Ghafari J. Problems associated with ceramic brackets suggest limiting use to selected teeth. Angle Orthod. 1992; 62:145-152
Wiechmann D, Rummel V, Thalheim A, Simon JS, Wiechmann L. Customized brackets and archwires for lingual orthodontic treatment. Am J Orthod Dentofacial Orthop. 2003; 124:593-599
Grauer D, Proffit WR. Accuracy in tooth positioning with a fully customized lingual orthodontic appliance. Am J Orthod Dentofacial Orthop. 2011; 140:433-443
Barthelemi S, Hyppolite MP, Palot C, Wiechmann D. Components of overbite reduction in lingual orthodontics: molar extrusion or incisor intrusion?. Int Orthod. 2014; 12:395-412
Hohoff A, Seifert E, Fillion D, Stamm T, Heinecke A, Ehmer U. Speech performance in lingual orthodontic patients measured by sonography and auditive analysis. Am J Orthod Dentofacial Orthop. 2003; 123:146-152
Miyawaki S, Yasuhara M, Koh Y. Discomfort caused by bonded lingual orthodontic appliances in adult patients as examined by retrospective questionnaire. Am J Orthod Dentofacial Orthop. 1999; 115:83-88
Stamm T, Hohoff A, Ehmer U. A subjective comparison of two lingual bracket systems. Eur J Orthod. 2005; 27:420-426
McMullin A, Waring D, Malik O. Invisible orthodontics part 2: lingual appliance treatment. Dent Update. 2013; 40:391-402
Lew KK. Attitudes and perceptions of adults towards orthodontic treatment in an Asian community. Community Dent Oral Epidemiol. 1993; 21:31-35
Reitan K. Tissue reaction as related to the age factor. Dental Record. 1954; 74:271-279
Dyer GS, Harris EF, Vaden JL. Age effects on orthodontic treatment: adolescents contrasted with adults. Am J Orthod Dentofacial Orthop. 1991; 100:523-530
Post-CCST Orthodontist, University of Manchester Dental Hospital, Higher Cambridge Street, Manchester M15 6HF and Salford Royal NHS Foundation Trust, Stott Lane, Manchester M6 8HD and Northenden House Orthodontics, Sale Road, Manchester, M23 0DF
Consultant in Orthodontics, University of Manchester Dental Hospital, Higher Cambridge Street, Manchester, M15 6FH, Salford Royal NHS Foundation Trust, Stott Lane, Manchester and Northenden House Orthodontics, Sale Road, Manchester, M23 0DF
The aim of this article is to explore the use of Incognito™ Lite as an alternative to competitors advertising a ‘Smile in Six Months’ or rather short-term orthodontics for improving dental appearance through tooth movement. The focus is on the varied clinical use of this appliance system and its comparative advantages, disadvantages and placement techniques. Some alternatives are discussed and appraised. Two cases successfully treated with Incognito™ Lite are then presented.
CPD/Clinical Relevance: A reliable and predictable tool for aesthetic alignment of teeth, creating a broader range of treatment options for both the clinician and the patient.
Article
Patients often request straight teeth in the shortest possible time using appliances that are invisible1 and comfortable. Dentists continue to search for the ultimate appliance that combines aesthetics and patient comfort with the ability to deliver optimal treatment outcomes consistently and efficiently. A number of appliance systems are in existence today that satisfy some, but not all, of the aforementioned criteria. Indeed, no appliance system is truly ‘invisible’ and until recently there has been a trade-off between aesthetics, treatment time and precision of tooth movement. Predictability of the result is also dependent on the operators' working knowledge of the appliance system and their clinical ability to get the most from it.
This article will present Incognito™ Lite as a predictable alternative to other short-term orthodontic treatment modalities, often referred to as a ‘Smile in Six Months’.
Incognito™ and Incognito™ Lite
Incognito™ is a lingual appliance system developed by Wiechmann using CAD/CAM technology.2 It has all the advantages of traditional lingual appliance systems, such as optimal aesthetics, three-dimensional tooth control, constant force application and an indirect bonding technique. Additionally, there are many unique advantages relating to this appliance system, which include the precise fit of custom-made, low-profile, cast gold alloy brackets and an accompanying customized series of Nickel Titanium and Beta III Titanium archwires, resulting in a predictable treatment outcome.3 The finishing process is simplified as accurate rebonding is possible and the preformed archwires reduce the need for additional wirebending.
Incognito™ Lite is a scaled back version of the Incognito™ system, designed to incorporate the ‘social six’ or canine to canine with an optional fourth bracket for the first premolar if further anchorage is needed, depending on the initial treatment aims. The number of teeth included on the appliance sets this apart from other appliance systems. Treatment aims are therefore somewhat limited but simple, predictable and rapid alignment of the upper labial segment is afforded within an average treatment time of six to nine months.4 Where optimal aesthetics are critical, lingual appliances are the most appropriate option for the treatment of orthodontic relapse or where minor labial segment tooth movements are necessary.4 By virtue of the customized bonding position on the lingual tooth surface, bracket profile and good bond strength, the lingual lite appliance may also help to reduce an increased overbite. Indeed, Barthelemi et al have demonstrated that this system is very efficient at overbite reduction, achieved principally by mandibular incisor intrusion.5 Further advantages include the indirect bonding technique which, when coupled with bracket placement in the anterior region of the oral cavity, facilitates ease of bracket placement and results in less accidental debonding. The vertical path of insertion and the self-retaining slot simplifies archwire placement. Together, the high precision bracket slots and customized archwires permit efficient torque expression to achieve precise tooth movement.
Patients might also be expected to adapt to the shortened appliance faster than with a full lingual appliance,4 perhaps due to increased tongue space. However, the disadvantages of a lingual lite appliance occur in part as a consequence of the restriction of the appliance to the anterior segment. As such, the buccal segments are not corrected and less arch expansion is achieved. This may restrict its use to dentitions that have good buccal occlusion. Patients wearing lingual appliances also tend to report speech alterations and tongue soreness in addition to problems associated with conventional fixed appliances, such as difficulty in maintaining oral hygiene and food adherence between appliance components. Studies have demonstrated that lingual appliances can have a negative effect on speech, according to both patients and speech professionals, although these are mostly short-lived and tend to resolve spontaneously by debond.6,7 Fortunately, custom-made lingual appliances have lower bracket profiles, which have been shown to reduce speech and functional problems.8 However, custom-made appliances are more laborious to construct and some contain precious metal alloys that makes them significantly more expensive than pre-formed systems. Another disadvantage common to all lingual appliance systems is limited direct visualization of the lingual aspects of teeth.9
Case selection is therefore of paramount importance. The demand for aesthetic appliances predominantly comes from adult patients who often have high expectations10 that require careful consideration from the outset. Adults are also more likely to present with a heavily restored dentition and/or a compromised periodontium. Initial tooth movement is often slower, perhaps due to reduced cellular activity,11 but the overall treatment timing can be comparable to younger patients due to better motivation, compliance and reduced breakages.12 As with conventional appliance treatment, such difficulties must be stabilized prior to and managed throughout orthodontic treatment. Permanent retention is often indicated as an adjunct to removable retainers in the dentally fit patient.
Construction of the appliance
The process of constructing the custom-made appliance involves sending a polyvinylsiloxane impression, wax bite and prescription to the 3M TOP-Service laboratory in Bad Essen, Germany, to allow accurate reproduction of the dentition. A wax set-up of the anticipated final result is fabricated according to the prescription for approval by the orthodontist prior to production of a high-resolution 3D digital model using a 3D scanner. Bracket components such as tie-wings and hooks are adjusted on customized bases for optimal positioning and are subsequently printed using Stereolithography equipment and cast. The customized archwires (0.014” SE NiTi, 0.016” x 0.022” SE NiTi and 0.0182” x 0.0182” Beta III Titanium) including any bends needed to obtain the desired final result are manufactured using a robot. Laboratory technicians set up the brackets in ideal positions on the stone model of the original malocclusion and make an indirect bonding tray to facilitate simple and accurate bracket placement.4,13 As the set-up is technically challenging, there has been a recent move towards a ‘digital set-up’ for enhanced precision. The teeth are digitized and assigned three-dimensional co-ordinates that give the technician complete control over final tooth positions within and between the arches. 2D screenshot documentation is provided with the lingual lite appliance, which shows the original malocclusion alongside the set-up which can be used for patient education in addition to their medicolegal record.
It is important to explain the bond-up procedure to the patient and isolate the teeth well. The bonding process depends on the type of surface to which the bracket is bonded. If indirectly bonding onto enamel using the clear precision tray, the tooth tissue should first be cleaned with pumice or micro-etched with 50 µm aluminium oxide, then etched for 30 seconds with 35% phosphoric acid, rinsed thoroughly and dried. A thin layer of bonding agent is applied to the bracket bases in the transfer tray. No metal primer is necessary if using RelyX™ Unicem 2 Automix (a dual cure self-adhesive resin cement), as recommended by the manufacturers. The tray is immediately seated and held firmly in situ for the curing time specified by the manufacturer during which the brackets are light-cured on all four sides. The retractor is removed then the tray is firmly peeled away, bracket positions are checked, excess adhesive is scaled from the bracket peripheries and floss is passed interdentally. If detected, posterior premature contacts must be eliminated.
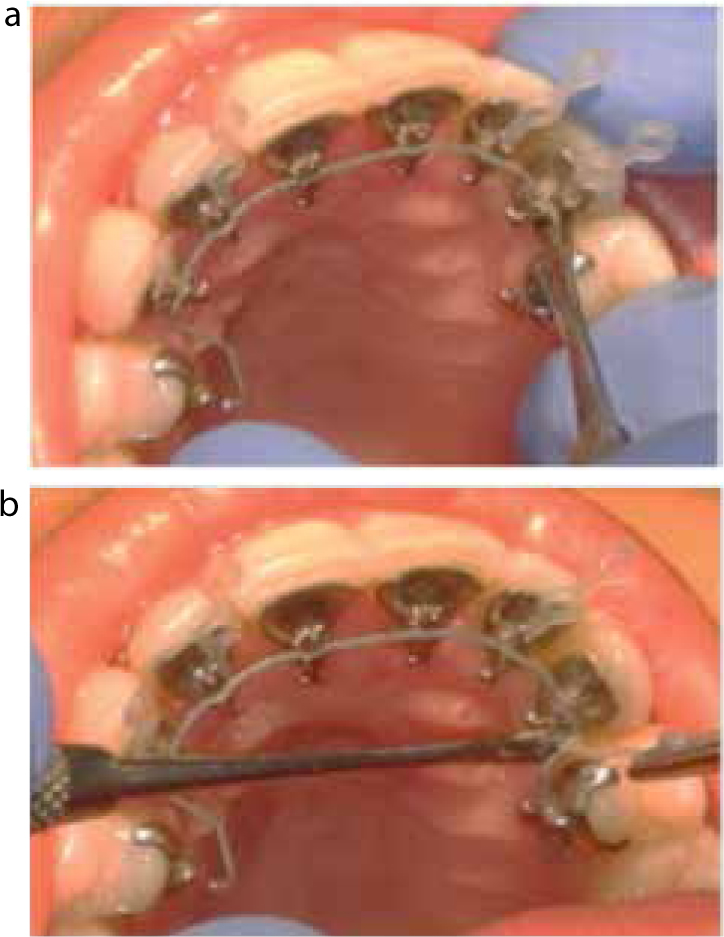
Archwire placement is relatively straightforward. The edge of the terminal bracket is marked on the archwire, which is trimmed extra-orally using the template for guidance. The final trim is completed intra-orally with the archwire fully seated. The wires are turned in distal to the bracket slot and tied in the wires using elastomeric modules, wire ligatures or reverse double overties (Figure 1).
Figure 1.
(a, b) Incognito™ Lite lingual brackets with reverse double overties. The end of four links of powerchain is placed over the bracket slot, under the archwire, using forceps. The powerchain is stretched and the second link is passed back over the bracket slot, securing it in place. The terminal two links are removed and discarded.
Alternatives to Incognito™ Lite
A multitude of removable and fixed appliance systems advertise a ‘Smile in Six Months’. They aim to treat minor orthodontic problems but often achieve little more than simple dental alignment. This is acceptable as the sole aim of treatment to a particular cohort of patients, who are often willing to forgo the gold standard Class I occlusion so long as a rapid, self-perceived improvement is achieved using aesthetic techniques. Removable appliance systems currently on the market as an alternative to short-term lingual appliances include Invisalign® Lite and Inman Aligners™. Fastbraces® and Six Month Smiles are labially bonded fixed appliance systems that also advertise reduced treatment times.
Invisalign Lite
Invisalign® was originally marketed as a clear, removable alternative to conventional braces14 for treating a variety of orthodontic problems such as crowded and spaced teeth, increased overbites, reverse overjets and crossbites. The original system consisted of a series of custom-made aligners, each worn for a period of 2 weeks for 20–22 hours per day, for up to 18 months, depending on the complexity of the case. More recently, Invisalign ‘Lite’15 (Figure 2) has been described as a faster alternative to Invisalign®, with treatment time around six months with a series of up to ten aligners using the same technology. The advantages are good aesthetics, short treatment times (due to the main indication for orthodontic retreatment following relapse, or mild malocclusions) and the consequential reduction in cost. The main disadvantage of this system is the limited indication for its use; only mild crowding and spacing is treatable using this system.
Figure 2. Upper and lower Invisalign® Lite aligners.
Inman Aligner™
The Inman Aligner™ system (Figure 3) relieves crowding and aligns the teeth using a single appliance with Nickel Titanium coil-springs and two acrylated wire bows that sit labial and palatal or lingual to the anterior teeth.16 The appliance is worn 16–20 hours per day. The patient attends regular two-to three-weekly appointments for review and adjustment of the appliance. Whilst this system offers rapid alignment of the incisors, the buccal segments remain unchanged and the burden of care is comparatively high. Common shortcomings of removable appliances are that they are not completely invisible from the labial aspect and full bodily control is unobtainable. Removable appliances serve to tip teeth into their final positions.17 Even with the introduction of attachments to be used alongside certain aligner systems, minor rotations are possible but full bodily control of the teeth is not.
Figure 3.
(a–e) Upper and lower Inman Aligners™.
Fastbraces
Fastbraces® Technologies advertise their labially bracket systems as comfortable, fast and affordable. They state typical treatment times of between three months and a year, but suggest treatment can be completed within weeks ‘if the alveolar bone responds well’.18 This is attributed to the triangular bracket design (Figure 4), coupled with the use of a single square, superelastic, nickel-titanium archwire which, they suggest, permits root movement from the outset, thereby reducing treatment time. This appliance system also claims to result in less root resorption and less sensitivity when compared to ‘other orthodontic brackets’ in the two studies quoted. However, the level of evidence upon which these claims are based is low. In reality there is a lack of good quality, independent research to confirm or refute these claims. The triangular bracket has a rectangular slot and so, in the authors' opinion, there does not seem to be a genuine advantage over conventional labial bracket designs. The slots are narrow in the mesio-distal dimension, resulting in an increased interbracket span, a consequential increase in archwire flexibility and reduction in friction, but at an anticipated cost of less precise control over individual tooth movements. The authors do not have any first-hand experience of this bracket system but a fundamental knowledge of biomechanics indicates that comprehensive treatment, or indeed anything more than very simple alignment, in a matter of weeks is unattainable.
Figure 4. A Fastbrace bracket.
Six Month Smiles®
Six Month Smiles® is a labially bonded fixed appliance system using Lucid-Lok® clear composite brackets and tooth-coloured archwires, which are capable of simple dental alignment and resolution of mild crowding or spacing within a 4–9 month period.19 Appliance adjustments are necessary every 4 weeks. The aims of treatment are limited but, by virtue of the labial bracket position, aesthetics are inferior in comparison. It is widely recognized by the orthodontic community that composite brackets are more prone to creep and distortion than metal brackets and hence exhibit inferior torque expression. A simulated intra-oral investigation concluded that polycarbonate brackets were responsible for higher torque losses and lower torque moments when compared to metal brackets.20 Over time, modifications have been made to improve the functional characteristics of composite brackets, albeit with limited success. One notable study compared the torque deformation of seven composite brackets with stainless steel brackets. Plastic brackets reinforced with metal slots suffered the least deformation under the application of torque. Pure polyurethane and pure polycarbonate exhibited less than when modified with ceramic or fibreglass.21
Tooth-coloured or coated archwires are also aesthetic in the short term but the coating tends to pick up extrinsic stains and abrade over time, which makes the archwire become more conspicuous. It is important to recognize that severe malocclusions cannot be treated comprehensively or safely within six months, irrespective of the appliance system used.
This adult female presented at the age of 27 years with concerns regarding the misalignment of her teeth. She was reluctant to wear conventional labial fixed appliances owing to their poor aesthetics and requested a short treatment time. The patient had previously undergone a course of orthodontic treatment but had failed to adhere to the recommended retention regimen. Upon examination, she had a Class I incisor relationship on a Class I skeletal base complicated by mild upper and lower arch crowding. The treatment aim was to achieve a well-aligned Class I incisor relationship whilst maintaining nicely interdigitating Class I buccal segments. The treatment plan involved placement of Incognito™ Lite appliances on the upper and lower anterior teeth from first premolar to first premolar. Her treatment progressed rapidly and a successful outcome was achieved when treatment was complete five months after initial placement. She was provided with upper (lateral incisor to lateral incisor) and lower (canine to canine) bonded retainers in addition to pressure-formed retainers for night-time wear.
Figure 5. Pre-treatment extra-oral frontal facial photograph of Case 1.Figure 6.
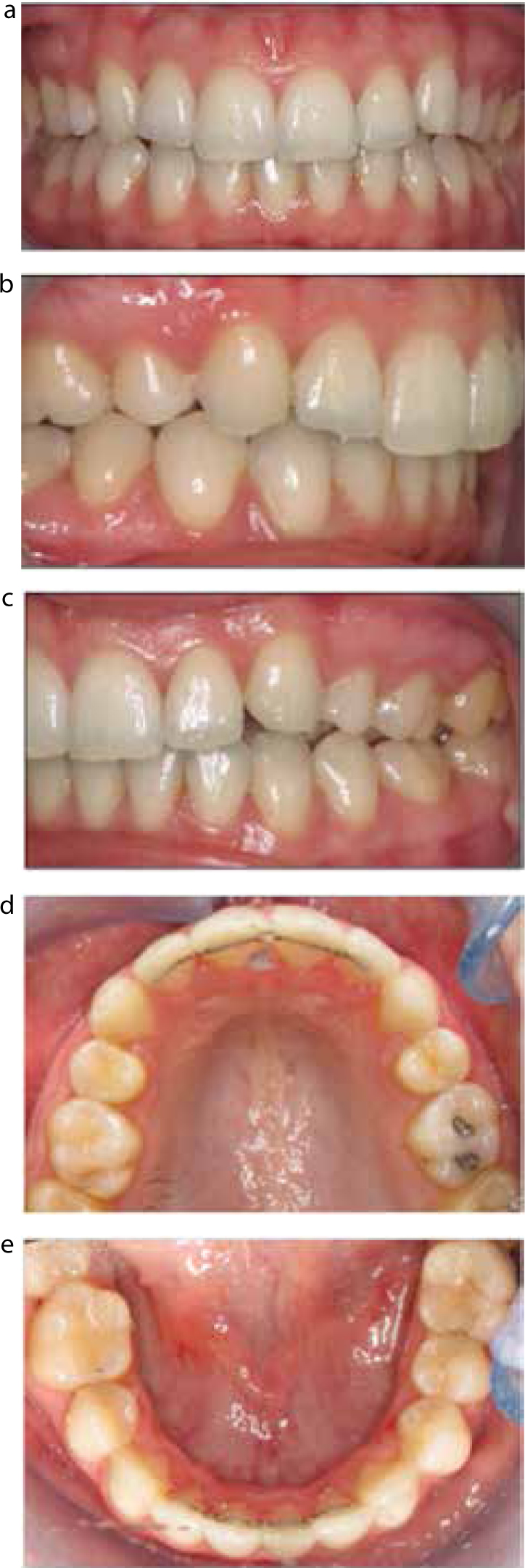
(a–e) Intra-oral photographs of Case 1 showing the Class I malocclusion with mild labial segment crowding.Figure 7.
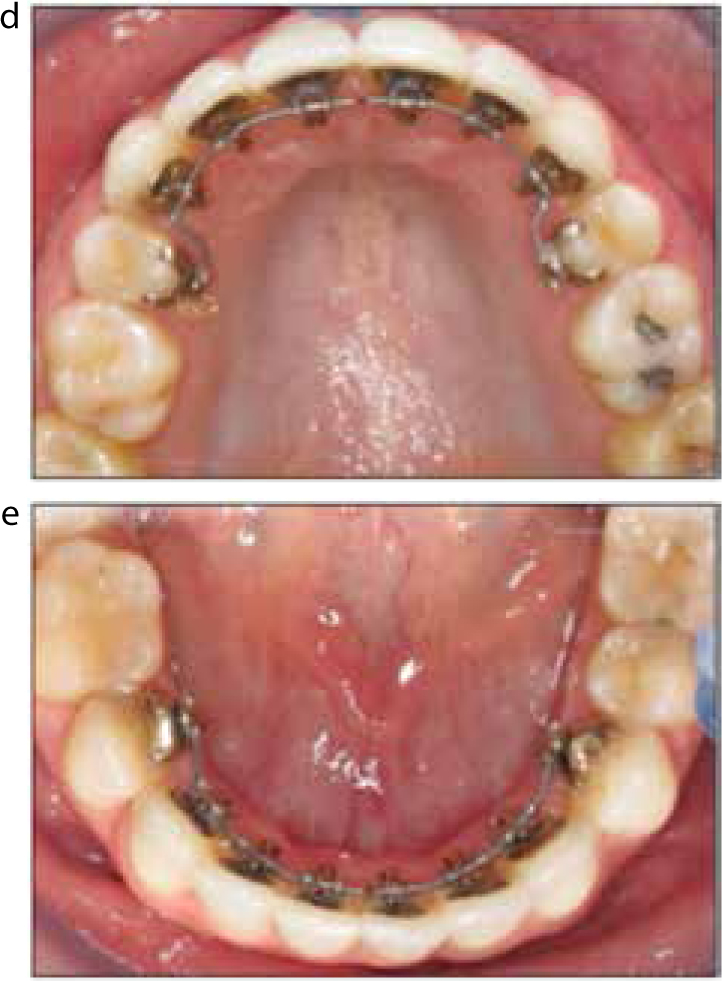
(a–e) Intra-oral photographs of Case 1 showing the finishing stage in the upper and lower arches with 0.0182” x 0.0182” Beta III Titanium.Figure 8. End of treatment extra-oral frontal facial photograph of Case 1.Figure 9.
(a–e) End of treatment intra-oral photographs of Case 1.
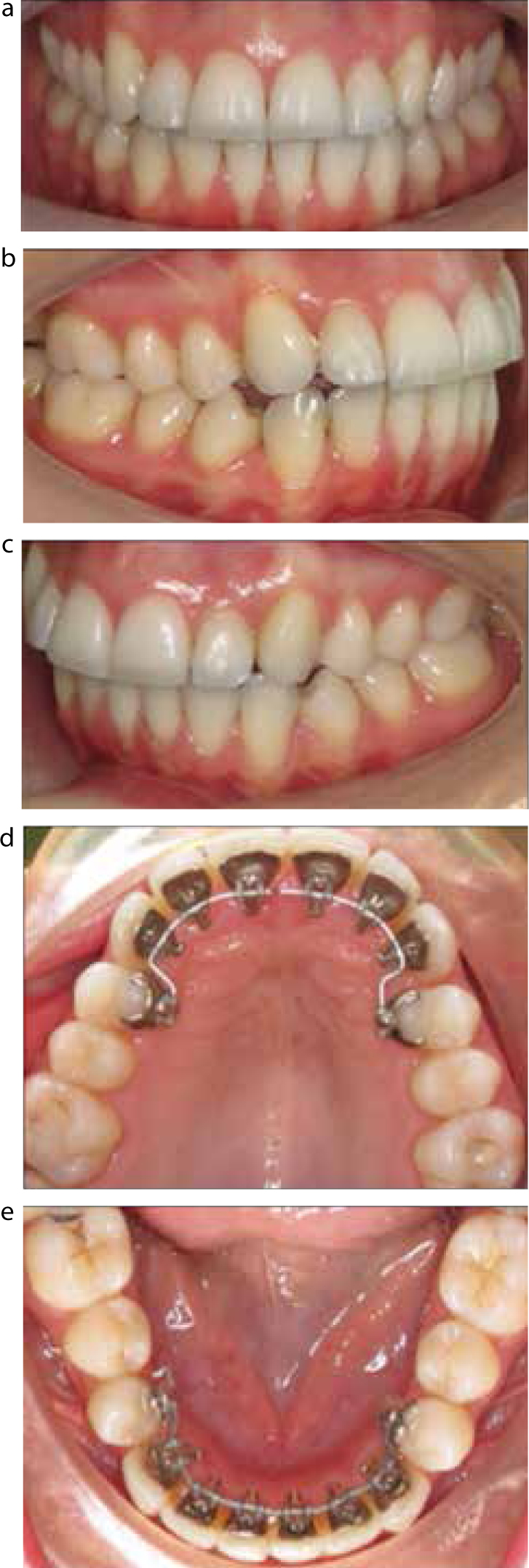
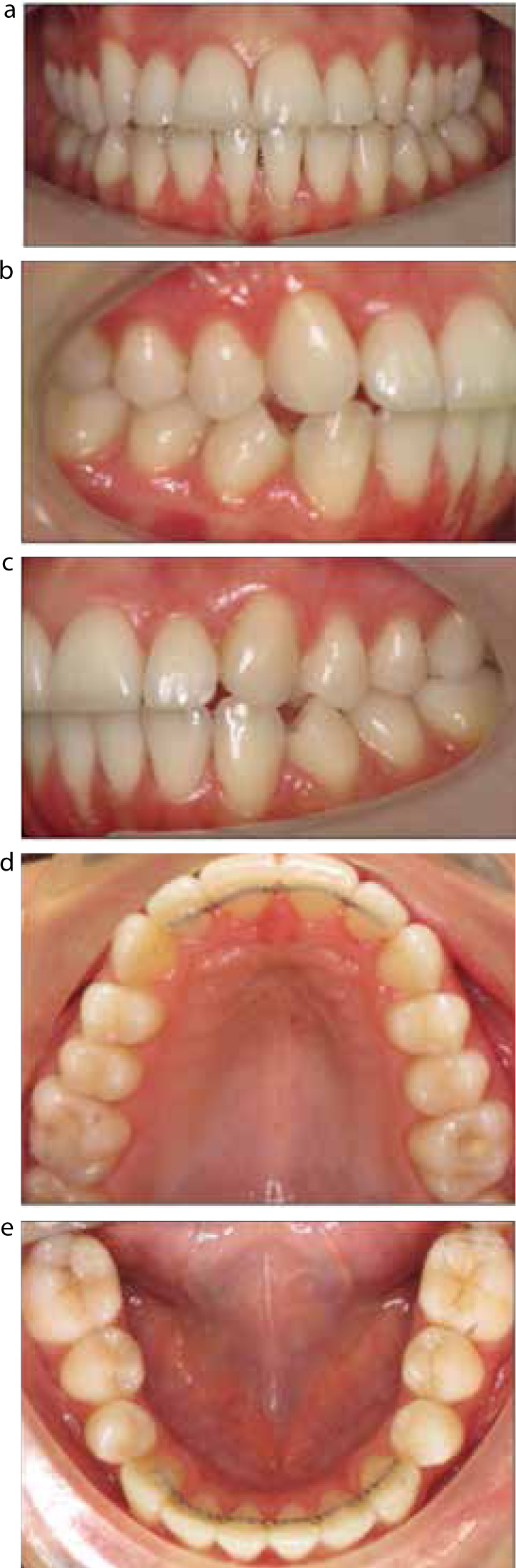
This 23-year-old female patient presented complaining about her dental crowding, which had partially returned following a previous course of orthodontic treatment. She had a Class II division 2 incisor relationship on a mild Class II skeletal base with mild upper and lower arch crowding, an increased and complete overbite and Class II buccal segments. Her upper first premolars were previously extracted as part of her original orthodontic treatment plan. As in the previous case, she was unwilling to wear conventional labial orthodontic appliances. Treatment was undertaken using Incognito™ Lite to align the labial segment and normalize the inclination of the incisors, leaving the Class II buccal segments unchanged. Again, the treatment time was short and was completed within 6 months. Upper (lateral incisor to lateral incisor) and lower (canine to canine) bonded retainers and pressure-formed retainers were provided for the patient to wear on a night-time basis.
Figure 10. Pre-treatment extra-oral frontal facial photograph of Case 2.Figure 11.
(a–e) Intra-oral photographs showing the Class II division 2 malocclusion with mild labial segment crowding and increased overbite of Case 2.Figure 12.
(a, b) Intra-oral photographs showing the aligning stage in the upper and lower arches with 0.016” x 0.022” SE NiTi archwires.Figure 13.
(a–e) End of treatment intra-oral photographs of Case 2
Conclusion
This article has presented Incognito™ Lite as a viable alternative to longer-standing methods of achieving a ‘Smile in Six Months’. Indeed, when compared to ‘invisible’ labial brackets made of ceramic or composite, the lingual lite appliance confers a significant advantage in terms of aesthetics as the entire appliance, including archwires, are hidden on the palatal or lingual aspect of anterior teeth. When the lingual appliance is compared to ‘clear’ aligner systems, the aesthetics are almost comparable but the full bodily control of the dentition provided by the fixed lingual appliance is far superior to the tipping movements afforded by removable appliances. Case selection is of paramount importance, and the lingual lite appliance is most suited to treating cases of orthodontic relapse or mild to moderate labial segment crowding.