The immune system: basis of so much health and disease: 4. immunocytes Crispian Scully Eleni A Georgakopoulou Yazan Hassona Dental Update 2024 44:5, 707-709.
The immune system is the body's primary defence mechanism against infections, and disturbances in the system can cause disease if the system fails in defence functions (in immunocompromised people), or if the activity is detrimental to the host (as in auto-immune and auto-inflammatory states). A healthy immune system is also essential to normal health of dental and oral tissues. This series presents the basics for the understanding of the immune system, this article covers cells of the immune system (immunocytes).
Clinical Relevance: Modern dental clinicians need a basic understanding of the immune system as it underlies health and disease.
Article
Crispian Scully Eleni A Georgakopoulou Yazan Hassona
The immune system employs various cells to protect humans from pathogens. All immune cells (immunocytes) are bone marrow-derived white blood cells (leukocytes) which have specialized functions (Article 1) and can be functionally categorized into three main groups:
Lymphocytes (B- and T-lymphocytes) – responsible for mediating the adaptive immune responses;
Antigen presenting cells (APCs), including macrophages, Langerhans and dendritic cells – process and present antigens to lymphocytes.
Killing cells, including natural killers (NKs), macrophages and polymorphonuclear neutrophilic leukocytes (PMNLs) – which kill invading pathogens.
Lymphocytes
T-Cells
T-lymphocytes are produced in the bone marrow from the pluripotential bone marrow haemopoietic stem cell and migrate to the thymus (hence the T) where they complete their development (Article 3). T-cells are particularly important in acquired immunity against:
Viruses;
Fungi; and
Certain bacteria (such as mycobacteria).
T-cells are also involved in mediating immunological processes such as:
Graft rejection and graft-versus-host reaction;
Delayed hypersensitivity;
Defence against cancer cells.
These functions are mediated by different subsets of T-lymphocytes distinguished by unique surface markers known as cluster of differentiation (CD); these surface markers also mediate antigen recognition, and interactions between T-cells and APCs by functioning as cell surface receptors (known as T-cell receptors, TCRs).
T-cells recognize antigens through their TCR. Some T-cells develop TCRs as they mature and these have an affinity to bind to MHC Class II antigens, and will become T-helper (Th) cells (identified by their expression of CD4 (CD4+ cells). Other T-cells as they mature develop TCRs that have an affinity to bind to major histocompatibility complex (MHC) Class I antigens and will become T-cytotoxic (Tc) cells identified by their expression of CD8 (CD8+ cells). Other groups of T-cells include gamma-delta T-cells (γδ T-cells) and regulatory T-cells (T-regs) (Table 1).
T-cell subset
Main function
T-helper
Help other immune cells by releasing cytokines, ie induce antibody production by B-cells, activate cytotoxic T-cells, and enhance the bactericidal activity of macrophages and phagocytes
T-cytotoxic
Eliminate virally infected and cancer cells, and mediate transplant rejection
Gamma-delta T-cells
Initiate and propagate immune responses
Regulatory T-cells
Dampen excessive inflammation and control immune tolerance
CD4+ cells
Features of CD4+ cells include the following:
Healthy adults usually have CD4 + T-cell counts of 1,000 or more per cubic millimeter (mm) of blood;
Also known as T-helper [Th] cells, CD4+ T-cells are important in the initiation of immune response by providing help to other cells, such as B-cells and macrophages;
Th-cells become activated when they are presented with antigens by MHC Class II molecules, which are expressed on the surface of APCs;
Activated Th CD4+ cells expand and differentiate into different effector T-helper (Th) subsets and secrete several cytokines and colony-stimulating factors (CSFs) that can:
Induce B-cell differentiation;
Induce CD8+ cytotoxic T-cell proliferation; and
Produce various soluble mediators (cytokines).
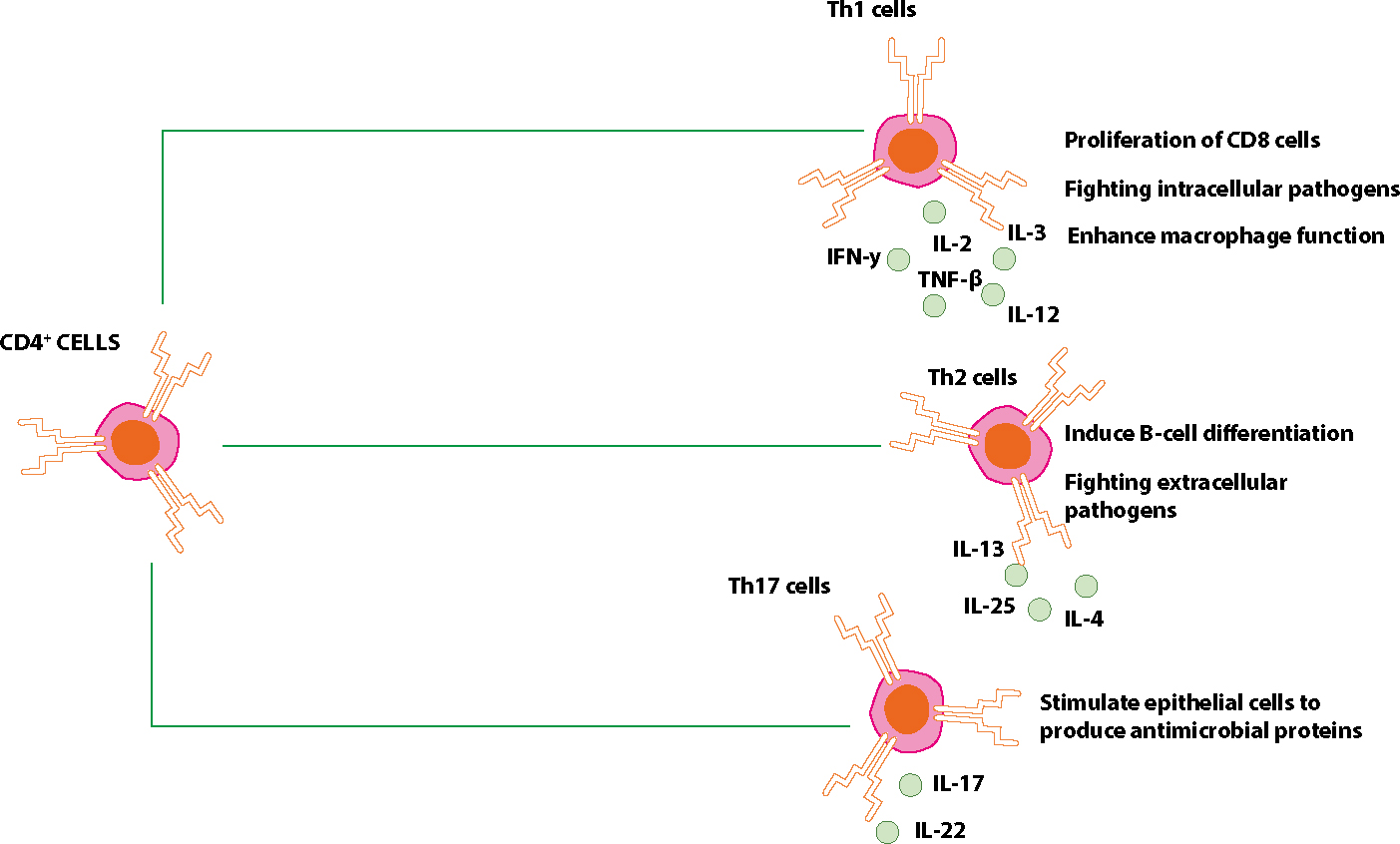
Th subsets include Th1, Th2 and Th17 – characterized by distinct effector functions and cytokine production (Table 2);
Th1-cells produce cytokines involved mainly in cell-mediated immune response and inflammation, eg IFN-γ, TNF-β, IL-2, IL-3 and IL-12;
Th1-cells are important for maximizing the killing efficiency of macrophages in the elimination of intracellular pathogens. They also promote the proliferation of cytotoxic CD8+ T-cells involved in type IV immune responses;
Th1-cells are suppressed by IL-10;
Th2-cells secrete IL-4, IL-13, and IL-25 thus stimulating B-cells to produce antibodies of immunoglobulin classes IgG, IgA and IgE;
Th2-cells are involved in type II and type III immune reactions, and in elimination of extracellular pathogens;
Th2-cells are suppressed by interferon;
Th17-cells produce IL-17 and IL-22 which stimulate epithelial cells to produce antimicrobial proteins active against Staphylococci and Candida.
Th1
Th2
Th17
Main cytokines
IL-2
IL-4
IL-17
IFN-gamma
IL-5
IL-22
IL-12
IL-10
Main defensive function against
Intracellular microbes
Helminths and extracellular microbes
Extracellular microbes
Involvement with disease
Inflammatory and autoimmune disease
Allergies
Autoimmune and auto-inflammatory disease
Th17-cells play an important role in defence against extracellular pathogens not efficiently cleared by other cells (Figure 1).
Figure 1. There are three main subsets of CD4+ T-cells: Th,1 Th2 and Th17.
CD8+ cells
CD8+ cells (cytotoxic T-cells [Tc]), are important in:
Eliminating virally-infected cells;
Eliminating cancer cells, and
Mediating transplant rejection.
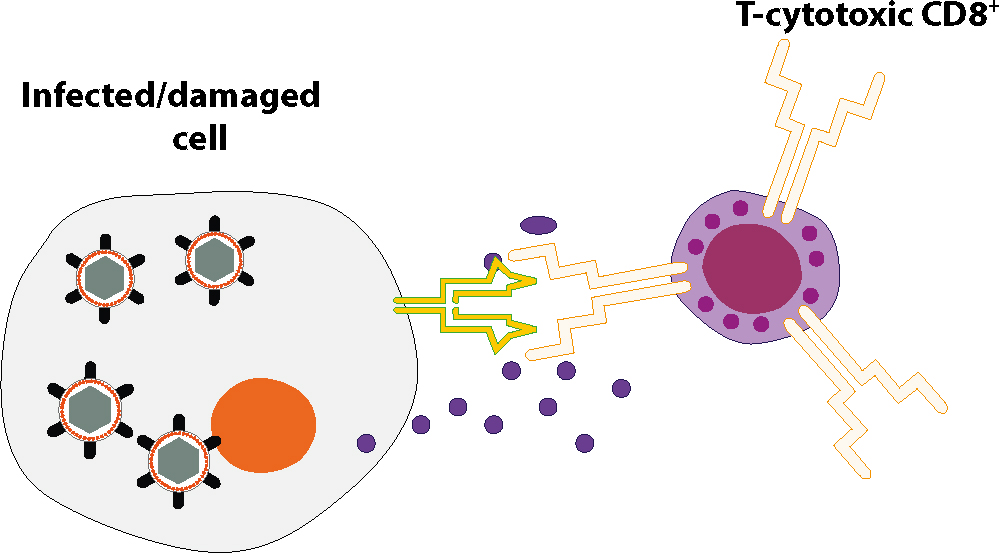
CD8+ cells constitute 35% of peripheral T-cells, and can recognize their targets by binding to antigens associated with MHC Class I molecules, which are expressed on the surface of almost all host cells. When exposed to infected/damaged cells, Tc-cells release their cytoplasmic storage granules that contain proteins, such as perforins, esterases (granzymes), and toxic cytokines which can induce apoptosis (programmed cell death) of the infected/damaged cells (Figure 2).
Figure 2. When exposed to infected/damaged cells, Tc cells release their cytoplasmic storage granules that contain proteins, such as perforins, esterases (granzymes) and toxic cytokines which can induce apoptosis (programmed cell death) of infected/damaged cells.
Gamma delta (γδ) T-cells
Features of Gamma delta (γδ) T-cells include the following:
γδ T-cells constitute less than 2% of peripheral T-cells;
These are a small subset of T-lymphocytes that have a different TCR from those of CD4+ and CD8+ T-cells;
γδ T-cells share characteristics of Th, Tc and NK cells, and some produce IL-17 and IFN-gamma;
The exact functions of γδ T-cells are not clear, but they are believed to straddle the interface between innate and acquired immunity.
Regulatory T-cells (T-regs)
T-regs are crucial for the maintenance of immunological tolerance. They suppress activation of the immune system and prevent pathological self reactivity (ie autoimmune diseases).
B-Cells
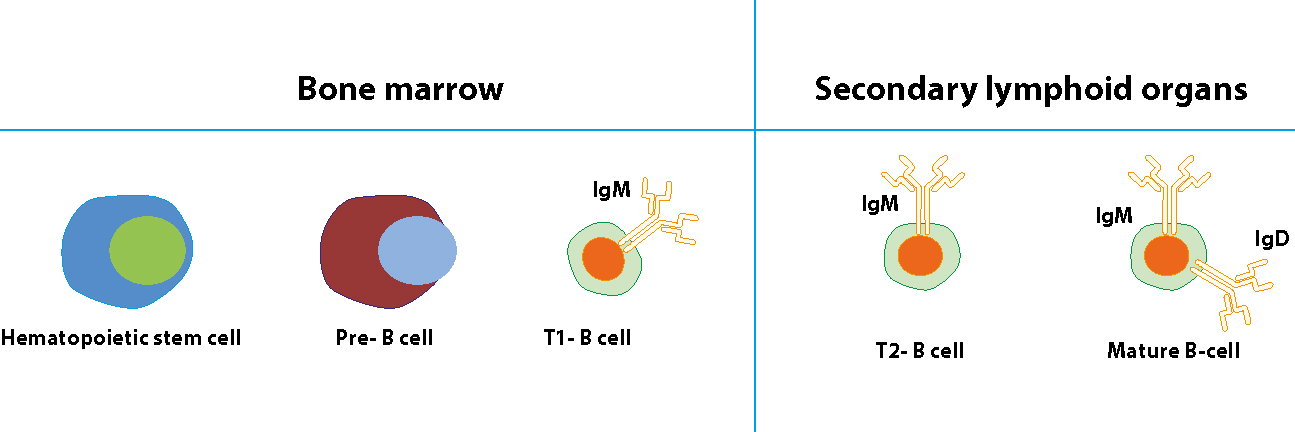
B-lymphocytes develop in the bone marrow from the pluripotential bone marrow haemopoietic stem cell, and migrate to secondary lymphoid organs (spleen and lymph nodes) where they complete their maturation. Once B-cell antigen receptors become functional, a transitional type 1 (T1) of B-cells migrate from the bone marrow to secondary lymphoid organs to mature further. Within the secondary lymphoid organs, T1 B-cells develop into transitional type 2 (T2)B-cells which finally develop into mature B-cells. B-cell development and maturation is characterized by rearrangement of the immunoglobulin (Ig) genes, and the expression on the cell surface of immunoglobulin receptors specific for a single antigenic epitope. B-cells can, via these receptors, recognize antigens directly (Figure 3).
Figure 3. B-cells develop in bone marrow and migrate to secondary lymphoid organs where they become mature cells expressing the B-cell receptors IgM and IgD.
B-cell function
B-lymphocytes protect particularly against pyogenic bacteria via humoral (antibody-mediated) acquired immunity.
Antibody responses
Antibody responses include:
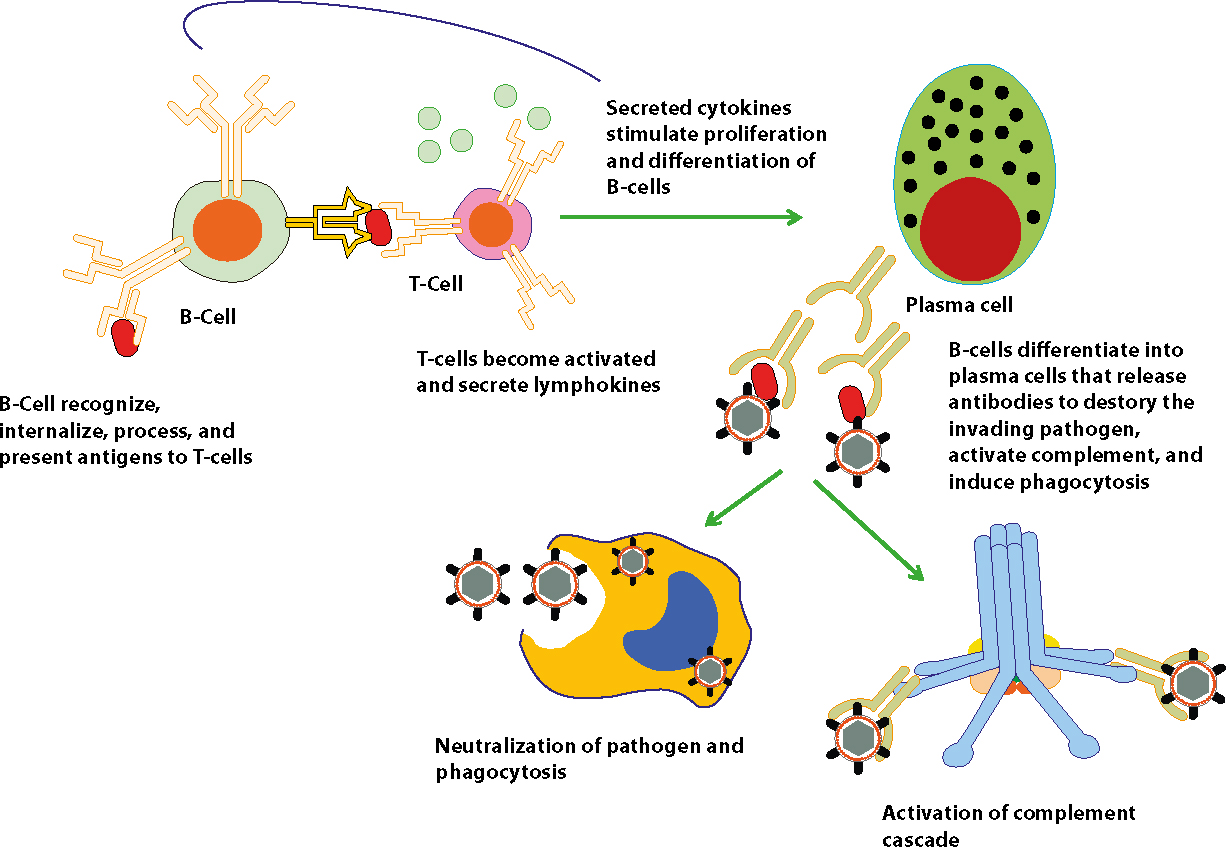
B-cells typically require Th-cell help to generate an effective antibody response (termed T-dependent antigen processing). T-dependent antigens bind to the B-cell immunoglobulin receptor, are internalized, processed, and presented in association with MHC Class II molecules to T-cells. The complex of antigen/MHC Class II is recognized by an antigen-specific T-cell, which then becomes activated, secreting cytokines (lymphokines) that act on activated B-cells to promote proliferation and/or differentiation (Figure 4).
B-cells can react without Th-cell help to T-independent antigens, which include some polysaccharides, and polymeric, or degradation-resistant antigens, however, these antigens induce a weaker humoral immune response, only IgM is secreted, and memory B-cells are not formed (Figure 5).
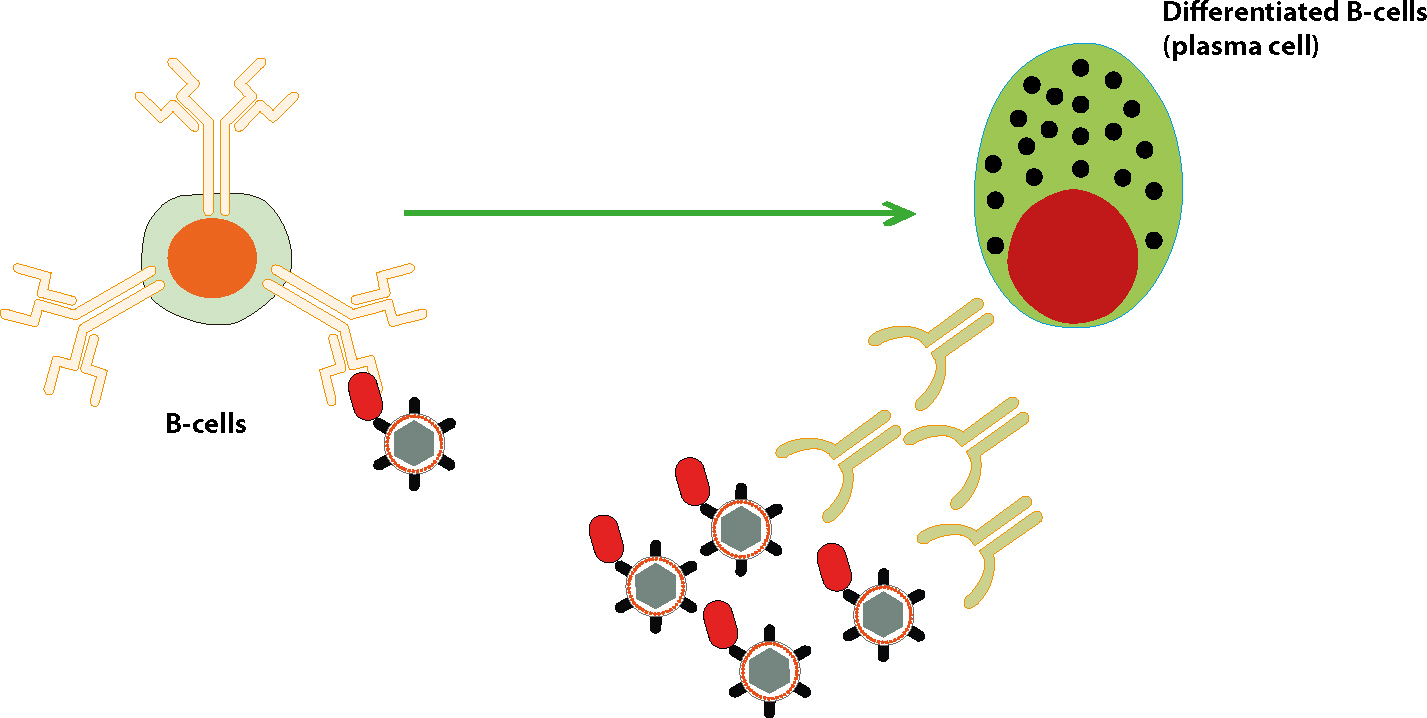
The first contact with a specific antigen elicits a primary immune response in which B-cells undergo clonal selection, and differentiate into antibody-producing plasma cells, and memory cells.
The primary immune response is complex and not rapid – it can last from days to several weeks and initially consists of a peak of IgM antibodies followed later by a switch to IgG.
During the immune response, the antibody affinity increases (affinity maturation), dependent on somatic mutation in the combining site (the immunoglobulin V-region), and competitive selection of responding clones.
Memory B-cells (and memory T-cells) develop so that subsequent exposure to the same antigen elicits a secondary immune response.
The secondary immune response develops more rapidly than a primary response, with mainly IgG antibodies, reaching a greater magnitude and lasting longer than the primary immune response.
B-cells that do not encounter the antigen, for which they are specific, die within a few days.
Figure 4. B-cells reaction to T-dependent antigens.Figure 5. B-cell reaction to T-independent antigens. B-cells recognize antigens on the surface of extracellular pathogens and differentiate into plasma cells that release antibodies to destroy the invading pathogen.
Humoral immunity (antibodies) protects via the following:
Neutralizing bacterial toxins (eg antitoxins to diphtheria or tetanus);
Attaching to bacterial surfaces and preventing adherence to their target cells;
Activating complement, leading to bacteriolysis (and inflammation);
Acting as opsonins which coat microbes, enhancing their phagocytosis;
Clumping pathogens (agglutination) leading to phagocytosis.
Humoral (antibodies) immunity can be either passively acquired or actively acquired.
Passively acquired immunity can be:
Natural (antibodies pass through placenta to foetus); or
Artificial (injection of antibodies, such as gamma globulin).
Actively acquired immunity can be:
Natural (follows clinical or sub-clinical infection); or
Artificial (follows immunization [vaccination] with live or killed infectious agents or their products).
Antigen presenting cells (APCs)
Antigen presenting cells are a heterogeneous group of immune cells that mediate the cellular immune response by processing and presenting antigens for recognition by T-cells. APCs are either:
Professional: these internalize and process antigens, and then display them, bound to MHC-II (major histocompatibility complex: Article 8), for recognition by T-cells; or
Non-professional: these include all nucleated cells expressing MHC-I.
There are three main types of APCs, dendritic cells being the most important. They are present in tissues that are in contact with external environment, such as the skin (called Langerhans cells) and mucosae (eg oral, nasal, respiratory, genital and intestinal).
Killing cells (phagocytes and others)
The main (professional) phagocytes are the polymorphonuclear neutrophilic leukocytes (PMNLs), and macrophages, and include the following features:
Phagocytes migrate towards targets such as bacterial proteins, clotting peptides, complement or cytokines;
The movement of leukocytes between the blood and tissues depends on leukocyte-endothelial cell adhesion molecules known as selectins, integrins and immunoglobulin gene superfamily inter-cellular adhesion molecules (ICAMs);
PMNLs include myeloid (bone marrow)-derived neutrophils which leave the bone marrow, to circulate in the blood;
Neutrophils persist in both blood and tissues for about six hours and, at sites of infection, they adhere to the capillary endothelium and force their way into the extracellular space by squeezing through endothelial junctions (diapedesis). They survive in the tissues for 1–2 days, phagocytosing and digesting foreign material that they encounter;
PMNLs are attracted towards antigens after an antigen-antibody (immune complex) reaction which activates complement to produce chemotaxins;
PMNLs can ingest (phagocytose) and, in their lysosomes, often kill micro-organisms coated by specific antibody and activated complement components (ie opsonized). PMNLs may also discharge degradative enzymes resulting in local tissue damage;
PMNLs contain defensive granules:
primary granules (consisting of defensins, myeloperoxidase, elastase, cathepsins); and
Eosinophils persist in both blood and tissues for somewhat longer than neutrophils, and function by using the contents of their granules to attack large parasites. Eosinophils also function in antibody-dependent cellular cytotoxicity (ADCC);
Basophils circulate for about 2 weeks and can bind immunoglobulin E (IgE). Basophils and mast cells have surface receptors for IgE, and they contain histamine, prostaglandins, leukotrienes and proteases. They are involved in immune responses to parasites and in immediate type hypersensitivity responses;
Mast cells resemble basophils, but their lifespan is 1–3 weeks;
Mononuclear phagocytes (monocytes and macrophages) are large phagocytic cells that can live for months or years. Monocytes leave the circulation by diapedesis, and transform into sessile or wandering macrophages which phagocytose and digest not only foreign particles, but also effete erythrocytes, dead or dying neutrophils, and fragments of cellular material;
Macrophages are, like neutrophils, attracted towards antigens after an antigen-antibody (immune complex) reaction. They can ingest (phagocytose) and, in their lysosomes, often kill micro-organisms coated by specific antibody and activated complement components (opsonized). They may also discharge degradative enzymes resulting in local tissue damage;
Macrophages, unlike other phagocytes, can be resting; or may become primed by inflammatory mediators, by interaction with opsonized particles, or by stimulation with a number of other agents for a response; or be fully activated with secretion of cytokines and other regulatory molecules;
Macrophages can initiate specific immune responses by antigen presentation, presenting fragments of digested foreign material to T-lymphocytes;
Macrophages also produce several cytokines that mediate or amplify host defence mechanisms;
Macrophages are activated by interaction with Th1-cells and cytokines such as IFN-γ and TNF-α, and then have enhanced ability to kill intracellular and extracellular parasites by the secretion of reactive oxygen species (ROS) and nitric oxide (NO);
Phagocytes release inflammatory mediators (eg leukotrienes such as LTB4 and prostaglandins such as PGE2), and have receptors for some complement components and for antibodies (immunoglobulins) and for structures on pathogens such as the F-met-leu-phe peptide found on all bacterial proteins. Bacteria, having been recognized, are then either:
Endocytosed if small, by virtually any cell by non-specific pinocytosis, or by binding to a specific cell surface receptor. Following internalization, endocytic vesicles fuse to form endosomes, which then fuse with primary lysosomes to form secondary lysosomes in which the bacteria are digested.
Phagocytosed, if large, by neutrophils, monocytes and macrophages. The plasma membrane of the phagocyte expands around and encloses the bacteria, forming a phagosome in which toxic oxygen metabolites termed reactive oxygen species (ROS) (superoxide anion, hydrogen peroxide, hydroxyl radical and singlet oxygen), along with nitric oxide (NO) kill the micro-organism, which is later digested by a process similar to that in endocytosis.
Conclusion
The immune system employs various cells to protect humans against pathogens.
Cells of the immune system are functionally categorized into lymphocytes, APCs, and killing cells.
Cells of the immune system interact with each other, and with other components of the immune system to provide effective protection.