Bamias A, Kastritis E, Bamia C Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: incidence and risk factors. J Clin Oncol. 2005; 23:(34)8580-8587
Storm T, Thamsborg G, Steinich T Effect of intermittent cyclical etidronate therapy on bone mass and fracture rate in women with postmenopausal osteoporosis. N Engl J Med. 1990; 322:1265-12
Watts NB, Harris ST, Genant HK Intermittent cyclical etidronate treatment of postmenopausal osteoporosis. N Engl J Med. 1990; 323:73-79
Harris ST, Watts NB, Jackson RD 4-year study of intermittent cyclic etidronate treatment of postmenopausal osteoporosis – 3 years of blinded therapy followed by one year of open therapy. Am J Med. 1993; 95:557-567
Khosla S, Bilezikian JP, Dempster DW Benefits and risks of bisphosphonate therapy for osteoporosis. J Clin Endocrinol Metab. 2012; 97:2272-2282
Merton R. The unanticipated consequences of purposive social action. Am Sociol Rev. 1936; 1:894-904
Marx Robert E. Uncovering the cause of “phossy jaw” Circa 1858 to 1906: oral and maxillofacial surgery closed case files – case closed. J Oral Maxillofac Surg. 2008; 66:2356-2363
Frank P, Ottomboni MA., 3rd edn. Chichester: Wiley; 2016
Taylor T, Bryant C, Popat S. A study of 225 patients on bisphosphonates presenting to the bisphosphonate clinic at King's College Hospital. Br Dent J. 2013; 214
Qi WX, Tang LN, He AN Risk of osteonecrosis of the jaw in cancer patients receiving denosumab: a meta-analysis of seven randomized controlled trials. Int J Clin Oncol. 2014; 19:403-410 https://doi.org/10.1007/s10147-013-0561-6
Grbic JT, Black DM, Lyles KW The incidence of osteonecrosis of the jaw in patients receiving 5 milligrams of zoledronic acid: data from the health outcomes and reduced incidence with zoledronic acid once yearly clinical trials program. J Am Dent Assoc. 2010; 141:1365-1370
Malden N, Lopes V. An epidemiological study of alendronate-related osteonecrosis of the jaws. A case series from the south-east of Scotland with attention given to case definition and prevalence. J Bone Miner Metab. 2012; 30:171-182
Lo JC, O'Ryan FS, Gordon NP Prevalence of osteonecrosis of the jaw in patients with oral bisphosphonate exposure. J Oral Maxillofac Surg. 2010; 68:243-253
Papapoulos S, Chapurlat R, Libanati C Five years of denosumab exposure in women with postmenopausal osteoporosis: results from the first two years of the FREEDOM extension. J Bone Miner Res. 2012; 27:694-701
Kyrgidis A, Vahtsevanos K, Koloutsos G Bisphosphonate-related osteonecrosis of the jaws: a case-control study of risk factors in breast cancer patients. J Clin Oncol. 2008; 26:463-468
Ruggiero SL, Dodson TB, Assael LA American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws – 2009 update. J Oral Maxillofac Surg. 2009; 67:2-12
Saad F, Brown JE, Van Poznak C Incidence, risk factors, and outcomes of osteonecrosis of the jaw: integrated analysis from three blinded active-controlled phase III trials in cancer patients with bone metastases. Ann Oncol. 2012; 23:1341-1347
Vahtsevanos K, Kyrgidis A, Verrou E Longitudinal cohort study of risk factors in cancer patients of bisphosphonate-related osteonecrosis of the jaw. J Clin Oncol. 2009; 27:5356-5362
Hoff AO, Toth BB, Altundag K Osteonecrosis of the jaw in patients receiving intravenous bisphosphonates. J Bone Miner Res. 2005; 20
Zervas K, Verrou E, Teleioudis Z Incidence, risk factors and management of osteonecrosis of the jaw in patients with multiple myeloma: a single-centre experience in 303 patients. Br J Haematol. 2006; 134:620-623
Khosla S, Burr D, Cauley J Bisphosphonate-associated osteonecrosis of the jaw: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2007; 22:1479-1491
Yamazaki T, Yamori M, Ishizaki T Increased incidence of osteonecrosis of the jaw after tooth extraction in patients treated with bisphosphonates: a cohort study. Int J Oral Maxillofac Surg. 2012; 41:1397-1403
Scoletta M, Arata V, Arduino PG Tooth extractions in intravenous bisphosphonate-treated patients: a refined protocol. J Oral Maxillofac Surg. 2013; 71::994-999
Tsao C, Darby I, Ebeling PR Oral health risk factors for bisphosphonate-associated jaw osteonecrosis. J Oral Maxillofac Surg. 2013; 71:1360-1366
Medication-related osteonecrosis of the jaw (MRONJ): realities, risks and responsibilities Lakshmi Rasaratnam Martin Kelleher Sarah Taylor Dental Update 2024 45:2, 707-709.
Authors
LakshmiRasaratnam
BDS Lond(Hons), MJDF,
Specialist Registrar, King's College London and William Harvey Hospital, Ashford, Kent
Considerable concern and confusion exists about Medication-Related OsteoNecrosis of the Jaw (MRONJ) which can be a painful, prolonged and debilitating condition caused by the death of jaw bone. The most common class of drugs causing this rare problem is the bisphosphonate group of drugs, which resulted in the term Bisphosphonate-Related OsteoNecrosis of the Jaw previously being given the acronym BRONJ.
CPD/Clinical Relevance: This article will help to update healthcare practitioners on assessing the realistic risks of patients developing MRONJ. It offers some ideas on reducing those risks in a practical way.
Article
If patients are on oral bisphosphonates, routine conservative dentistry is not a problem and, even if they need surgical treatment such as an extraction, osteonecrosis of the jaw afterwards is very rare (less than 1%).
Other drugs were developed to slow down bone resorption caused by many serious medical conditions and some are associated occasionally with OsteoNecrosis of the Jaw (ONJ), thereby giving rise to the term ARONJ (meaning Anti-Resorptive OsteoNecrosis of the Jaw). Subsequently, owing to the plethora of other drugs, sometimes used in combinations, which became implicated in developing this condition, the term Medication Related OsteoNecrosis of the Jaw (MRONJ) became the preferred term for this problem.
The range of anti-resorptive drugs available includes ones of varying potency and modes of action with differing risks of them being associated with osteonecrosis of the jaws. They are used either alone, or in combination with other drugs, to manage disorders such as severe osteoporosis, but increasingly for managing various bone complications of different types of cancers. MRONJ most commonly becomes apparent in patients who have been taking these drugs for very prolonged periods along with steroids, or those taking intravenous forms of the drugs, and who then undergo invasive surgical procedures, usually dental extractions.
While mercifully rare, jaw bone necrosis can be spontaneous, and is usually seen in oncology patients taking frequent (meaning once every 3 or 4 weeks) powerful bone protective drugs.
As a consequence of the rare but real risk of jaw bone necrosis, dentists, medical practitioners, and some patients have expressed confusion about the level of actual, or imaginary, risk of patients developing osteonecrosis of the jaw after jaw bone surgery. When it does occur, some have questioned where the present and future responsibilities for it developing ought to lie.
There has been a welcomed greater awareness of the potential seriousness of this jaw bone necrosis, with recent guidelines published by the Scottish Dental Clinical Effectiveness Programme1 outlining key strategies for risk assessment in those vulnerable patients in order to try to prevent jaw osteonecrosis problems developing, as well as providing management strategies for treating established MRONJ.
More effective communication between the medical and dental professionals is desirable to ensure that all patients who are due to begin, or are considering taking, medications, which will place them at higher risk of MRONJ, should be referred to a dentist for a comprehensive assessment and completion of any appropriate dental treatment before commencing these medications.
Ideally, these patients should also be helped with a customized preventive plan to minimize future risks of MRONJ becoming a problem prior to commencing on these important and helpful drugs.
Bisphosphonate drugs reduce the rate of bone resorption by interfering with osteoclastic functions and have become the standard treatment to help manage various bone problems, such as osteoporosis, as well as some malignant and non-malignant diseases affecting bones in various ways.2
Bisphosphonate drugs have been shown to prevent, delay, or minimize the effects of bone resorbing diseases and to improve patients' quality of life by reducing their serious bone pain and helping to prevent hip and other bone fractures by up to 60%.3-6 However, an undesirable consequence of using bisphosphonate medications is that proportionately greater amounts of the drug can be deposited in some ‘non-target areas’ of the body, such as the mandible and the maxilla. This results in reduced bone turnover and reduced osteoclastic cell functions, or frank cell death (apoptosis), in the untargeted osteoclasts of the lower and upper jaws.
If a patient who is taking these drugs needs extractions, or other invasive jaw bone surgery, then delayed healing can occur occasionally, with the jaw bone failing to heal normally afterwards, thereby producing the clinical picture of OsteoNecrosis of the Jaw (ONJ) (Figure 1).
Figure 1. Visible yellowish-grey, necrotic, exposed bone which was still obvious 6 months following removal of a tooth in a long-term bisphosphonate patient who was also on steroids.
Unintended effects of drugs
Many advances in medicine, while they are generally to be welcomed, have led to some unpredicted problems becoming apparent as the ‘law of unintended consequences’7 manifests itself over time and in varying circumstances. Drug companies generally tend to brush these off as mere ‘side-effects’ but, in reality, they are ‘effects’ of the drug which may, or may not, have become apparent in their previous, often highly selective, trials. Pharmaceutical companies usually concentrate on the positive benefits of the drugs, which is understandable from a commercial marketing perspective. Euphemisms are commonly used in the carefully worded, sometimes biased, reports of selective trials on carefully selected patients. However, the unwanted effects of some drugs, while being rare, can be serious, especially from the perspective of patients' quality of life. When these risks become more apparent over time, or some co-risks become more obvious, then patients, for consent reasons, ought to know about their individual and particular level of risks in advance of taking drugs, particularly if there are other viable options to reduce their risks.8
Changing the thinking about ‘Cancer’
Patients who would have previously died relatively soon after being diagnosed with various malignant diseases, many of which metastasize to bone, now survive with the condition, either with their cancer in remission or slowly progressing, provided they have favourable responses to ever-advancing treatments.
The net effect of those changes is that many cancers are no longer the acute killer disease that they were thought to be previously, but many have changed into being a chronic disease, often as a result of the newer, more effective, drug treatments. The dental profession's thinking about these patients' long-term dental issues therefore needs to change. In many cases these patients no longer ought to be thought of as ‘acutely ill-and-likely-to-die-soon-patients', but rather as chronic sufferers from their various diseases.
This change in their prognosis frequently results in increased longevity of their lives, but not necessarily with them being in good health. This outcome commonly results in them taking various long-term medications, often for other concurrent diseases. As a consequence of these changes, both dental and medical practitioners need to be more aware of the existence of possible osteonecrotic jaw problems in patients' futures if jaw bone surgery is likely, particularly in the mandible. The prevention of osteonecrosis of the jaw seems to be sensible and, whenever possible, it should be made a priority in the dental management of these patients.
More general dental practitioners are likely to have to treat these patients at some stage, due to various dental problems manifesting themselves over time. This will become more probable as dentate patients, many with already heavily compromised dentitions (‘The Heavy Metal Brigade’) get more frail as they age, while their dental hygiene effectiveness may well reduce. The dental deterioration can be compounded by xerostomia, frequently caused by the various other ‘anti’ drugs which reduce their protective saliva as an unwanted effect. Their uncomfortable dry mouths lead to them sipping drinks to lubricate their mouths, which then often means them sipping fluids other than just water (such as fruit juice) relatively frequently, particularly at night, as well as their overall diet potentially becoming more cariogenic in nature.
A ‘silver tsunami’ of dental problems has already built up in the ‘reasonably well’ ageing patients, many of whom have various or multiple comorbidities and take a variety of medications which can affect the oral environment.
Adequate resources of time, skills and finances have not been allocated to treat these properly, nor to prevent future problems developing, particularly under the very flawed NHS UDA system in England. To this ‘relatively healthy’ ageing group, the increasing numbers of survivors of many cancers are being added, many of whom will now survive for many years. However, there are scant, and certainly not adequate, state financial resources being made available to treat their present dental problems properly, let alone having a sensible system in place to help to prevent the predictable future ones developing.
Dentists trying to minimize complications from dental extractions, or other jaw surgery, may well ask for guidance from various dental or oral surgical specialists, medical practitioners or cancer specialists, partly because of the use of a bewildering array of newer drugs, eg Receptor Activator of Nuclear factor Kappa-B Ligand inhibitors (known as RANKL inhibitors) such as Denosumab (Prolia), becoming more common in managing some patients.
Some ‘aggressive prevention’ of dental problems developing seems to be appropriate and some pragmatic helpful hints and ideas about more effective prevention are offered later on in this paper.
Confusion about jargon, terminology and acronyms: BRONJ vs ARONJ vs MRONJ
BRONJ
Bisphosphonate drugs help to improve the quality of life of patients with various bone-affecting conditions, but they are sometimes associated with the undesirable consequences of occasional jaw necrosis. This is rare and usually happens following dental extraction, or other surgical intervention, involving the drug-affected jaw bone. When this condition was identified it was given the term ‘Bisphosphonate-Related OsteoNecrosis of the Jaw’ and it became better known by its acronym BRONJ.
ARONJ
Bisphosphonates are not the only drugs associated with these episodes of jaw necrosis. Other anti-resorptive bone medications, such as RANKL inhibitors (qv), and other classes of drugs, which were developed as alternatives to bisphosphonates, also became implicated in the ONJ condition developing. As a consequence of this, the condition was renamed Anti-Resorptive OsteoNecrosis of the Jaw (abbreviated to ARONJ).
MRONJ
More recently, as new classes of drugs continued to be developed that occasionally became associated with jaw bone necrosis developing, the preferred term morphed in to ‘Medication-Related OsteoNecrosis of the Jaw (MRONJ).
History and incidence
Unlike Osteo-Radio-Necrosis (ORN), which is caused by hypoxia, hypo-vascularity and hypo-cellularity of the bone as a result of radiation therapy to the head and neck region, MRONJ (formerly called BRONJ or ARONJ as discussed above) is a relatively new manifestation of a known old problem which used to be known colloquially as ‘Phossy jaw’.
Historically, people working in various aspects of the match-making industry from the late 1850s onwards developed signs and symptoms of jaw necrosis. This was as a result of the workers inhaling phosphorus fumes involved in the manufacture of ‘strike anywhere’ matches. The formula for yellow phosphorus is P4O10. When phosphorus is combined with water and carbon dioxide, which are normal parts of human respiration, and then mixed with readily available human amino acids, such as lysine, the resulting compounds, which were synthesized naturally by the body, were chemically very similar to alendronic acid or pamidronate – two of the common bisphosphonate drugs now used.9 Osteonecrosis of the jaw had become very rare in the UK because the hazards involved in the production of matches meant that there were manufacturing and law changes in the early 1900s. However, drug-related osteonecrosis of the jaw began to re-appear with the advent of the osteoclastic modifying bisphosphonate drugs about 20 years ago.
As is common with many drugs, low concentrations of the drugs are helpful, but much higher concentrations of drugs are generally more dangerous.10 Although the incidence of osteonecrosis of the jaw is quoted by many drug companies as being extremely rare, allegedly affecting somewhere between 1 in 10,000 to 1 in 100,000 people per year,11 the incidence of MRONJ in those people on the drugs who also have dental extractions is actually unknown, although some limited evidence regarding this is discussed later. Furthermore, the lasting effects of prolonged exposure to bisphosphonate drugs which are retained within the body, even after cessation of the medication, make it difficult to quantify the precise likely future incidence of MRONJ in these patients, especially if there are other risk factors involved (Figure 2).
Figure 2. Spontaneous necrosis of the bone in the lower right mandible after multiple years of oral bisphosphonates combined with steroids.
In many instances, MRONJ is relatively mild with only delayed healing occurring, or only small amounts of frank jaw necrosis developing, which may not even be reported accurately, or in a timely fashion, because there is no recognized central recording authority to which to report it. However, more serious presentations tend to occur, especially with multiple frequent intravenous bisphosphonate infusions or with RANKL inhibitors.12 There is, as yet, an unknown potential long-term impact of the various newer drugs, or combinations of them which are being marketed at present when these are then combined with oral surgical procedures.
A very accurate picture of incidence is difficult to get because there are probably issues of late or imprecise reporting of other factors which are important in the development of ONJ after extractions. These include the exact drug(s) involved, the mode of administration, ie oral or intravenous infusion or subcutaneous administration, the frequency and duration of the drug(s) delivered, as well as the site and difficulty of the dental extractions producing varying amounts of physical damage to the jaw bone. The incidence of complications for low risk patients being quite uncommon means that proper research would need enormous cohorts of patients to find any statistically significant results, which hinders accurate predictions of risk.
A paper by Ruggiero et al in 2014 on behalf of the American Association of Oral Maxillofacial Surgery outlined the following key findings:13
Estimates for developing ONJ after tooth extraction among cancer patients exposed to intravenous bisphosphonates ranges from 1.6 to 14.8%.
The risk of ONJ among cancer patients exposed to zolendronate appears to be somewhere between 50–100 times higher than cancer patients treated with a placebo.
The risk for ONJ among cancer patient exposed to Denosumab (Prolia), which is a RANKL inhibitor (qv), is comparable to the risk of ONJ in patients exposed to zolendronate.
In a case-control study among cancer patients exposed to zolendronate, tooth extraction was associated with a 16-fold increased risk for ONJ when compared to cancer patients without extraction (odds ratio [OR] = 16.4; 95% confidence interval [CI], 3.4–79.6).
In one longitudinal cohort study in a sample of cancer patients exposed to intravenous bisphosphonates (predominately zolendronate), tooth extraction was associated with a 33-fold increased risk for ONJ.
MRONJ is more likely to occur in the mandible (73%) than the maxilla (22.5%) but it can appear in both jaws (4.5%).
There are millions of prescriptions issued for oral bisphosphonates in the USA and the UK and only a small fraction of the patients on these drugs need extractions. Even then, there is a minimal risk of developing ONJ with oral bisphosphonates, unless there are other risk factors, such as prolonged exposure over very many years or concomitant steroids being involved.
Results vary according to the paper published and probably reflect the multiple variabilities and confounding factors in the reported groups.
However, some clinicians, particularly those oral surgeons who actually have to do the extractions in these patients on frequent intravenous bisphosphonate infusions or Denosumab, disagree with the published low figures,14 possibly for a variety of reasons. This may be because they are the ones who have to deal with the risky oral surgical procedures in their own centres, as well as coping with the post-extraction jaw necrosis problems of varying severity sent to them from elsewhere. One study on patients on intravenous amino-bisphosphonate therapy for metastatic bone cancer who also had extraction or other jaw surgical intervention, reported a 6–11% incidence of MRONJ.2,15
In summary, it seems clear that, following extractions, patients who have received, or are being given, multiple intravenous bisphosphonate infusions or Denosumab for cancer have significantly higher risks of developing ONJ than those patients who are just on oral bisphosphonates, or not on any anti-resorptive bone drugs at all.
Which conditions are treated with these drugs?
Table 1 illustrates some of the medical conditions that are frequently treated with bisphosphonate drugs. Table 2 demonstrates that potent bisphosphonates, such as Pamidronate (Aredia) or Zoledronic acid (Zometa) given at a high frequency are associated with a higher risk of MRONJ compared to very low reported figures for oral bisphosphonates.1,13,15 The list in Table 2 can help to identify higher risk drugs that require early referral to a dental professional, prior to starting the medication. However, patients who are already taking these medications must be assessed for risk based on the type of medication, frequency of intake, overall duration of drug intake, any concurrent glucocorticoid steroid use and previous MRONJ experience, as summarized in Table 3 according to the 2017 Scottish Dental Clinical Effectiveness Programme.1 Although these guidelines classify Denosumab use for any duration in osteoporosis/non-malignant bone diseases as a ‘low risk’, the authors feel that the risk is moderate-to-high, with risks quoted by other studies up to 2%.16,20Tables 4 and 5 provide a list of drugs used in the management of disease affecting the bony skeleton. Table 5 lists some newer drugs which have an impact on osteoblastic and osteoclastic functions. There is a known greater risk of MRONJ being associated with Denosumab, and limited evidence regarding certain anti-angiogenic medications, including Bevacizumab and Sunitinib and other anti-neoplastic drugs, which are in the late stages of trials.13
Non-malignant
Malignant
OsteoporosisOsteogenesis ImperfectaPaget's diseaseFibrous dysplasiaCystic Fibrosis patients with osteoporosisPrimary hyperparathyroidism
Multiple myelomaBreast cancerBony metastatic lesions, eg secondary to breast, prostate or renal cell cancersHypercalcaemia of malignancy
Note: historically, patients with rheumatoid arthritis and other autoimmune conditions were also treated with steroids. These patients are often missed when assessing risk of MRONJ due to the development of better disease-controlling drugs for this cohort of patients.
NB: ¥Odanacatib carries a risk of stroke and therefore is not marketed clinically.
Why and how does MRONJ occur?
The rapid bone turnover that occurs within the jaws makes them more susceptible to osteonecrosis than other bones. The risks are increased by the ease of bacterial access to the jaw bones, with the thin oral mucous membranes being easy to penetrate surgically. Dental infections are often due to extensive dental caries, and can spread from the dental pulp to the periapical tissues, before spreading infection into the jaw bone. Dental extractions and other surgical procedures, including implant placement, as well as severe periodontal disease, are other potential risks of producing jaw bone necrosis if there has been serious inhibition of osteoclastic function, which is an essential part of bone healing and remodelling.22
Mandible or maxilla?
The mandible (73%) is more than three times more susceptible than the maxilla (22.5%) to developing MRONJ, probably partly due to the bone density and partly to its known poorer blood supply. The reduction in perfusion of the mandibular bone in older patients often occurs as a result of age-related atherosclerosis of the inferior dental artery. The bone density in the mandible is obviously much greater than it is in the maxilla. However, both jaws can be affected concurrently by ONJ, but this is rare (4.5%).23
How does it present clinically and what are the diagnostic features?
MRONJ can present clinically as exposed, non-vital bone, or bone that can be probed through an intra-oral or extra-oral fistula, in the mandible or maxilla.
The diagnosis of MRONJ is made if the clinical picture persists for over eight weeks in a patient taking current/previous medication with anti-resorptive or anti-angiogenic properties, and where there has been no history of radiation therapy to the jaw, or no obvious metastatic spread of disease to the jaws.13
Symptoms and signs of MRONJ
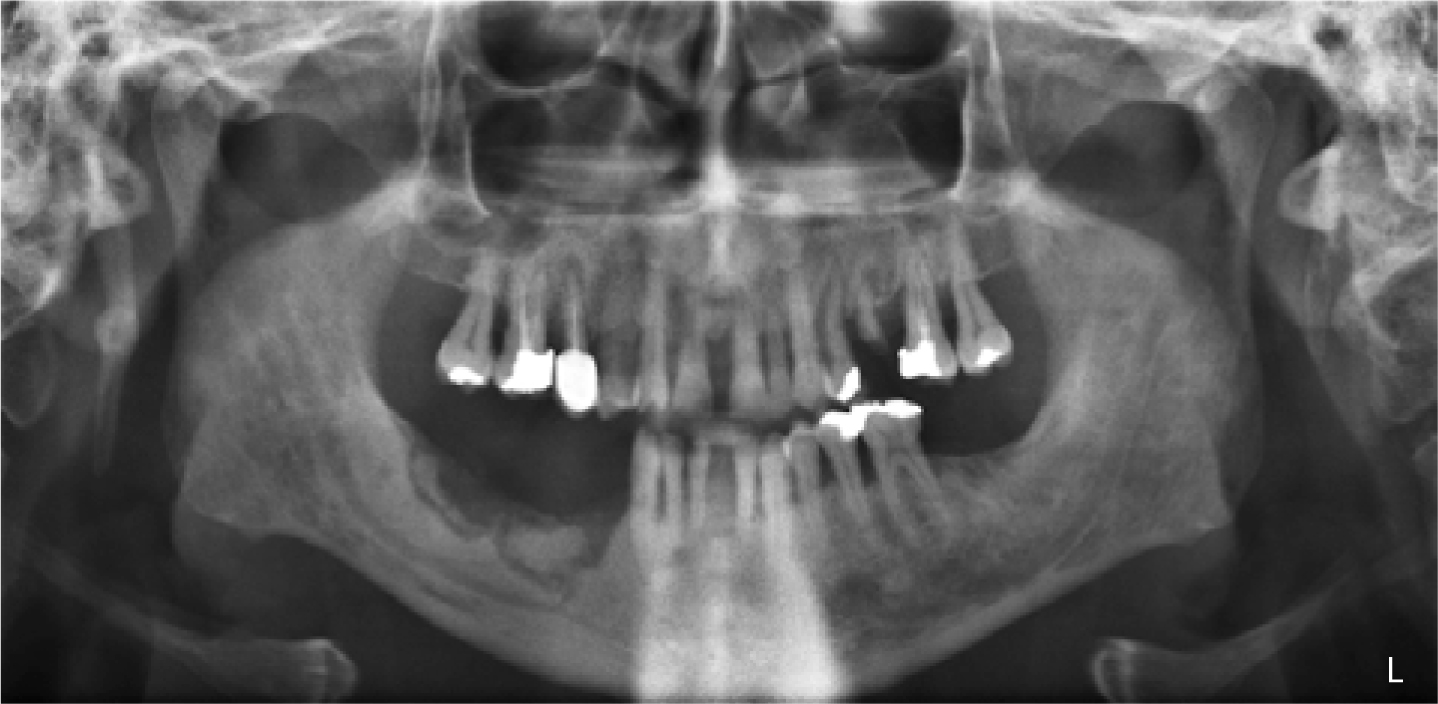
Early stage MRONJ may be identified by evidence of exposed bone, which may be sharp and traumatic to other soft tissues, in the absence of other symptoms. As it develops, or becomes secondarily infected, patients can report symptoms of pain, swelling, numbness, altered nerve sensation (paraesthesia) or other signs of infection. Figures 3 and 4 demonstrate the classic radiographic and clinical appearances of bone necrosis associated with MRONJ.
Figure 3. Dental panoramic tomograph demonstrating the extensive necrosis of the alveolus in the lower right jaw.Figure 4. Clinical appearance of persistent bone necrosis at 5 months in a patient having had one annual infusion of IV bisphosphonate therapy each year for the previous 3 years.
This condition can occur spontaneously, but is usually as a result of direct surgical trauma to the jaw bone, such as that caused by a dental extraction, or other oral surgical procedure. This is due to the poor bone healing after ‘normal surgical trauma’ as a direct result of the bisphosphonate therapy on the osteoclasts or RANKL-inhibitors affecting osteoclastic function activity, thereby inhibiting normal alveolar resorption and bone remodelling processes.
Risk factors of developing MRONJ
These can be grouped into:
Patient-related factors;
Drug-related issues;
Local risk factors that can increase the risks of developing MRONJ.13
Patient-related factors
Patient-related factors include:
Being immuno-compromised or taking immunosuppressant drugs;
Having a history of previous/current long-term steroid use;
Gender: there is a higher prevalence of MRONJ in females. This might be due to the nature of the bone disease being treated (ie osteoporosis or breast cancer with metastases).14,24,25
Drug-related risk factors
Drug-related risk factors include:
The relative potency of the medication, for instance, IV zoledronate produces 9.5-fold greater risk of producing MRONJ than IV pamidronate alone.26
The route of administration, eg IV bisphosphonates pose a greater risk than oral bisphosphonates.
Duration of medication use: increased duration of bisphosphonate use is associated with a greater risk, particularly if it is used for more than 4 years.13
Combination of bisphophonates used along with other drugs, eg steroids. The combination of bisphosphonates and steroids is often used in the management of autoimmune disease, eg rheumatoid arthritis. Bisphosphonates are also used to prevent bone loss caused by steroids. The concurrent use of corticosteroids along with oral bisphosphonates has been shown to cause an increased, but still low, risk of developing MRONJ.27
Dentists should be mindful that, in treating many autoimmune conditions, mono-clonal antibody based medications are replacing steroids as the treatment of choice. However, these patients may have had previous exposure to anti-resorptive medications, which are likely to have been bisphosphonates. Ideally, clinicians should ask probing questions about longstanding autoimmune medical conditions to try to determine what steroids, or other medications, have been involved in their previous management.
Local risk factors
Local risk factors include:
Dento-alveolar surgery, including:
- Dental extractions and their surgical difficulty;
- Dental implant placement;
- Periodontal surgery with bone exposure;
Periodontal disease;
Oral hygiene;
Ill-fitting dentures.
Discussion
The chances of patients on oral bisphosphonates only developing MRONJ are very low, with this only affecting about 0.5% of patients. However, this is provided they have not been on them for over 4 years and have not been on steroids simultaneously.
The risks for oncology patients exposed to IV bisphosphonates are much higher at an estimated 1.6–14.8%.28,29 Medical and dental practitioners should probably still be cautious as the real figures when all the combined risks are involved are still emerging. The risk of MRONJ is much greater when these patients undergo dental surgical procedures, such as extractions, with 52–61% of patients in some outlying studies undergoing dental extractions having been reported to get MRONJ.13,20,24
In 2008, Kyrgidis et al showed that cancer patients taking zoledronate had a 16 times greater risk of MRONJ after tooth extraction.21
A different study, by Vahtsevanos et al, showed the risks in their group of cancer patients having dental extractions to be as high as 33 times that of patients not on intravenous bisphosphonates.24
Another study, by Hoff et al, calculated that the risks of MRONJ in patients taking IV bisphosphonates who underwent dento-alveolar surgery were 7 times greater than those patients who did not have dento-alveolar surgery.25
The overall presence of inflammation in the oral cavity associated with dental disease has been shown to increase the risk of MRONJ.30
In summary, there are wildly differing figures quoted by different studies. These results are probably a reflection of variations in the reported groups. The inconsistency of the results are likely to be due to the duration of exposure to the drugs, or the possible combinations of bisphosphonates with other drugs and/or the different risk profiles of some anti-resorptive drugs and/or their frequency and mode of administration. Other factors which might explain variations could be related to the technical difficulty of the surgery being done and/or whether it was in the upper or lower jaw and/or the patient's gender, the previous duration of steroid use and/or the type of cancer being treated. These are just some of the factors which, when taken in combination, are difficult to evaluate accurately. Caution is therefore advised as the true picture is likely to take quite some time to become clearer.
Some patients with hypercalcaemia, oncological bone disease or bone pain associated with cancer metastasis really do require IV bisphosphonates, such as pamidronate, rather than oral bisphosphonates. However, in other cases of drug prescription, eg osteoporosis, it would appear that any prescriber of IV or subcutaneously delivered drugs should be cautious about under-estimating the importance and relevance of the MRONJ risks involved. Consideration should be given to whether prescription of intravenous or subcutaneous anti-resorptive medications should be limited to those very intolerant of oral preparations, or where there has been an inadequate response.
This is because the longer term increased risk of complications associated with these IV or SC preparations could well play a role in the oral surgical management of these patients for the rest of their lives, as illustrated in Figure 5.
Figure 5.
(a, b) Clinical views showing MRONJ affecting the lower left mandible following a dental extraction in a patient taking zometa 4 times a year with a concomitant history of steroid use. Interesting clinical observation: Seabond®, a commercially available denture relining material was used by the patient on a regular basis to cover the exposed bone and was deemed by the patient to be very helpful (product available from www.seabond.com). (c) Dental panoramic tomography showing significant left mandibular jaw destruction after failure to heal after 14 months. (d) Cone Beam CT scan of lower left mandible showing jaw bone destruction at 15 months of non-healing.
Should these drugs be stopped before extractions?
It is generally considered unnecessary to cease taking oral bisphosphonates taken for less than 3 years prior to dental extractions.13 Despite the possible consequences of MRONJ, patients should probably continue to take their oral low potency bisphosphonate medication (especially when this is not combined with steroids), for conditions such as post-menopausal osteoporosis, and undergo their routine dental treatment, as and when needed.
There is a lack of solid evidence supporting, or refuting, the use of a ‘drug holiday’ in patients taking the more potent anti-resorptive medications prior to dental surgical procedures. However, some feel that a drug holiday should be considered, on a pragmatic basis, in patients taking bisphosphonates for more than 4 years and those with other risk factors, such as exposure to gluco-corticosteroids, diabetes and/or smoking until soft tissue healing has occurred.13
The RANKL inhibitor, Denosumab, apparently has a shorter period of being retained in the body. Patients receiving this medication on a 6-monthly basis for management of osteoporosis should avoid extractions in the period after injections (where possible) and full healing has been demonstrated prior to any further doses. Where patients receive Denosumab as part of their cancer treatment, if extractions are likely to be needed, some discussions are required between oncologist, dentist and patient to evaluate the benefits of continued drug administration against the risk of developing MRONJ. In the authors' experience, a number of patients have had a pragmatic approach where their Denosumab was stopped for two months prior to, and two months following, their unavoidable dental extractions and seemed to heal slowly but reasonably well.
Summary
There is only a very low risk of MRONJ occurring in patients having oral surgical procedures if they are taking just oral bisphosphonates, without other risk factors such as taking steroids.
There is a significantly higher risk of MRONJ following extractions or other jaw bone surgery in those patients on the more potent intravenous infusion bisphosphonate drugs or oral bisphosphonates, if the duration is greater than 5 years, or those who are taking these drugs with concurrent glucocorticoid steroids for significant amounts of time.
Those being treated for the management of cancer with frequent anti-resorptive or anti-angiogenic drugs (or both) are at high risk of MRONJ, as are those patients who have had a previous diagnosis of MRONJ.
Subcutaneously delivered RANKL inhibitors (eg Denosumab) with glucocorticosteroids have a high risk of MRONJ.
Root filling of problematic teeth should be attempted, if at all possible, even if the tooth cannot be restored, but rather sealed with conventional radio-opaque glass ionomer cement (GIC) after canal disinfection. This is preferable, if possible, in order to avoid the risk of MRONJ developing in higher risk patients.
Responsibilities. Who is responsible?
It would seem prudent to put appropriate emphasis on preventing MRONJ developing from the outset. Responsible healthcare professionals involved in prescription of anti-resorptive medications should seek to refer such patients for proper dental assessments and appropriate treatment before commencing the drugs with a known higher risk of MRONJ. This would be to pre-empt and prevent future dento-alveolar surgery by eliminating active disease and putting a suitable preventive plan in place. Patients should be informed of the potential future risk to encourage them to engage with preventive strategies.
The recent Supreme Court ruling in the case of Montgomery versus Lanarkshire Health Board (2015) has implications here as it emphasized the recent paradigm shift in the clinician-patient relationship on information about material risks and consent.8 The subtle but significant change in emphasis means that patients now really do need to understand not just all of the relevant benefits but also all of the relevant potential risks associated with a particular treatment (even if they do not ask about them) before agreeing to the treatment.
It is the patients' prerogative to make their decisions after weighing up the risks, benefits, constraints and implications in their personal value system for their overall health and perception of their wellbeing in the longer term.
Prior to this judgment, both the medical and the dental professions had and still have a ‘duty of candour’ to protect the life and health of patients without causing them unnecessary harm.31
Failure to warn these patients adequately of the future risk of developing MRONJ, particularly after dento-alveolar surgery, which might well have been preventable, is open to criticism. Some might perceive that, by failing to recommend or refer for a dental assessment prior to starting drugs or a regimen deemed to be ‘higher risk’, that some medical practitioners might be unnecessarily increasing the future risk of MRONJ developing in their patients.
Some might argue that, after the Montgomery versus Lanarkshire Health Board ruling in 2015, that it is the consultant oncologist's, or the haematologist's, or the rheumatologist's responsibility to ensure that these patients are referred and seen for a comprehensive dental assessment prior to commencing any intravenous bisphosphonate infusions or, for example, a subcutaneously delivered monoclonal antibody such as Denosumab which have a higher risk of being associated with MRONJ following extractions.
The Montgomery vs Lanarkshire Health Board ruling would seem to imply that prescribers now have a responsibility to discuss any material risks in detail prior to prescription of these medications. Ensuring appropriate dental consultation to enable stabilization of existing dental disease and implementation of a preventive strategy could alleviate the threat of prescribers being exposed to future criticism or to litigation.
However, given the wide variety of conditions which now involve the prescription of potent anti-bone resorptive drugs, there is a logical argument that it is the responsibility of the prescribing clinician, whether that be the oncologist, or general medical practitioner, or rheumatologist or whoever, to ensure, in so far as possible, that foreseeable potential dental problems are dealt with before prescribing such potent and important drugs. That said, it also needs to be accepted that there is often some time urgency involved in wanting to start on these medications, which have often got life-saving and quality of life benefits. Another major problem for these unfortunate patients is that the supposedly available dental systems that are realistically available to help them are very far from perfect. Sadly, the very desirable ‘aggressive prevention’ is not a realistic financial proposition under the multiply flawed NHS UDA remuneration system in primary dental care.
Ideally, a co-operative multidisciplinary approach should be adopted when managing these patients.
This approach could be similar to that usually seen in the dental management of head and neck radiotherapy patients, or in managing those with inherited bleeding disorders, which are usually treated co-operatively with a team of radiotherapists, oncologists or haematologists and others, as appropriate.
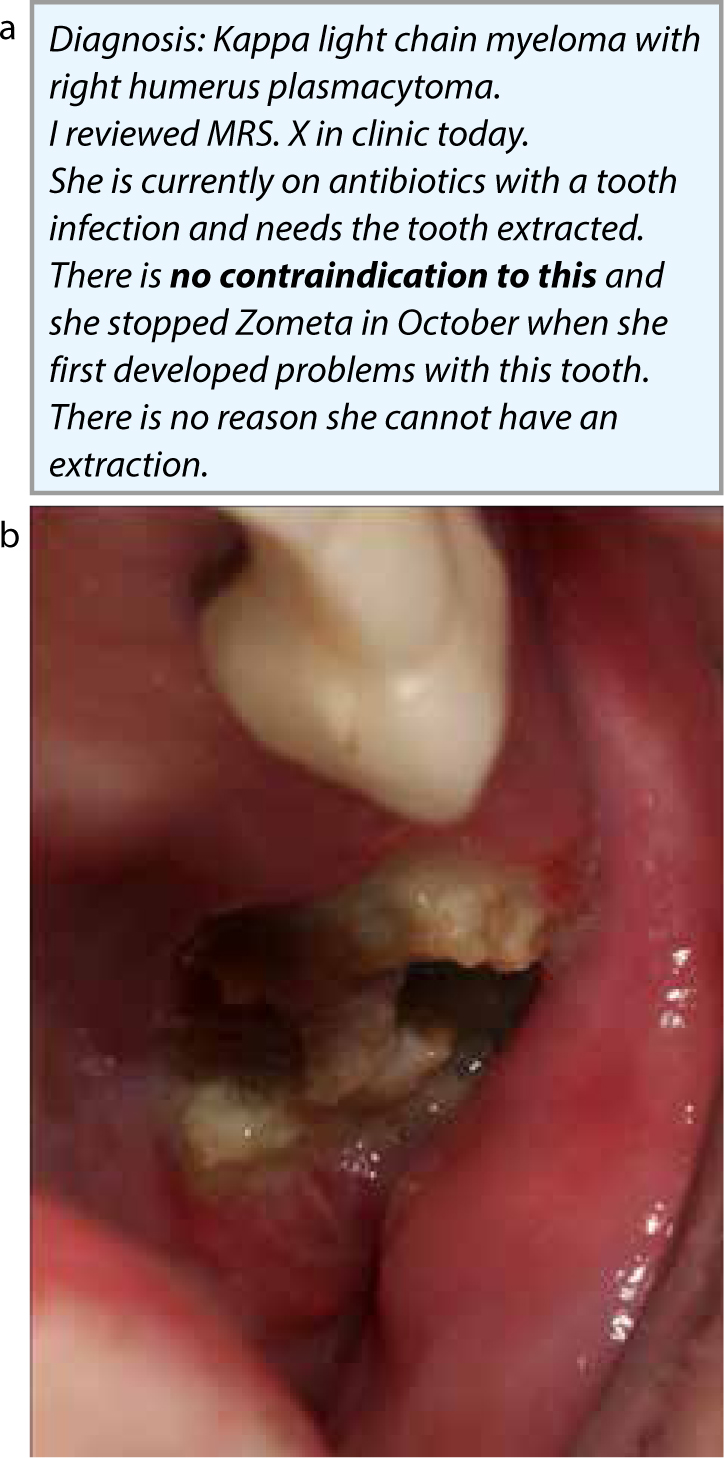
Case example
If the patient in Figure 6 had been seen by a suitably experienced dentist before starting frequent zolendronic acid this tooth could have been addressed, either with root canal filling, restoration and an appropriate preventive regimen, or with extraction. Following multiple infusions, and therefore a high risk of MRONJ, it might still have been possible to root fill and retain this as a root, even if it could not have been restored. It was most likely that it was the extraction which increased her risk of MRONJ, irrespective of any ‘drug holiday’ because bisphosphonates have exceedingly long half-lives. Needless to say, the subsequent costs in terms of quality of life and hospital visits were much greater than the possible costs of a ‘prevention of possible MRONJ’ root filling being done.
Figure 6.
(b) Painful necrotic maxillary jaw bone with obvious inflammation and with no signs of healing at 7 months after extraction.
Strategies to help to prevent MRONJ developing
The early identification of ‘dentally high risk’ patients can aid in the prevention or reduction of the risk of patients developing MRONJ. The patient ought to be assessed by an appropriately experienced dental practitioner, or possibly by a multidisciplinary ‘bisphosphonate or anti-resorptive clinic’, if one is available. This should help to reduce the risks of a vulnerable patient developing MRONJ by allowing time for the dental team to provide appropriate treatment, to give sensible advice and institute personalized preventive strategies early on, particularly in the higher risk group of patients. This should help them to prevent serious dental decay or periodontal (gum) disease problems developing and subsequently then requiring risky extractions.
Appendix 1 provides a template for the urgent dental referral to a Restorative Department for a patient at risk of MRONJ.
The importance of getting these patients on an aggressive prevention regimen needs to be stressed. These patients must be made aware that this ‘aggressive prevention’ regimen is for the remainder of their life, in order to minimize their risks of future dental disease and its possible jaw poor healing consequences.
One helpful hint is to take primary impressions in order to get study models and have vacuum-formed thin thermoplastic mouthguards with cervical reservoirs and a straight-line design extending one millimeter beyond the gingival margins. Superficially, these medical devices vaguely resemble bleaching trays, or Essix retainers, but they are customized differently as their object is to hold a viscous material within them in the critical cervical and interproximal areas to help to reduce caries. They are used to hold a high concentration fluoride material, such as Duraphat 5,000ppm toothpaste (Colgate–Palmolive (UK) Ltd, Guildford Surrey GU2 8JZ), in the evening for a couple of hours, or overnight, three times per week to help to protect the compromised dentition.
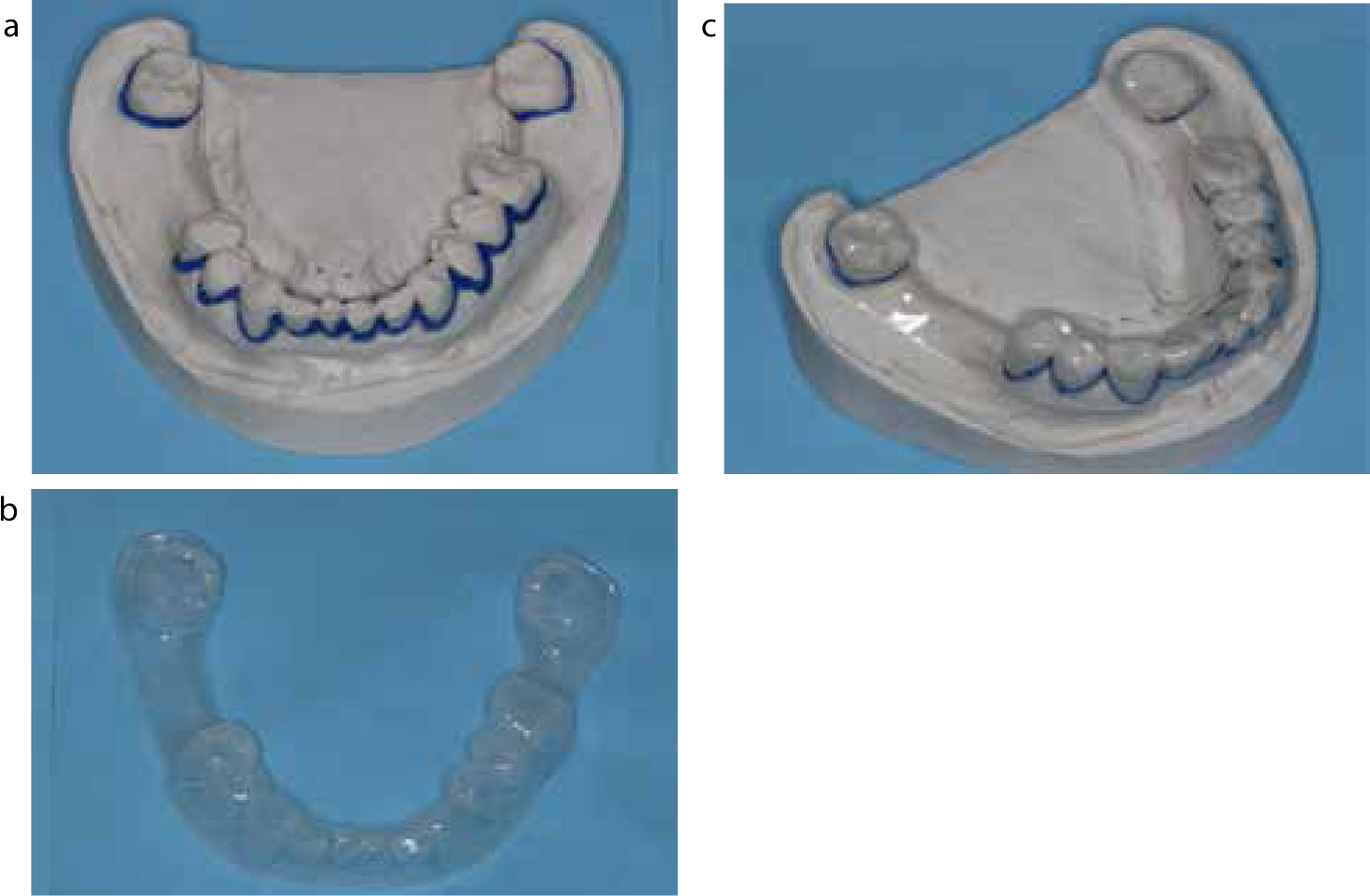
Figure 7 demonstrates the blocked-out casts and straight-line design mouthguard to provide appropriate reservoirs in the sub-contact zones of the teeth and in the cervical regions. This allows the high strength toothpaste to pool selectively in order to re-mineralize these more vulnerable areas.
Figure 7.
(a–c) The casts are modified by adding flowable composite block out material all the way around the necks of the vulnerable teeth up to the level of the contact zones. The one millimetre soft vacuum-formed suck down thermoplastic trays should then hold the caries-reducing viscous gel in the more caries-vulnerable areas for long periods as it will not be washed out by saliva because the straight line trays extend one mm beyond the gingival margins.
The authors suggest that, for patients with a compromised dentition, this pragmatic combination of the thixotropic high concentration neutral PH fluoride gel should be held inside the customized mouthguard and should be worn for a couple of hours before bedtime, or overnight, 3 times a week to try to reduce the risks of further caries developing.
Duraphat 5,000ppm is a prescription only medicine and contains 3 times the normal amount of sodium fluoride. However, it also contains n-lauryl sulphate which is a surfactant (a foaming agent) which can cause gingival redness or soreness on very rare occasions.
Alternatively, Sensodyne Pro Enamel (www.pronamel.co.uk) has 1450ppm of sodium fluoride. It contains 5% potassium nitrate, which is a de-sensitizing agent and does not contain n-lauryl sulphate. It does not require a prescription, it is much cheaper and is readily available over the counter. Obviously, it has less fluoride, although this may not be critical if it is contained within the customized mouthguard and indeed that combination is also known to be effective as a de-sensitizing regimen.
Another material that can be used within these customized mouthguards, again on a pragmatic basis, is Tooth Mousse® (www.GC-dental.com). This contains bio-available calcium and phosphate without fluoride. Calcium and phosphate are obviously lost from teeth during the carious process and having teeth covered with replacement calcium and phosphate ions held within these mouthguards in the danger zones makes a certain amount of pragmatic sense.
Plaque control
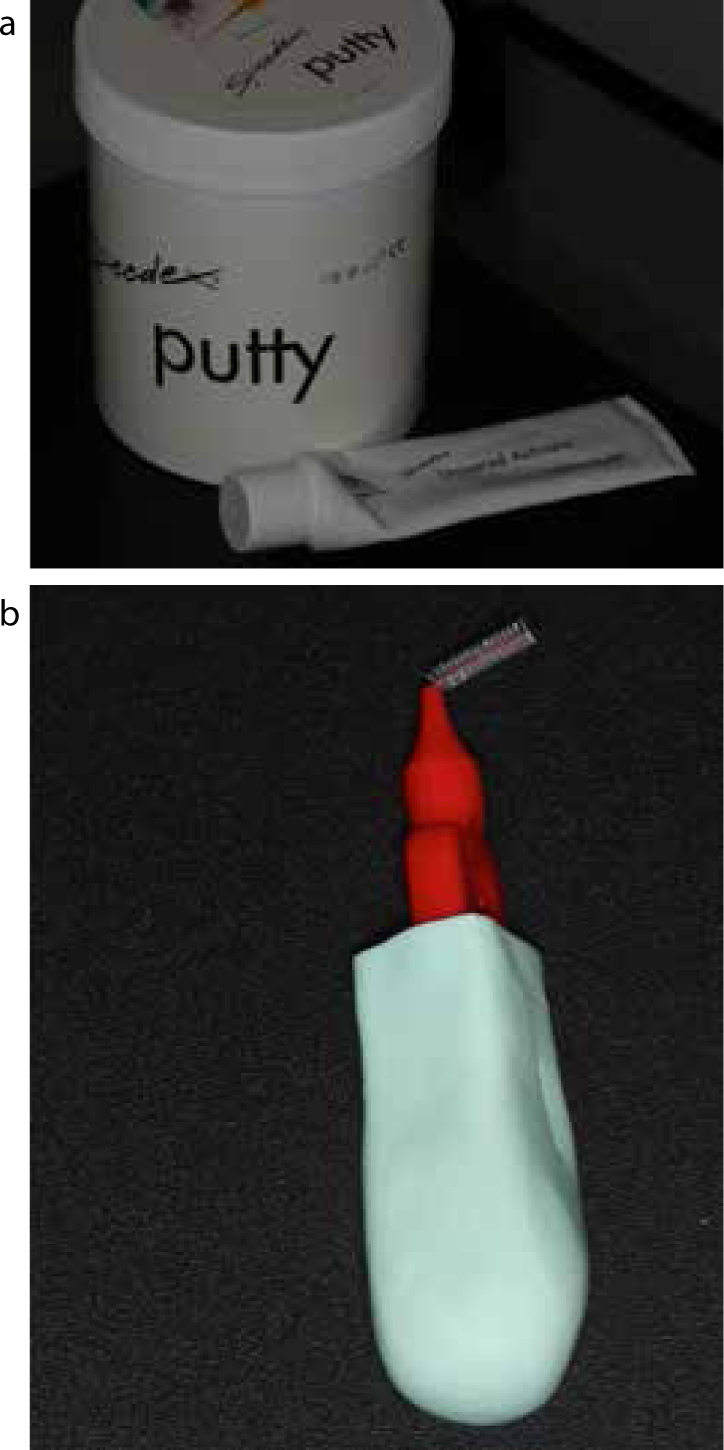
Periodontal health can be maintained by the daily use of angled interdental brushes that are used both vertically and horizontally to reduce the accumulation of plaque around the gingival tissues. The interdental brushes can be modified for patients with limited manual dexterity by adding silicone putty to modify electric toothbrushes, or to modify other interdental cleaning devices (Figures 8 and 9).
Figure 8.
(a–c) A range of straight and angled interdental brushes that can be used vertically and horizontally to remove the pathogenic plaque at least once a day.Figure 9.
(a, b) Modification of interdental brush with putty to improve grip for patients with limited manual dexterity.
Conclusions
The changing pharmacology involved in the management of bone and neoplastic diseases has impacted upon patients' risks of developing MRONJ following routine oral surgery, such as dental extractions. Once diagnosed, MRONJ can be painful and require protracted and complicated management, and the consequences can be very serious for the patient's quality of life. As is usually the case in healthcare, prevention is better than cure.
More effective communication between medical and dental care professionals can help to prevent or reduce the risks of patients developing MRONJ. Sensible and balanced awareness of the realistic risks involved is required by all involved in this area of healthcare.
Early and effective treatment of existing dental disease should be carried out before patients start on intravenous bisphosphonates, or other drugs with a similar risk of being associated with MRONJ developing in future. Adequate resources, education, training and planning are required now to enable these predictable problems to be addressed early on and for problems to be prevented from developing wherever possible.