Chapple ILC. Hypophosphatasia: dental aspects and mode of inheritance. J Clin Periodontol. 1993; 20:615-622
Rathbun JC. Hypophosphatasia: a new developmental anomaly. Am J Dis Child. 1948; 75:822-831
Fraser D. Hypophosphatasia. Am J Med. 1957; 22:730-746
Mornet E. Hypophosphatasia. Orphanet J Rare Dis. 2007; 2
Pauli RM, Modaff P, Sipes SL, Whyte MP. Mild hypophosphatasia mimicking severe osteogenesis imperfecta in utero: bent but not broken. Am J Med Genet. 1999; 86:434-438
Kozlowski K, Sutcliffe J, Barylak A, Harrington G, Kemperdick H, Nolte K Hypophosphatasia. Pediatr Radiol. 1976; 5:103-117
Mornet E. Hypophosphatasia. Orphanet J Rare Dis. 2007; 2
Brittain JM, Oldenburg TR, Burkes EJ. Odontohypophosphatasia: report of two cases. ASDC J Dent Child. 1975; 43:106-111
Eastman JR, Bixler D. Clinical, laboratory, and genetic investigations of hypophosphatasia: support for autosomal dominant inheritance with homozygous lethality. J Craniofac Genet Dev Biol. 1982; 3:213-234
Cheung WS. A mild form of hypophosphatasia as a cause of premature exfoliation of primary teeth: report of two cases. Pediatr Dent. 1987; 9:49-52
Bloch-Zupan A. Hypophosphatasia: diagnosis and clinical signs – a dental surgeon perspective. Int J Paediatr Dent. 2016; 26:426-438
Beumer J, Trowbridge HO, Silverman S, Eisenberg E. Childhood hypophosphatasia and the premature loss of teeth: a clinical and laboratory study of seven cases. Oral Surg Oral Med Oral Pathol. 1973; 35:631-640
Eberle F, Hartenfels S, Pralle H, Käbisch A. Adult hypophosphatasia without apparent skeletal disease: “odontohypophosphatasia “ in four heterozygote members of a family. Klin Wochenschr. 1984; 62:371-376
Grewal PS, Gupta KP. Prosthetic rehabilitation of a young patient with Hypophosphatasia – a review and case report. Contemp Clin Dent. 2012; 3
Sutcliffe P. Extrinsic tooth stains in children. Dent Pract Dent Rec. 1967; 17:175-179
Chapple ILC, Thorpe GHG, Smith JM, Saxby MS, Glenwright HD, Green A Hypophosphatasia: a family study involving a case diagnosed from gingival crevicular fluid. J Oral Pathol Med. 1992; 21:426-431
Van den Bos T, Handoko G, Niehof A, Ryan LM, Coburn SP, Whyte MP Cementum and dentin in hypophosphatasia. J Dent Res. 2005; 84:1021-1025
Olsson A, Matsson L, Blomquist HK, Larsson Å, Sjödin B. Hypophosphatasia affecting the permanent dentition. J Oral Pathol Med. 1996; 25:343-347
Reibel A, Manière M-C, Clauss F, Droz D, Alembik Y, Mornet E Orodental phenotype and genotype findings in all subtypes of hypophosphatasia. Orphanet J Rare Dis. 2009; 4
Baab D, Weinstein P. Longitudinal evaluation of a self-inspection plaque index in periodontal recall patients. J Clin Periodontol. 1986; 13:313-318
Watanabe H, Umeda M, Seki T, Ishikawa I. Clinical and laboratory studies of severe periodontal disease in an adolescent associated with hypophosphatasia. A case report. J Periodontol. 1993; 64:174-180
Plagmann HC, Kocher T, Kuhrau N, Caliebe A. Periodontal manifestation of hypophosphatasia. A family case report. J Clin Periodontol. 1994; 21:710-716
Lynch CD, Ziada HM, Buckley LA, O'Sullivan VR, Aherne T, Aherne S. Prosthodontic rehabilitation of hypophosphatasia using dental implants: a review of the literature and two case reports. J Oral Rehabil. 2009; 36:462-468
Professor in Paediatric Dentistry, Faculty of Dentistry, The University of Hong Kong, 2/F, Prince Philip Dental Hospital, 34 Hospital Road, Hong Kong, P R China
Hypophosphatasia has a wide clinical spectrum ranging from premature loss of primary teeth to neonatal death. The premature loss of primary teeth in a child with an otherwise unremarkable history may be the first sign of a more significant underlying disease. This report illustrates the role of the dental practitioner in facilitating the diagnosis of hypophosphatasia.
CPD/Clinical Relevance: This report outlines the signs and symptoms essential to facilitate the diagnosis of hypophosphatasia by the dental practitioner.
Article
Hypophosphatasia is characterized by a defect in bone and tooth mineralization and a deficiency in bone and serum alkaline phosphatase activity. It is an inborn error of metabolism with a wide clinical spectrum, ranging from premature loss of primary teeth to neonatal death.1 The term ‘hypophosphatasia’ was first used by Rathbun in 1948, who described the case of a young boy who died at two months of age from what appeared to be a severe form of rickets with weight loss and low levels of alkaline phosphatase.2 The prevalence of hypophosphatasia of this severity is estimated to be one in 100,000, based on paediatric hospital records in the USA.3 However, the incidence of moderate forms of hypophosphatasia is largely unknown and expected to be much higher.4
Hypophosphatasia may be expressed through a number of clinical presentations ranging from stillbirth with skeletal hypomineralization to premature loss of teeth in the absence of systemic and/or skeletal abnormalities. There are six recognized clinical forms of hypophosphatasia,4 categorized primarily on the age at the time of diagnosis. These are summarized in Table 1. Previous reports have illustrated a range in clinical presentations for hypophosphatasia with varying inheritance patterns.5,6,7 However, the role of the dental practitioner in diagnosing the condition, particularly in young children, is often less discussed.
Clinical Form
Inheritance
Bone Symptoms
Dental Symptoms
Clinical Diagnosis
Perinatal lethal
AR
Hypomineralization
na
Radiographs
Osteochondral spurs
Prenatal benign
AD
Bowing of long bones
na
Ultrasonography
Benign post-natal
Clinical examination
Infantile
AR
CraniosynostosisHypomineralization
Premature loss of deciduous teeth
Clinical examinationBiology (serum AP activity, PEA and PLP)
This clinical report demonstrates the importance of a comprehensive dental history and the value of the dental practitioner in initiating the diagnosis of hypophosphatasia.
Clinical report
Case 1
A general dental practitioner referred a 22-month-old boy to the paediatric dental clinic due to the loss of his mandibular primary anterior teeth. The teeth had shed spontaneously with no history of dental trauma. The two teeth, LRA and LLA, had exfoliated with one being lost at 18 months and the other at the age of 22 months, respectively. The patient was the only child in the family and was born prematurely (31 weeks) with an extra pulmonary artery and a cardiac septal defect at birth that spontaneously closed.
Clinical and radiographic examination confirmed the patient to be in his primary dentition, with teeth LRA and LLA missing, with no other dental abnormalities (Figure 1). Therefore a provisional diagnosis of hypophosphatasia was made and the patient was referred for biochemical testing, which revealed abnormally low levels of serum alkaline phosphatase (Table 2). Subsequently, the patient was diagnosed to have a mild form of hypophosphatasia without any short stature, skeletal deformities, bone pain or skeletal fractures.
Figure 1. Panoramic radiograph of a 22-month-old boy (Case 1) demonstrating missing teeth LRA and LLA and an age appropriate dentition.
Case Number
Serum alkaline phosphatase (145–420 U/L)
Urine hydroxyproline (60–160 umol/mmol)
Urine phosphoethanolamine (2–17 umol/mmol)
Case 1
90 U/L
223 umol/mmol
63.3 umol/mmol
Case 2
90 U/L
215 umol/mmol
60.3 umol/mmol
Case 2
A general dental practitioner referred a 33-month-old boy to the paediatric dental clinic due to the ‘loss of upper and lower primary teeth’. The patient was fit and healthy with an unremarkable medical history and normal physical proportions. He weighed 16 kilograms (75th percentile), was 103 centimetres tall (90th percentile) and had a head circumference of 51.5 centimetres (75th percentile). The primary teeth had shed spontaneously with no history of dental trauma. The LRA had exfoliated at 18 months of age, followed by the remaining three mandibular incisors (LRB, LLA, LLB) at approximately 24 months of age and the URA exfoliated at 30 months of age (Figure 2).
Figure 2. A 33-month-old boy (Case 2) presenting with prematurely exfoliated tooth URA showing an intact root with a distinct lack of cementum: (a) palatal aspect; (b) labial aspect.
When investigating his family medical history, his paternal great grandmother had type II diabetes and both his paternal grandparents were hypertensive. The patient's parents had no history of fractures and his mother had scoliosis as a teenager. However, both parents were of otherwise normal stature, none reporting having any dental problems. Notably, the patient's elder brother also experienced early exfoliation of his primary incisor tooth. The patient's mother had been well throughout pregnancy and the patient was born uneventfully at full-term and through normal vaginal delivery weighing 3.15 kilograms.
The patient did not exhibit dolicocephaly or kyphoscoliosis. He did not have skeletal deformities or joint swellings and the development of his hair and nails were normal. Examination of his heart, chest, abdomen, nervous system, along with renal and liver function tests, were all within normal limits. Furthermore, his developmental milestones were unremarkable.
Clinical examination revealed the patient to be in his primary dentition with generalized extrinsic black stains and no clinical evidence of carious lesions (Figure 3). Radiographic investigation found the permanent tooth germs developing appropriate to his chronologic age with no evidence of URA, LLA, LLB, LRA and LRB missing (previously exfoliated) (Figure 4). Therefore, a provisional diagnosis of hypophosphatasia was made and the patient was referred for biochemical testing which revealed low levels of serum alkaline phosphatase (Table 2). Subsequently, the patient was diagnosed with a mild form of hypophosphatasia without any short stature, skeletal deformities, bone pain or skeletal fractures.
Figure 3. Frontal clinical view of a 33-month-old boy (Case 2), demonstrating generalized black extrinsic stains and premature loss of teeth URA, LLA, LLB, LRA and LRB.Figure 4. Panoramic radiograph of a 33-month-old boy (Case 2) demonstrating missing teeth URA, LLA, LLB, LRA and LRB.
Case 3
Case 3 is a 5-year-old boy, who is an elder sibling of Case 2, with a history of early exfoliation of LLA (exfoliated at 3 years of age). Radiographic investigation revealed missing LLA with no evidence of developing teeth LL4, LL5, LR4, LR5 (Figure 5). Following biochemical testing, he was diagnosed with a mild form of hypophosphatasia, similar to that of his brother.
Figure 5. Panoramic radiograph of a 5-year-old boy (Case 3) demonstrating premature exfoliation of tooth LLA and no radiographic evidence of developing teeth LL4, LL5, LR4 and LR5.
Discussion
The cases described in this report exhibited similar characteristics, namely, premature exfoliation of unresorbed primary teeth, elevated levels of urine phosphoethanolamine, and lower levels of serum alkaline phosphatase levels. This facilitated the diagnosis to be a mild form of hypophosphatasia with no associated skeletal abnormalities.
Terminology
Brittain and co-workers suggested the term of odonto-hypophosphatasia to describe mild cases of hypophosphatasia in which premature exfoliation of primary teeth was the main clinical manifestation.8 It has been proposed that both odonto-hypophosphatasia and hypophosphatasia are the same genetic condition represented as varying phenotypes related to gene dosage.9 Cheung suggested that it may be more appropriate to refer to the conditions as hypophosphatasia with or without premature exfoliation of teeth.10 Although previous studies have suggested an association with severe dental caries, due to hypercalcaemia resulting in a poor appetite and eating problems,11 this association was not observed in the patients described in this report.12,13,14 Conversely, the presence of extrinsic black staining was found in Case 2. Previous studies have suggested a correlation with similar extrinsic staining and a low caries experience in children.15
Biochemical testing
Total serum alkaline phosphate is markedly reduced in hypophosphatasia, as illustrated in the present clinical reports and this is the major indicator for hypophosphatasia. Serum alkaline phosphatase levels may also be tested via gingival crevicular fluid, as described by Chapple et al.16 Notably, the serum alkaline phosphatase level could be only slightly lower than normal, or even within the normal range, and several tests may be necessary for accurate assessment. An elevated concentration of phosphoethanolamine in the urine is the secondary indicator for hypophosphatasia. Furthermore, an increased pyridoxal 5’-phosphate is a definitive and more sensitive marker for diagnosing hypophosphatasia.
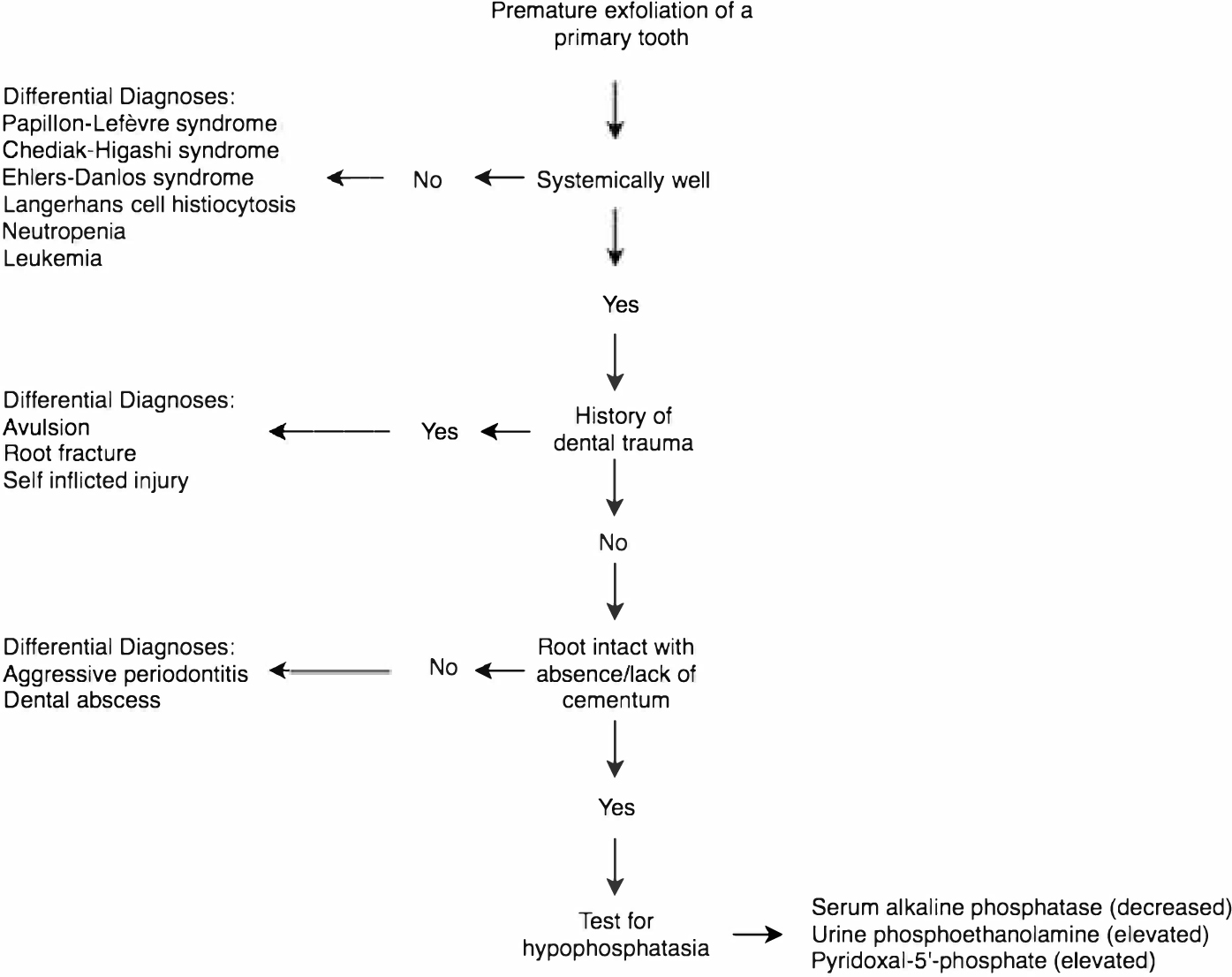
Biochemical testing does not always distinguish hypophosphatasia from other skeletal diseases, such as osteogenesis imperfecta, rickets and achondrogenesis. In observing the premature exfoliation of a primary tooth, it is crucial to consider and investigate for other differential diagnoses, such as Papillon-Lefėvre syndrome, Chediak-Higashi syndrome, Ehlers-Danlos syndrome, Langerhans' cell histiocytosis, neutropenia, leukemia, trauma, self-inflicted injury and localized aggressive periodontitis. A flowchart to guide the dental practitioner in facilitating the diagnosis of hypophosphatasia is illustrated in Figure 6.
Figure 6. Flowchart showing the diagnostic process and differentials in the diagnosis of hypophosphatasia.
Alternatively, screening for mutations in the tissue non-specific alkaline phosphatase gene may assist in confirming the diagnosis of hypophosphatasia. Genomic sequencing may detect approximately 95% of mutations in a severe case of hypophosphatasia. However, patients with milder forms often carry only one mutated allele, which is likely due to heterozygous expression of the disease.7
Dental manifestations, management and long-term consequences
A common diagnostic feature of hypophosphatasia is the premature loss of primary teeth, usually before the age of 3, particularly in the mandibular incisor region. These primary teeth exfoliate spontaneously with their roots intact and minimal or no cementum present.17 The first sign is often tooth mobility, which leads the patient and his/her family to seek dental advice. Therefore, the dental practitioner is frequently one of the first healthcare professionals to identify and facilitate the diagnosis of hypophosphatasia following appropriate investigation, particularly in young children.11
Literature on the longer-term consequences of hypophosphatasia remains equivocal. Reduced alveolar bone support, abnormal root resorption and premature loss of permanent teeth have all been reported as long-term consequences of hypophosphatasia.18 In this report, only Case 3 demonstrates hypodontia in the permanent dentition as well as premature loss of primary teeth. Given the young age at the time of diagnosis, the long-term consequences on the permanent dentition may be under reported. Therefore, long-term follow-up of these cases is required.
The prosthetic replacement of primary teeth in young children is not often undertaken due to the possibility of interfering with growth and development of the dental arches. However, treatment options to replace the missing permanent teeth are usually recommended. The options include fixed or partial prostheses or dental implants, with or without orthodontic therapy.
When performing restorative treatment in patients with hypophosphatasia, the increased size of the pulp chamber must be considered to avoid inadvertent pulp exposure.19 Dental abnormalities, such as bulbous crowns with cervical constriction, wide pulp chambers, taurodontism, short roots, enamel defects and altered eruption of teeth, may also be present and should be investigated.11
Several authors have also described an association between hypophosphatasia and periodontitis.20,21,22 Hypophosphatasia commonly affects the cementum and periodontal ligament rather than the quality of the alveolar bone. The use of dental implants to replace lost teeth is a viable option. Lynch and co-workers reported on the long-term success of dental implants in a young adult with hypophosphatasia.23 Nevertheless, a multidisciplinary approach, with both short- and long-term treatment options, is advisable to meet the specific needs of the patient.
Conclusion
The cases described in this report illustrate the role of the dental practitioner in facilitating the diagnosis of hypophosphatasia. Therefore, a sound knowledge of the physiologic norms and variations in developing children is essential to identify such otherwise unnoticed conditions. Nevertheless, the premature loss of primary teeth in a child with an otherwise unremarkable history may be the first sign of a more significant underlying disease. Children with hypophosphatasia require regular review for the maintenance of good oral hygiene and the establishment of preventive regimens to minimize periodontal risk factors. The cases presented in this report exhibit milder forms of hypophosphatasia which may lead to difficulties in diagnosis and it is possible that many similar cases may have been overlooked and consequently have either been misdiagnosed or never been diagnosed.