Socransky SS. Relationship of bacteria to the etiology of periodontal disease. J Dent Res. 1970; 49:203-222
Socransky SS, Haffajee AD. The bacterial etiology of destructive periodontal disease: current concepts. J Periodontol. 1992; 63:322-331
Grossi SG, Genco RJ, Machtei EE, Ho AW, Koch G, Dunford R Assessment of risk for periodontal disease. II. Risk indicators for alveolar bone loss. J Periodontol. 1995; 66:23-29
Clarke NG, Hirsch RS. Personal risk factors for generalized periodontitis. J Clin Periodontol. 1995; 22:136-145
Page RC, Sims TJ, Geissler F, Altman LC, Baab DA. Defective neutrophil and monocyte motility in patients with early onset periodontitis. Infect Immun. 1985; 47:169-175
Tal M. Periodontal disease and oral hygiene. Described by Antonic van Leeuwenhoek. J Periodontol. 1980; 51:668-669
Socransky SS, Haffajee AD, Smith C, Dibart S. Relation of counts of microbial species to clinical status at the sampled site. J Clin Periodontol. 1991; 18:766-775
Socransky SS, Haffajee AD, Cugini MA, Smith C, Kent RL Microbial complexes in subgingival plaque. J Clin Periodontol. 1998; 25:134-144
Ali RW, Skaug N, Nilsen R, Bakken V. Microbial associations of 4 putative periodontal pathogens in Sudanese adult periodontitis patients determined by DNA probe analysis. J Periodontol. 1994; 65:1053-1057
Grant DA, Flynn MJ, Slots J. Periodontal microbiota of mobile and non-mobile teeth. J Periodontol. 1995; 66:386-390
Mombelli A, Casagni F, Madianos PN. Can presence or absence of periodontal pathogens distinguish between subjects with chronic and aggressive periodontitis? A systematic review. J Clin Periodontol. 2002; 29:10-21
Duarte PM, Bastos MF, Fermiano D, Rabelo CC, Perez-Chaparro PJ, Figueiredo LC, Faveri M, Feres M. Do subjects with aggressive and chronic periodontitis exhibit a different cytokine/chemokine profile in the gingival crevicular fluid? A systematic review. J Periodontal Res. 2015; 50:18-27
Chapple IL, Genco R. Working Group 2 of Joint EFP/AAP Workshop. Diabetes and periodontal diseases: consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J Clin Periodontol. 2013; 40:106-112
Angelopoulos AP, Goaz PW. Incidence of diphenylhydantoin gingival hyperplasia. Oral Surg Oral Med Oral Pathol. 1972; 34:898-906
Seymour RA, Thomason JM, Ellis JS. The pathogenesis of drug-induced gingival overgrowth. J Clin Periodontol. 1996; 23:165-175
Ellis JS, Seymour RA, Steele JG, Robertson P, Butler TJ, Thomason JM. Prevalence of gingival overgrowth induced by calcium channel blockers: a community-based study. J Periodontol. 1999; 70:63-67
Calsina G, Ramón JM, Echeverría JJ. Effects of smoking of periodontal tissues. J Clin Periodontol. 2002; 29:771-776
Martinez-Canut P, Lorca A, Magán R. Smoking and periodontal disease severity. J Clin Periodontol. 1995; 22:743-749
Breivik T, Thrane PS, Murison R, Gjermo P. Emotional stress effects on immunity, gingivitis and periodontitis. Eur J Oral Sci. 1996; 104:327-334
Armitage GC. The complete periodontal examination. Periodontol 2000. 2004; 34:22-33
Miller SC.Philadelphia: P Blakiston's Son & Co Inc; 1938
Hamp SE, Nyman S, Lindhe J. Periodontal treatment of multirooted teeth. Results after 5 years. J Clin Periodontol. 1975; 2:126-135
Davies SJ, Gray RJ, Linden GJ, James JA. Occlusal considerations in periodontics. Br Dent J. 2001; 191:597-604
Armitage GC, Cullinan MP. Comparison of the clinical features of chronic and aggressive periodontitis. Periodontol 2000. 2010; 53:12-27
Armitage GC. Periodontal diagnoses and classification of periodontal diseases. Periodontol 2000. 2004; 34:9-21
Armitage GC. Development of a classification system for periodontal diseases and conditions. Ann Periodontol. 1999; 4:1-6
Diagnosis and management of chronic and aggressive periodontitis part 1: periodontal assessment and diagnosis Despoina Chatzistavrianou Fiona Blair Dental Update 2024 44:4, 707-709.
Authors
DespoinaChatzistavrianou
DDS MFDS RCSEd, MClinDent Pro, MPros RCSEd
Specialist in Prosthodontics, Specialty Registrar in Restorative Dentistry, Birmingham Dental Hospital and University of Birmingham School of Dentistry, Birmingham Community Healthcare NHS Trust, Birmingham, UK
Periodontal disease remains one of the most common diseases that affect the oral cavity. The differential diagnosis between chronic and aggressive periodontitis can be complex for some clinicians and the correct diagnosis is a key element in disease management. The three-part series will review periodontal clinical assessment and diagnosis, periodontal management and finally will discuss two clinical cases. This paper will focus on periodontal disease pathogenesis, periodontal clinical assessment and diagnosis.
CPD/Clinical Relevance: This paper aims to provide the general dental practitioner with an understanding of periodontal disease pathogenesis and to highlight elements in the clinical assessment which will help to establish the diagnosis.
Article
What is the aetiology of periodontal disease?
Periodontal disease is a complex inflammatory disease that affects the periodontal structures, including the gingiva, cementum, periodontal ligament and alveolar bone.1 Both chronic and aggressive periodontitis are plaque-related diseases initiated by bacteria (Figure 1).2 The host response, genetic predisposition and environmental risk factors do not initiate periodontal disease, however, can influence the extent and severity of periodontal disease (Table 1,Figure 2).3,4,5,6
Local Risk Factors
Systemic Risk Factors
Calculus
Smoking
Partial dentures
Diabetes, hormonal changes such as pregnancy
Overhanging and poorly contoured restorations
Certain medications
Malpositioned teethOpen contacts
Genetic predisposition
Furcations, root grooves and concavities, enamel pearls
Stress
Figure 1. Diagrammatic representation of the aetiology of periodontal disease.Figure 2.
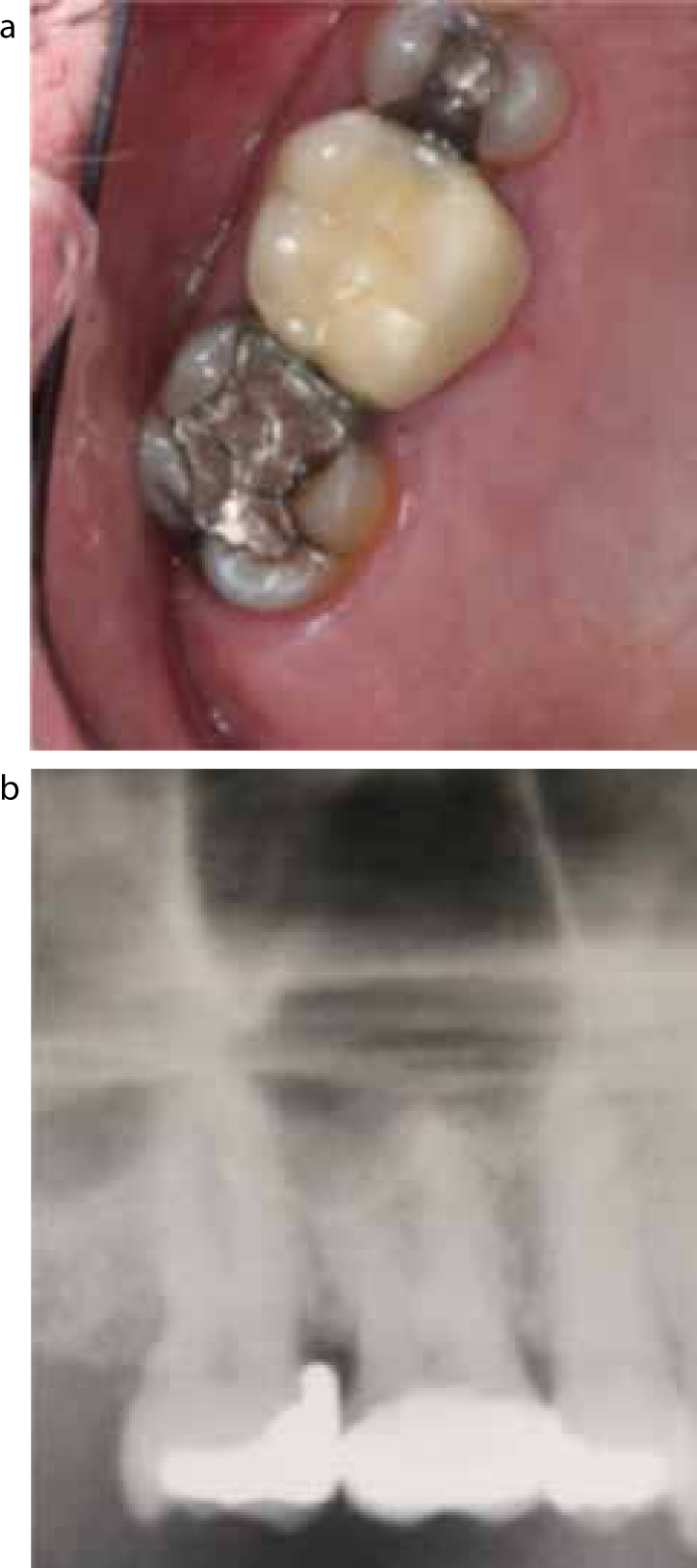
(a, b) A poorly contoured restoration resulted in increased pocket depth with bleeding on probing in the UR7 site. Replacement of the restoration and root surface debridement eliminated the pocket depth and bleeding on probing.
Which bacteria can cause periodontal disease?
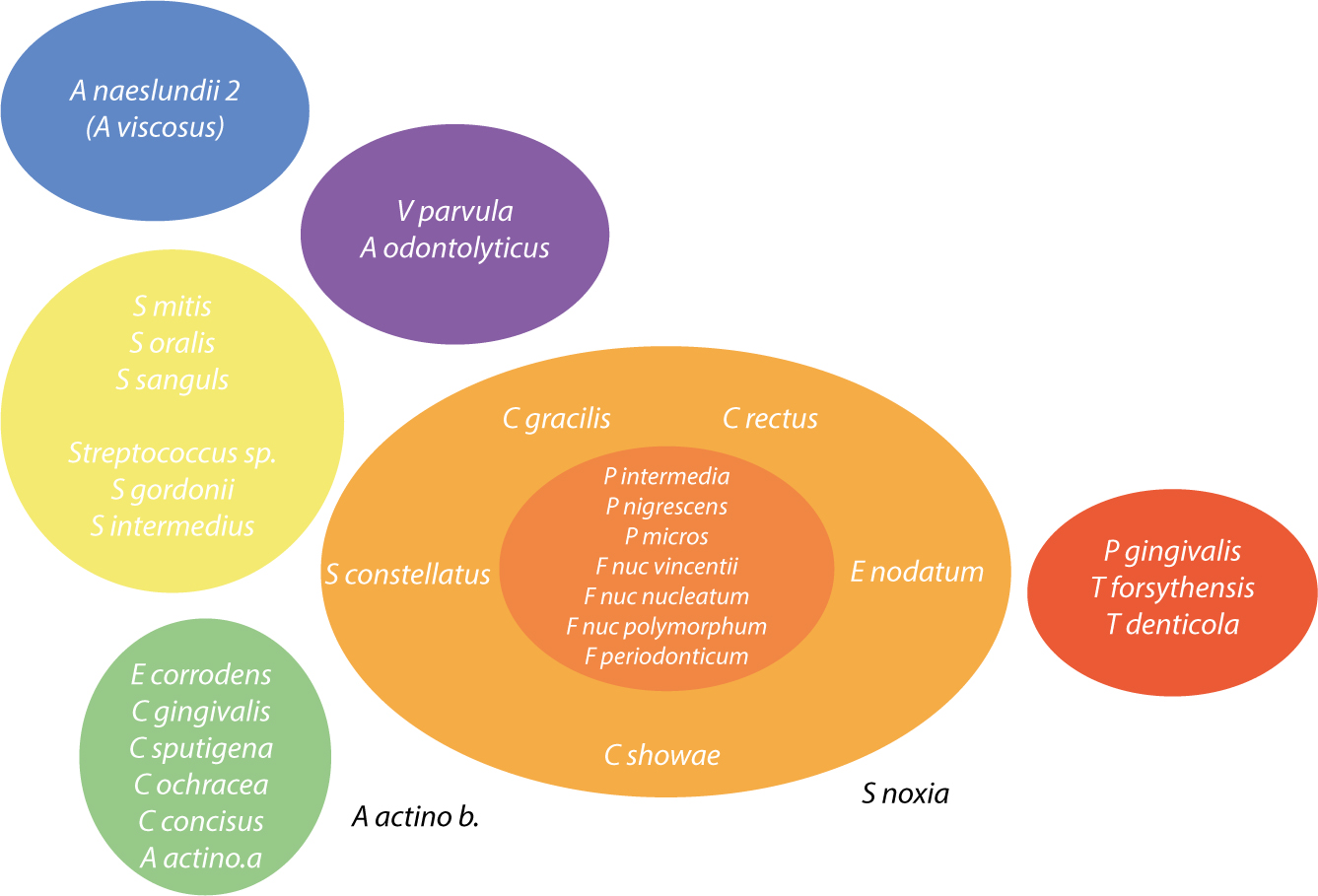
Subgingival plaque consists of a large and complex bacterial mixture of 400 or more species; certain bacterial combinations, under specific circumstances, can promote periodontal tissue breakdown.7 The bacterial species involved in the initiation and progression of periodontal disease have been classified based on their pathogenicity and grouped into complexes (Figure 3).8
Figure 3. Diagrammatic representation of the relationships between the microbial complexes.10
The most commonly reported red complex periodontal pathogens, Porphyromonas gingivalis, Aggregatibacter actinomycetemcomitans, Treponema denticola and Tannerella forsythia are anaerobic, Gram-negative organisms highly associated with increased pocket depth and bleeding on probing, especially P. gingivalis.8,9,10 Orange complex bacteria are associated with increased pocket depth, while bacteria in yellow, green and purple complexes are generally associated with healthy periodontal sites (Figure 3).8,9,10,11,12
Aggregatibacter actinomycetemcomitans, although commonly related with aggressive periodontitis, is not a categorical prognostic factor for this category of disease as its presence is not always detected in a number of patients diagnosed with aggressive periodontitis.13 Also, no differences could be detected in the crevicular fluid content for patients with aggressive periodontitis and chronic periodontitis.14
Clinical assessment of periodontal disease
A comprehensive periodontal examination is an essential component of periodontal management in order to determine the diagnosis and develop an effective management plan. The complete periodontal examination consists of three elements:
A detailed history;
The clinical examination; and
The radiographic examination.
Patient complaint and history
The patient's history of complaint(s) should be thoroughly investigated using open questions that explore the duration and severity of symptoms, any exacerbating or relieving factors, and the nature and detail of treatment that has been provided so far.
A detailed medical history will identify systemic diseases or medications that may be affecting periodontal tissues. Diabetes and periodontal disease are both complex chronic diseases with a bi-directional relationship.15 Hyperglycaemia in diabetes is related to adverse periodontal outcomes and a quantifiable relationship between periodontal disease severity and diabetes complications is reported.15 Medication, including phenytoin, cyclosporine and calcium channel blocking antihypertensives, can be related to gingival enlargement in susceptible patients and with suboptimal oral hygiene.16,17,18
Recent or past social history regarding smoking and stress levels should be noted. Smokers have a 2–6 times greater risk of periodontal disease, increased pocket depth and attachment loss compared to non-smokers.19 Smoking has a dose-related effect on periodontal disease; smoking 1, up to 10 or up to 20 cigarettes per day increases attachment loss by 0.5%, 5% and 10%, respectively.20 Emotional or psychological stress may influence the immune response to periodontal pathogens, and thus the progression and severity of periodontal disease.21
Oral hygiene habits, including toothbrushing frequency and technique, and use of interdental cleaning aids, demonstrates patient motivation and should be recorded. Formal intra-oral demonstration of oral hygiene techniques should have been undertaken as a pre-requisite for the management of periodontal disease and this should be noted alongside previous periodontal disease diagnosis and treatment provided so far.
Clinical examination
Thorough clinical examination of extra- and intra-oral tissues should be carried out as a norm, noting alterations in colour, contour and texture that may raise clinical suspicion and become additionally important if contributing to functional or aesthetic concerns.22
The required starting point of the periodontal examination is the Basic Periodontal Examination (BPE), a rapid screening tool that provides information regarding the next level of examination and treatment needed (Table 2, Figure 4).
BPE Scores
Scoring Codes
Interpretation of BPE Scores
0
No pockets >3.5 mm, no calculus/overhangs, no bleeding after probing (black band completely visible)
No need for periodontal treatment
1
No pockets >3.5 mm, no calculus/overhangs, but bleeding after probing (black band completely visible)
Oral hygiene instruction (OHI)
2
No pockets >3.5 mm, but supra- or subgingival calculus/overhangs (black band completely visible)
OHI, removal of plaque retentive factors, including all supra- and subgingival calculus
3
Probing depth 3.5–5.5 mm (black band partially visible, indicating pocket of 4–5 mm)
OHI, root surface debridement (RSD)
4
Probing depth >5.5 mm (black band entirely within the pocket, indicating pocket of 6 mm or more)
OHI, RSD. Assess the need for more complex treatment; referral to a specialist may be indicated
*
Furcation involvement
OHI, RSD. Assess the need for more complex treatment; referral to a specialist may be indicated
Figure 4. The WHO probe has a 0.5 mm diameter ball end and black banding of 3.5, 5.5, 8.5 and 10.5 mm.
The BPE score should be recorded with the WHO probe (often called a BPE probe). The WHO probe has a ball end 0.5 mm in diameter, and a black banding from 3.5–5.5 mm and 8.5–10.5 mm. A light probing force of between 20–25 grams should be used. Code 3 requires recording a 6-point pocket chart in that sextant only at post-treatment review and code 4 requires recording a 6-point pocket chart for the entire dentition pre-treatment and at post-treatment review.
The presence and site of plaque and calculus deposits, restoration overhangs/deficiencies, gingival inflammation, bleeding on probing or suppuration should be recorded.22 Gingival recession, mobility, furcation involvement, spacing and change in tooth position should be noted since they help determine the diagnosis and management of the periodontal disease (Tables 3 and 4).22,23,24
Tooth Mobility
Interpretation of Tooth Mobility
0
Physiologic movement when force is applied
1
Mobility less that 1 mm (horizontal)
2
Mobility more than 1 mm but less that 2 mm (horizontal)
3
Mobility both horizontal and vertical
Degree I
Horizontal loss of periodontal support up to 1/3 of the width of the root
Degree II
Horizontal loss of periodontal support exceeding the 1/3 and up to 2/3 of the width of the root
Degree III
Horizontal ‘through and through’ destruction
Occlusal analysis should identify the occlusal relationship and guiding tooth contacts in protrusion and lateral movements and any tooth clenching or habitual biting habits (nails/pens) need noting. Occlusal trauma will not initiate, but can aggravate, existing periodontal disease.25 The clinical status of existing teeth, restorations and any prosthesis should be noted to identify plaque retentive factors or teeth with guarded prognosis (Table 5).22
Patient Complaint
Bleeding gumsRecurrent infectionsMobile teethDrifting/change in tooth position
Medical History
DiabetesHormonal changes such as pregnancyMedication including phenytoin, cyclosporine and calcium channel blocking antihypertensives
Social History
Smoking (past or present, numbers of cigarettes a day, years of smoking/given up)Alcohol consumptionOccupationStress levels
Dental History
Regular/irregular attendeeOral hygiene habits (frequency and technique)Demonstration of OHI by GDP Perio Tx (by hygienist, GDP or specialist, when it was completed, if LA was used)
Extra-oral Examination
LymphadenopathyTMJSkeletal baseLip line
Intra-oral Examination
Soft tissuesOral hygiene statusGingival inflammation (localized/generalized)Plaque and calculus deposits (supra/subgingival)BOP (widespread/localized)BPERecessionFurcation involvementSpacing and change in tooth positionOcclusion (static and dynamic)Parafunction habits
Radiographic Report
Degree and pattern of bone loss (horizontal or vertical) Furcation defectsCalculus depositsApical periodontitis (perio-endo lesions, PDL widening)Status of restorations
Radiographic examination
A radiographic examination should be carried out of teeth with significant pocketing as evidenced by BPE code 3 and 4, mobility, furcation involvement or signs suggesting that other pathology may be present. Radiographs need to allow assessment of any bone loss and other pathology. Generally, bitewing views will be appropriate for BPE code 3 to ascertain bone levels or where clinical findings suggest additional investigation of caries or restorations. BPE code 4 will usually require periapical views to identify bone levels with respect to the tooth apex and possible involvement of apical tissues. Whilst dental panoramic tomographs provide a useful overview, in complex cases where there are a variety of dental problems they do not usually provide clarity of detail for assessing bone density and pattern. Periapical radiographs allow for more accurate and detailed assessment of periodontal bony defects to identify the degree and pattern of bone loss, presence of subgingival calculus deposits, any furcation or apical involvement and any other bone pathology (Table 5).22
Periodontal diagnosis
Clinical and radiographic examination will determine the periodontal diagnosis, which will guide the management plan. The periodontal diagnosis should include the type, severity and extent of the disease. Due to the different management of aggressive disease, it is important that correct differentiation from chronic disease is made and timely management is undertaken.
The primary features of aggressive periodontitis are rapid attachment loss and bone destruction inconsistent with the microbial deposits, familial aggregation and non-contributory medical history (Figure 5, Table 6).26 Localized aggressive periodontitis characteristically presents affecting first molar and incisor teeth with interproximal attachment loss on up to two or more permanent teeth (Figure 5).27 Generalized aggressive disease presentation affects at least three permanent teeth other than involved incisors and first molars.28
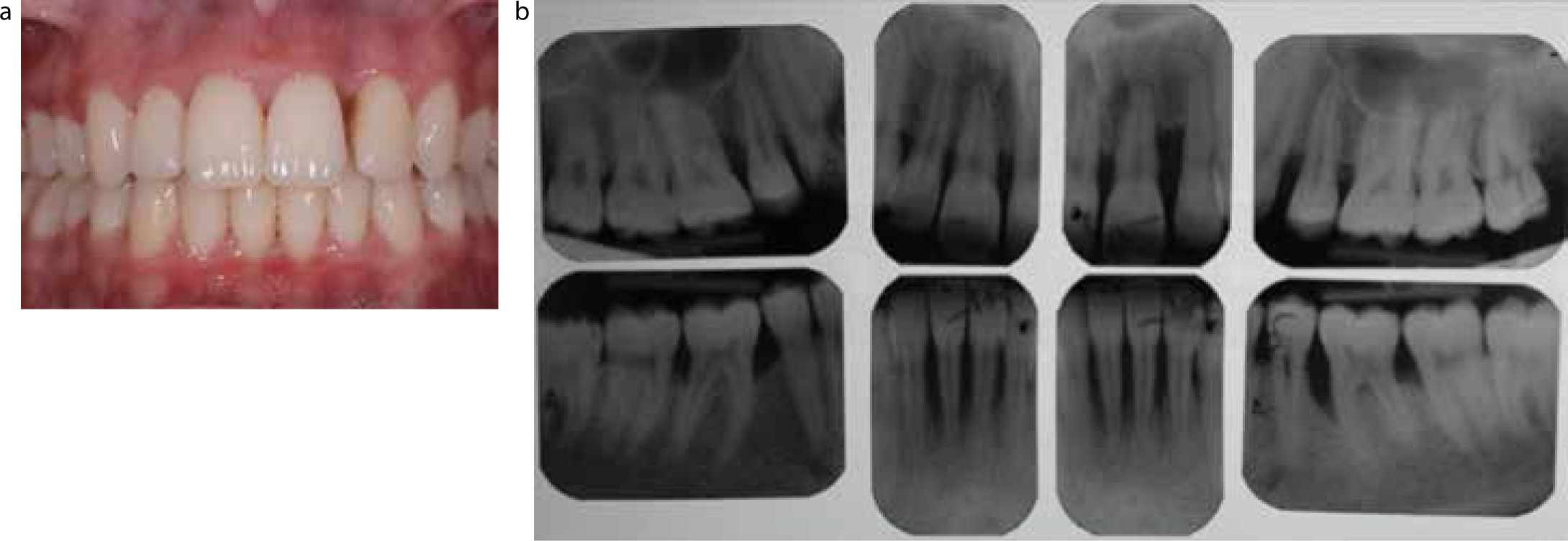
Figure 5.
(a, b) Clinical and radiographic presentation of a 17-year-old female patient with aggressive periodontitis. Rapid attachment loss and bone destruction inconsistent with the microbial deposits, familial aggregation and non-contributory medical history were noted. Vertical pattern of bone loss was noted in molars.
Aggressive Periodontitis
Chronic Periodontitis
Attachment loss
Rapid
Slow to moderate
Bone destruction in relation to the microbial deposits
Inconsistent
Consistent
Familiar aggregation
Yes
No
Medical history
Non-contributory
Contributory
Bone loss pattern
Vertical
Horizontal
Affected teeth
First molar and incisor teeth
Any in the arch
Chronic periodontal disease generally shows slow to moderate progression, which may periodically be rapid (Table 7, Figure 6).26 Associated risk factors include smoking and poor oral hygiene with usual presence of plaque and calculus deposits. The disease may be further modified by stress and systemic diseases, eg diabetes and HIV.26 Disease severity can be characterized according to clinical attachment loss (CAL) or bone loss (BL). Mild disease 1–2 mm CAL or 2–3 mm BL, moderate 3–4 mm CAL or 4–5 mm BL or severe 5+ mm CAL or 6+ mm BL (Table 7).28 The disease is considered to be localized if up to 30% of the teeth are affected and generalized if over 30% of the teeth are involved (Table 7).28
Aggressive Periodontitis Classification
Localized
Generalized
Affecting first molar and incisor teeth
Affecting at least three permanent teeth other than involved incisors and first molars
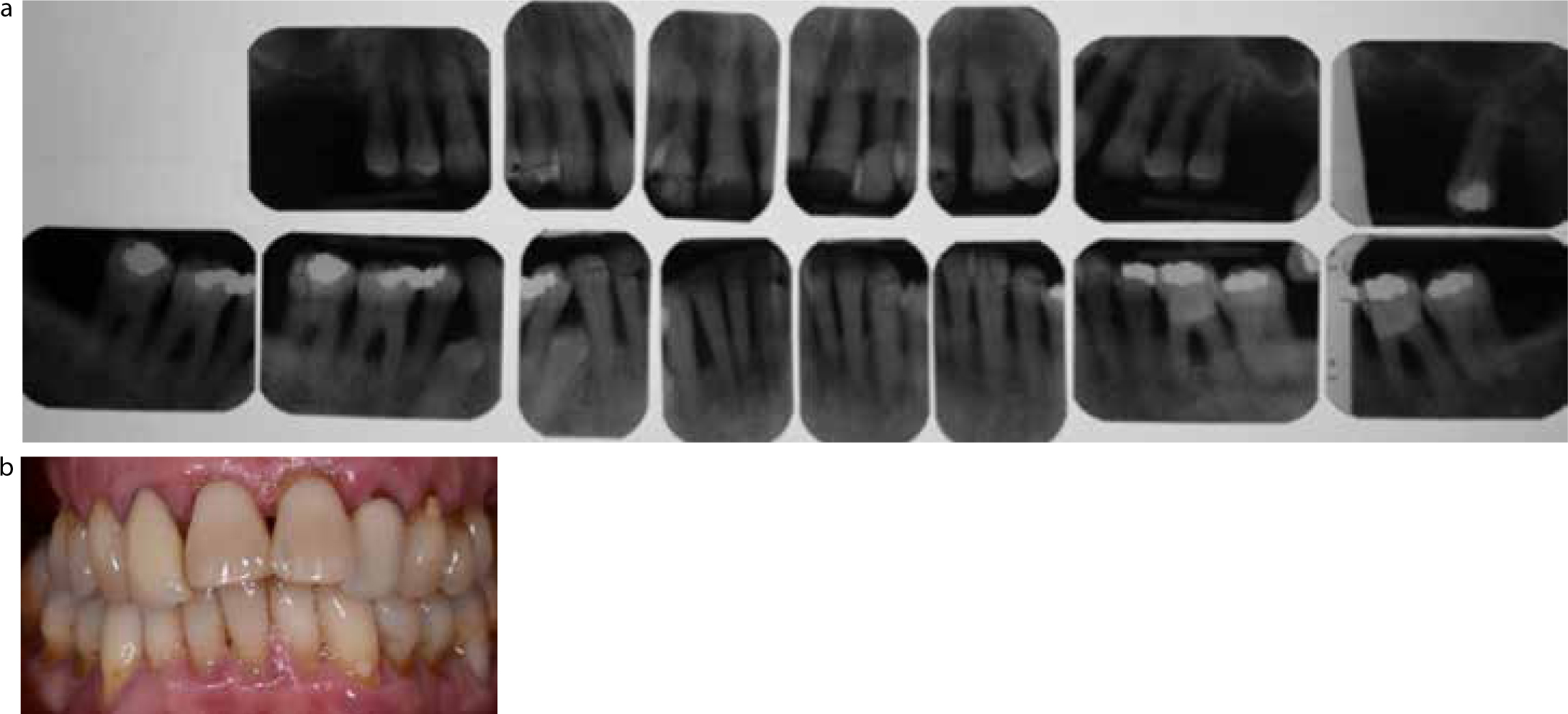
Figure 6.
(a, b) Radiographic and clinical presentation of a 69-year-old female patient with severe chronic periodontitis. Attachment loss and bone destruction were consistent with the poor oral hygiene. The periodontal disease was aggravated by smoking. Horizontal pattern of bone loss was noted in all remaining teeth.
Summary
Although our understanding of periodontal disease pathogenesis has improved, periodontal disease remains one of the most common diseases that affects the oral cavity. The differential diagnosis between chronic and aggressive periodontitis is important since the two forms of disease require different management. The management of chronic and aggressive periodontitis will be discussed in the second part of the series. A discussion of the literature will be provided in the third part of the series using two clinical examples.