Rushton MA. A case of dentinal dysplasia. Guy's Hosp Rep. 1939; 89:369-373
Witkop CJ Hereditary defects of dentin. Dent Clin North Am. 1975; 19:25-45
O'Carroll MK, Duncan WK. Dentin dysplasia type I. Radiologic and genetic perspectives in a six-generation family. Oral Surg Oral Med Oral Pathol. 1994; 78:375-381
Melnick M, Levin LS, Brady J. Dentin dysplasia type I: a scanning electron microscopic analysis of the primary dentition. Oral Surg Oral Med Oral Pathol. 1980; 50:335-340
Wesley RK, Wysocki GP, Mintz SM, Jackson J. Dentin dysplasia Type I. Clinical, morphologic, and genetic studies of a case. Oral Surg Oral Med Oral Pathol. 1976; 41:516-524
Wesley RK, Wysocki GP, Mintz Jackson J. Dentin dysplasia type I. Clinical, morphologic, and genetic studies of a case. Oral Surg Oral Med Oral Pathol. 1976; 41:516-524
Tidwell E, Cunningham CJ. Dentinal dysplasia: endodontic treatment, with case report. J Endodont. 1979; 5:372-376
Ravanshad S, Khayat A. Endodontic therapy on a dentition exhibiting multiple periapical radiolucencies associated with dentinal dysplasia type 1. Aust Endod J. 2006; 32:40-42
Type-1 dentine dysplasia is a rare hereditary condition, associated with an abnormality in dentine formation. Deceptively, teeth have the clinical appearance of normality, however, radiographically, a different picture is seen; with multiple periapical radiolucencies associated with non-carious, unrestored teeth. This article reports the diagnostic and management challenges associated with dentine dysplasia in adults.
CPD/Clinical Relevance: Early diagnosis and preventive advice within primary care are imperative in the long-term outcomes.
Article
Dentine dysplasia (DD) is a rare, autosomal dominant condition that manifests itself clinically with discoloured and malformed teeth that can have a significant impact on a patient's confidence and self-esteem if untreated. Despite normal formation of enamel during tooth development, there is a hereditary disturbance in the formation in dentine with subsequent alterations in pulp development. The reason for this genetic disturbance is unknown and the condition can affect both the primary and secondary dentitions.1
The clinical manifestations were initially described by Ballschmiede,2 in 1930, and in 1939 Rushton3 described the clinical presentation and introduced the term ‘dentine dysplasia’ in a clinical case report. As more cases came to light in the dental literature, Witkop4 introduced the classification for dentine dysplasia in 1972 with 2 subtypes: Type-1 and Type-2.
Key features of Type-1 dentine dysplasia (Figure 1)6,7
Prevalence 1:100,000;
Also known as ‘radicular dentinal dysplasia’ because it mainly affects the roots with the coronal aspects of the tooth being spared;
Normal appearance of the teeth with healthy enamel;
The root appearance varies from pointed-conical to complete agenesis of the roots;
Partial or complete obliteration of the pulp chamber;
Characteristic horizontal lines at the cementum-enamel junction;
Unknown prevalence – thought to be lower than Type-1;
Also known as ‘coronal dentinal dysplasia’;
Primary teeth
Clinical crowns of primary teeth have an amber or brown/opalescent blue hue;
Pulp chambers of primary teeth become completely obliterated.
Secondary teeth
Crowns are largely unaffected or may have an amber/translucent appearance;
Roots are of normal shape and contour;
Abnormal pulp chamber shapes seen;
Intra-pulpal calcifications may be present;
Partial pulp obliteration is common.
Histology
Enamel and coronal dentine appear normal;
Deeper layers show atypical tubular dentine with an amorphous and irregular organization of the dentine.
Genetics
The inheritance pattern of DD is autosomal dominant with a 50% chance of an affected parent giving birth to a child with DD. It is not uncommon, however, for ‘normal’ parents to have a first generation child with DD.
To date, the genes involved in the transmission of Type-1 DD have not been identified. Wesley et al,8 in 1976, suggested that an abnormal interaction between odontoblasts and ameloblasts resulted in a disturbance in the differentiation and function of the ectomesenchymal odontoblasts.
Psycho-social challenges
Before even beginning to think about the clinical management, careful management of the psychological effect on patients and their families is paramount. An empathetic approach offering support and help but being realistic about what is achievable is fundamental. Patients with a parent with DD could be more prepared for the diagnosis and management plan, although the psychological impact on the child should not be underestimated.
The patients should be warned about future loosening of teeth and premature loss. This is often more difficult to accept in younger patients.
Clinical challenges
The clinical features of DD can present various challenges in the clinical management of the patient (Tables 1 and 2).
Challenge
Associated Risk
Short clinical roots with unfavourable crown:root ratios
Increased risk of mobility with premature exfoliation
Thin dentine with close proximity of the pulp chamber to the tooth surface
Pulp exposure during operative dentistry
Spontaneous pulp necrosis
Multiple endodontic treatments
Pulp canal obliteration
Discoloration of teeth; technical difficulties if pulp becomes necrotic; apical periodontitis/granuloma
Challenge
Associated Risk
Amber – translucent crown
Difficult to mask with psychosocial implications
Pulp canal obliteration
Discoloration of teeth; technical difficulties if pulp becomes necrotic; apical periodontitis/granuloma
Differential diagnosis
Dentine dysplasia differs from dentinogenesis imperfecta (DI), despite both conditions sharing similarities in the mode of inheritance being autosomal dominant (Table 3).
Clinical Appearance
Radiographic Appearance
Type-1 DD
Clinically appear normalMobility of teeth
TaurodontismShort rootsPeriapical radiolucenciesPulp obliterationHorizontal line at CEJ
Type-2 DD
Discoloration and attrition affecting primary dentition onlyPermanent teeth normal appearanceNo mobility
Normal crown:root ratioThistle-shaped pulp chamberPulp obliteration
Dentinogenesis imperfecta (DI)
Amber-grey opalescent appearance and attritionAffecting both primary and permanent dentitionNo mobility
As expected, management of patients with DD is difficult, complex and a multidisciplinary approach is ideal. Treatment timing will depend on the age of the patient, severity of the condition and extent of their symptoms.
The two main dilemmas associated with Type-1 DD with spontaneous pulp necrosis and apical radiolucencies include:
Whether to attempt root canal treatment in often asymptomatic patients;
When to extract mobile teeth.
The options therefore for managing asymptomatic teeth with apical involvement depend on:
The complexity of the endodontic treatment which is linked to the degree of pulp canal obliteration;
The potential effect of no treatment which may result in progressive bone destruction and compromised bone site for future implant consideration;
The clinical and psychological impact of extractions and replacement with removable prostheses until growth is complete.
Aim of treatment
The general aims in the management of DD are standard for many patient groups:
Remove the sources of infection/pain;
Retain teeth for as long as possible;
Protect teeth from non-carious tooth surface loss;
Restore function and appearance when teeth are lost.
Important foci for treatment
Promote and reinforce oral hygiene practices throughout childhood into adulthood;
Dietary advice to prevent primary dental disease;
Educate and counsel the patient and family on expected dental outcomes and prognosis of dentition in the long term;
Provide dental interventions when necessary in the most conservative way.
Case report
A fit and healthy 22-year-old woman (GS) was referred to the Restorative Department regarding recurrent abscesses associated with her upper right central incisor (UR1). The patient had been under the care of the Paediatric Department throughout childhood owing to her developmental anomaly where prevention was the main focus of care.
Active intervention was provided on two occasions; at the age of 8 when she sustained an enamel-dentine fracture to her UR1 after falling off her bicycle. The UR1 was restored with a composite restoration; at 14 years she complained of difficulty eating due to her ‘wobbly’ lower incisor teeth so a lingual-bonded retainer was placed in an attempt to make eating more comfortable.
Her father also had Type-1 DD and was rendered edentulous at an early age and was provided with complete dentures in Nigeria.
Salient clinical features at presentation for GS (Figure 2)
Full complement of dentition with suboptimal oral hygiene associated with the patient's fears of teeth falling out if brushed too hard;
Periodontal pockets of 6 mm associated with UL6 and UL7;
Lingual-bonded retainer present LL3–LR3;
Generalized gingival recession 1–3 mm;
Grade I mobility LR4–LR6;
Only 13 teeth responded positively to sensibility testing (UR8, UR5, UR4, UR3, UR2, UL1, UL3, UL5, UL8, LR8, LR7, LL5 and LL7).
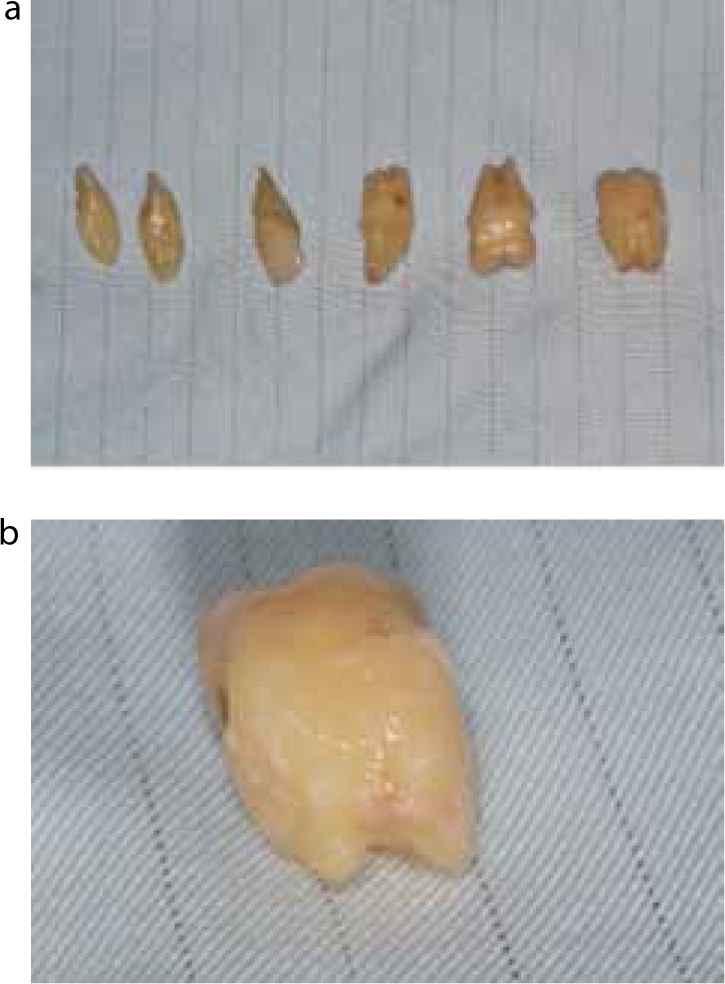
Figure 2.
(a–c) Pre-operative view of the patient with Type-1 dentine dysplasia. Note the normal appearance of the clinical crowns.
Radiographic report for GS
Pulp obliteration with thin crescent-shaped pulps;
Short and narrow root lengths with no radicular pulp;
Multiple periapical radiolucencies associated with the UR7, UR6, UR1, UL2, UL4, UL6, UL7, LR6, LR5, LR4, LR3, LR2, LR1, LL1, LL2, LL3, LL4, LL6 and LL8.
A Cone-Beam CT (CBCT) scan was taken of the LR4–LR5 region for further treatment planning which showed expansion of the buccal and lingual cortical plates (Figure 3).
Figure 3.
(a) Pre-operative dental panoramic tomography showing short malformed roots, obliterated pulp chambers and multiple periapical radiolucencies. (b–d) Pre-operative Cone-Beam CT scan demonstrating expansion of the buccal and lingual cortical plates.
Treatment challenges
When faced with a complex case such as the one presented, the following questions were considered:
How should the multiple periapical lesions on the majority of teeth be managed?
What should be done about the abscess associated with the previously traumatized UR1 with pulp canal obliteration?
What is the best treatment option for the mobile teeth in the lower right quadrant?
How aggressive should our approach to treatment be with this condition overall?
If multiple extractions are planned, should a Clinical Psychologist be consulted to prepare the patient for the loss of her teeth?
Due to the complex nature of GS's management and the difficult management questions above, we wanted to ascertain whether the approach to management would be influenced by the specialty and experience of the operator.
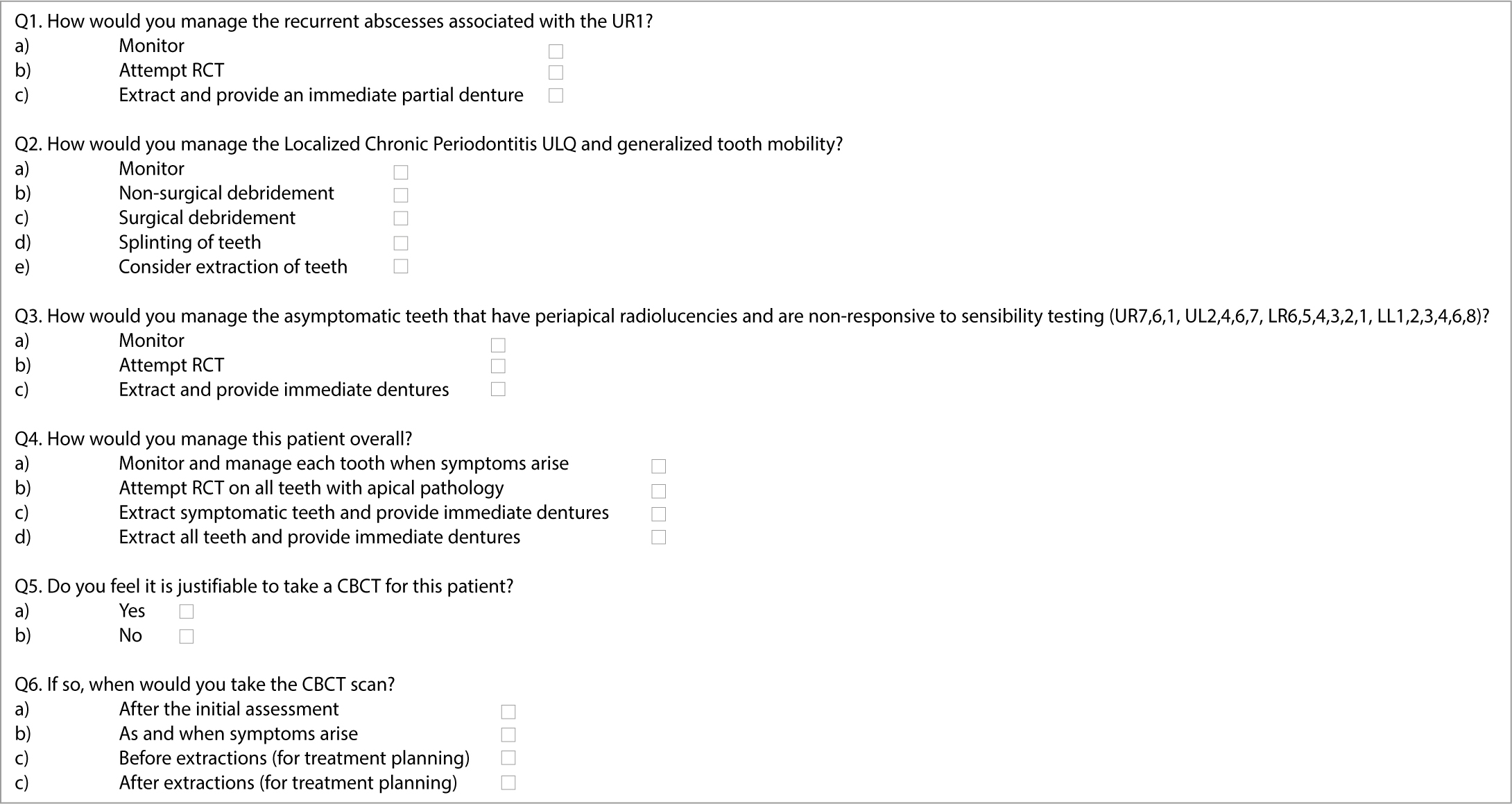
Sixty-four dentists in different specialties and experience were presented with GS's case history, which included the clinical and radiological findings shown in Figures 2 and 3. The clinicians were asked how they would manage various aspects of the case. The questionnaire can be found in Figure 4.
Figure 4. Questionnaire given to the dentists.
Results
Sixty-four dentists who attended a study day course were asked to complete the questionnaire. They included 5 GDPs, one of whom was out of clinical practice, 40 Dental Foundation Trainees, 2 Orthodontic Consultants, 2 Restorative Consultants, 6 Oral Surgeons and 9 Registrars of which 6 were Orthodontic, 1 Paediatric and 2 Restorative.
Although 73.4% of the dentists questioned had heard of DD before, only 12.5% had ever seen a case.
The overall treatment plans varied depending on the level of clinical experience; with experienced clinicians such as Consultants and Registrars preferring to monitor and manage the dentition on a pragmatic basis, whereas dental foundation trainees preferred to intervene earlier on with extractions or root canal treatment, despite the fact that the majority of the teeth had pulp canal obliteration making clinical endodontic treatment challenging.
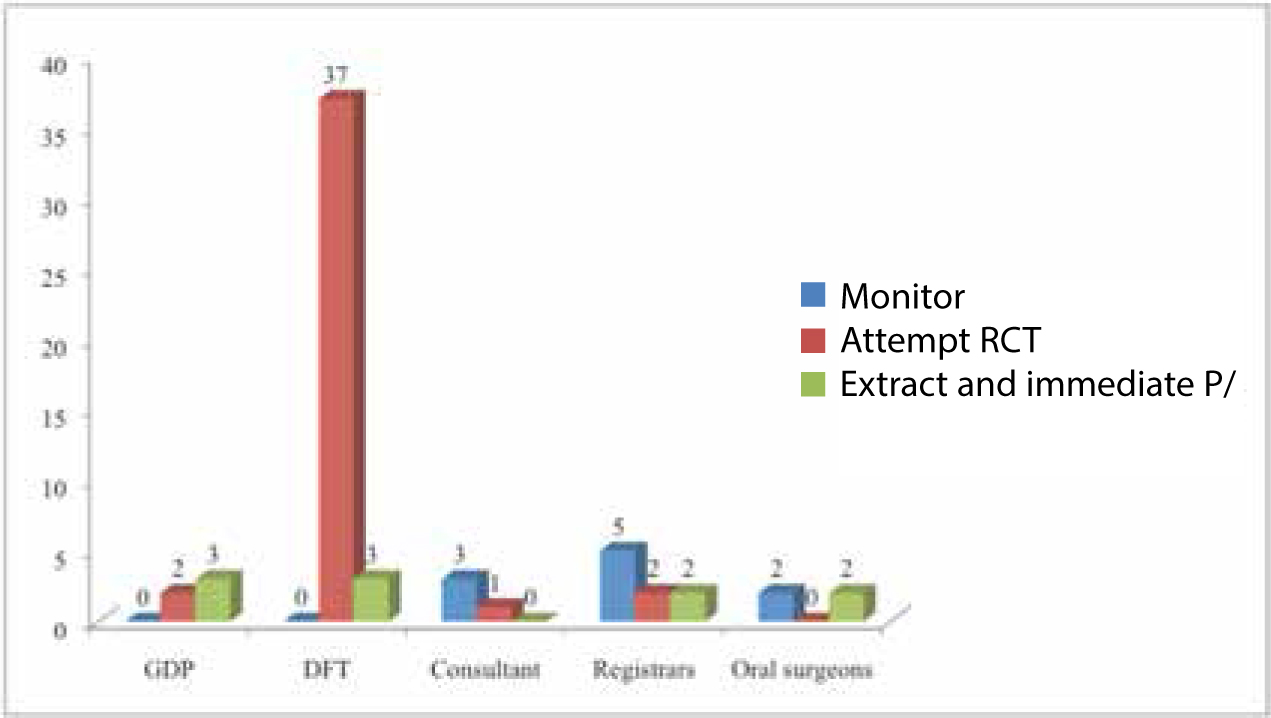
In response to the management of the upper right central incisor with pulp canal obliteration and a dental abscess, 44 of the 64 dentists surveyed (68.75%) would provide root canal treatment of this tooth (Figure 5). Ten dentists (15.6%) would monitor and ten (15.6%) would extract the tooth and provide an immediate partial denture.
Figure 5. Management of the abscess UR1 based on clinician type.
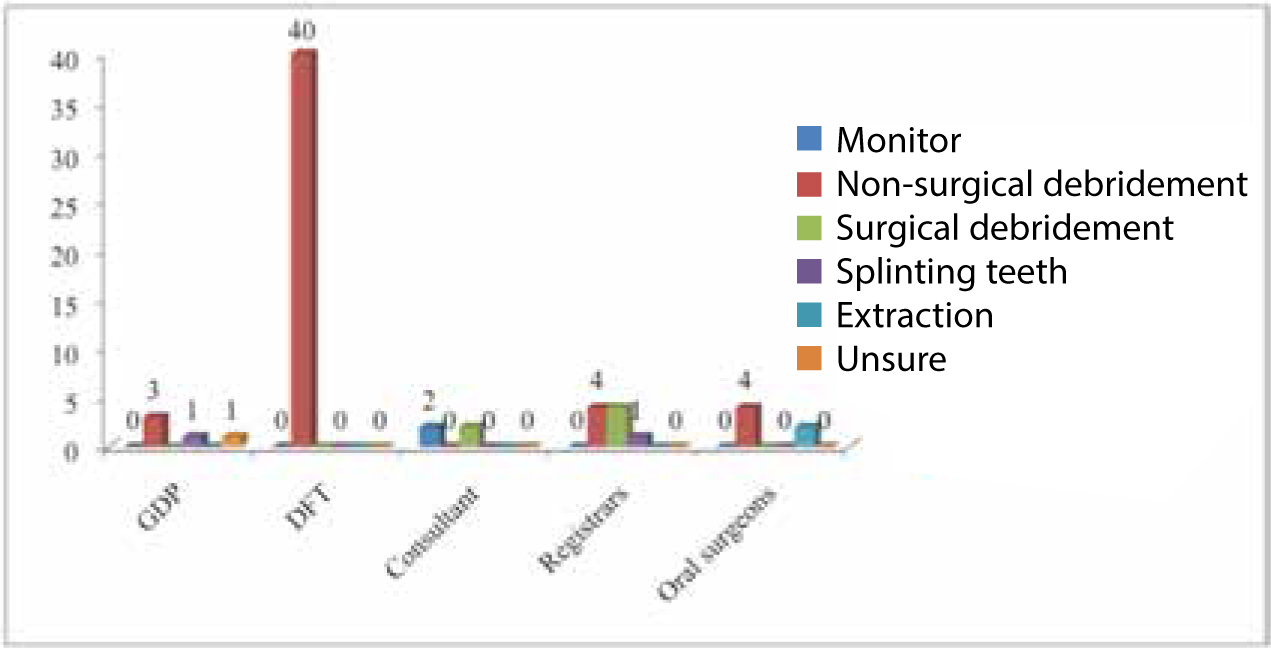
Fifty one (79.7%) dentists would provide non-surgical debridement to stabilize the mobile teeth in the lower right quadrant.
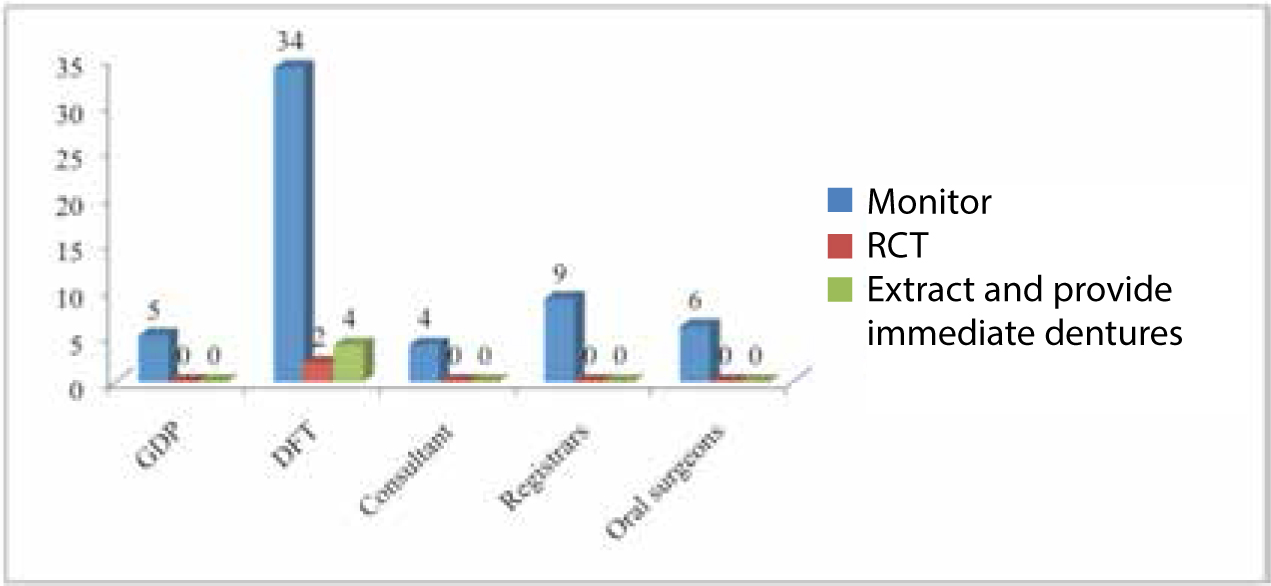
There was almost unanimous agreement (90.6%) that the multiple radiolucencies associated with the necrotic teeth should be monitored and 2 (3.1%) felt that they should be root-filled and 4 (6.2%) would extract them (Figures 6 and 7).
Figure 6. Management of mobile teeth in the lower right quadrant.Figure 7. Management of multiple periapical radiolucencies.
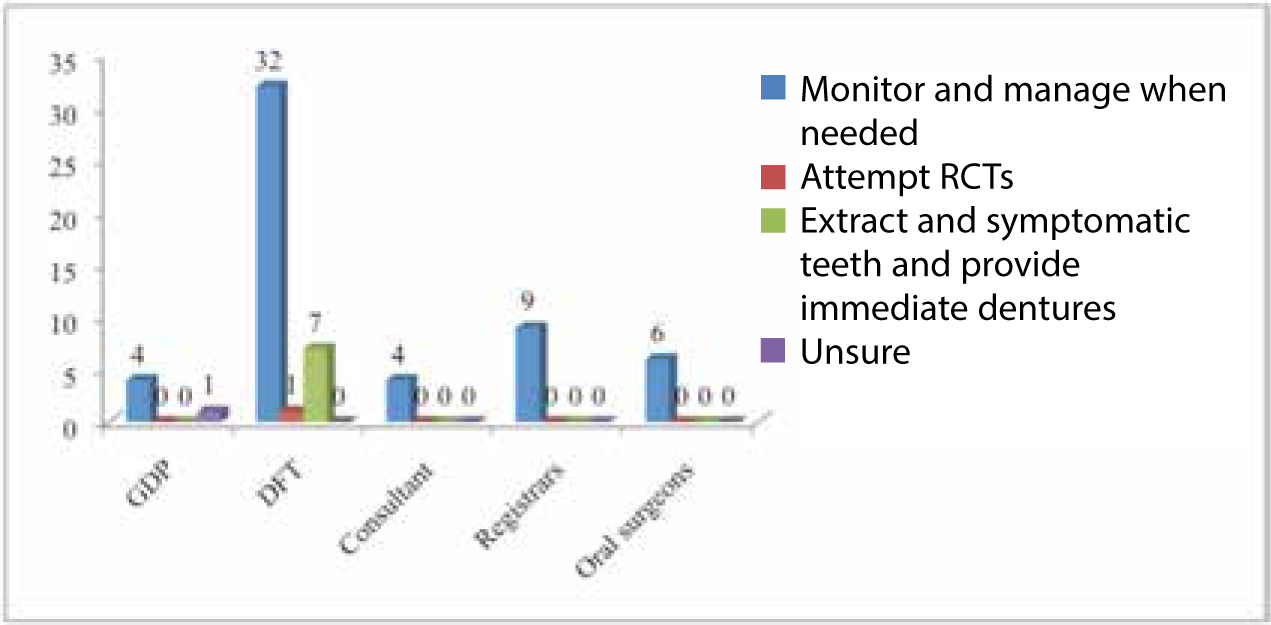
Similarly, 57 (85.9%) would monitor the case as a whole rather than provide invasive, irreversible treatment providing tooth-by-tooth management based on symptoms. Seven of the dentists would extract and provide immediate dentures.
Linked with the above, 47 (73.4%) would like a Cone-Beam CT scan to help plan the management of this patient, with 30 (46.9%) wanting the scan at the time of the initial assessment and 11 (17.2%) preferring to defer acquisition of a CBCT scan until just before the dental extractions. Four dentists (6.3%) would request a scan after the extractions (Figure 8).
Figure 8. Management overall.
Discussion
Type-1 DD is a rare, genetic disorder, resulting in a disturbed formation of dentine. The aetiology of the condition is largely unknown, however, some have suggested that the condition is due to the abnormal interaction between odontoblasts and ameloblasts. The clinical presentation of DD should be recognized as a separate entity from other developmental disorders of the dentition, such as Dentinogenesis Imperfecta, Type-2 DD and Amelogenesis Imperfecta. The key characteristics of Type-1 DD include clinically normal crowns with radiographic evidence of pulp obliteration, rootless teeth and cysts. As this condition is hereditary, there is a 1:2 chance of a child being affected if a parent already has the condition. However, first generation sufferers present with no family history of the disease and often find it difficult to come to terms with the diagnosis and long-term management needed.
The management of DD is complex, hence should be identified early on in a child's dental development within the primary care setting, with the focus on prevention followed by early referral to specialist services. It is often challenging to inform the patients with pulp canal obliteration and periapical abscesses on otherwise asymptomatic teeth that the treatment required involves extractions and removable dentures in the first instance. Hence, motivation for attending dental appointments is often poor. Attempts to treat these teeth endodontically can be considered, as shown by Tidwell and Cunningham9 and others,10 however, patients should be aware that root resorption, further mobility and eventual premature exfoliation of teeth will occur due to the progression of the disorder. Maintenance of periodontal health around mobile teeth is dependent on optimal oral hygiene and regular follow-ups at three-monthly intervals.
The results from the questionnaire revealed that, despite very little experience managing this condition, most dentists preferred a conservative, non-extraction approach. This is reassuring as it allows clinicians to consult other colleagues and delay treatment at a young age, which will inevitably require life-long maintenance. It also gives patients time to understand and come to terms with their condition and the long-term implications.
In the case illustrated above, a patient presenting with multiple cystic asymptomatic lesions with a poor long-term prognosis poses a real challenge to the dental profession. There are many approaches in the management ranging from conservative, monitoring and tooth-by-tooth treatment to extractions and fixed or removable prostheses.
Conclusion
Type-1 DD is a rare, hereditary condition associated with abnormal dentine formation resulting in early loss of teeth. The management of this condition is challenging and inevitably results in extractions and the dilemma on how to replace the teeth. A comprehensive and open discussion between the dental team and patients (and their families) is essential when embarking on invasive and complex treatment following the premature loss of teeth.