Renton T, Al-Haboubi M, Pau A, Shepherd J, Gallagher JE. What has been the united kingdom's experience with retention of third molars?. J Oral Maxillofac Surg. 2012; 70:48-57
Steed MB. The indications for third-molar extractions. J Am Dent Assoc. 2014; 145:570-573
Coulthard P, Bailey E, Esposito M, Furness S, Renton TF, Worthington HV. Surgical techniques for the removal of mandibular wisdom teeth (Review). The Cochrane Library. 2014; (7)
Abu Younis Mohammed H, Abu Hantash Ra'ed O Dry socket: frequency, clinical picture, and risk factors in a palestinian dental teaching center. Open Dent J. 2011; 5:7-12
Jesudasan JS, Wahab PU, Sekhar MR. Effectiveness of 0.2% chlorhexidine gel and a eugenol-based paste on postoperative alveolar osteitis in patients having third molars extracted: a randomised controlled clinical trial. Br J Oral Maxillofac Surg. 2015; 53
Veale B. Alveolar osteitis: a critical review of the aetiology and management. Oral Surg. 2015; 8:68-77
Lodi G, Figini L, Sardella A, Carrassi A, Del Fabbro M, Furness S. Antibiotics to prevent complications following tooth extractions. Cochrane Database Syst Rev. 2012; 11 https://doi.org/10.1002/14651858.CD003811.pub2
Libersa P, Roze D, Cachart T, Libersa JC. Immediate and late mandibular fractures after third molar removal. J Oral Maxillofac Surg. 2002; 60:163-165
Mason DA. Lingual nerve damage following lower third molar surgery. Int J Oral Maxillofac Surg. 1988; 17:290-294
Chiapasco M, De Cicco L, Marrone G. Side effects and complications associated with third molar surgery. Oral Surg Oral Med Oral Pathol. 1993; 76:412-420
Rood JP. Lingual split technique. Damage to inferior alveolar and lingual nerves during removal of impacted third molars. Br Dent J. 1983; 154:402-403
Schultze-Mosgau S, Reich RH. Assessment of inferior alveolar and lingual nerve disturbances after dentoalveolar surgery, and recovery of sensitivity. Int J Oral Maxillofac Surg. 1993; 22:214-217
Rood JP. Permanent damage to inferior alveolar and lingual nerves during the removal of impacted mandibular third molars. Comparison of two methods of bone removal. Br Dent J. 1992; 172:108-110
Gargallo-Albiol J, Buenechea-Imaz R, Gay-Escoda C. Lingual nerve protection during surgical removal of lower third molars. A prospective randomised study. Int J Oral Maxillofac Surg. 2000; 29:268-271
Gomes AC, Vasconcelos BC, de Oliveira e Silva ED, da Silva LC. Lingual nerve damage after mandibular third molar surgery: a randomized clinical trial. J Oral Maxillofac Surg. 2005; 63:1443-1446
Smith AC, Barry S, Chiong A. Inferior alveolar nerve damage following removal of mandibular third molar teeth. A prospective study using panoramic radiography. Aust Dent J. 1997; 42:149-152
Rood JP, Nooraldeen Shehab BAA. The radiological prediction of inferior alveolar nerve injury during third molar surgery. Br J Oral Maxillofac Surg. 1990; 28:20-25
Renton T, Hankins M, Sproate C, McGurk M. A randomised controlled clinical trial to compare the incidence of injury to the inferior alveolar nerve as a result of coronectomy and removal of mandibular third molars. Br J Oral Maxillofac Surg. 2005; 43:7-12
Dawood A, Patel S, Brown J. Cone beam CT in dental practice. Br Dent J. 2009; 207:23-28
Soares M, Batista W, Antonio P, Caldas L, Maia A. Study of effective dose of various protocols in equipment cone beam CT. Appl Radiat Isotopes. 2015; 100:21-26
Al-Okshi A, Lindh C, Salé H, Gunnarsson M, Rohlin M. Effective dose of cone beam CT (CBCT) of the facial skeleton: a systematic review. Br J Radiol. 2015; 88:(1045)
Pauwels R, Ivanauskaité Cockmartin L Estimating cancer risk from dental cone-beam CT exposures based on skin dosimetry. Phys Med Biol. 2014; 59:(14)3877-3891
Ludlow JB, Davies-Ludlow LE, Brooks SL. Dosimetry of two extraoral direct digital imaging devices: NewTom cone beam CT and Orthophos Plus DS panoramic unit. Dentomaxillofac Radiol. 2003; 32:229-234
Eyrich G, Seifert B, Matthews F 3-Dimensional imaging for lower third molars: is there an implication for surgical removal?. J Oral Maxillofac Surg. 2011; 69:1867-1872
Matzen LH, Christensen J, Hintze H, Schou S, Wenzel A. Influence of cone beam CT on treatment plan before surgical intervention of mandibular third molars and impact of radiographic factors on deciding on coronectomy vs surgical removal. Dentomaxillofac Radiol. 2013; 42
Maglione M, Costantinides F, Bazzocchi G. Classification of impacted mandibular third molars on cone-beam CT Images. J Clin Exp Dent. 2015; 7:e224-231
Pogrel M, Lee J, Muff D. Coronectomy: a technique to protect the inferior alveolar nerve. J Oral Maxillofac Surg. 2004; 62:1447-1452
Martin A, Perinetti G, Costantinides F, Maglione M. Coronectomy as a surgical approach to impacted mandibular third molars: a systematic review. Head Face Med. 2015; 11
Monaco G, de Santis G, Gatto MR, Corinaldesi G, Marchetti C. Coronectomy: a surgical option for impacted third molars in close proximity to the inferioralveolar nerve. J Am Dent Assoc. 2012; 143:363-369
Goto S, Kurita K, Kuroiwa Y, Hatano Y, Kohara K, Izumi M Clinical and dental computed tomographic evaluation 1 year after coronectomy. J Oral Maxillofac Surg. 2012; 70:1023-1029
Renton T, Hankins M, Sproate C, McGurk M. A randomised controlled clinical trial to compare the incidence of injury to the inferior alveolar nerve as a result of coronectomy and removal of mandibular third molars. Br J Oral Maxillofac Surg. 2005; 43:7-12
Leung YY, Cheung LK. Safety of coronectomy versus excision of wisdom teeth: a randomized controlled trial. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 2009; 108:821-827
Hatano Y, Kurita K, Kuroiwa Y, Yuasa H, Ariji E. Clinical evaluations of coronectomy (intentional partial odontectomy) for mandibular third molars using dental computed tomography: a case–control study. J Oral Maxillofac Surg. 2009; 67:1806-1814
Dolanmaz D, Yildirim G, Isik K, Kucuk K, Ozturk A. A preferable technique for protecting the inferior alveolar nerve: coronectomy. J Oral Maxillofac Surg. 2009; 67:1234-1238
Goto S, Kurita K, Kuroiwa Y, Hatano Y, Kohara K, Izumi M Clinical and dental computed tomographic evaluation 1 year after coronectomy. J Oral Maxillofac Surg. 2012; 70:1023-1029
Coulthard P, Kushnerev E, Yates JM, Walsh T, Patel N, Bailey E, Renton TF. Interventions for iatrogenic inferior alveolar and lingual nerve injury. Cochrane Database Syst Rev. 2014; (4) https://doi.org/10.1002/14651858.CD005293.pub2
NICE guidance for mandibular third molars has been available since 2000. This was set up to limit the surgical treatment of these teeth to symptomatic patients. There are numerous risks involved with surgical treatment of mandibular third molars and these should be explained in detail to the patient. Common and serious complications of mandibular third molar surgery are damage to the inferior alveolar and lingual nerve. Predicting the risk of inferior alveolar nerve injury is useful for treatment planning. The orthopantomogram (OPT) is the baseline special test for assessing this and numerous signs on an OPT can predict an increased risk of injury to the nerve. Cone beam computed tomography (CBCT) is being more frequently used to assess this relationship further and can influence treatment planning. Coronectomy is a technique whereby the crown of the tooth is sectioned and removed leaving the roots in situ. This has proven to be a useful technique in high risk cases, but is not without its own complications. The increase in availability of CBCT imaging and the recent resurgence of coronectomy as a treatment modality can increase the number of treatment options available to patients. We have proposed an algorithm to aid the treatment planning and informed consent processes associated with mandibular third molar surgery.
CPD/Clinical Relevance: This article is relevant to primary and secondary care dental practitioners as it will aid the investigation, treatment planning, correct referral and management of patients with problematic mandibular third molars.
Article
Current guidance
In March 2000 the National Institute for Health and Care Excellence (NICE) issued guidance on the extraction of wisdom teeth. This guidance stressed the discontinuation of prophylactic surgical removal of pathology free impacted third molars in the NHS and illustrated indications for removal. Simultaneous guidance from the Scottish Intercollegiate Guidelines Network (SIGN) from 2000 was withdrawn to be revised in February 2015, owing to a need for a review of the evidence as the document is over 10 years old.
The NICE guidance suggests limiting third molar surgery to patients with pathology, including unrestorable caries, untreatable pulpal or periapical pathology, cellulitis, abscess and osteomyelitis, resorption of the tooth or adjacent teeth, diseases of the follicle including cysts or tumours, teeth impeding surgery, teeth in the field of tumour resection. Severe or multiple episodes of pericoronitis indicate surgery.1
The SIGN guidance included some indications for prophylactic removal such as pre-radiotherapy or cardiac surgery, where the risk of retaining the wisdom tooth would outweigh the risks of removal. Other examples of indications for removal without symptoms as outlined by SIGN are periodontal disease associated with the second molar due to the position of the third molar and in those patients who have an occupation or lifestyle which inhibits access to regular dental care. The SIGN guidance also explicitly included caries in second molars judged to be caused by the impacted third molar, which could not be restored without removal of the third molar. The NICE guidance does include unrestorable caries in third molars, however it does not include removal of third molars in order to render second molars restorable.2 Since the implementation of the NICE guidance, the incidence of distal mandibular second molar caries has risen from 5% to 19%.3
The contrast between guidance from both British organizations illustrates the controversy surrounding the topic. Considering the amount of research that has been carried out since publication of the two documents, revision is indicated.
American attitudes were traditionally less conservative but are now veering away from a prophylactic approach. A recent American Dental Association (ADA) paper categorized third molars into four groups. The ADA guidance is less explicit. They advise careful diagnosis of the cause of symptoms and a tailored treatment plan for each patient as opposed to prophylactic removal at a young age which was their previous consensus.4
National guidance is a useful tool when used as part of the treatment planning process. However, each patient and case is different and, although it is important to consider the best evidence available, it is equally (if not more important) to discuss the options thoroughly with patients so that they can come to an informed decision, having weighed up the risks and benefits, in order to decide on the best option for them. This is of particular importance since the law on informed consent has changed following the Supreme Court judgment in relation to the Montgomery versus Lancashire health board case. It was judged that clinicians must divulge any material risk involved in a treatment plan and discuss reasonable alternatives.5
Risks of treatment
If the patient presents with mandibular third molars which fit the criteria for removal within the current guidance, any treatment decision must be made as part of a discussion with the patient following a thorough history and examination. Difficulty of the procedure can be predicted from several radiographic features, including position and angulation of the tooth and complexity of the roots. Once the difficulty of the surgical removal has been judged, this can aid decision-making with regards to adjunctive sedation or general anaesthetic and selecting a surgeon with a skill level appropriate to the task, ie whether the tooth should be removed in primary or secondary care and by whom.
Risks of surgical removal of lower third molars are post-operative pain, swelling, trismus, infection, dry socket, inferior alveolar nerve damage (causing temporary or permanent altered sensation to the lip, chin and teeth on that side), lingual nerve damage (causing temporary or permanent altered sensation to the anterior and altered taste sensation to the ipsilateral anterior two thirds of the tongue) and fracture of the mandible. Pain, swelling and trismus are all very common.
Dry socket
Incidence of dry socket varies greatly between studies. A 2014 systematic review shows a median incidence of 2.9% when using a triangular flap or 10% with an envelope flap.6Treponema denticola and other spirochetes are sometimes implicated in the condition and have been shown to produce fibrinolytic enzymes which break down the all-important blood clot.7 Many risk factors are involved, such as female gender, expertise of the surgeon and difficulty of extraction.8 Surgical removal presents a risk of nine times greater than normal forceps extraction.8 Smoking is thought to be a significant risk factor: one study demonstrated that smoking following surgery tripled the risk of developing dry socket. A recent randomized controlled trial gave an overall incidence of 4% in lower third molar surgery. In this study an incidence of 10% was observed in the control group, this was reduced to 2% when chlorhexidine gel was applied to the socket and no cases with postoperative application of non-resorbable eugenol based paste, Alvogyl®.9 However, it must be kept in mind that Alvogyl® has now ceased production and Alvogyl® has replaced this. This has a different composition and the results may not be applicable. Other techniques for prevention include plasma rich in growth factors and low level laser therapy, which are showing promising results but, due to the complexity and equipment needed, are unlikely to prove common, especially in the primary care setting.10
Post-operative infection
Surgical site infection is diagnosed by the presence of suppuration, lymphadenopathy or systemic signs of infection. A recent Cochrane review has quoted the incidence as 10% in young healthy patients rising to 25% in the immunocompromised. Even so, the review concluded that the risks of adverse events and antimicrobial resistance outweigh the benefit of prescribing antimicrobial prophylaxis11 Coulthard et al quote lower incidences of post-operative infection at 3-4.7% and these figures are closer to the authors' experience.6
Mandibular fracture
A rare but serious complication is fracture of the mandible (0.0049%), many of which occur 2–3 weeks post-operatively during mastication.12
Nerve injuries
The most important complication is damage to the inferior alveolar nerve or the lingual nerve, causing temporary or permanent altered sensation to the regions these sensory nerves supply. Altered sensation lasting longer than 6 months is usually categorized as permanent.13 Altered sensation could be loss of sensation, tingling, abnormal sensation or painful sensation. Incidence of temporary altered sensation to the lingual nerve is 0–15%,14,15 permanent being 0–2%.16,17 However, these figures included cases where the lingual split technique was used more commonly and this may not be representative of current techniques. In the past it was common practice to protect the lingual nerve with a retractor or other instrument. Lingual retraction has been shown to increase the risk of temporary damage to the lingual nerve (likely due to blunt trauma to the nerve when reflecting and retracting the lingual flap) but reduce the risk of permanent lingual nerve damage by protecting the lingual soft tissues from the drill whilst decoronating the tooth.18,19
The risk of temporarily damaging the inferior alveolar nerve is reported in 5% of cases.20 Permanent damage is reported in 0.2% of cases. Both of these figures are based on a prospective study by Smith in 1997 and were included in the recent Cochrane review by Coulthard et al.6 These incidences markedly increase when the third molar is positioned in close proximity to the inferior alveolar nerve and this can be judged pre-operatively using radiographic techniques. These complications are arranged along with incidences in Table 1.
Orthopantomographic tomography is routinely used to aid decision-making in third molar surgery. The radiographic warning signs for high risk of ID damage are:
Interruption of the white line, darkening of the root;
A recent study found an incidence of 19% of ID nerve damage in patients with these radiographic signs in total and 2% permanent. Juxta-apical area was also found to cause a clinically significant increase in risk of ID nerve damage (Figure 1).22
Figure 1. Radiographic warning signs on OPT. (a) Interruption of the white lines. (b) Darkening of the root. (c) Deflected root. (d) Diversion of the inferior alveolar canal. (e) Narrowing of the root. (f) Juxta-apical area.
If these radiographic signs are evident on an OPT, further imaging with cone beam computed tomography (CBCT) may be warranted.
CBCT is a relatively new technology which uses a cone-shaped beam and flat panel detector which together rotate about an axis in the centre of the area to be imaged, capturing slices as it goes. The computer software then converts this information into a 3 dimensional image which can then be viewed in several anatomical plains like conventional CT. The machine is akin to an OPT machine in its size and form. They are therefore available to use in a primary care setting, unlike conventional CT.23
Weighing up the risk of CBCT with the benefits of aiding treatment planning is important. Effective dose of CBCT has been measured at between 9.3–51.2 μSv for small fields of view used in dental imaging. Effective dose for full arch views ranges from 17.6–52.0 μSv. The range is due to the many different machines and also the different tissues exposed to the beam as the tissue weighting factor is used to calculate effective dose. The weighting factors were laid out by the ICRP in 2007. Larger doses have been quoted but this is due to not optimizing the machine to keep exposure as low as reasonably attainable (ALARA).24,25 This translates to an average risk of developing neoplasia at 2.7 to 9.8 per million, depending on age (younger patients having an increased risk due to higher life expectancy).26 This can be explained to the patient by relating the dose to other dental views such as OPT which, with doses up to 22 μSv, are comparable to CBCT.27
Radiographic signs on cone beam CT have been researched clinically. Significant signs are as follows:
Narrowing of the canal;
Direct contact between the nerve and root;
Fully formed roots;
A lingual course of the nerve with or without perforation of the cortical plate or an
Intra-root position of the nerve.
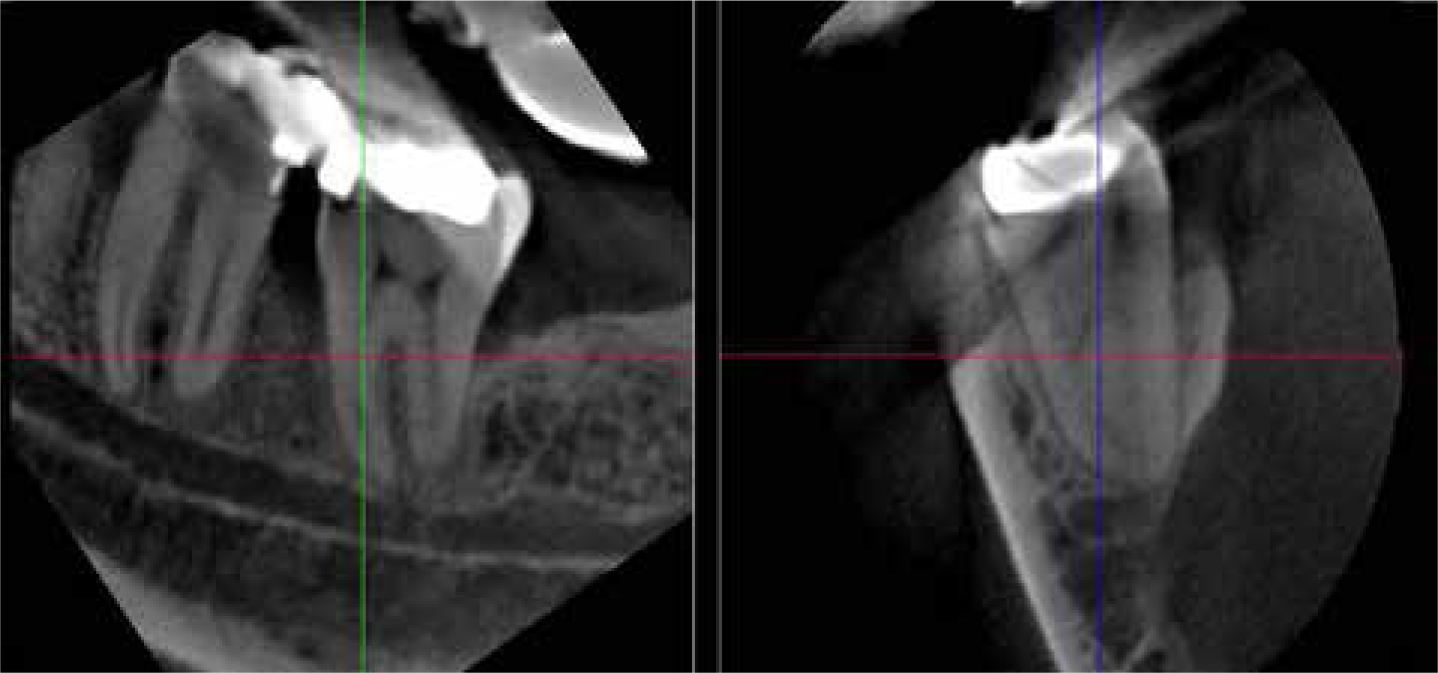
Direct contact and narrowing of the canal are the strongest indicators.28 This helps the surgeon to interpret the exact course of the nerve. Treatment plans can be influenced by findings on CBCT by either helping to plan technique for complete removal or to decide to carry out coronectomy. One study found 12% of treatment plans were changed following a CBCT between surgical removal and coronectomy. An additional factor influencing this decision was grooving or notching of the root by the nerve.29 A classification system has been proposed which could be useful for communication and treatment planning and in further research. This categorizes the positions into seven classifications, depending on the relative positions of the tooth and nerve.30 Two examples of how CBCT images compare with OPG are shown in Figure 2.
Figure 2. CBCT of mandibular third molar roots identified as high risk on DPT but they appear to be distant, inferior and buccal to IDC allowing for removal.
Coronectomy
Once the investigations have been assessed the surgeon can then advise the patient of the risks and benefits between surgical removal and coronectomy. Described by Pogrel et al, it is the technique of removing the crown of the tooth by raising a full thickness mucoperiostial flap, retracting the lingual soft tissues so as to protect the lingual nerve and completely sectioning the crown at 450 to attempt to avoid mobilizing the roots.31 The coronal portion is then reduced with burrs until the roots lie 3 mm below the alveolar bone and no enamel remains, leaving them in place so as to reduce the risk to the ID nerve.31 No pulp treatment should be performed on the retained roots as this increases risk of post-operative infection. Coronectomy is not indicated for teeth with caries involving the pulp, or teeth which are mobile.
In principle this technique should reduce incidence of ID nerve damage. A systematic review in 2015 investigated the comparison between coronectomy and surgical removal of the crown and roots. It was found that temporary ID nerve damage occurs in 0–9.5% of coronectomies32 compared with up to 19% for surgical removal. These figures do not account for failure of coronectomy which is due to either post-operative infection or mobilization of the roots during surgery. Mobilizing the roots is thought to devitalize them, resulting in a foreign body response, increasing the risk of post-operative pain and infection. In some studies analysed in the systematic review previously cited,32 the risk of failed coronectomy was 0%.31,33,34 In a separate study the rate was as high as 38%, 8% of which had temporary ID nerve damage. Women with conical roots were found to be at greatest risk.35 This stark difference could be due to differing technique. Lingual flaps and retraction are discouraged by some recent literature, contrary to Pogrel's surgical protocol due to the previously mentioned risk of transient lingual nerve damage caused by lingual retraction. 33,36 This therefore inhibits the complete sectioning of the crown with a bur, necessitating at least some small force to be placed on the roots during sectioning with a hand instrument. Monaco et al recommend sectioning mesio-distally as well as bucco-lingually so as to leave only one corner of crown to break when separating with a hand instrument.33 The reported rates of lingual nerve damage for coronectomy are 0–2%. None of these cases was permanent.32
Once the crown is sectioned from the roots they are essentially disimpacted, which gives rise to another complication of coronectomy: migration of the roots. Some would argue that this is not a complication as the roots are moving away from the ID nerve and towards the surface, but this can cause irritation and this situation often demands surgical removal. Root migration occurs in up to 85.3% of cases37 and this migration can be up to 4 mm after 24 months.38 This can translate to a re-operation rate of 6.9% but this can be due to infection as well as root exposure following migration.39 There was no significant difference in risk of post-operative pain and dry socket between coronectomy and surgical removal in a systematic review carried out.32
Overall coronectomy is a good treatment option to reduce the incidence of ID nerve injury in high risk cases. Root migration and re-operation are risks of the procedure but, as the roots could have migrated into a safer position, the risk of ID nerve injury is still reduced in these cases (Table 2).
Other methods have been reported in relation to the high risk third molar, including orthodontic disimpaction and sagittal split osteotomy to mobilize and relocate the nerve. Although these methods are worthy of mention, and have indeed shown excellent results, they are beyond the scope of this article.
The damaged nerve
If the patient suffers a nerve injury and has permanent altered sensation, there are a number of surgical, medical and psychological treatments which are performed. None of these has strong supporting evidence. Surgical management may involve removing scar tissue, opposing the transected nerve ends, nerve grafts, nerve decompression or low level laser therapy. Low level laser therapy has some weak evidence supporting it, but the other treatments have not been studied extensively according to a Cochrane review.40
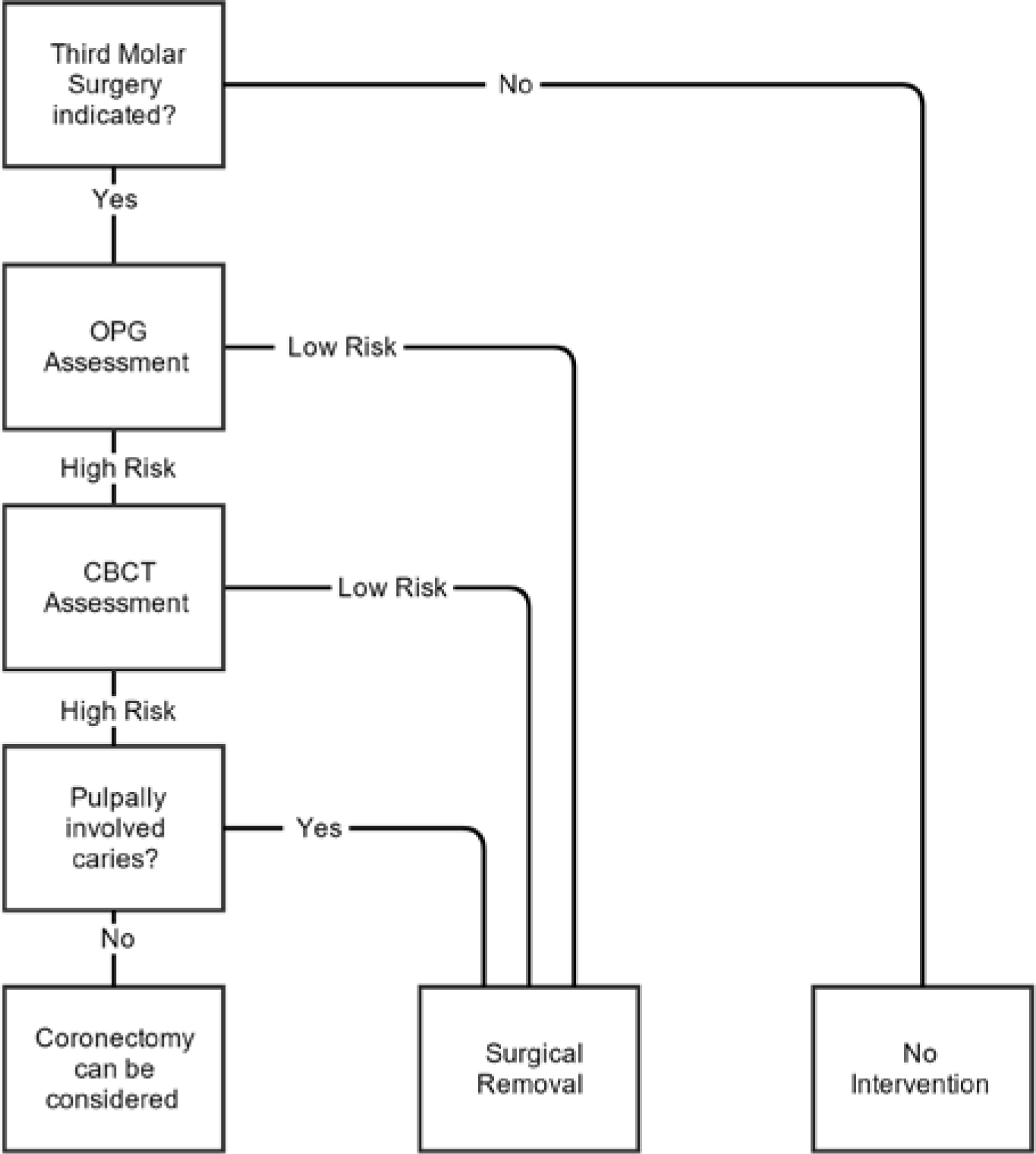
All this should be in mind when treatment planning and gaining consent for treatment for problematic mandibular third molars. Figure 3 provides a handy algorithm to help with the flow of the initial consultation.
Figure 3. Algorithm to aid the treatment planning process.