Turner JH, Reh DD. Incidence and survival in patients with sinonasal cancer: a historical analysis of population-based data. Head Neck. 2012; 34:877-885
Ashraf M, Biswas J, Dam A, Bhowmick A, Jha J, Singh V, Nayak S. Results of treatment of squamous cell carcinoma of maxillary sinus: a 26-year experience. World J Oncol. 2010; 1:28-34
Mehanna P, Smith G. Maxillary carcinoma: a wolf in sheep's clothing. Can Family Phys. 2009; 55:262-264
Ramachamparambathu AK, Vengal M, Mufeed A, Siyo N, Ahmed A. Carcinoma of maxillary sinus masquerading as odontogenic infection. J Clin Diagnost Res. 2016; 10
Mayr SI, Hafizovic K, Waldfahrer F, Iro H, Kütting B. Characterization of initial clinical symptoms and risk factors for sinonasal adenocarcinomas: results of a case–control study. Int Archiv Occup Environ Health. 2010; 83:631-638
, 5th edn. In: Watkinson JC, Gilbert RW (eds). London, UK: Taylor & Francis Ltd; 2012
Tiwari R, Hardillo JA, Mehta D, Slotman B, Tobi H, Croonenburg E Squamous cell carcinoma of maxillary sinus. Head Neck. 2000; 22:164-169
St-Pierre S, Baker SR. Squamous cell carcinoma of the maxillary sinus: analysis of 66 cases. Head Neck Surg. 1983; 5:508-513
Cantù G, Bimbi G, Miceli R, Mariani L, Colombo S, Riccio S Lymph node metastases in malignant tumors of the paranasal sinuses: prognostic value and treatment. Archiv Otolaryngol Head Neck Surg. 2008; 134:170-177
White SC, Pharoah MJ.St Louis, Missouri: Elsevier; 2014
Wright B. Contemporary medico-legal dental radiology. Aust Dent J. 2012; 57:9-15
Rushton L, Bagga S, Bevan R, Brown T, Cherrie J, Holmes PLondon: Health and Safety Executive; 2010
Binazzi A, Ferrante P, Marinaccio A. Occupational exposure and sinonasal cancer: a systematic review and meta-analysis. BMC Cancer. 2015; 15
Santos MRM, Servato JPS, Cardoso SV, de Faria PR, Eisenberg ALA, Dias FL Squamous cell carcinoma at maxillary sinus: clinicopathologic data in a single Brazilian institution with review of literature. Int J Clin Exp Pathol. 2014; 7:8823-8832
Lee CH, Hur DG, Roh H-J, Rha K-S, Jin H-R, Rhee C-S Survival rates of sinonasal squamous cell carcinoma with the new AJCC staging system. Archiv Otolaryngol Head Neck Surg. 2007; 133:131-134
The Role of the General Dental Practitioner in the Detection of Squamous Cell Carcinoma of the Maxillary Antrum Andreas Chatzipantelis Stephen James Brown Alastair Campbell Dental Update 2024 45:1, 707-709.
Authors
AndreasChatzipantelis
BDS, MFDS, MSc, LLM
Dental Core Trainee in Restorative Dentistry, Charles Clifford Dental Hospital of Sheffield, UK
Antral squamous cell carcinoma (SCC) is a relatively uncommon head and neck malignancy. Fewer than 400 cases are reported annually in the UK. As it is uncommon and often shows slow progression, it can be misdiagnosed in the early stages. This report describes a case involving a 52-year-old patient who presented at the emergency department of a district hospital complaining of facial swelling and recent dental issues. Further investigation revealed the presence of a mass in the right maxillary antrum, subsequently confirmed as SCC on histology. Significant pathology may be the underlying cause of symptoms which appear trivial. Persistent symptoms in the absence of a reasonable cause should raise suspicion.
CPD/Clinical Relevance: A general dental practitioner is likely to be the initial point of contact of patients with maxillary antrum malignancies of the maxillary sinus; identification of suspicious signs and symptoms can help in early detection and treatment.
Article
Squamous cell carcinoma (SCC) of the maxillary antrum is an uncommon malignancy of the head and neck. Cancer Research UK reports that fewer than 400 patients are diagnosed each year with SCC of the maxillary sinus, corresponding to just 0.2% of cancer cases in the UK.1 In this case report, an SCC is presented located in the maxillary sinus, with initial symptoms resembling dental-related pathology. Finally, when a general dental practitioner should consider referral to secondary care will be discussed.
Case report
A 52-year-old male presented at A&E in a Yorkshire Hospital with a right-sided infra-orbital swelling. He complained of 3–4 weeks of pain which had slowly progressed to a swelling. He also reported the loss of a tooth from the same region. Medically, he was fit and well, a smoker of 6–10 cigarettes per day and he consumed 40 units alcohol per week. He was employed as a joiner.
The patient initially reported his symptoms to his general dental practitioner (GDP) and received dental intervention. This included extraction of the UR4 (but with fracture and retention of the apices), which at that time was considered attributable to the swelling. During a subsequent appointment at the dentist, incision and drainage of an intra-oral swelling was performed, along with a prescription of antibiotics. The swelling failed to improve and the patient elected to attend A&E.
During attendance at A&E, the patient complained of right-sided mild facial swelling in the infra-orbital area, tender and non-fluctuant without change of colour or other signs of cellulitis. Sensory nerve function was intact. Intra-orally, there was buccal swelling around the UR4 apical area, which was tender to palpation. The patient did not present with any associated general symptoms, such as pyrexia or rigors, and there were no palpable facial/cervical lymph nodes. There were no additional remarkable intra-oral findings.
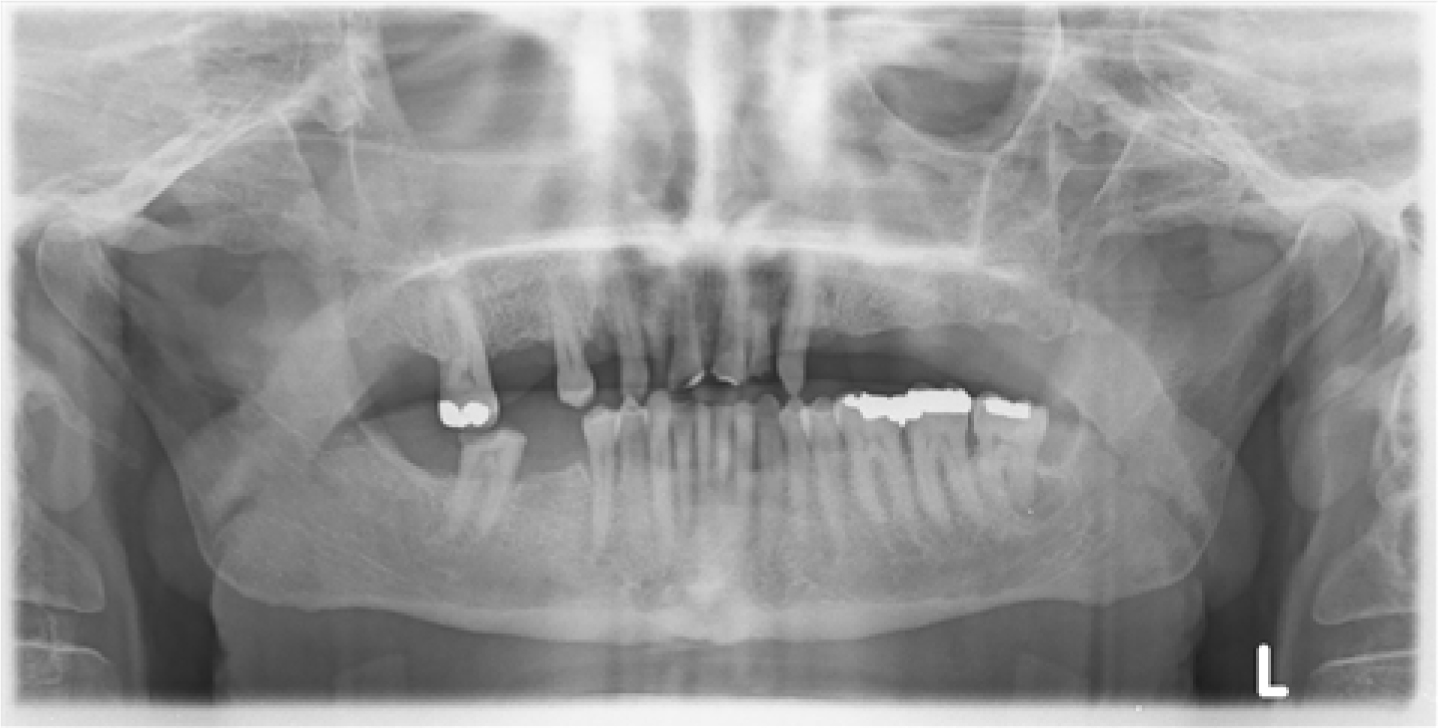
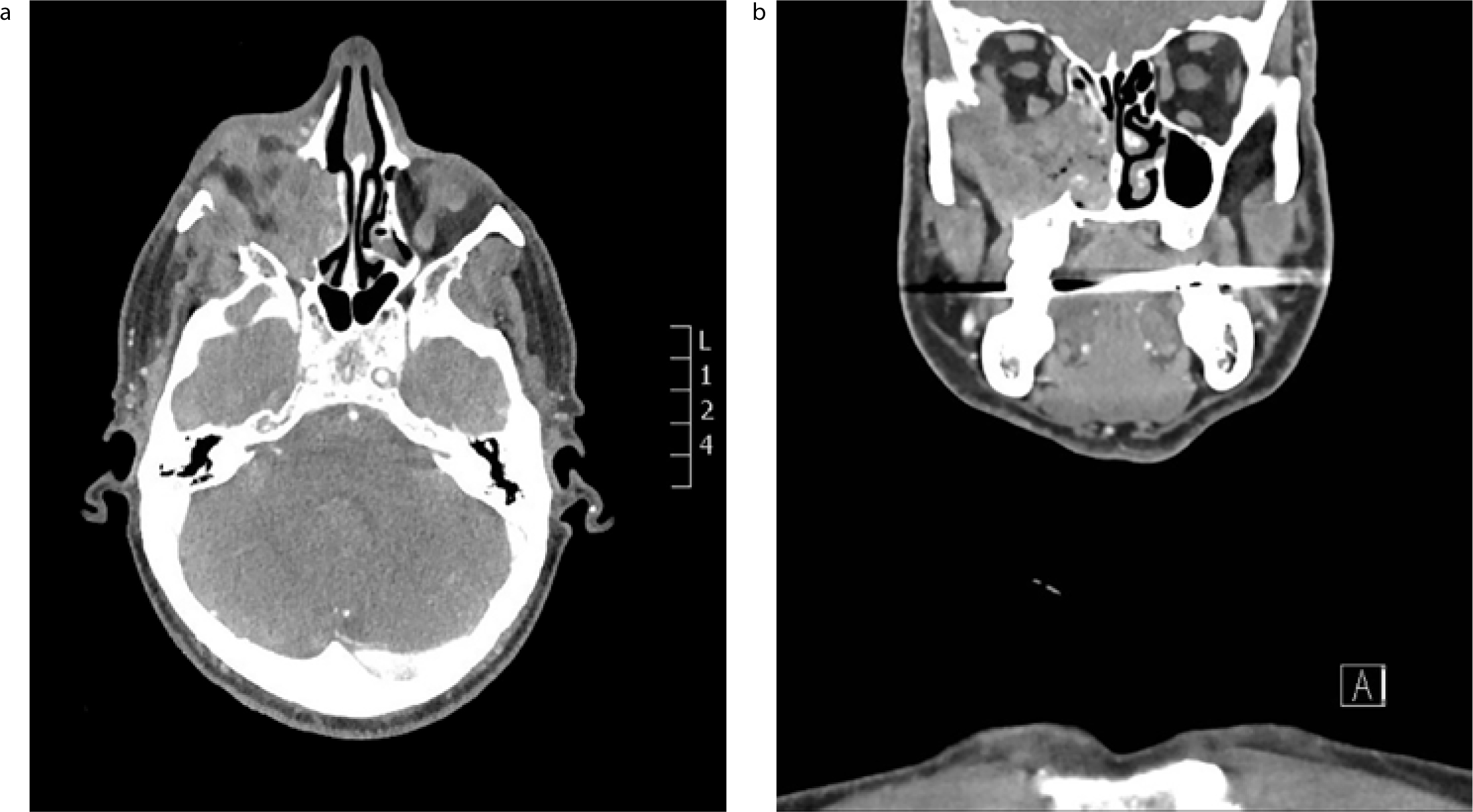
An orthopantomograph was taken and this suggested the presence of retained apices of UR4, so incision for drainage was performed intra-orally, but no pus discharged (Figure 1). The patient was reviewed one week afterwards in the outpatient department, and found to have an increase of the swelling with loss of sensation in the maxillary trigeminal nerve distribution. An urgent computerized tomography (CT) scan revealed the existence of a mass in the right maxillary sinus. CT findings included invasion, with aggressive bone destruction of adjacent structures, including the floor and lateral wall of the maxillary sinus. The tumour had invaded superiorly through the orbital floor, medially into the nasal cavity and postero-laterally into the infratemporal fossa (Figure 2).
Figure 1. OPG showing loss of definition of the right infra-orbital rim and the sinus floor with irregular bone levels and opacification of the sinus cavity.Figure 2. CT showing heterogeneous mass present in the right maxillary antrum with destruction of the lateral and medial sinus wall and invasion through the orbital floor: (a) axial plane; (b) coronal plane.
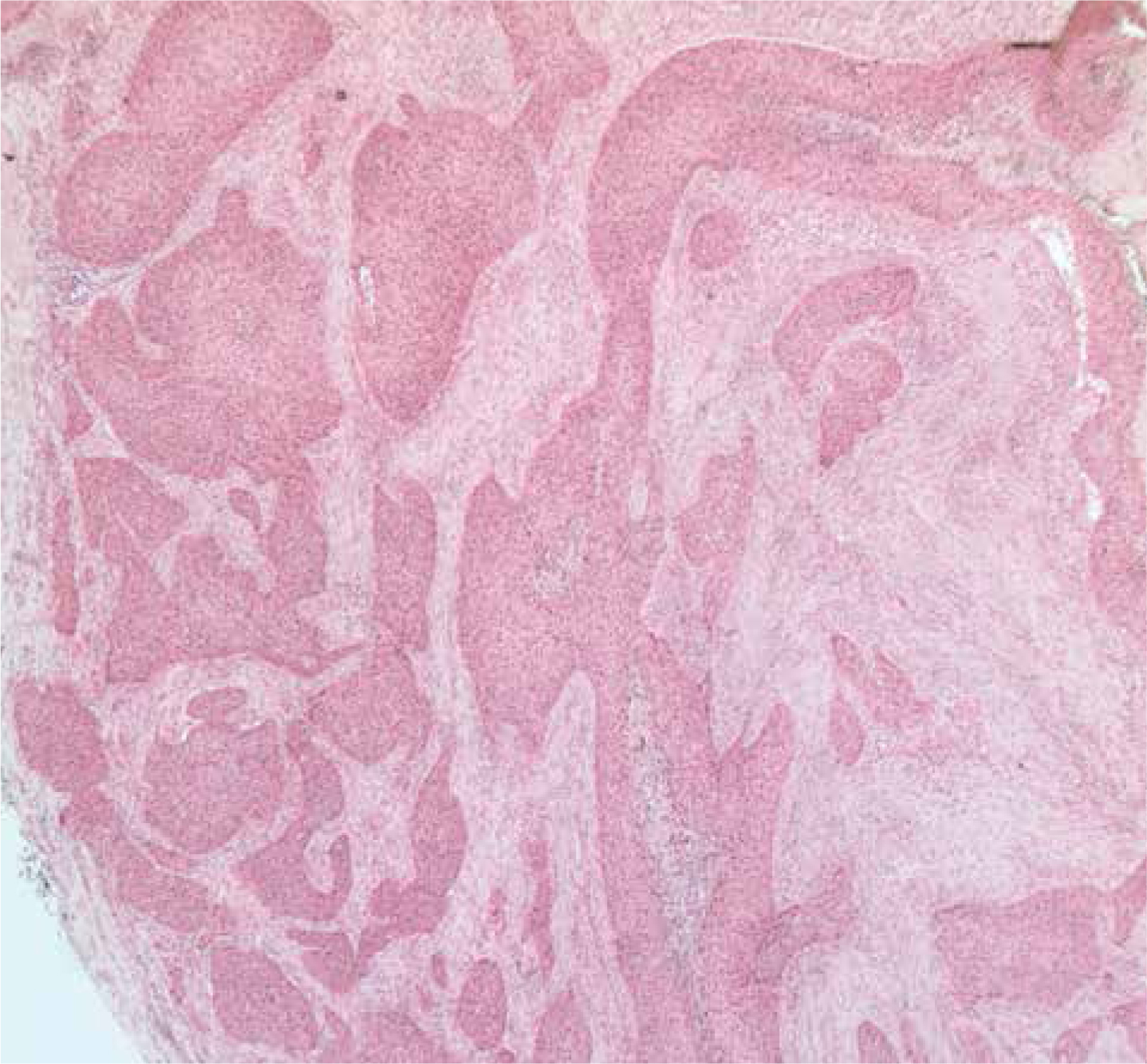
Incisional biopsy of the mass (via the swelling in the buccal sulcus) was reported as a moderately differentiated, focally keratinizing, squamous cell carcinoma (Figure 3). This was staged as T4b N0 M0 SCC of the right maxillary sinus.
Figure 3. Histology: mucosa infiltrated by strands and islands of moderately differentiated squamous cell carcinoma. Focal keratinization is seen and there is a lack of host inflammatory response to the tumour cells.
Discussion
Squamous cell carcinoma of the maxillary sinus is an uncommon cancer. It accounts for 0.1-0.2% of all cancers2 and just 1–3% of head and neck cancers.3 However, SCC is the pathology of 50–70% of sinus malignancies.2
Maxillary SCC can present with a number of different clinical signs or symptoms, some of which can be misdiagnosed as pathology of dental origin, especially in the early stages.4 Often, the first point of contact for a patient with SCC in the sinus will be with a general dental practitioner because of the similarity of the initial symptoms with those of dental infection.5 Poor oral hygiene and neglected dentition may also reinforce the perception that the symptoms have an odontogenic cause. Further to this, initial symptoms can also misleadingly be attributed to other benign pathologies of the sinuses, such as sinusitis or inflammatory sinonasal polyps.6 In late stages, the mass can cause more significant symptoms, such as trismus, paraesthesia, epistaxis or proptosis, all of which should be considered red flags for prompt referral (Table 1).7
Common Symptoms
Dental:
Dental pain
Intra-oral swelling
Tooth mobility
Trismus
Nose:
Blockage
Mucus secretion
Epistaxis
Cheek:
Sensory neuropathy (infra-orbital nerve) that may present as:
anaesthesia
altered sensation
neuropathic pain
Eye:
Bulging
Watering
Reduced acuity/vision loss/double vision
Restricted movement
Proptosis
Other Symptoms:
Facial pain
Facial lump/growth
Symptoms from the ear
Palpable facial/cervical lymph nodes
Unfortunately, the patient often presents noticeable or significant symptoms only in the late stages as the cavity of the sinus allows the tumour to extend to a significant size unobstructed before causing any symptoms through its destructive properties.8,9
When the tumour starts to invade the underlying tissues of the sinus lining, more prominent symptoms will present, including pain and extra-oral swelling. Further symptoms may also include dental pain, tooth mobility, intra-oral swelling or a combination of the above. Paraesthesia of the infra-orbital nerve, nasal congestion, sensory alteration, restriction to ocular mobility and proptosis are more significant symptoms in late stages of the malignancy.7
Lymph node metastasis is relatively uncommon in maxillary sinus malignancies. This is due to the limited connection of the maxillary sinus with the lymphoid system. This should be kept in mind during the examination.10
Radiographically, the maxillary sinuses are often included on intra-oral periapical radiographs (PAs) and always on orthopantomographs (OPTs). In the initial stages, the findings may not be specific; in more advanced stages, the infra-orbital rim and/or the sinus floor, nasal floor and alveolar process may present a noticeable loss of definition.11
The general dental practitioner is expected to identify incidental abnormal findings on routine dental radiographs. Careful interpretation of plain films and more advanced imaging (such as CBCT) is essential. Further to the medical concerns for the patient, there are potential litigation issues in cases of failure to detect non-dental pathology in such imaging.12
Suspicion should also be raised when, in the presence of symptoms, there is no evident dental pathology in the area. If the dental history of the patient is unremarkable, the presence of unexplained symptoms should be investigated thoroughly.4
Furthermore, it is also important for a dental practitioner to be able to identify patients that have high risk factors for such sinister pathology. Antral SCC has well-established risk factors, including smoking and work-place exposures, chemical exposure, etc (Table 2).7,13,14 It also has a predilection for males.2,15
Common Exposures
Work placement exposure related with specific chemical exposure
wood dust
leather dust
chromium
nickel
cloth fibres
mineral oils
Smoking
The majority of maxillary sinus malignancies are reported in the late stages, affecting long-term prognosis. The anatomical considerations in the region makes surgical resection challenging, with potential significant adverse effects to adjacent structures such as the eyes (necessitating orbital exenteration), nose, the relevant cranial nerves and even the brain if the tumour extends through the skull base.7,15
The 5-year survival rate is around 50%, but is variable with stage at detection.16 Early detection significantly improves survival outcome, especially if there is no nodal involvement. If diagnosis occurs in late stages, the long-term prognosis is poor.2,14,15,16
Conclusion
Squamous cell carcinomas of the maxillary sinus are uncommon, and patients usually only report tangible symptoms in their late stages. It is very likely that the initial point of contact will be with the general dental practitioner. The rarity of the malignancy makes prompt detection challenging. GDPs are required to record a thorough history, examination and all relevant investigations. Persistence of symptoms in the absence of other evident dental or medical pathology should raise suspicion and escalation should be considered. Finally, a dental practitioner should also take into consideration incidental findings which can appear during regular radiographic examinations and be especially vigilant when interpreting specialized imaging, such as OPT and CBCT. If unsure, he/she should seek specialist advice early. Early escalation is of paramount importance for improving long-term prognosis for these patients.