Davies SJ, Gray RMJ, Whitehead SA. Good occlusal practice in advanced restorative dentistry. Br Dent J. 2001; 191:421-434
McCullock AJ. Making occlusion work: 2. Practical Considerations. Dent Update. 2003; 30:211-219
Pretty IA, Ellwood RP, Brunton PA., Aminian A. Vital tooth bleaching in dental practice: 1. Professional bleaching. Dent Update. 2006; 33:293-300
Siderido ID, Karabela MM, Vouvoudi EC. Physical properties of current dental nanohybrid and nanofill light-cured resin composites. Dent Mat. 2011; 27:598-607
Salimi H, Mosharraf R, Savabi O. Effect of framework design on fracture resistance of zirconium oxide posterior fixed partial dentures. Dent Res J. 2012; 9:754-769
Occlusal changes occur slowly throughout each person's lifetime via the process of physiological tooth wear (TW). Importantly, once the occlusal scheme has been irreversibly changed beyond a certain point, then a chain reaction of restoration failures may commence. The trigger varies for each individual and it cannot always be predicted when, where or if this occurrence will take place. Importantly, when the patient attends with failing or failed dental treatment, particularly following repeated attempts to resolve it, then a detailed investigation of the occlusion must precede treatment. Any immediate repair or replacement without consideration of the underlying aetiology would simply suffer the same consequences.
CPD/Clinical Relevance: Understanding the impact of occlusal changes on the overall survival of restorations and the health of the remaining dentition can help in early diagnoses, prevention and treatment.
Article
This paper will focus on the occlusal changes that can occur throughout an individual's lifetime. Physiological TW describes the loss of dental hard tissues by means other than caries, trauma or developmental disorders. This is an irreversible part of the ageing process, with an estimated vertical tooth surface loss of enamel at 20–38 µm per annum.1 The aetiology of TW is multifactorial in nature and the underlying factors are subcategorized into attrition, abrasion, abfraction and erosion. Therefore, the process of TW depends on numerous contributory factors including: diet, dental appliances/restorations, inherent occlusal issues, oral hygiene methods, psychological influences, parafunctional habits and underlying medical complications. The overall changes that occur to the occlusion may result in damaging premature contacts, deflective contacts and interferences, which can lead to occlusal overloading. Unfortunately, without early intervention, the resulting outcome could be disastrous.
Therefore, the importance of a thorough occlusal assessment on a regular and consistent basis cannot be over emphasized due to the constantly evolving nature of the dentition within the unforgiving oral environment. Not only is this information vital for correct diagnoses, but it will aid implementation of appropriate preventive measures and treatment planning. This calculated approach will avoid embarrassing situations, whereby recently fitted restorations repeatedly fail without warning. The dentist and patient are then left in a difficult position in terms of both financial compensation and the continuation of their professional relationship.
Case report
A 58-year-old, fit and well male presented with fractured upper front teeth, which had occurred approximately one year previously. These were artificial teeth, as part of a bridge structure, which had been in place for over 15 years. The upper right front tooth (UR1) was lost during childhood as the result of trauma. Repeated failed attempts had been made to correct the fractured teeth, which included porcelain repair and replacement of the entire bridge structure, following debonding of the current bridge. However, the replacement bridge prosthesis subsequently became loose within a short period of time and the old one was re-fitted following patient request. The patient had never been satisfied with the appearance of the current bridge.
The patient had been a regular attender to his previous dental practitioner, brushed twice per day with an electric toothbrush, but admitted only using floss and super-floss on rare occasions. Fluoride-containing toothpaste was being used without the use of mouthwash. He had a previous history of acid reflux, which had been resolved for approximately two years prior to the dental appointment.
Extra-oral examination was unremarkable (Figure 1). The patient had a relatively low smile line (Figure 2) however, despite this, he would prefer an ‘all-white replacement’ if a new bridge were to be provided.
Intra-oral examination demonstrated normal soft tissue appearance. The patient had a full dentition which was heavily restored. A fixed-fixed three unit porcelain fused to metal (PFM) bridge comprised a UR2 and UL1 abutment (A) teeth, including an UR1 pontic (P). Fractured veneering porcelain was evident on the central incisors. A fractured UL6 amalgam restoration was also present on the disto-occlusal surface with secondary caries (Figure 3).
Figure 3. Fractured UL6 amalgam restoration on disto-occlusal surface.
Examination of the occlusion revealed:
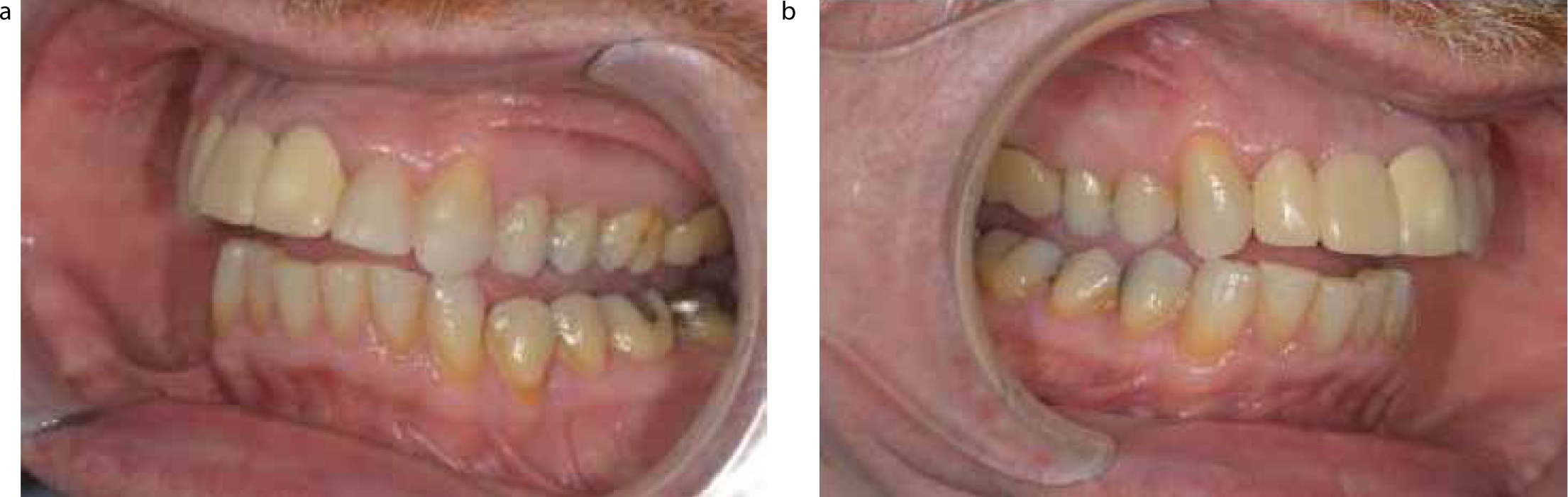
Lateral excursive movements – loss of smooth, uninterrupted canine guidance (Figure 4); this was ascertained using the patient's previous dental records, which contained 30 years of information. Non-working and working side excursive interferences on the posterior amalgam restorations and heavy contacts on the bridge units. Interferences are defined as ‘contacts on a tooth or restoration that interfere with smooth mandibular excursive movements’ and which will adversely affect the distribution of heavy occlusal forces.2
UL6 amalgam restoration was a working side, non-working side and protrusive interference.
A grade 2 score on the Smith and Knight Index was allocated to the UL3, UR3 and UL2; this being defined as incisal loss of enamel with minimal dentine exposure.
Anterior guidance – posterior interferences on the molar teeth (Figure 5).
Heavy contacts were noted on the palatal aspects of the bridge units in ICP, which was assessed using 8 µm Shimstock metal foil (Hanel, Germany). The patient reported that the bite had never felt ‘quite right’ since it was initially fitted.
No signs of active bruxism, which would include tongue scalloping and ridging of the cheeks.
No parafunctional activities/habits determined.
Figure 4.
(a, b) Loss of canine guidance and interferences right (a) and left (b) sides.Figure 5. Relationship of the bridge in protrusion.
Nothing of relevance to tooth wear/erosion was recorded.
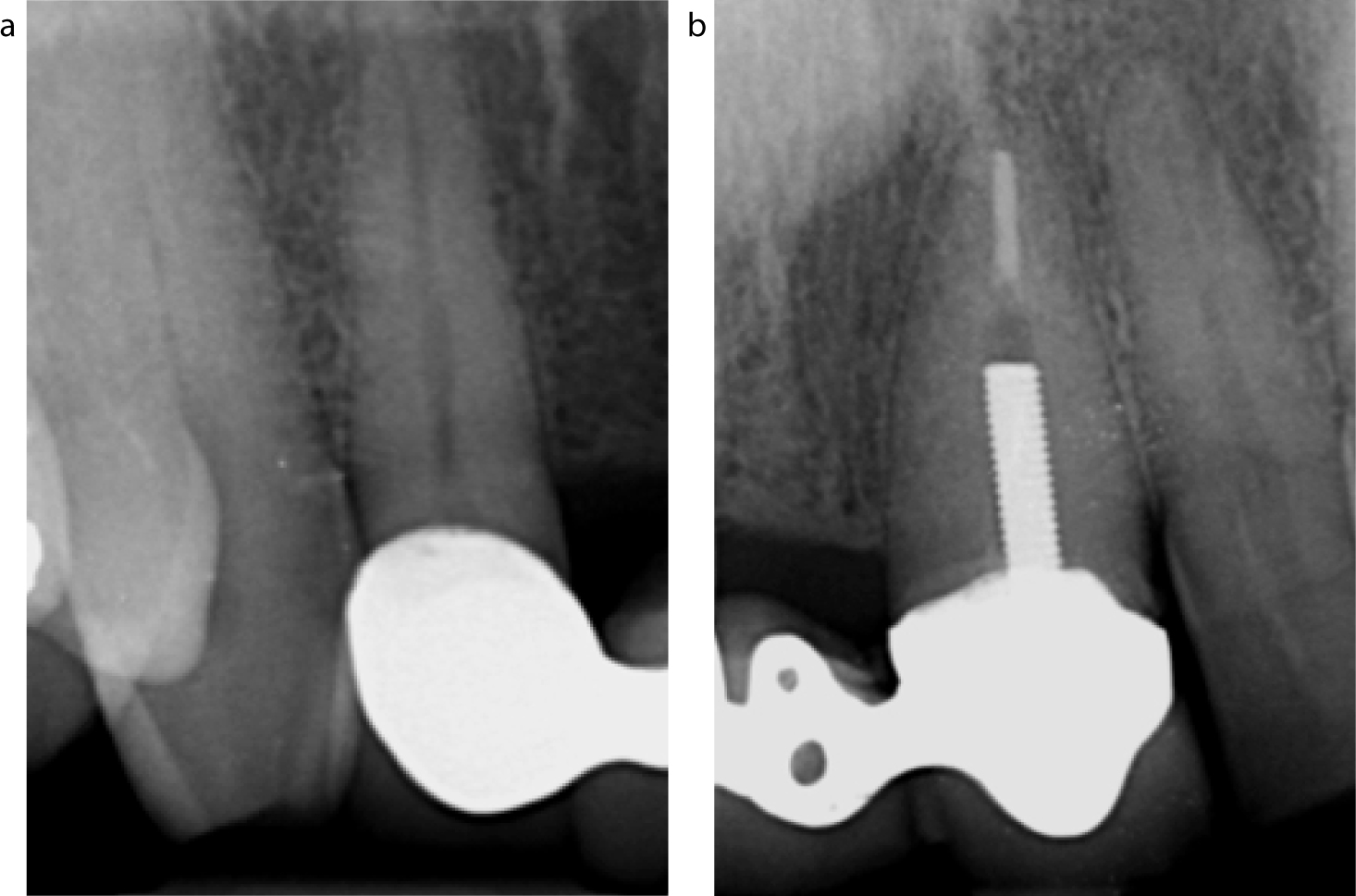
Peri-apical radiographs UL1 and UR1 (Figure 6) indicated acceptable root canal treatment of the UL1 and an active post in place. There was no evidence of peri-apical pathology, caries or a retained root. Importantly, an adequate crown to root ratio of 2:3 was noted with regards to both the abutment teeth.
Figure 6. Pre-operative peri-apical radiographs of the UR2 and UL1.
The UL6 demonstrated normal responses to pulp sensibility testing and the peri-apical radiograph was unremarkable.
Diagnoses
Fractured porcelain units – UR1(P) and UL1(A) – on three unit PFM bridge. Occlusal issues were present with the prosthesis in ICP and during excursive movements (as previously mentioned); the history suggested that this had been worsening over time.
UL6 had a fractured amalgam restoration and secondary caries with normal responses to sensibility testing. The tooth was a working/non-working side and protrusive interference.
Loss of canine guidance due to erosion and attrition.
The main aetiological factor was physiological TW, which had resulted in changes to the occlusion over time. Therefore, the occlusal scheme that the restorations were originally designed for were no longer appropriate for the patient and this resulted in occlusal overloading with subsequent failure.
Aesthetic issues with the bridge
Symmetry
The maxillary midline was not coincidental with the facial midline.
Incisal plane
The incisal plane was not parallel to the interpupillary line.
Incisal edge placement
The smile line was not coincidental with the curvature of the lower lip.
The buccal surfaces of the maxillary central incisors did not contact the inner or mucosal surface of the mandibular lip when the ‘f’ sounds were spoken (Figure 7).
Figure 7. The incisal edges of the maxillary central incisors should touch the wet/dry border of the lower lip. In this case, they are positioned too far labially due to incorrect tooth angulations.
Treatment Options
Fractured fixed-fixed bridge
Replacement fixed-fixed bridge – the patient was keen to have this form of treatment.
Implant-retained crown UR1 – declined by the patient due to the surgery and time factors.
Partial denture UR1 – the patient declined this option as he had used a removable appliance in the past and could not tolerate it.
The patient was made aware that the post may also need replacement after further inspection following bridge removal; this would normally be required if the post was loose or fractured. Considering that the post was threaded there would be a greater risk associated with root fracture.
Restoration of canine guidance
The most appropriate and minimally invasive option was direct resin-composite build-ups on the UL3 and the UR3.
Restoration of the UL6
The patient decided to have a direct resin-composite restoration. He declined the alternative long-term indirect treatment options due to the increased associated costs and time factors.
Treatment stages
The casts were mounted on a semi-adjustable articulator and the diagnostic wax-up was then fabricated:
Conformation to the current occlusal scheme;
Create canine guidance – to achieve a mutually protected occlusion that would help reduce stress on the bridge during function and harmonize mandibular movement;2
Protrusion with even incisal contacts, balancing pressure on the bridge units, and creating posterior disculsion;
Freedom in centric-anteroposterior freedom in ICP will help prevent overloading of the bridge prosthesis;
Aesthetic improvements on the aforementioned areas – this is mainly achieved with correct functional planning.3
This is useful for determining the feasibility of treatment and visualization of the end point; this information acts as a blueprint during the treatment stages.4
The fixed-fixed bridge was sectioned and removed. Upon examination, the active UL1 post was loose; however, there was no evidence of a vertical root fracture. This was subsequently removed and replaced with a quartz-fibre post, which was bonded with resin-luting cement under rubber dam isolation for adequate moisture control. A resin-composite core was then built-up to augment the occluso-gingival length, thereby increasing the retention and resistance form of the abutment tooth.5
Following preparation of the UL1 and UR2 (Figure 8), the upper and lower impressions were taken. A provisional chairside bridge was then made from bis-acryl resin and cemented with temporary luting cement.
It is important to highlight the clinical considerations which took place during this procedure:
Post length – 97% success rates are achieved where the length of the post is at least equal to the clinical crown height.6 The post should not exceed one-third of the diameter of the root.7
The ferrule effect – the coronal tooth tissue embraced by the crown. A minimum 1–2 mm height and 1mm thickness of tooth structure is required. This will significantly reduce the incidence of vertical root fracture, providing improved resistance to lateral forces.8
Biological width – following bone sounding and assessment of the pocket depths, it was determined that the patient had a high crest, with sulcus of 0.5 mm present around the UL1 and UR2. Considering the margin of a crown should be placed no closer than 2.5 mm from the alveolar bone, the preparation was limited to the gingival tissue crest.9
An interim indirect acrylic fixed-fixed bridge – a long-term provisional restoration was required to assess both the occlusion and aesthetics. Furthermore, this can be used as a guide during construction of the definitive restorations.10,11
Customized upper and lower bleaching trays were fitted and the patient was provided with 10% carbamide peroxide (CP) gel.
Two week review to assess whitening results, followed by a period of three weeks before the direct resin-composite stage is commenced as CP adversely affects the adhesive bond strength to enamel.12
Nano-hybrid direct resin-composite was selected for the UR3, UL3 and UL2 (Figure 9). This material has excellent mechanical properties, high wear resistance, high surface characteristics and aesthetics combined with reduced shrinkage at 1.4–2.2%.13 The UL6 was subsequently restored at the same appointment using the same resin-composite material. The restorations were then completed with the appropriate shaping, finishing and polishing stages.
Yttrium stabilized zirconium oxide framework was used with layered feldspathic porcelain on the labial surfaces for improved aesthetics. This was chosen due to the patient's request for an ‘all-white bridge’ and its outstanding mechanical properties and high biocompatibility. Its flexural strength is approximately 900–1200 MPa and fracture toughness ranges between 8–12 MPa/m2.14
Figure 8. Preparation of UL1 and UR2 abutments.Figure 9. Restoration of canine guidance on left (a) and right (b) sides using direct resin-composite – interim bridge in place.
Following the try-in stage and clinical/aesthetic assessment, the bridge was cemented with resin-modified glass ionomer. The occlusion was re-assessed in ICP and excursive movements with Shimstock foil. In particular, every measure was taken to ensure that there was: anteroposterior freedom in ICP, canine guidance without interferences, even contacts on the incisors during protrusion and the conformative approach was maintained (Figure 10). 8. An upper stabilization splint was then prescribed to wear at nights in order to protect the restorations. 9. The bridge has now been in situ for over six months without any issues (Figures 11–12).
Figure 10. Even contacts in protrusion.Figure 11. Post-operative smile view – following curvature of the lower lip.Figure 12. Post-operative ‘F’ sound position at the lower lip wet/dry border.
Discussion
The occlusal scheme of each and every patient is constantly adapting and changing as a result of the deteriorating effects of erosion, abrasion, abfraction and attrition. This may eventually reach the stage where the shift in the occlusion has a major impact upon the health of the teeth and longevity of restorations.
It is strongly advised that a proactive and preventive approach is adopted during the early stages, as opposed to the ‘wait-and-see’ philosophy. If it is deemed more appropriate to restore the worn dentition, then it is important to develop a minimally invasive and evidence-based treatment ideology. The practitioner must conduct a thorough clinical and radiographic examination, which will help form the basis of the definitive diagnoses, treatment plan and maintenance strategy. It is important to consider what has changed and why, including any limitations, barriers or failures that have occurred as a consequence.
The ‘Examine, Design, Execute and Check’ (EDEC)10 principle, which was used for this case, is a useful tool to help simplify the planning process with regards to occlusion:
Examine – the first stage involves a detailed assessment of the pre-existing occlusion.
Design – plan the necessary occlusal, functional and aesthetic requirements. It has been demonstrated that when the posterior teeth are separated during excursive and protrusive movements, almost all the elevator muscles switch off, thereby reducing forces on the temporomandibular joints and anterior/posterior teeth.3 Therefore, restoration of canine guidance will reduce stress on the bridge during function. For the design to be done effectively, articulated study models, a diagnostic wax-up and an intra-oral mock-up are invaluable tools. Keep in mind that form will follow function.
Execute – treatment is commenced at this stage. In this case, the occlusion and aesthetics were trialed with an interim bridge, which were subsequently incorporated into the final bridge design.
Check – ensure that the desired post-operative occlusion and aesthetics were successful.
Summary
The patient was restored to a more youthful ‘occlusal age’, which is a suitable long-term solution to correct the underlying physiological TW and subsequent occlusal issues that had taken place during his lifetime. It is impossible to predict exactly what could have happened if early intervention had not taken place. However, it was clear that the dentition was heading towards an unpredictable situation with a potential variety of undesirable scenarios including: further TW, tooth sensitivity and pain, repeated failure of restorations, temporomandibular dysfunction, invasive restorative procedures and tooth loss.
In the author's opinion, more clinicians need to be aware of the underlying threat to the patient's dental health from TW, which is easily overlooked unless one recognizes the clinical signs.
Key Point
If the functional design of the prosthesis and restorations are well planned and executed, then a pleasing aesthetic outcome will be arrived at naturally.