Haas DA, Lennon D. A 21 year retrospective study of reports of paresthesia following local anesthetic administration. J Can Dent Assoc. 1995; 61:319-330
Hillerup S, Jensen RH, Ersboll BK. Trigeminal nerve injury associated with injection of local anesthetics: needle lesion or neurotoxicity?. J Am Dent Assoc. 2011; 142:531-539
Renton T, Adey-Viscuso D, Meechan JG, Yilmaz Z. Trigeminal nerve injuries in relation to the local anaesthesia in mandibular injections. Br Dent J. 2010; 209 https://doi.org/10.1038/sj.bdj.2010.978
Malamed SF. Nerve injury caused by mandibular block analgesia. Int J Oral Maxillofac Surg. 2006; 35:876-877
Hillerup S, Jensen R. Nerve injury caused by mandibular block analgesia. Int J Oral Maxillofac Surg. 2006; 35:437-443
Renton T, Janjua H, Gallagher JE, Dalgleish M, Yilmaz Z. UK dentists' experience of iatrogenic trigeminal nerve injuries in relation to routine dental procedures: why, when and how often?. Br Dent J. 2013; 214:633-642 https://doi.org/10.1038/sj.bdj.2013.583
Shabazfar Nl, Daubländer M, Al-Nawas B, Kämmerer PW. Periodontal intraligament injection as alternative to inferior alveolar nerve block – meta-analysis of the literature from 1979 to 2012. Clin Oral Investig. 2014; 18:351-358 https://doi.org/10.1007/s00784-013-1113-1
Malamed SF, Gagnon S, Leblanc D. Articaine hydrochloride: a study of the safety of a new amide local anesthetic. J Am Dent Assoc. 2001; 132:177-185
Simon MA, Vree TB, Gielen MJ, Booij LH. Comparison of the effects and disposition kinetics of articaine and lidocaine in 20 patients undergoing intravenous regional anaesthesia during day case surgery. Pharm World Sci. 1998; 20:88-92
Meechan JG. The use of the mandibular infiltration anesthetic technique in adults. J Am Dent Assoc. 2011; 142:19S-24S
Corbett IP, Kanaa MD, Whitworth JM, Meechan JG. Articaine infiltration for anesthesia of mandibular first molars. J Endod. 2008; 34:514-518
Meechan JG, Jaber AA, Corbett IP, Whitworth JM. Buccal versus lingual articaine infiltration for mandibular tooth anaesthesia: a randomized controlled trial. Int Endod J. 2011; 44:676-681
Smith T, Urquiola R, Oueis H, Stenger J. Comparison of articaine and lidocaine in the pediatric population. J Mich Dent Assoc. 2014; 96:34-37
Lima JL, Dias-Ribeiro E, Ferreira-Rocha J, Soares R, Costa FWG, Fan S, Sant'ana E. Comparison of buccal infiltration of 4% articaine with 1:100,000 and 1:200,000 epinephrine for extraction of maxillary third molars with pericoronitis: a pilot study. Anesth Prog. 2013; 60:42-45
Darawade DA1, Kumar S2, Budhiraja S2, Mittal M3, Mehta TN4. A clinical study of efficacy of 4% articaine hydrochloride versus 2% lignocaine hydrochloride in dentistry. J Int Oral Health. 2014; 6:81-83
Thakare A1, Bhate K1, Kathariya R2. Comparison of 4% articaine and 0.5% bupivacaine anesthetic efficacy in orthodontic extractions: prospective, randomized crossover study. Acta Anaesthesiol Taiwan. 2014; 52:59-63 https://doi.org/10.1016/j.aat.2014.04.006
Monteiro MR1, Groppo FC, Haiter-Neto F, Volpato MC, Almeida JF. 4% articaine buccal infiltration versus 2% lidocaine inferior alveolar nerve block for emergency root canal treatment in mandibular molars with irreversible pulpits: a randomized clinical study. Int Endod J. 2014;
Trullenque-Eriksson A1, Guisado-Moya B. Comparative study of two local anesthetics in the surgical extraction of mandibular third molars: bupivacaine and articaine. Med Oral Patol Oral Cir Bucal. 2011; 16:e390-e396
Gregorio LV1, Giglio FP, Sakai VT, Modena KC, Colombini BL, Calvo AM A comparison of the clinical anesthetic efficacy of 4% articaine and 0.5% bupivacaine (both with 1:200,000 epinephrine) for lower third molar removal. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 106:19-28
Keetley A, Moles DR. A clinical audit into the success rate of inferior alveolar nerve block analgesia in general dental practice. Prim Dent Care. 2001; 8:139-142
Wright EF. Medial pterygoid trismus (myospasm) following inferior alveolar nerve block: case report and literature review. Gen Dent. 2011; 1:64-67
El-Kholey KE. Infiltration anesthesia for extraction of the mandibular molars. J Oral Maxillofac Surg. 2013; 71:1658.e1-e5
Benson BW1, Prihoda TJ, Glass BJ. Variations in adult cortical bone mass as measured by a panoramic mandibular index. Oral Surg Oral Med Oral Pathol. 1991; 71:349-356
Articaine-only buccal infiltrations for mandibular molar extractions: an alternative to inferior dental nerve blocks Danyal H Awal Zehra Yilmaz Samira Osailan Tara Renton Dental Update 2024 44:9, 707-709.
Authors
Danyal HAwal
BDS BSc(Hons)
Senior House Officer, King's College Hospital, London, UK
Professor of Oral Surgery, King's College London; Honorary Consultant in Oral Surgery, King's College Hospital NHS Foundation Trust and Guy's and St Thomas' NHS Foundation Trust, London
This article assesses the efficacy of the articaine-only buccal infiltration technique (AOBIT) in providing LA for adult mandibular molar extractions. In 112 patients the AOBIT effectiveness was judged against the need for repeat or supplemental infiltrations and rescue 2% lidocaine inferior dental blocks (IDBs). Sufficient anaesthesia was achieved in 57% of patients using the AOBIT, with another 27% requiring an additional dose via the AOBIT. The remaining 16% required a rescue 2% lidocaine IDB. The AOBIT could be a suitable alternative to 2% lidocaine IDBs for routine adult mandibular molar extractions, and may subsequently reduce the incidence of LA-related nerve injury.
CPD/Clinical Relevance: Debilitating nerve injury in relation to the administration of IDBs may be more common than we think. This article assesses the articaine-only buccal infiltration technique (AOBIT) as an alternative in providing local anaesthesia for routine adult mandibular molar extractions.
Article
Nerve injuries related to the administration of local anaesthesia (LA) can leave patients with lifelong neuropathic pain and may occur more frequently than we think.1,2 Inferior dental blocks (IDB) and other nerve blocks are routinely used to anaesthetize mandibular molar teeth in the UK and are often associated with an increased risk of nerve damage when compared with infiltrative techniques.3,4,5 IDBs have up to a 1 in 14,000 risk of temporary or permanent inferior dental nerve injury and this rate indicates a higher incidence of motor or sensory neuropathy when compared with spinal and epidural blocks.6 It must be mentioned that a majority of neuropraxic injuries tend to be temporary in nature, however, those that go on to be permanent tend to be life-changing.
Despite this, many dental practitioners consider IDBs to be the safest and most reliable technique for achieving anaesthesia in the mandibular molar region. Other alternatives to IDBs have been previously explored, with the most notable being periodontal intraligamentary injections. However, a recent extensive meta-analysis comparing the two techniques was unable to demonstrate the technique convincingly as a viable replacement.7
The focus of this paper was on the articaine-only buccal infiltration technique (AOBIT), which is already used routinely for implant dentistry. It could potentially provide a practical alternative to IDBs, thus decreasing the incidence of LA-related nerve injury3 while also improving the efficacy of LA administration, due to a simpler and more predictable technique.
Articaine was introduced for use in clinical dentistry in 1976. It was initially marketed in Germany and has subsequently spread throughout Europe, Canada and the United States. Its unique molecular structure means that it is the only amide local anaesthetic to contain a thiophene ring and lack an aromatic one.8 Additionally, it is the only widely used amide to contain an extra ester ring within its chemical structure.8 The advantages of this include its low toxicity following inadvertent intravascular injection, the rapid onset of surgical anaesthesia and better diffusion through tissues when compared with conventional 2% lidocaine.9 Despite 4% articaine having a stable 97% market share in Germany and rapidly increasing markets in the USA, Canada, and other countries, 2% lidocaine still remains the gold standard in the UK.6
One reason for this is that, when articaine has been used for IDBs, it has been associated with a higher risk of nerve injury. This, however, is likely to be due to the higher 4% concentration of anaesthetic rather than the agent itself.5 Moreover, the block technique itself cannot be excluded as a cause.
Interestingly, evidence suggests that articaine-only infiltrations are currently demonstrating similar efficacy to 2% lidocaine IDBs for mandibular dentistry when given in both the buccal and lingual aspects.10,11,12,13 This study aimed to evaluate the AOBIT's success in providing anaesthesia for routine adult mandibular molar extractions and ultimately negate the need for IDBs or lingual infiltrations, which may unnecessarily put the inferior dental or lingual nerves at risk. This could potentially decrease the incidence of LA-related nerve injury while improving patient comfort and increasing local anaesthetic success rates.
Aims
The primary aim of this study project was to evaluate whether 4% articaine infiltrations, given via the AOBIT, could provide adequate anaesthesia for routine adult mandibular molar extractions.
A secondary aim was to identify and assess the implications of the parameters age, gender, ethnicity and tooth type in relation to effectiveness of the AOBIT.
Method
This was a prospective study of 112 patients that was carried out over a 3-month period at the Department of Oral Surgery, King's College Hospital (KCH). The selection criteria included patients over the age of 17, who were scheduled for single-tooth routine mandibular molar extractions under LA without sedation. We defined ‘routine’ dental extractions as teeth whose removal could be expected through the use of elevators, forceps, luxators and tooth sectioning alone. We included any routine extractions that turned into surgical procedures, which we defined as those requiring bone removal or soft tissue flaps. The study excluded those with reported articaine allergies, surgical extractions, cases using sedation and patients with rapidly spreading soft tissue infections.
With consent, using a conventional aspirating dental syringe with a 30 gauge needle, about two-thirds of a 2.2 ml cartridge of 4% articaine with 1:100,000 adrenaline (Septocaine ®) was given towards the apices of the tooth to be extracted via buccal infiltration.
The remaining third was split equally and administered via two separate additional interpapillary infiltrations given either side of the crown of the tooth to be extracted, ensuring blanching of the corresponding lingual attached gingivae to indicate an adequate depth of penetration.
At least 2 minutes were allowed to lapse before the patient was checked for adequate anaesthesia using a dental probe
If the patient discerned any pain, a ‘repeat’ dose of articaine was immediately administered via the AOBIT.
If no pain was discerned after the initial dose, then the extraction process was initiated.
If the patient expressed pain at any point after initiation of the extraction process, ‘supplemental’ dose of articaine was given via the AOBIT, so long as an initial ‘repeat’ dose wasn't required. The clinician was allowed to tailor the ‘repeat’ or ‘supplemental’ injection doses to the clinical scenario, with the option of providing a maximum of 2.2 ml.
If the patient continued to express pain after being given two separate doses of articaine, then a rescue 2% lidocaine IDB was administered to allow completion.
Figure 1. The articaine-only buccal infiltration technique. (a) Two-thirds of the 2.2 ml 4% articaine cartridge initially given via buccal infiltration towards the apices of the tooth to be extracted. The remaining one-third of the cartridge is used for two additional interdental papillary infiltrations. (b) First of the two additional interdental papillary infiltrations being given through the medial gingival papilla. The second would be given through the distal gingiva using the same technique. (c) Blanching of the lingual attached gingivae upon administration of the medial interdental papillary infiltration, indicating an adequate depth of trans-buccal anaesthetic penetration.
The recommended safe dose of 4% articaine 1:100,000 adrenaline is around 7 mg/kg for a healthy adult and this was not exceeded during the study. To ensure reliability, an appropriately trained member of staff was on hand to perform or supervise use of the AOBIT. The effectiveness of the infiltration technique was judged against the need for supplemental or rescue 4% articaine AOBIT injections or 2% lidocaine IDBs, while also taking into account patient factors and the difficulty of the extraction.
Data collection and analyses
Study parameters were recorded during the appointment, the data were collated onto an Excel spreadsheet and analysed using the SPSS statistical software. Where data was categorical, appropriate Chi-squared tests were carried out and P values of less than 0.05 indicated statistically significant results.
Results
General demographics
A total of 112 patients were included in this study, with a mean age of 41.4 and a range 19.8–79.3 years. There was a 54% (n = 60) male majority compared to a 46% (n = 52) female minority. Of the 55% (n = 62) of the patients who stated their ethnicity, 50% (n = 31) of these patients were of Afro-Caribbean descent, 32% (n = 20) of Caucasian and the remaining 18% (n = 11) grouped as ‘other’. The ‘other’ category included those of Asian, Chinese and South American origin. A total of 112 teeth were extracted among the patient cohort, all of which were mandibular molars; 44% (n = 49) were first molars, 38% (n =43) were second molars and only 18% (n = 20) were third molars.
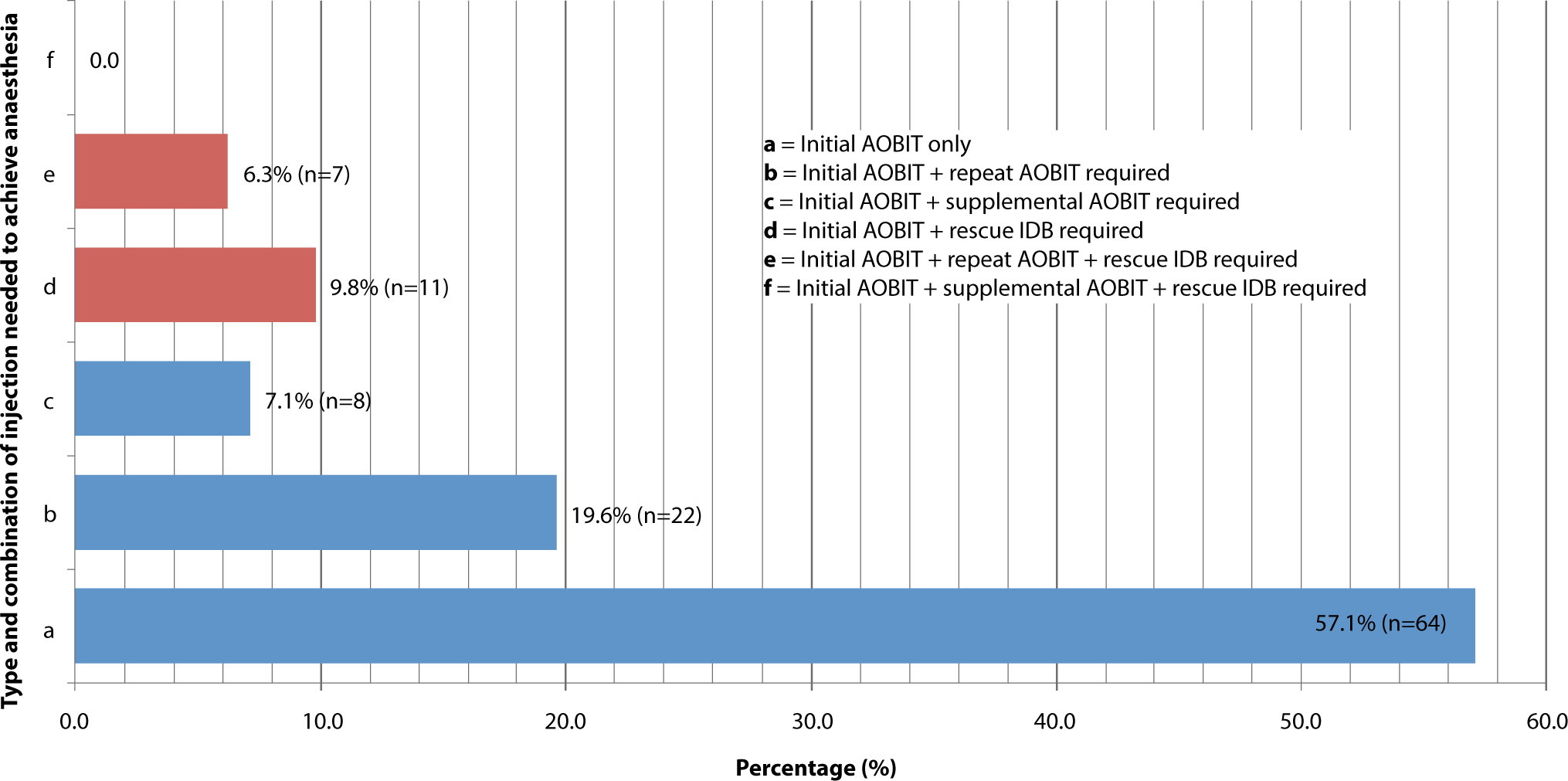
Fifty-seven percent (n = 64) of extractions were completed successfully with the use of an initial single dose of articaine (≤2.2 ml) given via the AOBIT. A further 20% (n = 22) required a repeat dose of articaine (≤2.2 ml) immediately following the initial dose and 7% (n = 8) required a supplemental dose (≤2.2 ml) at some point during the process to allow completion (Figure 2). This brings the total success of achieving adequate anaesthesia for extraction using 4% articaine via the AOBIT, with or without repeat/supplemental injections, to 84%. The remaining 16% (n = 18) of extractions required a 2% lidocaine rescue IDB to enable completion. However, 10% (n = 11) indicated no attempt at a repeat or supplemental injection following the initial articaine injection and this extra dose may have prevented the need for the rescue IDB.
Figure 2. Total efficacy of the articaine-only buccal infiltration technique (AOBIT) in achieving adequate local anaesthesia.
Mean doses of administered articaine
The mean initial dose given via the AOBIT for all extractions (including those that required a rescue IDB) was 2.01 ml [0.7–2.2 ml, SD 0.40], with the repeat dose being 1.93 ml [0.5–2.2, SD 0.53] and supplemental being 1.43 ml [0.2–2.2, SD 0.73]. The mean total dose of articaine administered was 2.61 ml [0.9–4.4, SD 1.09].
Articaine efficacy versus demographic factors and tooth type (Table 1)
Table 1 summarizes the efficacy of the AOBIT in comparison to the individual demographic factors and tooth type. After inferential statistics were carried out, a P value of >0.05 was calculated for all categories, therefore indicating a lack of statistical significance in the results.
Initial AOBIT only required for successful extraction (%)
Initial AOBIT with a repeat or supplemental AOBIT injection required for successful extraction (%)
Rescue IDB required to allow completion of the extraction (%)
Gender (P = >0.05)
Male (n = 60)
55
28
17
Female (n = 52)
60
25
15
Ethnicity (P = >0.05)
Afro-Caribbean (n=31)
65
19
16
Caucasian (n = 20)
45
35
20
Other (n = 11)
55
18
27
Age (P = >0.05)
18–29 (n = 28)
64
29
7
30–39 (n = 27)
48
33
19
40–49 (n = 24)
58
17
25
50–59 (n = 23)
61
22
17
60+ (n = 10)
50
40
10
Tooth type (P = >0.05)
1st molar (n = 49)
57
27
16
2nd molar (n = 43)
53
26
21
3rd molar (n = 20)
65
30
5
Discussion
Articaine in the literature
In recent years, there have been a number of studies assessing the viability of using articaine in routine dentistry. Four percent articaine has been shown to be a well-tolerated alternative in paediatric dentistry,14 with increasing popularity among restorative dentists.15 It has been shown to be superior to both 2% lidocaine16 and 0.5% bupivicaine17 in orthodontic extractions, and may even be more effective in managing irreversible pulpitis.18
Two studies were found to assess its applicability to molar extractions, with both finding 4% articaine more appropriate then 0.5% bupivicaine for third molars.19,20 The authors, however, were unable to find any similar studies assessing the use of 4% articaine via the AOBIT for extraction of specifically adult mandibular molars.
The AOBIT
This study indicated an 84% (n = 94) success when giving 4% articaine via the AOBIT, with or without supplemental or repeat injections. The success of ID blocks using 2% lidocaine is estimated to be anywhere between 39–91%, depending on operator experience.21 This indicates that the AOBIT could potentially be as reliable as conventional 2% lidocaine IDBs in achieving anaesthesia for single-tooth mandibular molar extractions, providing an adequate dose of articaine is administered. A major contributing factor to this is its simplicity, via direct introduction in proximity to tooth apices and the avoidance of ‘blind’ administration through several anatomical planes, which an IDB requires. Block injections, however, may be more suitable if multiple teeth require anaesthesia.
The AOBIT may be more comfortable for patients peri-operatively due to the minimal depth of tissue penetration and its technical reliability, which decreases the need for repeat injections. A visual-analogue scale could be used in future studies to assess this formally. Additionally, IDBs result in an average of 3 hours and 25 minutes of debilitating persistent numbness of the tongue and lip and it is unlikely that patients would prefer persistent oral and lingual numbness if given the option.
The use of the AOBIT may also minimize the risk of the complications associated with block injections and IDBs, including the formation of haematomas or needle fractures within the deep tissue spaces and trismus or muscle spasms due to the excessive opening.22
Most importantly, it is expected that the AOBIT carries a lower risk of inferior dental or lingual nerve injury when compared with IDBs, as the needle avoids the mandibular linguala and medial pterygoid muscle, where these nerves reside. It must be mentioned, however, that the AOBIT can put the mental nerve at risk due to the anatomical proximity of the mental foramen to the premolar apices, if applied incorrectly. While this can be considered a significant risk, it should be comparatively much lower when compared to IDBs due to the advantage of having better vision and more reliable anatomical landmarks to guide infiltrations, as well as the avoidance of ‘blind’ administration.
Some clinicians may hold reservations over a technique that failed in 16% (n = 18) of cases, however, to achieve a reduction in LA-related nerve injury, the solution may lie in adopting a culture where infiltrative anaesthesia is the gold standard and IDBs are reserved for supplementation only.
Articaine dose
The total mean dose for all extractions was 2.61 ml and the mean total dose for successful extractions only was slightly lower at 2.51 ml. This indicates the potential need for articaine cartridges to exceed the standard 2.2 ml cartridge size if the AOBIT were to be widely implemented. One study found larger 3.6 ml infiltration doses of 4% articaine to be very effective in third molar extractions23 and is an important practical aspect to consider when thinking about the future.
Demographics and tooth type
We were unable to discern any significant correlation between efficacy and demographic factors (P>0.05), probably due to the small sample size. If a larger sample were assessed it could be expected that men, Afro-Caribbeans and younger patients would need greater doses of articaine due to their higher mean cortical mandibular bone density.24
We were unable to identify any significant relationship between efficacy and tooth type (P>0.05). One would expect more posterior teeth or teeth with minimal bone loss and less mobility to require a greater dose of articaine, due to an increased volume of bone surrounding apices and the overlying external oblique ridge. Additionally, teeth exhibiting inflammation or pulpitis are likely to require greater doses of articaine due to the lowered environmental pH, which reduces the efficacy of the base element of an anaesthetic agent.
Study limitations
Whilst this work contributes towards the much needed evidence base to support the use of infiltration techniques for routine dentistry, its limitations must be recognized. As this is a single group study that lacks a control, it is generally non-informative on comparative effectiveness, thus evaluating our results of the AOBIT against inferior dental blocks should be interpreted with caution. More robust studies that include a control should be sought in future.
Selected clinical tutors chose appropriate cases using their expertise, as opposed to randomizing patient selection and thus will have introduced bias. Secondly, a majority of extractions were performed by dental students under the tutor's supervision, therefore affecting reliability. However, we believe in allowing students to perform the technique; we demonstrated its simplicity and therefore its potential applicability to all dental practitioners.
Finally, the AOBIT was only applied to routine extractions in this study and, despite the protocol, which included those that turned into surgical extractions, not a single extraction did. Whether AOBIT would be applicable for more complex extractions or for surgical removal of wisdom teeth remains to be established in future studies.
We recommend that a prospective randomized study be undertaken to evaluate the efficacy of the AOBIT technique against IDBs. This will, however, involve significant funding for MHRA and Clinical Study group support. Finding significant financial support for such work is challenging in the current environment.
Conclusion
With the acknowledged limitations of this work, the authors understand that further, more robust research will be required before the AOBIT for routine adult mandibular molar extractions can be fully endorsed. We hope that this paper has highlighted the potential that exists for the AOBIT to provide a suitable alternative to IDBs ultimately to reduce the incidence of LA-related nerve injury whilst potentially improving patient comfort, increasing anaesthetic success rates and decreasing some of the other serious risks associated with block injections. Making the AOBIT the gold standard could potentially lead to radical changes in how the administration of local anesthesia is taught and practised within the UK, with the ultimate goal of improving patient care.