London (UK): Health and Social Care Information Centre;
Goodwin M, Sanders C, Davies G, Walsh T, Pretty IA. Issues arising following a referral and subsequent wait for extraction under general anaesthetic: impact on children. BMC Oral Health. 2015; 15
London (UK): Department of Health; 2000
London (UK): The Association of Paediatric Anaesthetists of Great Britain and Ireland; 2011
Rodd H, Hall M, Deery C, Gilchrist F, Gibson BJ, Marshman Z. ‘I felt weird and wobbly.’ Child-reported impacts associated with a dental general anaesthetic. Br Dent J. 2014; 216
: The Royal College of Anaesthetists and The Association of Anaesthetists of Great Britain and Ireland; 2008
Hosey MT, Bryce J, Harris P, McHugh S, Campbell C. The behaviour, social status and number of teeth extracted in children under general anaesthesia: a referral centre revisited. Br Dent J. 2006; 200:331-334
Davies C, Harrison M, Roberts G.: Royal College of Surgeons England; 2008
Report of the Intercollegiate Advisory Committee for Sedation in Dentistry.London (UK): The Dental Faculties of the Royal Colleges of Surgeons and the Royal College of Anaesthetists; 2015
Graves CE, Berkowitz RJ, Proskin HM, Chase I, Weinstein P, Billings R. Clinical outcomes for early childhood caries: influence of aggressive dental surgery. J Dent Child (Chic). 2004; 71:114-117
Berkowitz RJ, Amante A, Kopycka-Kedzierawski DT, Billings RJ, Feng C. Dental caries recurrence following clinical treatment for severe early childhood caries. Pediatr Dent. 2011; 33:510-514
Amin M, Nouri R, ElSalhy M, Shah P, Azarpazhooh A. Caries recurrence after treatment under general anaesthesia for early childhood caries: a retrospective cohort study. Eur Arch Paediatr Dent. 2015; 16:325-331
Poureslami HR, Van Amerongen WE. Early Childhood Caries (ECC): an infectious transmissible oral disease. Indian J Pediatr. 2009; 76:191-194
Shepherd AR, Hill FJ. Orthodontic extractions: a comparative study of inhalation sedation and general anaesthesia. Br Dent J. 2000; 188:329-331
Arch LM, Humphris GM, Lee GT. Children choosing between general anaesthesia or inhalation sedation for dental extractions: the effect on dental anxiety. Int J Paediatr Dent. 2001; 11:41-48
Blain KM, Hill FJ. The use of inhalation sedation and local anaesthesia as an alternative to general anaesthesia for dental extractions in children. Br Dent J. 1998; 184:608-611
: Public Health England; 2014
Holland IS, Walls AW, Wallwork MA, Murray JJ. The longevity of amalgam restorations in deciduous molars. Br Dent J. 1986; 161:255-258
Innes N, Stewart M, Souster G, Evans D. The Hall Technique; retrospective case-note follow-up of 5-year RCT. Br Dent J. 2015; 219:395-400
London: General Dental Council; 2013
Subka S. Validity and acceptability of a laser fluorescence device compared to conventional methods for detection of proximal caries in primary teeth.: The University of Sheffield; 2015
This article aims to provide general dental practitioners (GDPs) with the knowledge to improve their referrals primarily for children who they feel require a dental general anaesthetic. It discusses the impact of a general anaesthetic (GA) on a child and the financial impacts of dental general anaesthetics (DGAs). The risks of DGAs are well recognized and the ways in which the dental team in primary, secondary care and service commissioners can reduce the risk of repeat DGAs are discussed.
CPD/Clinical Relevance: Dentists should be aware of the risks involved in GA and the importance of reducing repeat DGAs.
Article
Dental caries is a preventable disease, yet it is still the most common reason a child between five to nine years old is admitted to hospital in England and Scotland.1 Dental caries can have a significant impact on children‧s lives; they may suffer pain, difficulty eating, sleepless nights, have time off school and it can affect their body weight, cause communication difficulties and impaired cognitive development.2 Dental caries is often treated under general anaesthetic (GA), particularly if the patient is pre-cooperative, anxious, medically compromised or because of the nature of the treatment.
In addition to the impact of caries on a child‧s life there are also risks associated with a GA and therefore it should only be undertaken when absolutely necessary.3 Short-term effects include nausea, vomiting, headache, sore throat, dizziness and mild allergic reaction; these usually resolve in 48 hours but can take up to a fortnight.4 Recent research5 has identified pre-, peri- and post-operative impacts of dental general extractions from a child‧s perspective. Interestingly, the most negative physical impact described was not pain but hunger and disturbed eating and, in some cases, the children reported greater discomfort from the cannula post-operatively than from the extractions. A dental general anaesthetic (DGA) has been said to carry a risk of a life-threatening problem of about 1 in 400,000, which is considerably less than a child being seriously injured in a road accident.6 With correct assessment, treatment planning and preventive care the number of children undergoing a repeat DGA can be markedly reduced.
Cost of dental general anaesthetics in the UK
The cost of hospital admissions for the treatment of caries in children in England in 2012/13 was £30 million7 and this increased to £35 million for tooth extractions in 2014/15.8 The rate of tooth extractions was 462.2 per 100,000 population in 2014/15 (33,871 episodes of care). This is statistically similar to 2013/14 (455.5 per 100,000 population, 32,741 episodes), but a significant increase since the start of the time series in 2011/12 (445.7 per 100,000 population, 30,761 episodes).9
Dental general anaesthetics services
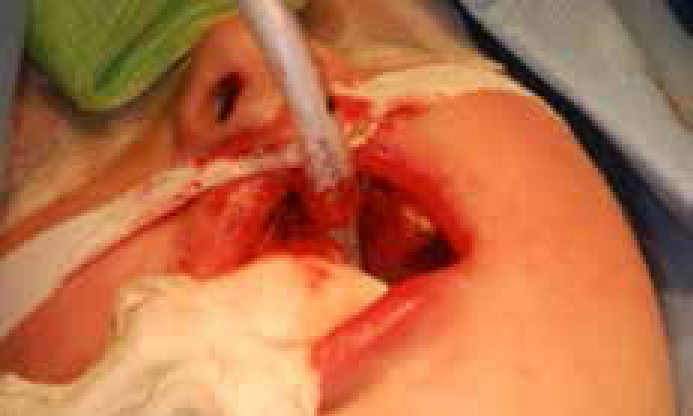
In the UK, since 2001, DGA has been restricted to a hospital setting. There are differing services available but, unfortunately, a postcode lottery still exists as to which services can be accessed. Some NHS Trusts may only offer an extraction DGA ‘exodontia’, while others offer a comprehensive care service with and without access to intra-oral radiographs peri-operatively. Comprehensive dental care under GA is primarily available for medically compromised patients or those needing complex care. This latter service is clearly superior to an extraction only service. A study of children presenting for DGA extractions concluded that perhaps ‘pre-cooperative’ children should have a greater opportunity for tooth restoration rather than extraction under general anaesthetic.10Figure 1 shows a child with oral intubation about to undergo comprehensive dental care and Figure 2 a child having extractions under GA.
Figure 1. A child with oral intubation about to undergo comprehensive care under general anaesthesia.Figure 2. A child who has had all primary molars and upper primary incisors removed under GA.
There is useful guidance available for the use of GA in paediatric dentistry.4,11,12 Both the Guidelines for the Management of Children Referred for Dental Extractions under General Anaesthesia4 and the recent Standards for Conscious Sedation in the Provision of Dental Care12 recommend that all children should be under the care of a Consultant in Paediatric Dentistry and treatment planned by a specialist with appropriate training. This recommendation has not been implemented across the UK. In fact, the majority of children are treated on direct referral from a GDP to an exodontia list, without a comprehensive assessment including radiographs.
Full treatment planning by a specialist or consultant will reduce the incidence of repeat DGA. After all, is there any other group of patients who have treatment under GA without a specialist or consultant treatment plan in place? Why does this matter? Poor assessment and treatment planning will result, as evidenced below, in unjustifiable repeat procedures.
Repeat dental general anaesthetics
Unfortunately, new carious lesions have been reported in 37–52% of children only six months after their initial treatment under GA.13,14 In a recent cohort study,15 the recurrence of caries (relapse) rate was 21.6% during a three-year follow-up. This study identified that ASA-2 children and those with less than a full primary dentition present at the initial GA were almost three times more likely to experience relapse as compared with ASA-1 and children with more than 20 teeth present. A survey of children attending six district general hospitals in the north-west of England found 12–37% of these patients were attending for a repeat DGA.2 These hospitals provided in the main a direct referral to the GA appointment without a treatment planning visit. On the other hand, consultant led services with pre-assessment including radiographs (either before or during the procedure for pre-cooperative children) show repeat GA rates within two years of approximately 1%. It must be remembered that these services will see many ASA II patients and these are included in these figures.
In addition to the effects on the child of a repeat GA, it impacts on already highly stretched services in several areas including waiting list length, staffing and financial pressures.
Of course, the best outcome would be if the patient‧s caries risk could be reduced from high to low. Unfortunately, those with a high caries risk are more susceptible to further carious lesions16 and, due to the aforementioned risks, it is essential that patients undergoing a DGA have their caries addressed in such a way as to minimize new lesion development.
Appropriate treatment planning
A DGA should only be undertaken if it is the most appropriate form of clinical management for the patient. It is often used to manage the most anxious children but it is important to remember that this process can be distressing for both the child and his/her parent and may compound existing dental anxiety.
In some patients, DGA will be the most appropriate first line treatment strategy. However, for others, behavioural management techniques alongside local anaesthetic (LA), LA and inhalation sedation (IS) or intravenous sedation (for young people aged 12–16 years12) should be appropriately considered for the provision of dental treatment rather than necessarily proceeding straight to DGA. Various studies have shown less morbidity and psychological distress when opting for IS.17,18 Similarly, to the DGA services, the availability of these options varies greatly between areas, so it is important that the services available in a particular region are known.
The referring practitioner must ensure that patients are aware that they are not necessarily going to receive a GA. Dentists should be aware that orthodontic extractions of erupted permanent premolar teeth are rarely undertaken under GA in healthy children11 owing to the evidence of success in managing these extractions under inhalation sedation,19 so GDPs should not propose this as an option to children and their parents. However, since this article is focusing on DGA and reducing repeat DGAs, we will not discuss these management strategies any further.
The importance of thorough treatment planning to prevent repeat GA cannot be overemphasized. When the decision has been made to proceed with GA it is essential to minimize and ideally eliminate repeat GAs. GDPs have a duty of care to provide preventive information to children and their parents and it must be stressed that the child is susceptible to further carious lesions if it is not followed. Some units will offer preventive care alongside a GA appointment but this is not the norm. In any case, the child‧s dental practice is the only site where effective ongoing prevention can be provided, and the GDP should refer to Delivering Better Oral Health: an Evidence-based Toolkit for Prevention for this.20
As well as the focus on prevention, it is important to manage existing caries appropriately prior to an exodontia DGA. All carious teeth that are amenable to restoration should be restored prior to the GA, as the patient may refuse restorative treatment planned for after the GA. Therefore, all specialists plan for the patient to wake dentally fit with no remaining restorative treatment need. The waiting period for exodontia services are a lot shorter than comprehensive care services (but availability varies from area to area), so if a child can co-operate for restorative treatment but not extractions, appropriate, timely, restorative treatment followed by exodontia will minimize his/her time in pain by avoiding the wait for a comprehensive GA list.
All restorative care should be provided to an adequate standard. For example, intra-coronal restorations placed without LA have a much poorer prognosis than those that are placed with it.21 The success of the Hall Technique using preformed metal crowns22 means that these are a very effective treatment and can be left in place at the time of the GA.
The specialist or consultant treatment planning works to the rule that any tooth whose prognosis is unclear will be removed. Therefore, restorations placed without local anaesthetic or large restorations – either in terms of area or closeness to the pulp – will be removed. The aim is to try to ensure that there is no reason for further treatment within two years.
The role of the GDP in the referral process
Table 1 presents the information required for a new patient consultation at a dental hospital and associated children‧s hospital within the UK and highlights relevant information that GDPs should be providing in their referral letters. The provision of this information will aid consultants and specialists, should minimize repeat radiographs and generally improve the pathway of care for patients.
Information Required
Urgency
Pain history
Language
Is an interpreter required?
Detailed medical history
Provide an up-to-date medical historyIncluding any hospital treatment they are receiving or due to receive
Detailed social history
How will they travel to and from the hospital?
Detailed dental history
Are they a regular or symptomatic attender?Has any treatment been provided? Was restorative treatment completed with LA. What is their view of the prognosis of the restorations present?
Oral hygiene habits
Adherence to the Oral Health Prevention Toolkit
Clinical and radiographic examination
Provide a full clinical reportProvide radiographs or confirm none has been taken and send the radiographs, with the referral (either originals or CD – print not acceptable, as these are of very low diagnostic value)
Provision of information to parents and consent
The parents must be informed of the risks of a general anaesthetic if this is the reason for referral
Many services provide a ‘one stop’ service working to the GDP‧s treatment plan and, unfortunately, these are the services with the highest repeat GA rates.2 Therefore, it is essential to know to which service the referral is being made, as starved children with anxious parents presenting to an assessment appointment expecting a GA is never appropriate. This can cause people to be understandably upset or even angry and is clearly completely avoidable with some thinking ahead.
Informed consent must be obtained in writing from a parent or guardian with parental responsibility.23 It is important that the family is advised of this at the time of referral as often patients attend appointments with grandparents who are unable to provide consent unless they are the legal guardians; this can cause frustration and delay to a patient‧s treatment.
Importance of radiographic examination
Every effort should be made to obtain as detailed a clinical and radiographic examination as possible to avoid repeat general anaesthetics. Dentists often seem to dismiss children‧s ability to be able to cope with radiographs, without even attempting to take them. This has been found not to be the case in a study of 82 children (mean age 6.4 years) referred for extractions under GA, which reported that only a small percentage (10%) found it ‘hard’ or ‘very hard’ to accept radiographs; the majority (75%) found it ‘very easy’ or ‘easy’ and the remaining 15% didn't mind it.24 If the child is unable to tolerate radiographs due to behavioural or medical issues, the facilities to take radiographs under GA should be available and utilized, as a comprehensive treatment plan is not possible without them.11
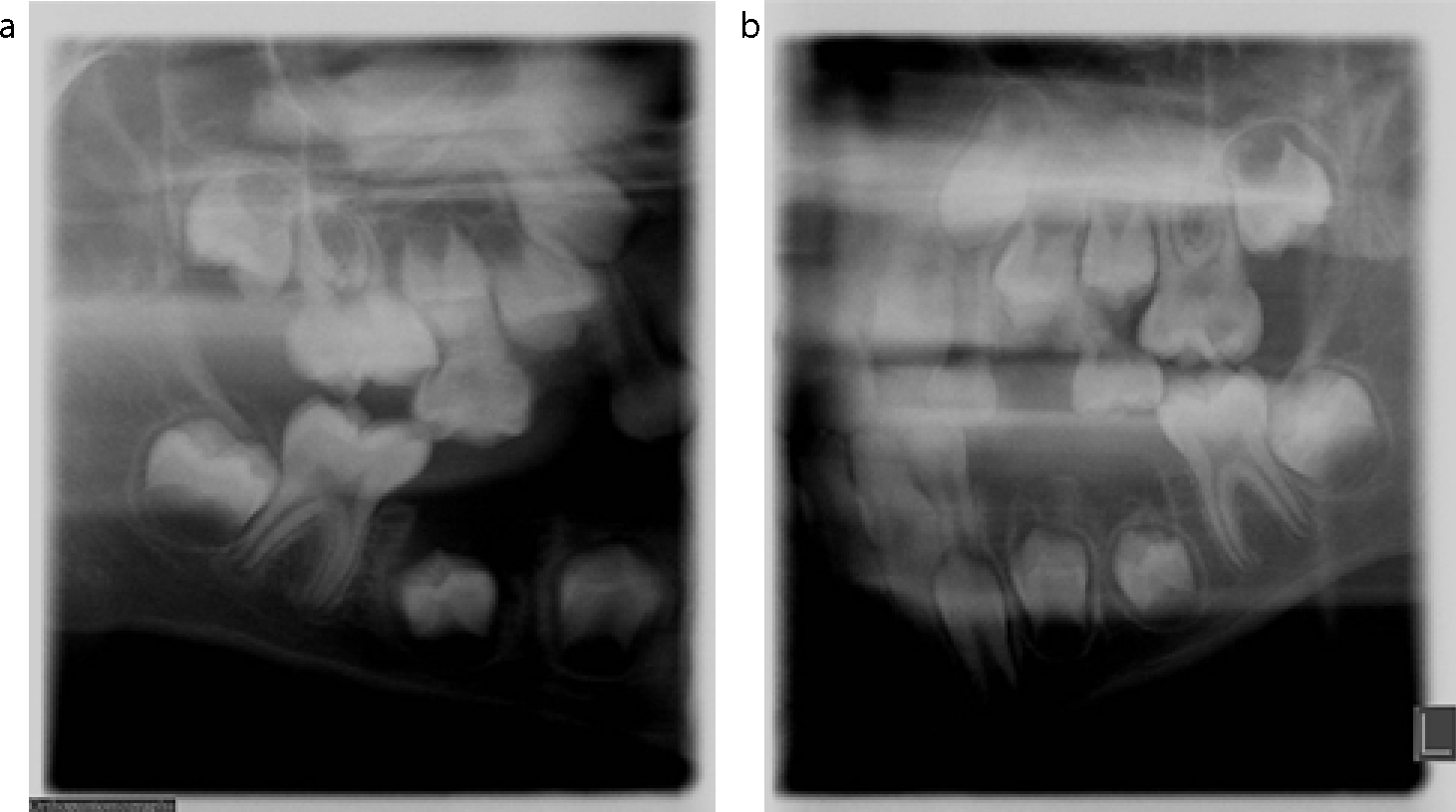
A mouth can appear ‘caries free’ or, as is often the case when a patient is referred from his/her general dental practitioner, that ‘a single cavitated lesion is present’ and radiographic examination reveals multiple interproximal lesions. Figures 3a and b show a child referred for management of an unrestorable upper left first primary molar. The other teeth appeared clinically sound. However, once bitewing radiographs were taken (Figures 3c and d), the following was diagnosed: mesial dentine caries upper right, lower left and lower right first primary molars and the upper left second primary molar. There is also an impacted upper left first permanent molar, which has resorbed the upper left second primary molar to involve the pulp. If this child had proceeded to exodontia without a full assessment including radiographs, the treatment plan would have been inappropriate and could have resulted in a repeat general anaesthetic within a short time.
Figure 3. The upper and lower dental arches of a 6-year-old child referred because of unrestorable caries in upper left first primary molar. (a) Upper arch showing the caries in upper left first primary molar. (b) Apparently caries-free lower arch. (c, d) Right and left bitewing radiographs showing mesial dentine caries in upper right, lower left, lower right first primary molars and upper left second primary molar. There is mesial enamel caries in upper right, lower left, lower right second primary molars and upper left first primary molar. There is also an impacted upper left first permanent molar.
Dentists should all be aware of the guidelines available for taking radiographs and follow the appropriate intervals, depending on caries risk, as laid out in the FGDP‧s Selection Criteria for Dental Radiography25 and always, when cooperation allows, before referral for GA, especially when referring to a ‘one stop’ service without the facilities for assessment and treatment planning by a specialist or consultant.
Examples of poor assessment
Below are three cases where poor assessment and treatment planning has led to pain, increased anxiety, time off school and work for patients and their parents or guardians and a repeat GA in a short time span. They were initially seen at services not run by paediatric dentists but were then seen at the Paediatric Dentistry Department at Charles Clifford Dental Hospital, Sheffield because of further pain from the remaining teeth.
Figure 4 shows a sectional OPG bitewing from an 8-year-old child. The patient presented in pain two weeks after having a GA for the removal of the upper left first primary molar, lower right and left first and second primary molars. This radiograph demonstrates ectopic eruption of the maxillary first permanent molars (upper left first permanent molar into pulp of the upper left second primary molar and the upper right first permanent molar close to pulp of the upper right second primary molar) and caries in the upper left first permanent molar. The patient‧s level of anxiety means that she will require a further GA to complete her treatment.
Figure 4. (a, b) Sectional OPG taken only 2 weeks after the patient had received a DGA. It demonstrates the impacted upper right and left second molars and caries in the occlusal surface of upper left first molar.
Figure 5 presents the clinical images and sectional OPG of a five-year-old girl who presented with pain affecting her sleep ten days after having her upper right second primary molar and lower right first primary removed under GA at a ‘one stop’ service without treatment planning by a specialist or consultant. With the exception of the caries detected on the radiograph in the upper left first primary molar, the caries is obvious clinically. The referring dentist had clearly neither made adequate treatment plans nor made an adequate referral for her first DGA.
Figure 5. The upper and lower arches and right and left bitewings of a child who had had upper right second primary molar and lower right first primary molar removed under GA 10 days previously. (a) Upper arch showing healing socket in upper right second primary molar. Caries in upper right primary canine and upper left primary second molar. There is also significant tooth surface loss affecting the upper primary incisors. (b) Lower arch showing healing in lower right first primary molar. Caries in lower left first and second primary molars and possibly lower right second primary molar. (c) Sectional OPG showing, in addition to the caries noted clinically, caries in upper left first primary molar
Figure 6 presents a 3-year-old pre-cooperative child who had had an upper clearance and his lower primary molars removed two weeks previously. He presented in severe pain and required the removal of his lower anterior teeth under GA, as an urgent procedure.
Figure 6. Anterior view of 3-year-old patient who had had an upper clearance and his lower primary molars removed two weeks previously under GA. The caries present in his remaining lower teeth is obvious.
Treatment for all three of the above cases was not planned by a specialist/consultant in paediatric dentistry. It is clear that all three should not have needed a repeat GA had they received comprehensive treatment planning prior to their first DGA. They are examples of what must be happening across the country because of inadequate services. These services must undertake audits and service evaluations in order to improve standards of care and identify areas, for example, inadequate assessment that may lead to a high incidence of repeat procedures.
Conclusion
Despite the risks and impacts to patients and their families, DGA remains an important way of managing dental disease for children, but it is important that a child is under the care of a paediatric dental consultant or specialist to optimize care and minimize the risk of repeat DGA. The DGA must not be a standalone procedure – prevention is key to minimize further the risk of recurrence of dental disease and the Delivering Better Oral Health: an Evidence-based Toolkit for Prevention20 is an invaluable toolkit for dental care professionals.
Referring clinicians have a responsibility to make sure that patients are appropriately referred for treatment. They should ensure that carers are aware of the different options available and the risks involved.