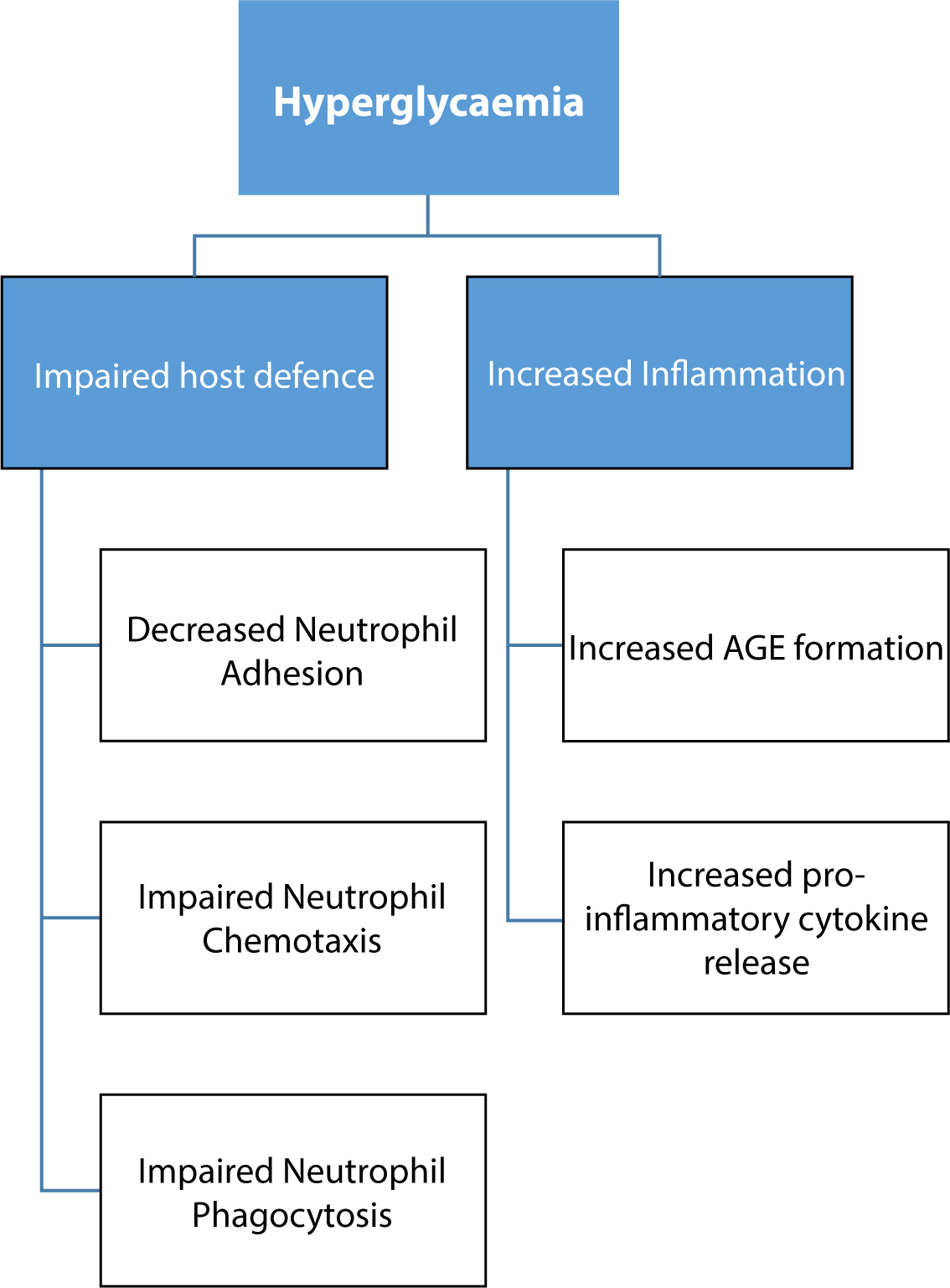
Neutrophils act as one of the first defence barriers against bacterial infection by phagocytosing and subsequently killing bacteria. However, hyperglycaemia of diabetes causes changes in neutrophil function so that the phagocytosis process is impeded26 and the body's ability to eliminate bacteria is impaired (Figure 2). The impediment in patients with diabetes occurs due to a state of poor glucose utilization for the energy dependent process of chemotaxis, where neutrophils are drawn to infective agents.27 Secondly, studies have shown neutrophils in hyperglycaemic states demonstrate abnormalities in adherence, and production of adhesion molecules and free radicals affecting their ability to phagocytose bacterial cells.28,29
Figure 2. A brief summary of the effects of hyperglycaemia on host tissue defence.
Other inflammatory responses are also up-regulated in people with diabetes. Diabetes causes up-regulation of pro-inflammatory cytokines from monocytes and neutrophils and down-regulation of growth factors from macrophages.30 This can lead to chronic inflammation due to the up-regulation of pro-inflammatory markers, progressive tissue damage and diminished ability to repair tissue (discussed later) due to the altered macrophages and the cumulation of the effect of Advanced Glycation End-products (AGEs), which is irreversible. AGEs form from the non-enzymatic binding of glucose to proteins, which can alter protein structure and function, including cross-linkage of collagen to the basement membrane in connective tissue, which may impair and delay healing. AGEs also bind to a complementing receptor on immune cells known as RAGE (Receptors for AGEs) and co-ordinate a pro-inflammatory sequence, as well as oxygen radical and cytokine release. This further exacerbates the inflammatory response.
Diabetes also affects the immune system via the impairment of movement of immune components. As mentioned above, diabetes is associated with increased artherosclerotic plaque in blood vessels significantly impeding flow and impaired leukocytic response due to reduced flow and the thickened basement membrane.31 Dental pulp and blood vessels contributing to the teeth are already limited due to capillary size and therefore the response is even more profound in the oral cavity (Figure 2).31
How does diabetes influence dentistry in everyday dental practice?
Conservative dentistry
Given the need for a diet restricted in refined carbohydrates and other cariogenic foods, it would be rational to expect a lower incidence of caries in diabetics. However, Type II diabetic patients were found to have an increased prevalence of active caries32 and root surface caries33 when compared to non-diabetics. This may be attributed to the reduced salivary flow reported in diabetes patients from the disturbed glycaemic control,34 reducing remineralization of enamel being demineralized by acidic insult from cariogenic bacteria. The higher glucose content in the saliva of diabetes patients35 further contributes to dental caries. Longer duration of diabetes also correlates with increased manifestations of caries.36
Periodontal disease
Result of an altered host-pathogen relationship
Evidence from one meta-analysis found periodontal disease in diabetics to be significantly greater in severity.37 Diabetes patients display deeper probing pocket depths and number of sites bleeding on probing to be significantly more prevalent than the non-diabetes control group.36
According to a recent review, the increased severity of periodontal diseases is associated with hyperglycaemia in poorly controlled diabetes.38 Taylor et al reported that poor glycaemic control increases the risk of and progression/severity of alveolar bone loss;39 these researchers have also suggested a gradient between glycaemia control and risk of progression of bone loss.
Being richly vascularized, the periodontium exhibits complications of the microangiopathy (as previously outlined) associated with the diabetic state. Constant insults from the oral bacterial biofilm induces an immune response whilst diabetes results in altered neutrophil, monocyte and macrophage function.40 The bacteria are persistent in the periodontal pocket due to the impaired adherent, chemotactic and phagocytic functions of neutrophils.41 Prolonged wound healing in diabetes is associated with the increased apoptosis found in diabetes patients,42 and the aforementioned effects of AGEs on connective tissue structure and function.
Increase in inflammation of the periodontium results from modifications in host defences, including elevation of pro-inflammatory mediator levels. There is evidence to suggest a hyperactive response to bacterial antigens,40,43 and up-regulation of TNF-a in response to antigens from P. gingivalis – gram-negative bacteria in diabetic patients.38 These changes also contribute to poor glycaemic control, supporting this bidirectional relationship of diabetes and periodontal disease. Exaggeration of the inflammatory response and resultant increased periodontal destruction could arise from the AGE–RAGE interaction (outlined earlier).44
Periodontal abscesses
Elevation of blood glucose levels may be associated with the formation of periodontal abscesses. Drainage of the pocket may be affected by microflora composition and changes in the host defence system.45 Fibrin secretions can result in closure of the pocket margin to the tooth surface and the pressure of the local suppuration inside a closed pocket may lead to sclerosing and focal abscess formation.
Influence on periodontal treatment
There is evidence to suggest that a similar response to non-surgical periodontal therapy is seen in diabetes patients with good glycaemic control as in non-diabetes healthy control patients.46 In another study, subjects with better controlled diabetes exhibited a greater percentage improvement in clinical attachment loss in comparison to poorly controlled diabetes patients, following periodontal therapy.47
Endodontics
It has been suggested that, like periodontal disease, peri-apical disease may contribute to poorer glycaemic control48 and increases in:
The prevalence of peri-apical lesions;
The size of osteolytic lesions; and
The likelihood of asymptomatic infections having also been associated with diabetes.48
Calcifications appear more likely to be ‘sickle-shaped’ and more likely to be present in the pulp chamber of teeth in diabetes patients. The extent of these calcifications may be such that only remnants of the pulpal vasculature may be observed;49 it has been reported that females with well-established diabetes have more peri-apical lesion associations with root-treated teeth than short-duration diabetic and non-diabetic women.49
The changes in the dental pulp of a diabetes patient has also been associated with a condition referred to as ‘Diabetic Odontalgia’. It was proposed that the impaired pulpal vascular supply may lead to pulpal necrosis and otherwise inexplicable odontalgia.50
It would also be reasonable to suggest that patients with diabetes are at increased risk of pulpal infection and necrosis,51 given that the pulp has an impaired circulation and neutrophil function is also impaired. This altered pulpal environment could also encourage propagation of any present anaerobic bacteria.
Peri-apical lesions create bony defects both the dentist and patient hope will heal once the infective source is controlled through endodontic treatment. However, bony healing may be impaired in diabetes patients, given the microangiopathy associated with the condition.
Whilst the European Society of Endodontology consider a peri-apical lesion persistent four years after endodontic treatment as ‘post treatment disease’,52 reconsideration of the time period of four years may be prudent in patients with diabetes.
Oral surgery
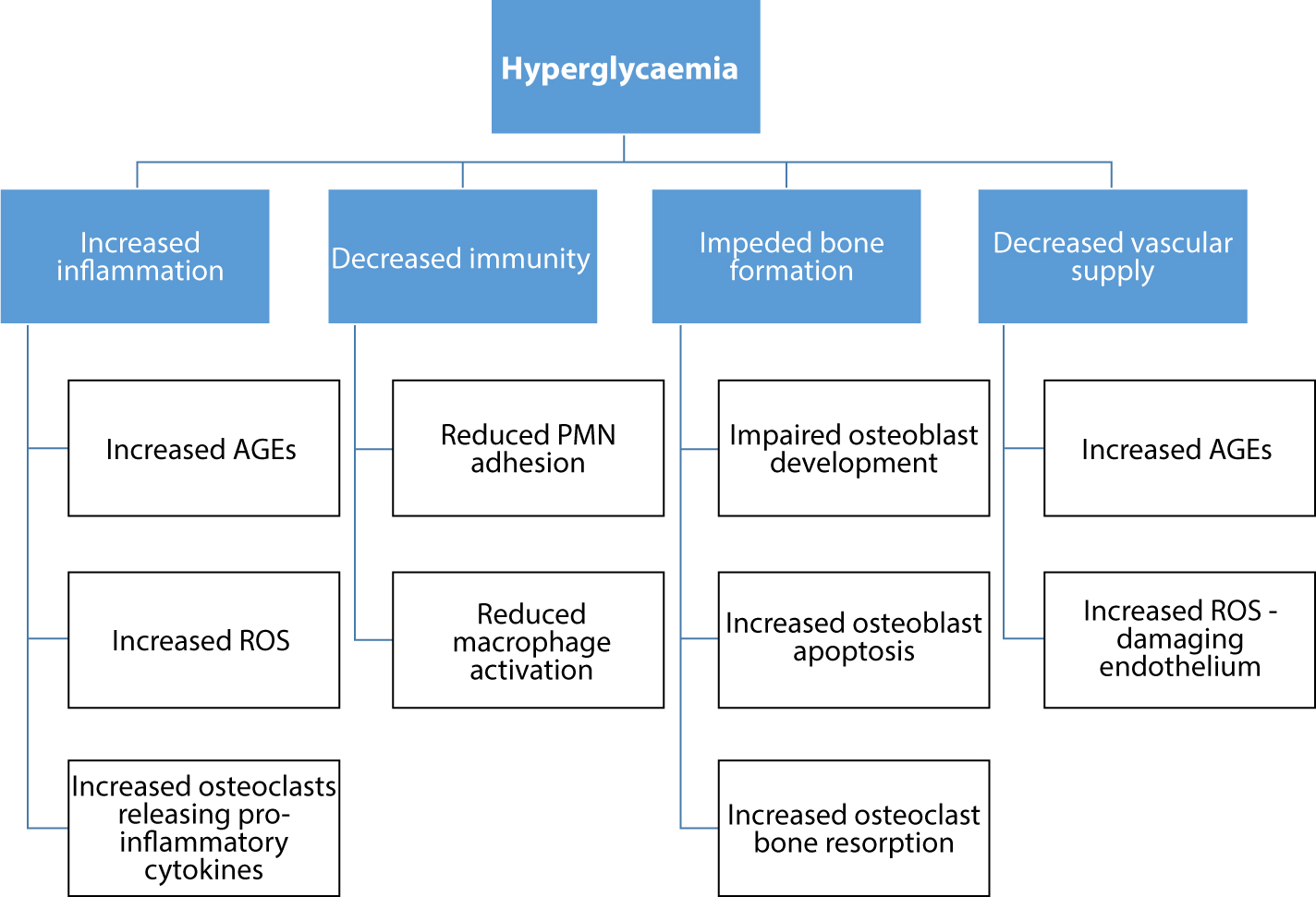
Patients suffering from long-standing hyperglycaemia, which may include those undiagnosed, are at greatest risk from delayed and prolonged wound healing (Figure 3).25 Hyperglycaemia increases levels of AGEs; these molecules bind to circulatory proteins and promote inflammation and alter regulation of growth factors to reduce vascular supply and increase vascular damage.53
Figure 3. Diagram outlining the effects of hyperglycaemia on wound and bony healing
Endothelial cells of blood vessels are affected by glycaemic levels, rather than insulin. Excess blood glucose is converted into sorbitol, creating Reactive Oxygen Species (ROS). This causes further damage to the blood vessels, compounding the damaging effects of AGEs that form in the hyperglycaemic environment.54
These vascular changes compound the changes on the immune system associated with diabetes. The adhesion of PolyMorphoNuclear leukocytes (PMNs) to tissue basement membranes is reduced in diabetes.55 This can result in prolonged inflammation and the wound healing process, as well as reduced defence from infection in the wound.56 Furthermore, PMNs in patients with diabetes exhibit hyperactivity, producing increased levels of ROS, which further damage the local environment.56
Macrophages also play an important role healing. They induce apoptosis of immune cells and promote tissue regeneration.57 However, it has been suggested that macrophage activation is reduced in the hyperglycaemic state58 and function is impaired by AGEs derived from the hyperglycaemic state.59 These changes also lead to delayed or impaired wound repair in diabetes patients.60
Diabetes also impairs wound healing through its hypoxic effects. Impaired blood vessel production (angiogenesis) in patients with diabetes61 can lead to impaired oxygen perfusion. Although initial hypoxia initiates wound healing, prolonged hypoxia impairs wound healing.62 The reduced blood supply also results in reduced fibroblast migration and proliferation,61,63 impeding production of collagen required for wound healing. Furthermore, the reduced oxygen supply results in ROS levels reaching a level exceeding anti-oxidant capacity,64 resulting in oxidative stress and additional tissue damage.62
The diabetic state is also an important consideration in oral surgery because of its effect on bone healing. AGEs have been associated with osteoblast apoptosis65 and interference with osteoblast development.66 In diabetics, osteoclasts resorb more bone and release cytokines to trigger further inflammation in response to LipoPolySaccharide (LPS), released by gram-negative bacteria; whereas in healthy individuals, the osteoclast numbers are well regulated. Furthermore, regulation of the neuropeptides responsible for bony healing is reduced in diabetes patients, impairing osseous healing.54 In summary, diabetes is unfavourable for wound and bony healing due to negative alterations to blood vessels, immune system components and oxygenation.
Delayed healing of extraction sockets has been observed in diabetes patients, creating a need to delay placement of a dental implant.67 Implant survival rate is lower, even in diabetes patients with good glycaemic control.68 It has been recommended that HbA1c levels are tested for prior to surgical treatment.69 HbA1c is an indicator of glycated haemoglobin and can be used to measure long-term glycaemic control. A recent systematic review concluded that diabetics with poor glycaemic control exhibit an increased risk for peri-implantitis and implant failure, as well as reduced osseointegration.70 The same review concluded that implant procedures are as predictable as in healthy patients when diabetes patients have good glycaemic control (Figure 3).70
Oral medicine
Oral candidiasis may be prevalent in patients with higher levels of HbA1c. This is likely due to the effect of diabetes on the immune system, which has previously been discussed. Furthermore, the presence of a denture, covering relatively large areas of the oral mucosa, is associated with oral yeast infection.71 This may be explained by reduced salivary flow over the oral mucosa34 and the reduced immunological properties of saliva72 associated with diabetes.
Like endothelial cells, neural cells do not require insulin for the uptake of glucose; excessive levels of ROS are required to remove the excess glucose taken up into neural cells. This may ultimately result in nerve damage and neuropathy in diabetes and explain the reduced salivary gland function and salivary flow associated with diabetes. This could also explain the development of burning mouth syndrome in patients with diabetes with no oral abnormalities.73
According to one study, xerostomia is more prevalent in diabetes patients than patients without diabetes.36 Diabetes may impact on the salivary glands through reduced vascularity and nerve damage, altering its salivary output and immunological qualities. This may be compounded by poor denture hygiene and/or inappropriate denture design. These points also bear relevance in the prevention and management of dental caries.
Table 1 offers a brief summary of the effects of diabetes.
Potential effect(s) of diabetes
Caries
Diabetes patients produce less saliva to act as an ion buffer for enamel demineralization; and the saliva may contain higher levels of glucose – increasing caries risk
Periodontal Disease
Microangiopathy and impaired immune response associated with diabetes, which in turn has been associated with increased probing pocket depths
Elevated blood glucose may be associated with periodontal abscess formation
Endodontics
Calcifications in the pulp chamber are more prevalent. Combined with the reduced circulation associated with diabetes – pulpal repair is impaired
Impaired pulpal circulation associated with diabetes may lead to pulpal necrosis and pain in a tooth with no clinical signs of pathology (diabetic odontalgia)
Periapical bony healing post treatment is also impaired due to the reduced vascular supply
Oral Surgery
Increased AGEs promote inflammation, impaired immunity delays wound and bone healing
Poor glycaemic control increases risk of peri-implantitis and is associated with reduced osseointegration
Oral Medicine
Impairment of the immune system increases risk of oral candidiasis
Neural damage associated with diabetes, reduced vascular supply could be linked with xerostomia
Prosthodontics
Increased risk of candidiasis when mucosal coverage is incorporated into design
Montgomery Ruling and consent
Clinicians would traditionally have been supported in negligence claims if their conduct was deemed in line with that of a responsible body within their profession. This was the application of the ‘Bolam’ test. However, the Supreme Court's ruling of the Montgomery case now means that clinicians should tell patients of material risks which they would want to know. If a reasonable patient in the same position would view the risk as significant, or the clinician believes or should believe that the patient would attach risk, it may be deemed a reasonable risk which the patient should be informed about.
Considering the effects of diabetes on treatment in general dental practice discussed and the Montgomery ruling, dentists should make diabetic patients aware of the significance of their condition on their dental treatment and oral health.
Conclusion
There is a significant proportion of the UK's population currently with undiagnosed diabetes. The dental team play a role in identifying these cases from oral signs and symptoms, which have been discussed in this review.
Furthermore, patients with diabetes should be educated and informed about the effects that their condition may have on their oral health and treatment. This may be critical in diabetes patients with poor glycaemic control.