Celikoglu M, Miloglu O, Kazanci F. Frequency of agenesis, impaction, angulation, and related pathologic changes of third molar teeth in orthodontic patients. J Oral Maxillofac Surg. 2010; 68:990-995
Renton T, Yilmaz Z. Profiling of patients presenting with posttraumatic neuropathy of the trigeminal nerve. J Orofac Pain. 2011; 25:333-344
Assael LA. Coronectomy: a time to ponder or a time to act?. J Oral Maxillofac Surg. 2004; 62:1445-1446
Cheung LK, Leung YY, Chow LK, Wong MC, Chan EK, Fok YH. Incidence of neurosensory deficits and recovery after lower third molar surgery: a prospective clinical study of 4338 cases. Int J Oral Maxillofac Surg. 2010; 39:320-326
Haug RH, Perrott DH, Gonzalez ML, Talwar RM. The American Association of Oral and Maxillofacial Surgeons age-related third molar study. J Oral Maxillofac Surg. 2005; 63:1106-1114
Lopes V, Mumenya R, Feinmann C, Harris M. Third molar surgery: an audit of the indications for surgery, post-operative complaints and patient satisfaction. Br J Oral Maxillofac Surg. 1995; 33:33-35
Smith JG, Elias LA, Yilmaz Z, Barker S, Shah K, Shah S The psychosocial and affective burden of posttraumatic neuropathy following injuries to the trigeminal nerve. J Orofac Pain. 2013; 27:293-303
Elias LA, Yilmaz Z, Smith JG, Bouchiba M, van der Valk RA, Page L PainDETECT: a suitable screening tool for neuropathic pain in patients with painful post-traumatic trigeminal nerve injuries?. Int J Oral Maxillofac Surg. 2014; 43:120-126
Gerlach KL, Hoffmeister B, Walz C. [Dysesthesia and anesthesia of the mandibular nerve following dental treatment]. Dtsch Zahnarztl Z. 1989; 44:970-972
Renton T. Oral surgery: part 4. Minimising and managing nerve injuries and other complications. Br Dent J. 2013; 215:393-399
Kipp DP, Goldstein BH, Weiss WW Dysesthesia after mandibular third molar surgery: a retrospective study and analysis of 1,377 surgical procedures. J Am Dent Assoc. 1980; 100:185-192
Black CG. Sensory impairment following lower third molar surgery: a prospective study in New Zealand. NZ Dent J. 1997; 93:68-71
Gϋlicher D, Gerlach KL. Sensory impairment of the lingual and inferior alveolar nerves following removal of impacted mandibular third molars. Int J Oral Maxillofac Surg. 2001; 30:306-312
Tay AB, Go WS. Effect of exposed inferior alveolar neurovascular bundle during surgical removal of impacted lower third molars. J Oral Maxillofac Surg. 2004; 62:592-600
Queral-Godoy E, Valmaseda-Castellon E, Berini-Aytes L, Gay-Escoda C. Incidence and evolution of inferior alveolar nerve lesions following lower third molar extraction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 99:259-264
Blondeau F, Daniel NG. Extraction of impacted mandibular third molars: postoperative complications and their risk factors. J Can Dent Assoc. 2007; 73
Ghaeminia H, Meijer GJ, Soehardi A, Borstlap WA, Mulder J, Berge SJ. Position of the impacted third molar in relation to the mandibular canal. Diagnostic accuracy of cone beam computed tomography compared with panoraly. Int J Oral Maxillofac Surg. 2009; 38:964-971
Szalma J, Lempel E, Jeges S, Olasz L. Darkening of third molar roots: panoralic associations with inferior alveolar nerve exposure. J Oral Maxillofac Surg. 2011; 69:1544-1549
Kim JW, Cha IH, Kim SJ, Kim MR. Which risk factors are associated with neurosensory deficits of inferior alveolar nerve after mandibular third molar extraction?. J Oral Maxillofac Surg. 2012; 70:2508-2514
Guerrero ME, Nackaerts O, Beinsberger J, Horner K, Schoenaers J, Jacobs R Inferior alveolar nerve sensory disturbance after impacted mandibular third molar evaluation using cone beam computed tomography and panoraly: a pilot study. J Oral Maxillofac Surg. 2012; 70:2264-2270
Smith WP. The relative risk of neurosensory deficit following removal of mandibular third molar teeth: the influence of radiography and surgical technique. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013; 115:18-24
Selvi F, Dodson TB, Nattestad A, Robertson K, Tolstunov L. Factors that are associated with injury to the inferior alveolar nerve in high-risk patients after removal of third molars. Br J Oral Maxillofac Surg. 2013; 51:868-873
Nguyen E, Grubor D, Chandu A. Risk factors for permanent injury of inferior alveolar and lingual nerves during third molar surgery. J Oral Maxillofac Surg. 2014; 72:2394-2401
Deppe H, Mucke T, Wagenpfeil S, Kesting M, Linsenmeyer E, Tolle T. Trigeminal nerve injuries after mandibular oral surgery in a university outpatient setting – a retrospective analysis of 1,559 cases. Clin Oral Invest. 2015; 19:149-157
Jain N, Thomas S, Prabhu S, Jain S, Pathak AD, Pillai A Influence of tooth sectioning technique and various risk factors in reducing the IAN injury following surgical removal of an impacted mandibular third molar. Oral Maxillofac Surg. 2015; https://doi.org/10.1007/s10006-015-0540-3
Piecuch JF. What strategies are helpful in the operative management of third molars?. J Oral Maxillofac Surg. 2012; 70:S25-S32
Bruce RA, Frederickson GC, Small GS. Age of patients and morbidity associated with mandibular third molar surgery. J Am Dent Assoc. 1980; 101:240-245
Hasegawa T, Ri S, Shigeta T, Akashi M, Imai Y, Kakei Y Risk factors associated with inferior alveolar nerve injury after extraction of the mandibular third molar – a comparative study of preoperative images by panoraly and computed tomography. Int J Oral Maxillofac Surg. 2013; 42:843-851
Leung YY, Cheung LK. Correlation of radiographic signs, inferior dental nerve exposure, and deficit in third molar surgery. J Oral Maxillofac Surg. 2011; 69:1873-1879
Leung YY, Cheung LK. Risk factors of neurosensory deficits in lower third molar surgery: a literature review of prospective studies. Int J Oral Maxillofac Surg. 2011; 40:1-10
Rood JP, Shehab BA. The radiological prediction of inferior alveolar nerve injury during third molar surgery. Br J Oral Maxillofac Surg. 1990; 28:20-25
Rud J. Third molar surgery: perforation of the inferior dental nerve through the root. Tandlaegebladet. 1983; 87:659-667
Alantar A, Roisin-Chausson MH, Commissionat Y, Aaron C, Barda L, Debien J Retention of third molar roots to prevent damage to the inferior alveolar nerve. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995; 80
Renton T, Hankins M, Sproate C, McGurk M. A randomised controlled clinical trial to compare the incidence of injury to the inferior alveolar nerve as a result of coronectomy and removal of mandibular third molars. Br J Oral Maxillofac Surg. 2005; 43:7-12
Howe G, Poynton H. Prevention of damage to the inferior alveolar nerve during extraction of mandibular third molars. Br Dent J. 1960; 109
Kaeppler G. Conventional cross-sectional tomographic evaluation of mandibular third molars. Quintessence int. 2000; 31:49-56
Blaeser BF, August MA, Donoff RB, Kaban LB, Dodson TB. Panoralic risk factors for inferior alveolar nerve injury after third molar extraction. J Oral Maxillofac Surg. 2003; 61:417-421
Ohman A, Kivijarvi K, Blomback U, Flygare L. Pre-operative radiographic evaluation of lower third molars with computed tomography. Dent Maxillofac Radiol. 2006; 35:30-35
Susarla SM, Sidhu HK, Avery LL, Dodson TB. Does computed tomographic assessment of inferior alveolar canal cortical integrity predict nerve exposure during third molar surgery?. J Oral Maxillofac Surg. 2010; 68:1296-1303
Katakam SK, Shankar U, Thakur D, Reddy TP, Hari KR, Janga D. Comparison of orthopantomography and computed tomography image for assessing the relationship between impacted mandibular third molar and mandibular canal. J Contemp Dent Pract. 2012; 13:819-823
Eyrich G, Seifert B, Matthews F, Matthiessen U, Heusser CK, Kruse AL 3-Dimensional imaging for lower third molars: is there an implication for surgical removal?. J Oral Maxillofac Surg. 2011; 69:1867-1872
Umar G, Obisesan O, Bryant C, Rood JP. Elimination of permanent injuries to the inferior alveolar nerve following surgical intervention of the “high risk” third molar. Br J Oral Maxillofac Surg. 2013; 51:353-357
Xu GZ, Yang C, Fan XD, Yu CQ, Cai XY, Wang Y Anatomic relationship between impacted third mandibular molar and the mandibular canal as the risk factor of inferior alveolar nerve injury. Br J Oral Maxillofac. 2013; 51:e215-219
Pathak S, Mishra N, Rastogi MK, Sharma S. Significance of radiological variables studied on orthopantomogram to predict post-operative inferior alveoler nerve paresthesia after third molar extraction. J Clin Diagnost Res (JCDR). 2014; 8:ZC62-64
Peker I, Sarikir C, Alkurt MT, Zor ZF. Panoraly and cone-beam computed tomography findings in preoperative examination of impacted mandibular third molars. BMC Oral Health. 2014; 14
Maglione M, Costantinides F, Bazzocchi G. Classification of impacted mandibular third molars on cone-beam CT images. J Clin Exp Dent. 2015; 7:e224-231
Huang CK, Lui MT, Cheng DH. Use of panoraly to predict postsurgical sensory impairment following extraction of impacted mandibular third molars. J Chin Med Assoc (JCMA). 2015; 78:617-622
Matzen LH, Christensen J, Hintze H, Schou S, Wenzel A. Influence of cone beam CT on treatment plan before surgical intervention of mandibular third molars and impact of radiographic factors on deciding on coronectomy vs surgical removal. Dent Maxillofac Radiol. 2013; 42
Neves FS, de Almeida SM, Boscolo FN, Haiter-Neto F, Alves MC, Crusoe-Rebello I Risk assessment of inferior alveolar neurovascular bundle by multidetector computed tomography in extractions of third molars. Surg Radiol Anat (SRA). 2012; 34:619-624
Bell GW. Use of dental panoramic tomographs to predict the relation between mandibular third molar teeth and the inferior alveolar nerve. Radiological and surgical findings, and clinical outcome. Br J Oral Maxillofac Surg. 2004; 42:21-27
de Melo Albert DG, Gomes AC, do Egito Vasconcelos BC, de Oliveira e Silva ED, Holanda GZ. Comparison of orthopantomographs and conventional tomography images for assessing the relationship between impacted lower third molars and the mandibular canal. J Oral Maxillofac Surg. 2006; 64:1030-1037
Maegawa H, Sano K, Kitagawa Y, Ogasawara T, Miyauchi K, Sekine J Preoperative assessment of the relationship between the mandibular third molar and the mandibular canal by axial computed tomography with coronal and sagittal reconstruction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 96:639-646
Monaco G, Montevecchi M, Bonetti GA, Gatto MR, Checchi L. Reliability of panoraly in evaluating the topographic relationship between the mandibular canal and impacted third molars. J Am Dent Assoc. 2004; 135:312-318
Ludlow JB, Davies-Ludlow LE, Brooks SL, Howerton WB. Dosimetry of 3 CBCT devices for oral and maxillofacial radiology: CB Mercuray, NewTom 3G and i-CAT. Dent Maxillofac Rad. 2006; 35:219-226
Hashimoto K, Kawashima S, Kameoka S, Akiyama Y, Honjoya T, Ejima K Comparison of image validity between cone beam computed tomography for dental use and multidetector row helical computed tomography. Dent Maxillofac Radiol. 2007; 36:465-471
Loubele M, Guerrero ME, Jacobs R, Suetens P, van Steenberghe D. A comparison of jaw dimensional and quality assessments of bone characteristics with cone-beam CT, spiral tomography, and multi-slice spiral CT. Int J Oral Maxillofac Implants. 2007; 22:446-454
Cespedes-Sanchez JM, Ayuso-Montero R, Mari-Roig A, Arranz-Obispo C, Lopez-Lopez J. The importance of a good evaluation in order to prevent oral nerve injuries: a review. Acta odontol Scand. 2014; 72:161-167
Pippi R. A case of inferior alveolar nerve entrapment in the roots of a partially erupted mandibular third molar. J Oral Maxillofac Surg. 2010; 68:1170-1173
Shahidi S, Zamiri B, Bronoosh P. Comparison of panoraly with cone beam CT in predicting the relationship of the mandibular third molar roots to the alveolar canal. Imag Sci Dent. 2013; 43:105-109
Tolstunov L. The quest for causes of inferior alveolar nerve injury after extraction of mandibular third molars. J Oral Maxillofac Surg. 2014; 72:1644-1646
Park W, Choi JW, Kim JY, Kim BC, Kim HJ, Lee SH. Cortical integrity of the inferior alveolar canal as a predictor of paresthesia after third-molar extraction. J Am Dent Assoc. 2010; 141:271-278
Tantanapornkul W, Okochi K, Bhakdinaronk A, Ohbayashi N, Kurabayashi T. Correlation of darkening of impacted mandibular third molar root on digital panoramic images with cone beam computed tomography findings. Dent Maxillofac Radiol. 2009; 38:11-16
Ueda M, Nakamori K, Shiratori K, Igarashi T, Sasaki T, Anbo N Clinical significance of computed tomographic assessment and anatomic features of the inferior alveolar canal as risk factors for injury of the inferior alveolar nerve at third molar surgery. J Oral Maxillofac Surg. 2012; 70:514-520
Dawood A, Patel S, Brown J. Cone beam CT in dental practice. Br Dent J. 2009; 207:23-28
Ghaeminia H. Coronectomy may be a way of managing impacted third molars. Evid Based Dent. 2013; 14:57-58
Martin A, Perinetti G, Costantinides F, Maglione M. Coronectomy as a surgical approach to impacted mandibular third molars: a systematic review. Head Face Med. 2015; 11
Long H, Zhou Y, Liao L, Pyakurel U, Wang Y, Lai W. Coronectomy vs. total removal for third molar extraction: a systematic review. J Dent Res. 2012; 91:659-665
Leung YY, Cheung LK. Safety of coronectomy versus excision of wisdom teeth: a randomized controlled trial. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 108:821-827
Renton T. Update on coronectomy. A safer way to remove high risk mandibular third molars. Dent Update. 2013; 40:362-368
Dolanmaz D, Yildirim G, Isik K, Kucuk K, Ozturk A. A preferable technique for protecting the inferior alveolar nerve: coronectomy. J Oral Maxillofac Surg. 2009; 67:1234-1238
Hatano Y, Kurita K, Kuroiwa Y, Yuasa H, Ariji E. Clinical evaluations of coronectomy (intentional partial odontectomy) for mandibular third molars using dental computed tomography: a case-control study. J Oral Maxillofac Surg. 2009; 67:1806-1814
O'Riordan BC. Coronectomy (intentional partial odontectomy of lower third molars). Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 98:274-280
Pogrel MA, Lee JS, Muff DF. Coronectomy: a technique to protect the inferior alveolar nerve. J Oral Maxillofac Surg. 2004; 62:1447-1452
Leung YY, Cheung LK. Safety of coronectomy versus excision of wisdom teeth: a randomized controlled trial. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 108:821-827
Frenkel B, Givol N, Shoshani Y. Coronectomy of the mandibular third molar: a retrospective study of 185 procedures and the decision to repeat the coronectomy in cases of failure. J Oral Maxillofac Surg. 2015; 73:587-594
Agbaje JO, Heijsters G, Salem AS, Van Slycke S, Schepers S, Politis C Coronectomy of deeply impacted lower third molar: incidence of outcomes and complications after one year follow-up. J Oral Maxillofac Res. 2015; 6
Leung YY, Cheung LK. Long-term morbidities of coronectomy on lower third molar. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2016; 121:5-11
Monaco G, De Santis G, Pulpito G, Gatto MR, Vignudelli E, Marchetti C. What are the types and frequencies of complications associated with mandibular third molar coronectomy? A follow-up study. J Oral Maxillofac Surg. 2015; 73:1246-1253
Patel V, Sproat C, Kwok J, Beneng K, Thavaraj S, McGurk M. Histological evaluation of mandibular third molar roots retrieved after coronectomy. Br J Oral Maxillofac Surg. 2014; 52:415-419
Leung YY, Cheung LK. Coronectomy of the lower third molar is safe within the first 3 years. J Oral Maxillofac Surg. 2012; 70:1515-1522
R (on the application of Rose) v Thanet Clinical Commissioning Group. 2014;
Lubbers HT, Matthews F, Damerau G, Kruse AL, Obwegeser JA, Gratz KW Anatomy of impacted lower third molars evaluated by computerized tomography: is there an indication for 3-dimensional imaging?. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011; 111:547-550
Walker JE. Inferior dental nerve perforating root. A case report. Br Dent J. 1968; 124:467-468
Mishra YC. Entrapment of the neurovascular bundle by the roots of an impacted mandibular third molar – a case report. Br J Oral Maxillofac Surg. 1987; 25:261-264
Motamedi MH. Impacted lower third molar and the inferior alveolar nerve. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 87:3-4
Ecuyer J, Debien J. [Surgical deductions]. Actual Odontostomatol (Paris). 1984; 38:695-702
Knutsson K, Lysell L, Rohlin M. Postoperative status after partial removal of the mandibular third molar. Swed Dent J. 1989; 13:15-22
Zallen RD, Massoth NA. Antibiotic usage for coronectomy: is it necessary?. J Oral Maxillofac Surg. 2005; 63
Leung YY, Cheung LK. New approach in extraction of impacted wisdom teeth. The Hong Kong Med Diary. 2010; 15:8-9
Tolstunov L, Javid B, Keyes L, Nattestad A. Pericoronal ostectomy: an alternative surgical technique for management of mandibular third molars in close proximity to the inferior alveolar nerve. J Oral Maxillofac Surg. 2011; 69:1858-1866
Wong C, Collin J, Hughes C, Thomas S. Surgical emphysema and pneumomediastinum after coronectomy. Br J Oral Maxillofac Surg. 2015; 53:763-764
Leizerovitz M, Leizerovitz O. Reduced complications by modified and grafted coronectomy vs. standard coronectomy – a case series. Alpha Omegan. 2013; 106:81-89
Patel V, Sproat C, Samani M, Kwok J, McGurk M. Unerupted teeth associated with dentigerous cysts and treated with coronectomy: mini case series. Br J Oral Maxillofac Surg. 2013; 51:644-649
Patel V, Kwok J, Sproat C, McGurk M. To retrieve or not to retrieve the coronectomy root – the clinical dilemma. Dent Update. 2013; 40:370-376
Chalmers E, Goodall C, Gardner A. Coronectomy for infraoccluded lower first permanent molars: a report of two cases. J Orthod. 2012; 39:117-121
Coulthard P, Bailey E, Esposito M, Furness S, Renton TF, Worthington HV. Surgical techniques for the removal of mandibular wisdom teeth. Cochrane Database Syst Revs. 2014; 7
Risk assessment of M3Ms and decisions on ordering a CBCT and prescribing a coronectomy Tara Renton Dental Update 2024 44:10, 707-709.
Authors
TaraRenton
BDS, MDSc, PhD
Professor of Oral Surgery, King's College London; Honorary Consultant in Oral Surgery, King's College Hospital NHS Foundation Trust and Guy's and St Thomas' NHS Foundation Trust, London
Coronectomy is a procedure that is evidence based in order to prevent inferior alveolar nerve injury (IANI) related to surgery for high risk mandibular third molars (M3Ms). The justification for undertaking coronectomy rather than third molar removal is based upon risk assessment of the M3M, for which one has no clear parameters. There is international acceptance of this technique, however, there are many outstanding issues relating to the criteria for prescription, investigation and decision-making for this procedure including: risk factors for IAN injury/indications for cone beam CT scan (CBCT); indications for coronectomy as seen on plain films and then on to CBCT; complications/contra-indications of coronectomy; legal issues; and recommendations.
Thus this personal opinion paper was aimed at highlighting the complexities around investigating, prescribing, patient consent and undertaking coronectomies, in order to assist the clinician in making surgical decisions faced with an ever changing evidence base and lack of specific criteria.
CPD/Clinical Relevance: Third molar surgery is one of the most common surgical procedures undertaken on the NHS. Up to 48% of patients are reported to be at higher risk of inferior alveolar nerve injury after assessment with dental pantomograms, but the numbers do vary depending upon the patient cohort. This paper aims to unravel some of the conflicting evidence and attempts to provide some useful practical tips on the optimal management of these patients.
Article
Mandibular third molar (M3M) extractions are the most often performed procedures in the field of oral surgery.1 M3M is a challenging surgical procedure due to close proximity to anatomical structures such as the IAN and lingual nerves. Inferior alveolar nerve injury (IANI) is avoidable and should be prevented where possible as trigeminal sensory neuropathies result in long-term chronic pain and disability for 70% of patients affected.2
Coronectomy (partial tooth removal, deliberate vital root retention and partial odontectomy) has become a routine oral surgical procedure with the aim to minimize risk of IANI in relation to the removal of high-risk M3Ms. Coronectomy, a coded surgical procedure both in US (OMFS Category service 2 D7251) and Japan, has been defined as a method of removing the crown of a tooth but leaving the roots untouched, which may be intimately related with the IAN, so that the possibility of nerve injury is reduced. At the inception of this technique, questions were raised3 and, despite its increasing popularity and acceptance, many concerns remain
In an attempt to address these issues, this personal opinion paper is presented and aims to highlight the necessary research in this field.
Risk factors for IAN injury/indications for CBCT
The main justification for considering a coronectomy is based upon the assessed risk of IANI related to M3M surgery and its prevention. It is well recognized that, after dry socket, nerve injury is the most common complication related to M3Ms.
Neurosensory impairment is a common complication of extraction of impacted M3Ms, and the incidence ranges from 0.35% to 8.4%.4,5,6 The consequences of sensory nerve injury are unpleasant and result in a negative effect on a patient's life, often with medicolegal repercussions. The consequences for the patient with IANI include:
70% of IANI patients experience a combination of neuropathic pain, anaesthesia and altered sensation with mechanical allodynia and hyperalgesia.2
Reduced daily function is reported, relating to; eating, speaking, drinking, kissing and socializing, resulting in an adverse impact on daily life, mainly due to elicited pain.2
Severe psychological impact due to pain, altered daily function and the iatrogenic nature of the injury, results in psychological sequelae including:
Thus psychological therapies, including cognitive behavioural, acceptance or mindfulness strategies (in conjunction with medical management for chronic neuropathic pain) are often recommended.
The subsequent sensory disturbance due to IANI, may occur after direct or indirect trauma during M3M removal.9 For example, it may result from direct compression of the nerve leading to blunt nerve trauma by instruments or the elevated roots. The IAN may be damaged by rotating instruments used for the surgical procedure or after IAN regional anaesthetic block injections.10,11 The IANI incidence varies depending upon the study design, cohort selected and risk level of those M3Ms included in the design (Table 1).11,12,13,14,15,16,17,18,19,20,21,22,23,24,25
1,106 impacted mandibular third molars were removed from 687 patientsIANI 3.6%IANI at 6 months was 0.91%Risk factors: patient's age, the development of the roots, the degree of impaction, and the radiographic position of the IDC
53 third molars from 40 patientsIAN was exposed in 23Nerve injury occurred in 5 patientsThe lingual position of the inferior dental canal was significantly associated with IAN injuryNo difference in prediction by PAN or CBCT
0.35% of patients developed IAN deficitDepth of impaction was related to IANI (P < 0.001).Post-operative recovery from IANAt 6 months 67% of IANI had resolved
Retrospective study of 537 M3M extractions in 318 patientsIANI occurred in 25/235 (11%)Excessive haemorrhage during extraction; and a close relationship of the roots to the IAN were associated with a significantly higher risk (odds ratio 43.77) of IANI
Study group 104 cases/135 controlsIANI rate of 0.81% of patientsIn the absence of specific radiographic signs, the risk of neurosensory deficit of the IAN could be negligible
IANI 1/79 and 1/86 CBCT not better than panoral in pre-assessmentSignificant differences in making a correct diagnosis of neurovascular bundle exposure at the extraction of impacted teeth were found between the 2 modalities (P = 0.029)
Temporary IANI 11%Increased risk when root apices were intimate to the ID nerve and lowest (0.9%) when close or distant from the nervePermanent IANI 0.4% per tooth ID vessel bleed associated with 20% IANI
149 subjects who had 235 M3MsMean age 31 years IANI in 25/235 (11%) of M3MsIncreasing age >25 P = 0.04; Female P = 0.05Cortical perforation in the IDC as assessed CT (IDC) P = 0.03
11,599 lower third molars were removed in 6,803 patientsIANI 0.68%Risk factors for permanent IANI were increasing age, surgery performed by staff dentists, type of anaesthesia, and mesioangular impactions
169 LM3s (115 patients)IAN injury was observed in 7.7% M3MsAll exhibited absence of corticationA dumbbell-shaped IDC was considered a useful predictor for IAN injury (sensitivity, 69.2%; specificity, 84.6% [P = 0.005])
Specific risk factors related to developing IANI during M3M surgery
Patient age
It is well understood that patients over the age of 25 years are more likely to be affected by persistent IANI when the nerve is damaged during oral surgery.26 The reasons for this might be that the healing ability decreases with increasing age and that more bone is usually removed owing to completely formed roots or increased bone mineralization.27 Blondeau and Daniel recommended that prophylactic M3M extraction should be avoided in patients aged 24 years or older because of a high possibility of complications, such as permanent neurosensory deficits, infection, and alveolitis.16
Gender
Females have been reported to be more at risk of persistent IANI.22
Surgeon experience
The prevalence of IANI is also dependent on the surgeon experience and the methods used.27,28,29
Eruption status and depth of impaction
A literature review of 32 prospective articles29 highlighted that unerupted M3M status was the strongest indicator for IANI (erupted 0.32% deficit; partially erupted 0.67% deficit; unerupted 3% deficit). Interestingly, the depth of impaction and the pattern of impaction illustrated no statistical differences. However, this is likely due to the different systems used to describe impaction pattern and depth.
Type of impaction
In 2013, Smith presented a clinical study on 1,000 patients, removing 1,589 impacted M3Ms.21 The incidence of IAN neurosensory deficit was highest with horizontal impaction (4.7%) and lowest when the M3Ms were vertically impacted (0.9%). However, the difference between each type of impaction was not statistically significant (P > 0.01).
Intra-operative nerve exposure and bleeding during surgery
Clinical exposure of the IAN neurovascular bundle during surgery may notify the surgeon about an increased risk of post-operative IANI, resulting in a 20% risk of post-operative paraesthesia, with a 70% chance of recovery within one year.14 IAN bleed during surgery is also reported to be associated with increased IANI.21
Indications for coronectomy as seen on plain films and then on CBCT
Orthopantomography
The radiographic position of the M3M in relationship to the Inferior dental canal (IDC) has been shown to be useful in assessing the risk of damage to the IAN following extraction. Plane film radiographic signs on panorals indicative of possible IAN risk include:
Roots of tooth crossing the superior border of the IDC21 (Figure 1);
Diversion of the IDC (darkening of the root)30,31 (Figure 2);
Figure 1. Clinical view of a panoral illustrating M3M roots of tooth crossing the IDC.Figure 2. Clinical view of a panoral illustrating diversion of the IDC (darkening of the M3M root) with CBCT confirming proximal relationship of M3M roots and IDC.Figure 3. Clinical view of a panoral illustrating interruption of the lamina dura associated with the M3M roots.Figure 4. Clinical view of a panoral illustrating juxta-apical area associated with the M3M roots.
Most studies (Table 2)29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49 report a combination of panoral risk factors predisposing to IANI. A study performed21 on a total of 12,842 patients who underwent extraction of the M3M, using univariate logistic regression analysis, reported that the significant risk panoral factors for panoral IANI were:
Case controlled study of 8 IANI cases and 17 controls with panoral assessment to ascertain radiographic risk factorsPositive radiographic signs associated with IAN injury (P < .0001) included:
Panoramic views of 88 M3Ms followed by CT examinations with respect to presence of a dark band across the rootsThe course of the IDC was:
31% buccal, 33% lingual, 26% inferior and 10% inter-radicular
Tooth contact with the IDC in 94% and with the lingual cortex in 86%
In 23%, grooving of the root by the IDC was judged to be present In 63% of the cases where a dark band across the roots was observed on panorals CT revealed grooving of the root
80 M3Ms retrospective cohort study sample included patients considered at risk of IANI. Primary outcome variable was intra-operative visualization
52 third molars (64.1%) had evidence of loss of cortical integrity
Loss of cortical integrity had a high sensitivity (≥0.88) but low specificity
A cortical defect size ≥3 mm was associated with an increased risk for intra-operative IAN visualization with a high sensitivity and specificity (≥0.82 or = 0.49) as a diagnostic test for IAN visualization.
A prospective study of 30 patients with 42 impacted M3Ms comparison of OPG and CT in localizing IAN and M3M:
z-value >1.5 in darkening of roots (1.98)
deflection of root (2.00)
interruption of z-value = 0 in narrowing of IDC and dark, bifid apexes. Also it showed P-value <0.05 in all the radiographic signs except narrowing of the IDC and and dark and bifid apexes
515 surgical M3Ms with 3-dimensional (3D) imagingIANI 9.4%. Predictors of IANI were:
narrowing of the IDC (OR, 4.95; P < .0001)
contact IAN and the root (OR, 5.05; P = .0008)
fully formed roots (OR, 4.36; P = .045)
IAN lingual course with (OR, 6.64; P = .0013)
without (OR, 2.72; P = .007) perforation of the cortical plate
an intra-root (OR, 9.96; P = .003) position of the IAN
multivariate analysis showed narrowing of the IDC (adjusted OR, 3.69; 95% CI, 1.88 to 7.22; P = .0001) and direct contact (adjusted OR, 3.10; 95% CI, 1.15 to 8.33; P = .025) to be the strongest independent predictors
50 high risk M3Ms were assessed by means of panorals and then compared to CBCT 78% of teeth showing darkening of roots in the panoral showed loss of cortication on CBCT in 68% of cases66% of cases displayed thinning or loss of the lingual cortical plate, 33% of which were related to the IDC and 30% the tooth itself
537 extractions in 318 patients High risk (CBCT). The risk IANI is increased if M3Ms intersect the IDC, on its buccal side and loss of the white line of the IDC or the diversion of the IDC; excessive haemorrhage during extraction; and a close relationship of the roots to the IDC. Many panoramic findings were not consistent with CT findings (275 of 440 teeth; 62.5%)
The ratio of IANI in the extraction group with a lingual position between the roots was significantly higher (P < 0.05) than that in the group with other positions
100 impacted M3Ms. Four of seven radiological findings including; grooving of roots, hooked roots, bifid roots and obliteration of white line are significantly related to post-operative IANI
a significant difference in number of roots detected on DPR versus CBCT images
darkening of the roots and interruption of the white line on DPR images were significantly associated with the presence of contact between the IMTM and the IDC on CBCT images
Eight different classes of M3M relationship with IDC (classes 0–7) and six of them (classes 1–6) were subdivided in two subtypes (subtypes A–B):
mainly buccal or apical course of the IDC followed by lingual position and inter-radicular one
no differences have resulted in terms of anatomic relationship between males and females apart from a higher risk of real contact without corticalization of the IDC when the IAN had a lingual course for female group
younger patients showed an increased rate of direct contact with a reduced calibre of the IDC and/or without cortication
120 M3Ms. Seven radiographic signs were the predictor variables: (1) darkening of the root(s); (2) interruption of the radio-opaque line of the IDC; (3) diversion of the IDC; (4) dark and bifid apex; (5) deflection of the root(s); (6) narrowing of the IDC; and (7) narrowing of the root(s). Three of the radiographic signs were statistically associated with IAN sensory impairment (P < 0.05):
interruption of the radio-opaque line [sensitivity = 0.92, specificity = 0.45, positive predictive value (PPV) = 0.17, negative predictive value (NPV) = 0.02]; (2)
diversion of the IDC (sensitivity = 0.77, specificity = 0.84, PPV = 0.37, NPV = 0.03);
narrowing of the IDC (sensitivity = 0.69, specificity = 0.65, PPV = 0.19, NPV = 0.05). However, the other four radiographic signs, namely darkening of the root(s), dark and bifid apex, deflection of the root(s), and narrowing of the root(s), were not statistically associated with IAN sensory impairment (P > 0.05).
186 M3Ms treatment plan did no change for 164 cases (88%), but changed for 22 teeth (12%) after CBCT:
direct contact between the third molar and the IDC had the highest impact on deciding on coronectomy [odds ratio (OR) = 101.8, P < 0.001].
direct contact was not a sufficient factor, however;
lumen narrowing of the IDC (OR = 38.9–147.2, P < 0.001) and
IDC positioned in a bending or a groove in the root complex (OR = 32.8, P = 0.016) were additional IDC-related factors for deciding on coronectomy
CBCT influenced the treatment plan for 12%. Direct contact in combination with narrowing of the IDC lumen and IDC positioned in a bending or a groove in the root complex observed in CBCT images were significant factors for deciding on coronectomy
178 M3Ms with one or more of the specific radiographic signs:
IANI (5.1%) was significantly greater than that in the control group (0.56%; P = 0.01)
darkening of root and displacement of the IDC by the root were radiographic signs significantly related to IDN exposure (P = 0.001 and P = 0.019, respectively)
darkening of the root was the only sign significantly related to a post-operative IDN deficit (P = 0.016). When two or more radiographic signs were present, the risk of a post-operative IDN deficit was significantly increased (P = 0.001)
33 individuals (63 M3M extraction) pre-operative evaluation by MDCT before extraction. Significant association between IAN exposure and the tomographic relationship between the roots of third molars and the IDC (P = 0.015). Conventionally, all cases of IANI and haemorrhage occurred when the roots of the third molar presented in an at-risk relationship with the IDC, however, this association was not statistically significant (P > 0.05)
a statistically significant association was found between the lingual course of the mandibular IDC and IAN exposure (P = 0.03)
In contrast, another study, using multivariate logistic regression analysis, revealed that the significant risk factors were:
A darkening of the root;
Deflection of the root;
Narrowing of the root;
Dark and bifid apexes of the root; and
Narrowing of the IDC.
The narrowing of the root was the most significant type of superimposition, followed by dark and bifid apexes of the root.30,31
A recent study4 reported the radiographic risk factors significantly (P < 0.001) related to IANI to be:
Diversion of IDC by M3M root 30% deficit;
Darkening of M3M root 11.6% deficit;
Deflected M3M root by IDC 4.6% deficit.
In a later study,30 the same authors evaluated 178 M3Ms in 118 patients, where radiographic risk factors were identified including:
Darkening of root;
Abrupt narrowing root;
Interruption one line or both lines of lamina dura (LD);
Displacement of the IDC by M3M roots.
Of M3M radiographs examined, 65.7% illustrated a minimal of one radiographic signs, 27.5% two signs and 5.1% demonstrated three signs. Both darkening of root (P < 0.001) and deviation of IDC (P < 0.019) predicted the highest risk for IANI exposure during surgery. Darkening of root ONLY was a radiographic sign of significantly increased IANI risk (P = 0.016). If there was more than one radiographic risk factor, IANI was a significantly increased risk (P = 0.005). Intra-operative IAN exposure (P < 0.001) was also significantly related to exposure, 16.2% IANI deficit versus non-exposed 1.1% IANI deficit. Intra-operatively, 13.5% of M3Ms resulted in IAN exposure; of those with IAN exposure, 20.6% had post-operative IANI.
However, the presence or absence of these radiographic signs does not always determine the possibility of IANI, indicating that the panoral does not have high diagnostic accuracy in the assessment of risk in surgical extractions of lower M3Ms.50/51 When the radiological marker on the panoral indicates that there is a close relationship between the M3M and the IDC, additional investigation using computed tomography (CT) may be recommended to verify the relationship in a three-dimensional view.38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53 This 3D imaging allows the surgeon to further scrutinize the need for modified surgery or intentional coronectomy,10 potentially resulting in a change of practice in up to 90–95% of cases. M3M removal was at ‘high risk’ based on panoral radiography, which would otherwise be recommending a coronectomy. The use of cone beam computed tomography (CBCT) for high-risk M3M may also be associated with reduced morbidity to the IAN.41,42 CBCT has been introduced to improve conventional CT because it reduces the radiation dose, offers high spatial resolution, and decreases costs.54 The software associated with cone-beam CT provides better imaging quality of M3Ms and their surrounding structures compared with conventional hospital-grade CT scans.55,56
CBCT has higher radiation dose and added expense compared with panoral, however, the new generation of CBCT scans have reduced radiation dose (less than twice as much as a panoral radiograph) and lowered costs, but these may not be available internationally.
There are several important CBCT radiographic signs that may indicate a higher risk to the IAN and assist the clinician in case selection for coronectomy57
M3M root perforation by the IDC
If the tooth is perforated, though rare, a CBCT will confirm this, thus avoiding unnecessary nerve injury during extraction and leading to recommendation of a coronectomy.58
IDC perforation or loss of LD
Shahidi et al reported that the loss or interruption of the cortical line (LD) on the panoral, having a close correlation with proximity of the IAN to the M3M, was confirmed on a CBCT scan panoral.59 This is ‘highly suggestive of the risk of nerve injury’. Also, an IDC's LD perforation, as seen on a CBCT scan (Figure 5), can be closely correlated to darkening of the root seen on a panoral.53
Figure 5. Clinical view of the IDC's LD perforation associated with the M3M roots, as seen on a CBCT scan.
LD interruption by the root(s) or crown of the M3M.39,40,41,42
Monaco et al stated that the risk of IAN injury increased from the average of 1–5% to 20–30% when the IDC LD by roots was observed.53
The length of the IDC perforation or defect it depends on
The impaction depth and angulation of a M3M are critical.39 An IDC cortical defect length (distance) of at least 3mm on a CT scan has been associated with an increased risk for intra-operative IAN exposure.
Deformation of the IDC at the point of contact with M3M roots (Figure 6)
This may indicate proximity and risk of IANI. The intimate proximity of a M3M can modify the common oval configuration of the IDC toward a more ‘dumbbell’ or ‘tear-drop’ shape or a concave configuration.60 Invagination of the IDC or ‘compression’ (concave deformation) of the IDC can result from the proximity of root(s) of a M3M. In a second study, among 169 LM3s (115 patients), IAN injury was observed in 13 of 169 M3Ms (7.7%), and all 13 cases with IANI exhibited absence of cortication. A dumbbell-shaped IDC was considered a useful predictor for IANI (sensitivity, 69.2%; specificity, 84.6% [P = 0.005]).25
Figure 6. Clinical view of the common oval configuration to a ‘dumbbell’ IDC shape indicating proximity of the M3M roots to the IDC as seen on a CBCT scan.
CBCT prediction of nerve exposure
In a study by Neves et al,49 in all 14 cases where IAN was exposed during surgery, the pre-operative assessment by multi-detector computed tomography (MDCT) images classified the relationship between the roots of the M3Ms and the IDC as at-risk (the tooth roots invade and restrict the IDC space). There was a statistically significant relationship between IAN exposure and the relationship between the roots of the M3Ms and the IDC (P = 0.015).
Care must be taken to scrutinize the presence of bifid IDCs as, often, a smaller branch may be passing close to the M3M roots and on extraction will cause partial permanent IANI (Figure 7).46
Figure 7. Clinical view of a bifid IDC passing close to the M3M roots as seen on a CBCT scan indicating the need for coronectomy.
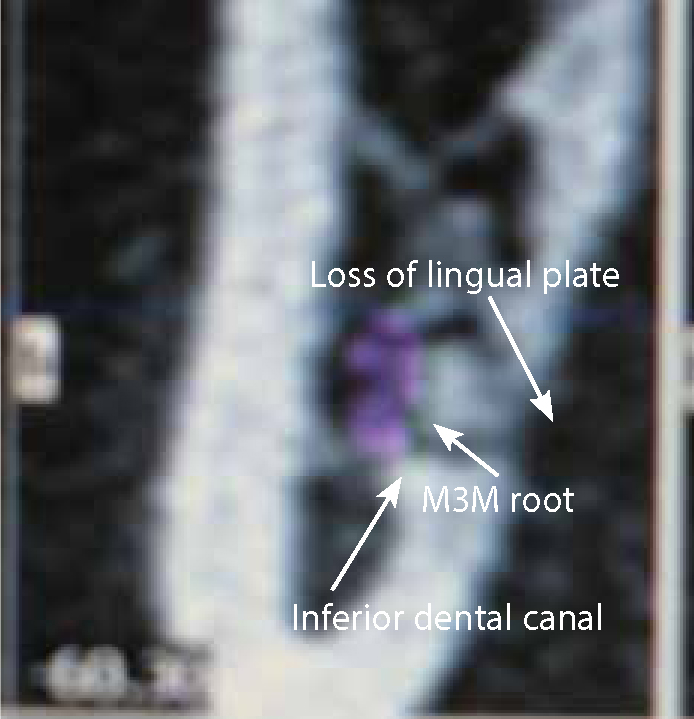
M3M roots positioned between missing lingual cortex and IDC
Of high risk M3M cases reported, 30% have a defect of the lingual cortex.42 If the M3M root is sandwiched between the IDC and lost lingual cortex, this may be a secondary decision factor to undertake a coronectomy (Figure 8).10
Figure 8. Clinical view of a M3M root sandwiched between the IDC and lost lingual cortex as seen on a CBCT scan, possibly indicating a coronectomy.
Buccal position of roots
Buccal position of roots in contact with a lingually placed IDC may be associated with increased IANI rate (Figure 9).43,61
Figure 9. Clinical view of the buccal position of the M3M roots in contact with a lingually placed IDC as seen on a CBCT scan.
Specific criteria to progress from panoral to CBCT (Table 3)
The criteria are not yet evidence based, however, based upon the existing literature, darkening of root is the only panoral radiographic sign that is significantly associated with increased IANI risk (P = 0.016). However, if there was more than one radiographic risk factor, IANI was significantly at increased risk (P = 0.005).4 The M3M roots should be proximal to (touching/passing roof and/or floor) IDC with the following features which correlate with CBCT identification of IDC proximity and M3M roots:62
Darkening of M3M root only or with;
Diversion of IDC by M3M root; OR
Deflected M3M root by IDC.
Plain Radiographic Signs Indicative of Possible IAN Risk Include:
Diversion of the IDC
Darkening of the root
Narrowing of the root/IDC
Interruption of the IDC lamina dura
Interruption of the juxta-apical area
CBCT radiographic signs if increased risk to IAN
Loss of IDC cortex (>3 mm)
Dumbbell distortion of IDC
Lingual position of IDC to roots
Perforation of tooth roots by IDC
Inter-radicular IDC with multiple roots
Undertaking a coronectomy based on a panoral alone
If 100 patients display aforementioned risk indices on a panoral, then 98 of the 100 patients will experience no permanent IANI on M3M removal, based upon the evidence presented. Conversely, if 100% of the patients undergo coronectomy, then 98 are undergoing partial tooth removal when they should have undergone extraction. Therefore, the author suggests that further risk assessment using CBCT will optimize the correct surgical choice for each patient, restricting prescription of coronectomy only to the cohort of patients at risk of permanent IANI (2%). Based upon the argument above then, in the author's opinion, all patients should undergo CBCT (as lower radiation dose as possible) to try to achieve extraction for those patients not at risk of permanent nerve injury (98%) and the choice of coronectomy for the 2% of patients who are at likely risk of IANI.
Access to CBCT
It will not always be possible to have physical or financial access to CBCT for risk assessment prior to M3M surgery. If a patient is at obvious risk, based upon the panoral findings, a decision should be agreed between patient and clinician as to whether a coronectomy should be undertaken, based upon the full understanding of the related risks of coronectomy as against the preferred removal of the M3M.
Additional information provided by CBCT compared with a plain panoral
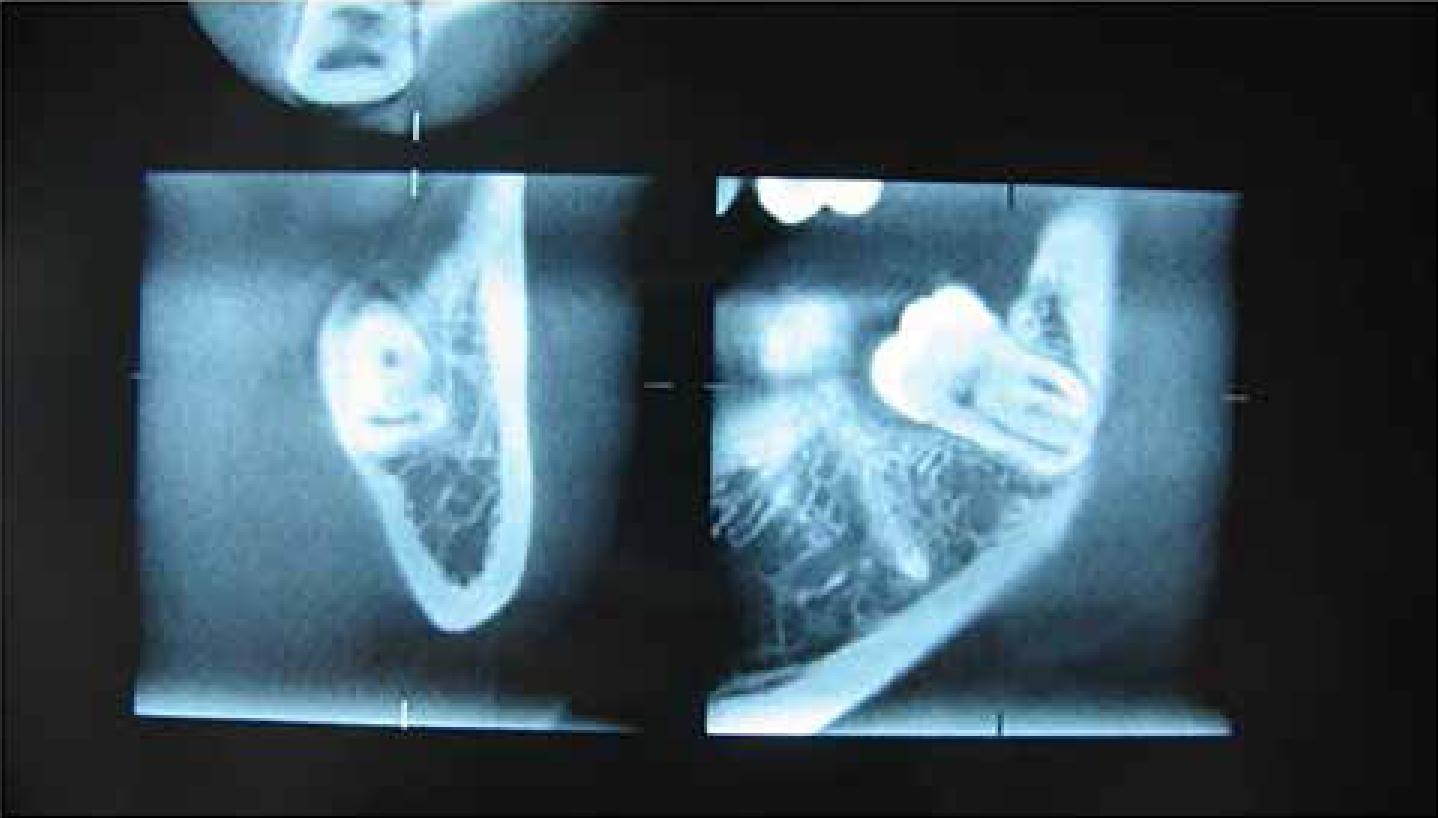
The position of the IDC in relation to the M3M roots is critical. A report of CT images of 90 high risk M3Ms reported that, within 31% of the CT images the course of the mandibular IDC was buccal, in 33% lingual, in 26% inferior and in 10% inter-radicular (the high risk group). When considering contact or distortion of the IDC adjacent to the M3M, the tooth was in contact with the mandibular IDC in 94% and with the lingual cortex in 86% of cases. In 23% of the cases, grooving of the root by the IDC was judged to be present. In 63% of the cases where a dark band across the roots was observed on panoramic radiographs, the CT revealed grooving of the root38 with cortical perforation of the IDC, correlating with darkening of the root seen on the panoramic radiography, providing relevant information for the clinician.31,61,63Figure 10 illustrates a case whereby the M3M appears to be high, based upon DPT imaging but, when assessed using a CBCT, the roots are distant to the M3M roots, allowing for removal rather than an unnecessary coronectomy in this case. In the author's experience, this represents 95–96% of cases which appear high risk on DPT but the CBCT provides sufficient information to allow removal rather than coronectomy.
Figure 10. Clinical view of CBCT scan confirming distant relationship of M3M roots to IDC despite panoral appearing high risk. Removal not coronectomy would be indicated.
Minimizing radiation when undertaking CBCT
When assessing patients before M3M extraction, a thorough clinical history and examination needs to be performed prior to radiological examination. Normally, a panoral is sufficient to show the M3M and the relationship to the IDC. However, if high risk, then CBCT is required whilst utilizing the smallest field of view (FOV) and, where compatible, reduced rotation (180° instead of 360°) or higher speed rotation have been demonstrated to minimize radiation exposure to the patient.64
The criteria on CBCT that may indicate coronectomy rather than removal
Based upon the evidence presented, the risk factors related to significant risk of IANI (Table 3) include:
Tooth root perforation by IDC: the ‘polo minted’ tooth is the single unambiguous indicator for coronectomy. This is estimated to be a rare phenomenon (Table 2);28,29,30,31,32,33,34,35,36,37,,38,39,40,41,42,43,44,45,46,47,48,49
Lingual position of the IDC in relation to the M3M roots;
Direct contact is reported to be significantly associated with IANI but usually in relation to additional CBCT findings. Multivariate analysis showed narrowing of the IAN IDC to be the strongest independent predictors of IANI;41
Decortication: a cortical defect size ≥3mm was associated with an increased risk for intra-operative IAN visualization, with a high sensitivity and specificity (≥0.82);39
Altered shape of IDC: CBCT influenced the treatment plan for 12%. Direct contact in combination with narrowing of the IDC lumen and IDC positioned in a bending or a groove in the root complex observed in CBCT images were significant factors for deciding on coronectomy.41,48
Loss of lingual cortex occurs frequently (30%) and may be a second indication for undertaking coronectomy if a root is positioned between the missing lingual cortex and the IDC.4
Complications and contra-indications for coronectomy
A coronectomy should not be undertaken on a low risk tooth unless the patient is informed that it is a bone maintenance procedure, which is likely to require a root IDC to preserve the root long term. Indications for coronectomy are based upon several criteria including:
When there is an indication for extraction;
The tooth in question has been identified as ‘High risk’ of IANI (M3M or other tooth);
The patient is healthy (medical history and social-follow-up accessibility);
Dental (vital tooth).
Contra-indications for coronectomy include the following.
Dental factors
Non vital tooth;
Active caries into the pulp, or demonstrating periapical abnormality;
M3Ms that are mobile should be excluded as they act as a mobile foreign body and become a nidus for infection or migration;
M3Ms associated with tumours;
Horizontally impacted M3Ms are more difficult to obtain a successful coronectomy due to high placement of the retained root surface in relation to the alveolus.
Medical history
Immunocompromised, with likely poor healing, is a contra-indication for coronectomy and removal is advised whereby the patient may be more at risk of infection with retention of roots.
Social and psychological factors
The patient's understanding is compromised;
Travelling/difficult access to healthcare;
Specific indications to remove the tooth. Avoidance of third molar surgery will avoid nerve injury, which is possible for non-diseased unerupted M3Ms in accordance with AAOMS 2016 Guidelines recommending active surveillance for 23% of M3Ms (http://www.aaoms.org/docs/govt_affairs/advocacy_white_papers/management_third_molar_white_paper.pdf);
Patients scheduled for future surgery involving the site.
A systematic review of four studies (two RCTs and two CCTs) involving 699 patients and 940 M3Ms report that coronectomy was converted to extraction during surgery due to root loosening or mobilization in 2.3% to 38.3% of cases. Re-operation was required in 0% to 4.9% of the coronectomy group due to persistent pain, root exposure or persistent apical infections. Root migration was only reported in three studies and ranged from 13.2% to 85.9%. Furthermore, it was reported that coronectomy can protect IANs in the extraction of M3Ms with high risk of nerve injury, as compared with total removal, and that the risk ratios of post-operative infections were similar between the two surgical modalities.65
A recent systematic review66 evaluated the clinical effectiveness of the surgical technique of coronectomy for third molar extraction in close proximity with the IAN. The authors assessed the following variables: IANI, lingual nerve injury, post-operative adverse effects, pulp disease, root migration and rate of re-operation. Ten articles qualified for the final analysis. The successful coronectomies varied from a minimum of 61.7% to a maximum of 100%. Coronectomy was associated with a low incidence of complications in terms of IANIs (0–9.5%), lingual nerve injury (0–2%), post-operative pain (1.1–41.9%) and swelling (4.6%), dry socket symptoms (2–12%), infection rate (1–9.5%) and pulp disease (0.9%). Migration of the retained roots seems to be a frequent occurrence (2–85.3%). Their conclusion was that coronectomy appears to be a safe procedure, at least in the short term, with a reduced incidence of post-operative complications.
A further systematic review67 of four studies indicated that the pooled risk ratio (coronectomy vs total removal) was 0.11 (95% CI = 0.03–0.36), 1.03 (95% CI = 0.54–1.98), 0.55 (95% CI = 0.28–1.05), and 1.14 (95% CI = 0.57–2.30) for IANIs, post-operative infection, dry socket, and pain at one week after surgery, respectively. One of these studies indicated a relatively high rate of failed coronectomy (38.3%, compared with 2.3–9.4% in others). This may have been due to a higher proportion of narrowing roots and vertical impactions leading to easier mobilization of the M3M roots. Although the rate of root migration was high (13.2–85.29%), the distances of migration were short (3.06 ± 1.67 mm), and in directions of moving away from the nerves.
Furthermore, low rates of re-operation and root exposure were reported. The authors therefore concluded that coronectomy appears superior to total removal for reducing IAN damage and could be used in clinical practice for third molar extractions with high risk of nerve injury.
Dry socket symptoms and infection
Rates for socket infection (2–12%), infection rate (1–9.5%) and pulp disease (0.9%) were reported in a systematic review of four studies.66 A randomized controlled trial involving 171 coronectomies and 178 controls reported a significantly lower pain and ‘dry socket’ incidence in the coronectomy group.68 Similar rates of ‘dry socket’ symptoms were reported by Renton.69 The established diagnostic criterion of a dry socket occurs where the blood clot fails to form or is lost from the socket post extraction.
IANI deficit
In recent years, more studies have been published, including two RCTs and a review where a lower incidence of IANIs was found compared to complete extraction of M3M.67,68,69 A further two prospective cohort studies, one case control study and one retrospective study exist.63,70,71,72 In all of these studies, a clear benefit was found regarding IANIs for high-risk M3Ms. In the two RCTs, the incidence of IANIs ranged from 0% to 0.65% for coronectomy and 5.1% to 19% in the control group where M3Ms were extracted conventionally.69 The only patient who suffered from IANI in the coronectomy group recovered after 12 months, whereas 33.3% of patients who had extraction had persistent IANI after a 12-month period. Therefore coronectomy does significantly reduce IAN deficit in relation to removal of high risk M3Ms:
Pogrel et al: no (0%) IANI injuries were seen in relation to coronectomy.73
Renton: reported no IANI injuries in relation to coronectomy 0% vs 19% removal. The high failed coronectomy rate was related to subtotal section of the crown resulting in mobilization of the roots intra-operatively. As a result the technique has been modified. As the operator is aware of the absolute high risk of IANI with scrutiny of the CBCT, it is essential not to mobilize the roots, therefore a wider groove of pulpal depth is drilled using a fissure bur (surgical drill) and the crown elevated off the roots with less force than the earlier technique.69
Leung and Cheung: 0.65% IANI rate for coronectomy versus 5.10% removal.74
Coronal root migration
Migration of the roots was identified in 80% of 116 patients and was increased in younger patients.74 In a total of 10 cases of failure, four were treated with repeat coronectomy. The other 6/173 cases were treated with re-operation (ie removal of residual roots). Immediate post-operative radiographic imaging is recommended, as well as follow-up evaluation 12 months after surgery. In addition, a repeat coronectomy is recommended for cases in which enamel retention is diagnosed in order to prevent residual roots from becoming infected.75
Root migration with eruption
Three percent at 3 years eruption and necessary removal has been reported.74 Renton reported a 2% eruption with late extraction at 5 years.69 A study of coronectomies was undertaken in 64 patients.76 The most common complication was tooth migration away from the mandibular IDC (n = 14), followed by root exposure (n = 5). Re-operation to remove the root was performed in cases with periapical infection and root exposure.
Migration of the roots was found in younger patients. In a total of 10 cases of failure, four were treated with repeat coronectomy. The other 6/173 cases were treated with re-operation (ie removal of residual roots). Immediate post-operative radiographic imaging is recommended, as well as follow-up evaluation 12 months after surgery.
Re-operation rates
Late extraction due to root migration is reported in many studies. Extraction in 3.6% of cases was necessary due to late eruption77 and 6% retained enamel.78 On removal of these roots, one study reported that there was no pathology associated with retained roots when removed.79
Repeat coronectomy is reported and successful if enamel remnants require removal.75
Re-operation was performed in 20 cases (3.26%) in order to:
- remove residual enamel (2);
- avoid chronic infection (2);
- for root exposure (13) and root removal (2.12%);
- avoid vague pain (2) resulting in roots being removed;
- do orthognathic surgery in one case and remove root.80
Legal issues
There was a National Health Service Litigation Authority (NHSLA) case that concluded that it was a breach of duty not to offer a patient with high risk M3M a coronectomy.81
The role of the oral maxillofacial radiologist
Liability issues include who should be responsible for IANI when a bifid nerve is overlooked and partial permanent IANI results after M3M removal. The surgeon must be primarily responsible for the surgery and, as a result, must be competent in reading the CBCT and reporting the risk assessment. There are additional issues regarding CBCT, including radiographic reporting of a large anatomical area and the legal responsibilities of both clinician and radiologist.64
CBCT assist in risk of IANI reduction
CBCT examination helps provide additional relevant information to assist in the treatment decision, thus facilitating selection of an appropriate case either to remove or coronect the M3M. Some authors have described minimal change in practice due to CBCT assessment.39 Another study reported that CBCT is a valuable diagnostic adjunct for identification of an increased risk for M3M extraction resulting in IANI. However, the use of CBCT does not translate into a reduction of IANI and other post-operative complications.17 A later study reported that the 186 M3Ms treatment plans did not change for 164 cases (88%), but changed for 22 M3Ms (12%) after CBCT. Direct contact between the third molar and the mandibular IDC had the highest impact on deciding on coronectomy (odds ratio (OR) = 101.8, P < 0.001). Direct contact was not a sufficient factor. However, lumen narrowing of the IDC (OR = 38.9–147.2, P < 0.001) and IDC positioned in a bending or a groove in the root complex (OR = 32.8, P = 0.016) were additional factors for deciding on undertaking a coronectomy.48
Conversely, other reports claim that, due to the high variability of the anatomical relationship in case of high-risk M3Ms, a CBCT scan should be performed for thorough case planning.82 Furthermore, using CBCT will avoid unnecessary coronectomies, thus increasing removal without nerve injury, which is the optimum possible treatment. Over 30% of high-risk M3Ms, as seen on panoral radiography, are found to be distant from the IDC on CBCT and therefore should be extracted.82 Further, research is required to ascertain the benefit of CBCT in these cases. Renton described a change in practice of over 95% of cases based upon CBCT findings, resulting in only 5% of M3Ms undergoing coronectomy.69 If a patient is unsuitable or the M3M is carious, thus extraction is indicated, CBCT can offer an excellent planning tool to miminize risk to IAN when planning surgery. Again, the evidence to support this practice is emerging.
IANIs are preventable
Indications for M3M vary internationally, however, AAOMS 2016 White paper for M3M surgery likely reflects the most common practice with active surveillance (non-extraction of approximately 23% of M3Ms that are unerupted and non-diseased). Alternative methods described how to minimize the risk, based on coronectomy to IAN on extraction of M3Ms.83,84,85 Later came several studies evaluating partial tooth removal, which was later named ‘coronectomy’, as in removal of a tooth crown.33,86,89 A recent systematic review concluded that coronectomy is a safe procedure with reduced rates of IANIs, similar rates of ‘dry socket’ symptoms and post-surgical infection compared to M3M extraction.67
Standards of care
Training
Should those not trained to remove M3Ms undertake a coronectomy? It is an adverse event knowingly to leave non high risk roots behind without informing the patient. Root retention may be indicated for ridge maintenance with prior root canal treatment (RCT) OR if the root is displaced. Therefore, surgeons undertaking coronectomy procedures must be suitably trained to remove and/or retrieve the tooth, should the roots be mobilized during coronectomy.
Patient consent
Joint decision-making involves both patient and clinician. The patient must understand the potential risk of his/her chosen intervention. Explaining the potential gain, avoiding life-long IANI is relatively simple for the patient to understand. However, explaining the complex potential complications of coronectomy (possible intra-operative root mobilization34 with necessary extraction, early77 and late post-operative infections68) is difficult and an information sheet is recommended (Trigeminalnerve.org.uk pdf Coronectomy patient information leaflet). The patient must have a good grasp of potential risks, thus coronectomy should be undertaken when all possible information is available in order to prevent unnecessary patient distress and complaints.
Poor technique
The aim of the coronectomy technique is to leave the high-risk roots with a vital pulp to allow dentine and bone integration and healing,58 and to remove all enamel. The technique is explained and illustrated in detail.90 Most failures of coronectomy have been reported to be either related to root mobilization during the procedure or inadequate removal of enamel.
Root mobilization
Once the roots are mobilized they need to be removed as infection and repeat surgery will ensue.34 Mobilization of the roots can be prevented by a more expansive section of the crown from the roots, but care must be taken not to injure the lingual nerve which has been reported.91
Lingual nerve injury
It has been suggested that, if there is a missing lingual plate, there may be increased risk to the lingual nerve during coronectomy. However, to date only rare cases have been reported.
Inadequate enamel removal
Any retained enamel fragment will act as a foreign body and cause infection and failure of the coronectomy.79 When the crown is sectioned off the root, the underside of the crown and root surface must be carefully scrutinized for any enamel fragments. Reduction of the root surface using a rosehead bur can be carried out carefully, especially on the lingual aspect.
Use of high speed front exhaust drills are not recommended
As described in a recent report of surgical emphysema has been described.92 In addition, there are many unfortunate ‘You Tube’ videos, to which some may turn for training, illustrating very poor practice and using high-speed drills.
Bone rim
In an early study, Renton et al34 recommended achieving an alveolus bony rim around the sectioned M3M root surface of 2–3 mm. This is often impossible due to the lack of a lingual plate adjacent to the M3M. As long as the enamel is removed and wound toilet is good, no further reduction of the root surface is indicated.
Primary closure
This is recommended by most studies and optimizes healing. Several studies mention early post-operative dehiscence persisting, leading to necessary root removal.80 To date there are no periodontal health and osseous regeneration outcome studies that have compared coronectomy to extraction.
Adjunctive procedures
Antimicrobial (AM) cover for surgery
In early studies, antimicrobials were prescribed routinely for coronectomy,89 however, recent studies avoid the prescription of AMs.80,89
Bone grafting
A case report illustrates that grafting over the exposed root surface, may prevent root migration.93 Leung (in a verbal presentation at ICOMS Melbourne 2015) reported a detailed series of patients where grafting had delayed root migration. However, as the coronectomy procedure is relatively successful without the additional expense of site grafting, further research is required to justify grafting coronectomy sites.
Pulpotomy, pulp dressing or root canal
As the pulpal tissue remains vital in the coronectomied root system there is no indication for pulpectomy, pulpotomy or root canal treatment.79
Related cysts
The author routinely undertakes excision of benign odontogenic cysts whilst coronecting the involved M3M or M2M. However, the pathology must be confirmed and patient reviewed.94,95
Ankylosed M3Ms or other high risk teeth
There are two reports of coronecting high risk ankylosed first and second molars in younger children.96
Post-operative radiography
Some authors have recommended routine post-surgical panoral radiography, in order to determine whether or not migration has taken place or to check for the complete removal of enamel, Other studies recommended panoral follow-up at 1 month and at 6–12 months.75 However, the author will only arrange post-operative radiography based upon the development of clinic symptoms. Post-surgical panorals or CBCTs are not recommended as part of routine coronectomy practice.
Recommendations
Coronectomy is an effective and accepted method for minimizing IANIs related to the management of high-risk M3Ms.97 However, explicit criteria for requesting a CBCT based on risk assessment of the panoral are not yet absolutely clear. Nor are there explicit criteria for recommending a coronectomy based on CBCT findings as yet. This leaves a degree of ambiguity and uncertainty in prescribing coronectomy rather than extraction for M3Ms.