Socransky SS. Relationship of bacteria to the etiology of periodontal disease. J Dent Res. 1970; 49:203-222
Socransky SS, Haffajee AD. The bacterial etiology of destructive periodontal disease: current concepts. J Periodontol. 1992; 63:322-331
Grossi SG, Genco RJ, Machtei EE, Ho AW, Koch G, Dunford R Assessment of risk for periodontal disease. II. Risk indicators for alveolar bone loss. J Periodontol. 1995; 66:23-29
Clarke NG, Hirsch RS. Personal risk factors for generalized periodontitis. J Clin Periodontol. 1995; 22:136-145
Treatment of plaque-induced gingivitis, chronic periodontitis, and other clinical conditions. J Periodontol. 2001; 72:1790-1800
Armitage GC, Cullinan MP. Comparison of the clinical features of chronic and aggressive periodontitis. Periodontol 2000. 2010; 53:12-27
Armitage GC. Periodontal diagnoses and classification of periodontal diseases. Periodontol 2000. 2004; 34:9-21
Armitage GC. Development of a classification system for periodontal diseases and conditions. Ann Periodontol. 1999; 4:1-6
Axelsson P, Nyström B, Lindhe J. The long-term effect of a plaque control program on tooth mortality, caries and periodontal disease in adults. Results after 30 years of maintenance. J Clin Periodontol. 2004; 31:749-757
Teughels W, Dhondt R, Dekeyser C, Quirynen M. Treatment of aggressive periodontitis. Periodontol 2000. 2014; 65:107-133
Herrera D, Alonso B, León R, Roldán S, Sanz M. Antimicrobial therapy in periodontitis: the use of systemic antimicrobials against the subgingival biofilm. J Clin Periodontol. 2008; 35:45-66
Griffiths GS, Ayob R, Guerrero A, Nibali L, Suvan J, Moles DR, Tonetti MS. Amoxicillin and metronidazole as an adjunctive treatment in generalized aggressive periodontitis at initial therapy or re-treatment: a randomized controlled clinical trial. J Clin Periodontol. 2011; 38:43-49
Lindhe J, Westfelt E, Nyman S, Socransky SS, Haffajee AD. Long-term effect of surgical/non-surgical treatment of periodontal disease. J Clin Periodontol. 1984; 11:448-458
Isidor F, Karring T. Long-term effect of surgical and non-surgical periodontal treatment. A 5-year clinical study. J Periodontal Res. 1986; 21:462-472
Walker CB. The acquisition of antibiotic resistance in the periodontal microflora. Periodontol 2000. 1996; 10:79-88
Preshaw PM, Heasman L, Stacey F, Steen N, McCracken GI, Heasman PA. The effect of quitting smoking on chronic periodontitis. J Clin Periodontol. 2005; 32:869-879
Heasman L, Stacey F, Preshaw PM, McCracken GI, Hepburn S, Heasman PA. The effect of smoking on periodontal treatment response: a review of clinical evidence. J Clin Periodontol. 2006; 33:241-253
Needleman I, Suvan J, Moles DR, Pimlott J. A systematic review of professional mechanical plaque removal for prevention of periodontal diseases. J Clin Periodontol. 2005; 32:229-282
Axelsson P, Lindhe J. The significance of maintenance care in the treatment of periodontal disease. J Clin Periodontol. 1981; 8:281-294
Armitage GC. The complete periodontal examination. Periodontol 2000. 2004; 34:22-33
Diagnosis and management of chronic and aggressive Periodontitis part 3: two clinical reports Despoina Chatzistavrianou Fiona Blair Dental Update 2024 44:7, 707-709.
Authors
DespoinaChatzistavrianou
DDS MFDS RCSEd, MClinDent Pro, MPros RCSEd
Specialist in Prosthodontics, Specialty Registrar in Restorative Dentistry, Birmingham Dental Hospital and University of Birmingham School of Dentistry, Birmingham Community Healthcare NHS Trust, Birmingham, UK
Although our understanding of periodontal disease pathogenesis has improved, periodontal disease remains one of the most common diseases that affects the oral cavity. Diagnosis, and therefore correct management, of chronic and aggressive periodontitis can be challenging. The first and second paper of this three-part series focused on periodontal pathogenesis, periodontal examination and diagnosis and management of chronic and aggressive periodontitis. This third and final paper will discuss two clinical cases putting theory into practice.
CPD/Clinical Relevance: This paper aims to provide the general dental practitioner with an understanding of diagnosis and management of chronic and aggressive periodontitis using two clinical examples.
Article
Understanding periodontal disease pathogenesis is a key element in diagnosis and management of the disease. There should be clear understanding that both chronic and aggressive periodontitis are diseases caused by plaque.1,2 The host response and genetic and environmental risk factors do not initiate disease but can affect the extent and severity of the condition.3,4
Effective management of chronic and aggressive periodontitis is dependent on correct diagnosis and differentiation between the two forms of disease, as they are treated differently.5,6
The first paper of this three-part series discussed periodontal disease pathogenesis and highlighted elements in the clinical assessment, which will help the clinician to establish the diagnosis of chronic and aggressive periodontal disease. A staged approach should be followed in disease management to eliminate periodontal pathogens, correct behavioural factors, such as oral hygiene and smoking, and re-establish an environment that supports beneficial micro–organisms.6
The second part offered an overview of the literature regarding the aim of periodontal treatment, the management of chronic and aggressive disease and the prognosis of periodontally involved teeth.
This final paper will discuss two clinical cases aiming to apply the theory into the everyday clinical practice.
Clinical report 1
Patient complaint and history
A 17-year-old female patient presented complaining of gum bleeding when toothbrushing, gingival margin soreness of posterior teeth, mobile teeth and spaces between teeth. The medical history was non-contributory and she was a non-smoker. The patient was a student and reported high stress levels and a familial aggregation was suggested, with her mother reporting losing teeth in her early 30s due to periodontal disease.
The dental history revealed toothbrushing twice a day with the use of an electric toothbrush and occasional use of floss for interdental cleaning, but there had been no formal instruction of oral hygiene techniques. A hygienist had undertaken debridement under local anaesthesia.
Clinical examination
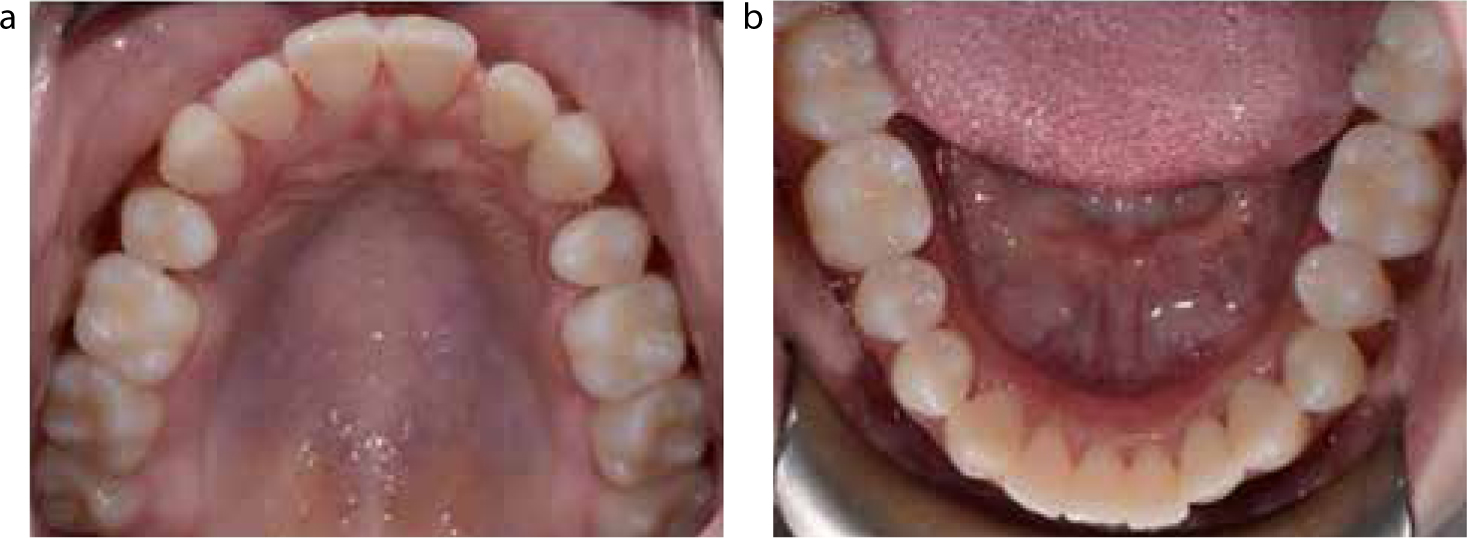
Extra-oral examination was unremarkable. Intra-orally, the oral hygiene appeared to be good with only minimal localized subgingival plaque deposits. There was localized gingival inflammation with bleeding on probing (Figures 1 and 2).
Figure 1. Labial view before treatment.Figure 2.
(a) Upper and (b) lower occlusal views before treatment.
BPE score was noted of:
4 (6)
4 (UL123)
4 (56)
4 (765)
4 (21, 12)
4 (56)
( ) indicate teeth affected
The UL126, LR16, LL6 displayed mobility of grade 1. Spacing was recorded of 1 mm at UR12, 2 mm at UL12 and 1 mm at UL34. The occlusion was Class 1 with protrusive guidance on UR1, UL1, LR1, LL1 and canine guidance in right and left excursions. The patient reported a nail-biting habit, especially during the exam period.
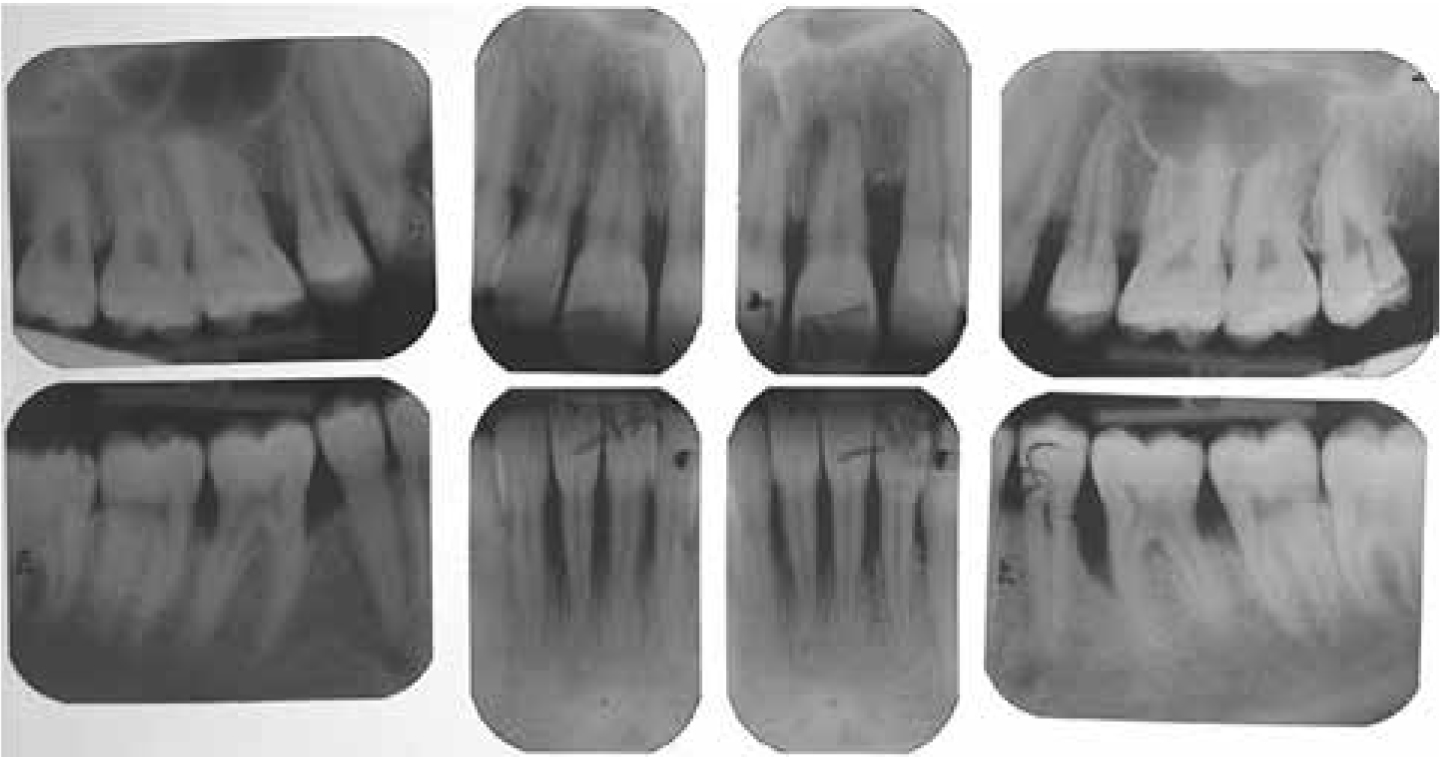
Radiographic examination
The radiographic examination required full mouth periapical views since BPE code 4 scores were recorded in all sextants and multiple mobile teeth were identified. The following radiographic findings were noted:
20–30% localized bone loss at UR8721, UL56, LR6, LL7;
40% localized bone loss at UR6 with a vertical bone defect;
50% localized bone loss at LR1, LL126 with vertical bone defect LL6;
A diagnosis of generalized aggressive periodontitis was made based on key features:
From the patient complaint and history, the patient was a non-smoker, the medical history was non-contributory and there was familial aggregation;
From the clinical examination, the oral hygiene was good with minimal plaque or calculus deposits, and significant attachment loss was noted for the patient's age with notable involvement of incisor and first molar teeth;
From the radiographic examination, there was significant bone destruction with vertical defects inconsistent with the presence of microbial deposits. The predominantly affected teeth were the incisor and first molar teeth;7,8,9
As there were more than two teeth, other than the affected incisor and molar teeth, the condition fell into the category of generalized rather than localized disease.
Periodontal management
Behavioural change
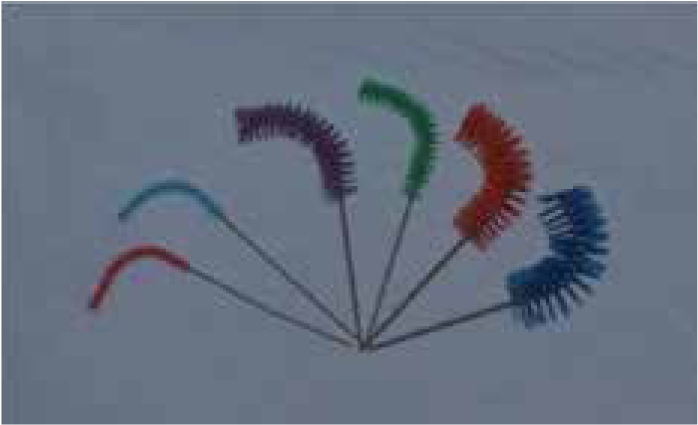
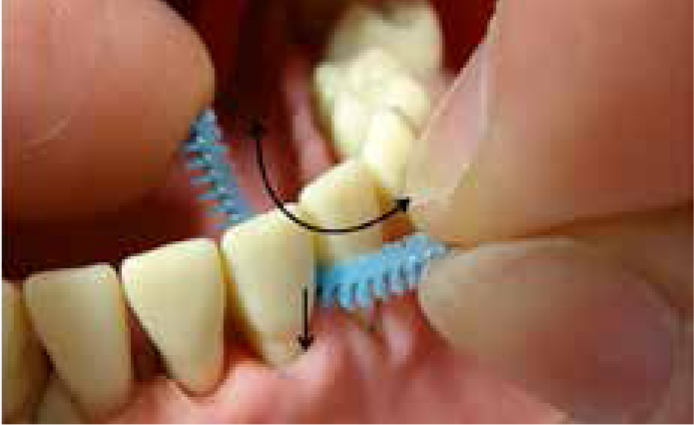
The periodontal management involved delivery of phased treatment, as discussed in the second part of the series, with the first stage being a recording of plaque and gingival bleeding indices and a detailed six-point pocket chart.5 Oral hygiene techniques were demonstrated in the patient's mouth, including the Bass toothbrushing technique and emphasis on interdental cleaning with interdental brushes using a bimanual technique to achieve targeted and controlled subgingival cleaning (Figures 4 and 5).10 The patient in turn demonstrated correct use of techniques, which was noted in her record.
Figure 4. Curved interdental brushes (Vision Interdental Perio BrushTM). The authors favour these interdental brushes since they have the ideal shape, length and physical resistance to clean optimally into deeper pockets.Figure 5. The use of curved interdental brushes. A bimanual technique is used to apply gentle pressure to push the bend of the brush into the pocket whilst moving the brush backwards and forwards.
Non-surgical periodontal treatment
Plaque scores indicated a good level of oral hygiene (below 20%) and supragingival cleaning, followed by subgingival debridement in all pockets ≥5 mm, was carried out under local anaesthetic. Local anaesthesia was essential to allow instrumentation to the full depth of the pocket without causing discomfort to the patient. Site-specific curettes (Gracey) and ultrasonic instrumentation were used to achieve thorough cleaning of the root surfaces. Confirmation of removal of calculus deposits was verified using an Explorer (ODU); the ball end of the WHO probe can also be used.
Systemic antibiotics (amoxicillin 500 mg tds 7 days combined with metronidazole 400 mg tds 7 days) were prescribed as an adjunct to treatment. The micro-organisms associated with aggressive disease are capable of tissue invasion and therefore may evade instrumentation. Significant improvement in pocket depth reduction has been demonstrated for adjunctive use of systemic antimicrobials when treating aggressive disease.11,12 As recommended, the systemic antibiotics were commenced on the day of completion of the initial therapy root surface debridement, to ensure removal of biofilm that might interfere with antimicrobials carried in the pocket gingival crevicular fluid.13 An alternative antimicrobial regimen, should amoxicillin or metronidazole be contra-indicated, is doxycycline with a 200 mg first day loading dose and to follow with 100 mg once a day for 21 days. Given the increasing emergence of antimicrobial resistance in periodontal microflora, this alternative should be considered if previous adjunctive therapy for aggressive disease is unsuccessful.14,15,16
Review following non-surgical periodontal treatment
The patient was reviewed after the recommended three-month healing period for repeat chartings, which confirmed pocketing had resolved. Subsequently, the patient was discharged to her dentist to enter a maintenance programme for three-month recording of plaque and gingival bleeding indices, reinforcement of oral hygiene techniques and supra- and subgingival cleaning. Yearly full mouth detailed six-point pocket charting is required to detect recurring disease.5,6
Clinical report 2
Patient complaint and history
A 59-year-old female patient presented complaining of bleeding gums and recurring infections in posterior teeth. The medical history was non-contributory and she reported smoking five cigarettes per day for over 10 years. The patient was a mental health support worker and reported low stress levels. Familial aggregation for periodontal disease was not reported.
The dental history revealed toothbrushing twice a day with an electric toothbrush and use of spiral brushes for interdental cleaning, but there had been no formal instruction of oral hygiene techniques. A hygienist had undertaken debridement under local anaesthesia.
Clinical examination
The extra-oral examination was unremarkable. Intra-orally, the oral hygiene was fair supragingivally, however there were generalized subgingival plaque and calculus deposits. There was localized gingival inflammation with bleeding on probing.
BPE score was noted of:
4 (762)
4 (UL2)
4 (57)
4 (765)
4 (321, 12)
4 (57)
( ) indicate teeth affected
The UR7, UL57, LL7 and LR87 displayed grade 1 mobility. Spacing of 1 mm was recorded at LR321. There was an anterior open bite with protrusion and lateral excursions guided on posterior teeth. The patient reported no para-functional habits.
Radiographic examination
The radiographic examination required full mouth periapical views since BPE code 4 was recorded in all sextants and multiple mobile teeth were identified. The following radiographic findings were noted:
30–70% generalized bone loss;
Furcation involvement at UR76, LR67, LL7;
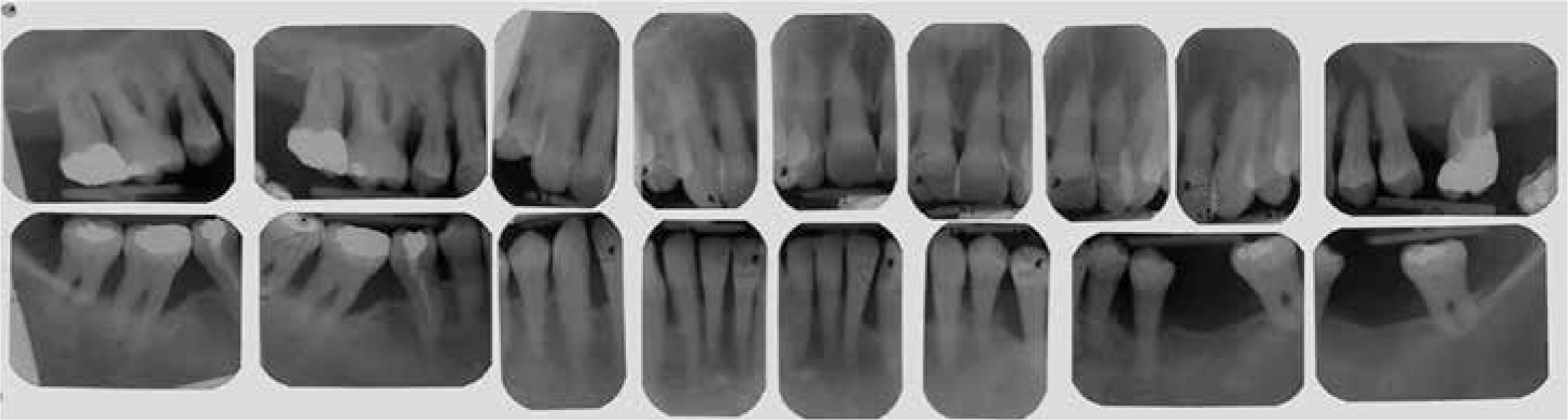
Suboptimal root canal treatment with no evidence of peri-apical radiolucency at UL7 and LR5 (Figure 6).
Figure 6. Pre-operative radiographs.
Diagnosis
A diagnosis of generalized severe chronic periodontitis was made based on key features:
From the patient complaint and history, smoking was identified as a systemic risk factor and no familial aggregation of disease was reported;
From the clinical examination, the oral hygiene was inadequate subgingivally, with generalized subgingival plaque and calculus deposits;
From the radiographic examination, there was significant bone destruction consistent with the clinical finding of generalized subgingival deposits and the pattern of bone loss was generally horizontal;7,8,9
As more than 30% of teeth were involved the category of disease was generalized rather than localized;
As the majority of teeth showed >5 mm bone loss, the degree of disease was severe.
Periodontal management
Behavioural change
Periodontal management involved delivery of phased treatment, the first step being smoking cessation advice and discussion of the adverse effects of smoking on the periodontium and overall health.17,18 Baseline recording of plaque and gingival bleeding indices, and detailed six-point pocket chart were completed.5,6 Oral hygiene techniques were demonstrated in the mouth, including Bass toothbrushing and curved interdental brushes with a bimanual technique.10
Non-surgical periodontal treatment
With plaque scores indicating a good level of oral hygiene (below 20%) supragingival cleaning followed by subgingival debridement in all pockets ≥5 mm was carried out, under local anaesthetic with curettes and ultrasonic scalers.5,6
Review following non-surgical periodontal treatment/periodontal surgery
At the 3-month review appointment, residual pockets with bleeding on probing were noted at a number of sites, some with detectable subgingival deposits, and a second course of non-surgical periodontal treatment was indicated to remove any detectable deposit, again under local anaesthetic.14,15
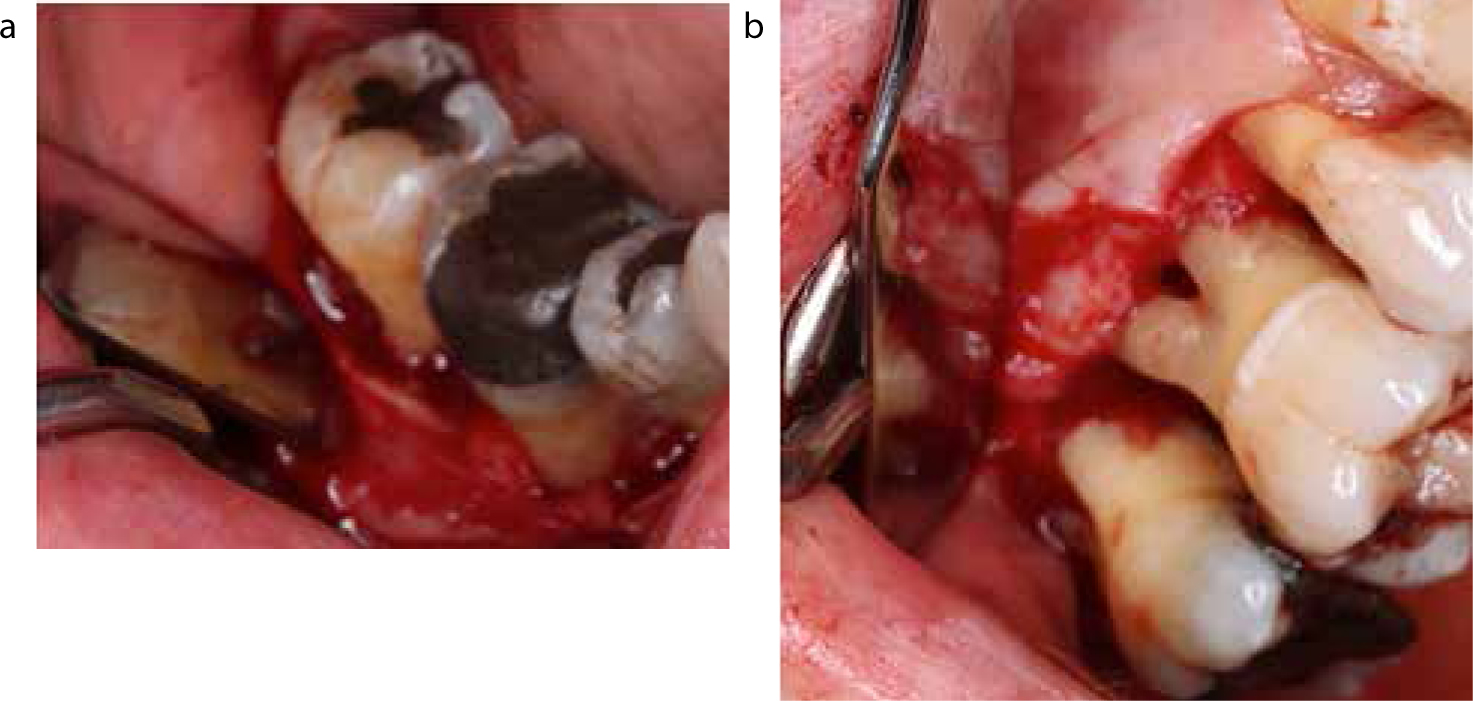
At the subsequent 3-month review appointment, there had been significant improvement with isolated sites with recorded pocketing ≥5 mm and bleeding on probing at UR764, UL7, LR76 and LL57. Surgical periodontal treatment followed as the patient was compliant, maintaining a good level of oral hygiene and had refrained from smoking over 1 year.14,15 Importantly, subgingival deposits were not detectable at the remaining sites and, in this situation, surgical treatment with open flap debridement is indicated for improved access and visualization of root surface sites, especially where there is furcation involvement (Figures 7 and 8). Surgery is not indicated in smokers due to compromised healing.
Figure 7. The clinical view at the 3-month review appointment following the second course of non-surgical periodontal treatment. Although the oral hygiene was optimal, pocket depths over 5 mm with bleeding on probing were noted in the UR764, UL7, LR76 and LL57 sites.Figure 8.
(a, b) The operative views of the surgical intervention. Note that flaps are minimal and a conservative approach is followed.
Periodontal maintenance
At the 3-month review appointment following the surgical periodontal treatment, the patient maintained a good level of oral hygiene and no significant pocket depths were noted. The patient entered a maintenance programme, as outlined previously.
As discussed in part 2 of this series, maintenance is the most important element of periodontal management, with repeated reinforcement and monitoring of oral hygiene technique having a similar effect to regular professional mechanical debridement.19 A patient-tailored recall programme can help maintain excellent standards of oral hygiene and unaltered attachment level; without maintenance, recurrence of disease is likely.20
Discussion
Both chronic and aggressive periodontitis are plaque-related diseases initiated by bacteria. The host response, genetic predisposition and environmental risk factors do not initiate periodontal disease; however, these can influence the extent and severity of the disease.1,2,3,4 A comprehensive periodontal examination is an essential component of periodontal management in order to identify all features that will determine the diagnosis and to inform an effective management plan.21 The periodontal diagnosis should include the type, severity and extent of the disease.7,8,9 Aggressive disease may progress quickly and with significant attachment loss, therefore it is essential to identify correctly and differentiate this disease from chronic disease so that effective and timely management is undertaken.5,6 Behavioural management is essential to address the all-important hygienic control of bacterial plaque and to encourage smoking cessation, where necessary. The patient records should indicate all discussions, decisions and interventions in management of their condition, which must be supported by appropriate charts and reports; a look back especially should be required. Periodontal care is currently one of the highest areas of litigation and is set to increase. Cases can be brought from the time the patient becomes aware of the problem and an investigation may look back as far as 25 years. Patient records need to note all relevant investigations and findings, and should record any advice and treatment given, and also that which may have been ignored or declined by the patient.
Summary
This three-part series aimed to provide the general dental practitioner with an understanding of diagnosis and management of chronic and aggressive periodontitis. The first paper reviewed periodontal disease pathogenesis, periodontal clinical assessment and diagnosis of chronic and aggressive periodontitis. The second focused on the aim of periodontal treatment, the management of chronic and aggressive periodontitis and the prognosis of periodontally involved teeth. Finally, this final paper discussed the scientific evidence regarding diagnosis and management of chronic and aggressive periodontitis using two clinical examples.