Atia GS, May J. Dental fluorosis in the paediatric patient. Dent Update. 2013; 40:836-839
Elkhazindar MM, Welbury RR. Enamel microabrasion. Dent Update. 2000; 27:194-196
Nixon PJ, Gahan M, Robinson S, Chan MFW-Y. Conservative aesthetic techniques for discoloured teeth: 1. The use of bleaching. Dent Update. 2007; 34:98-107
Nixon PJ, Gahan M, Robinson S, Chan MFW-Y. Conservative aesthetic techniques for discoloured teeth: 2. Micro-abrasion and composite. Dent Update. 2007; 34:160-166
Mascarenhas AK. Risk factors for dental fluorosis: a review of the recent literature. Pediatr Dent. 2000; 22:269-277
Thylstrup A, Fejerskov O. Clinical appearance of dental fluorosis in permanent teeth in relation to histologic changes. Community Dent Oral Epidemiol. 1978; 6:315-328
Tekle-Haimanot R, Melaku Z, Kloos H, Reimann C, Fantaye W, Zerihun L, Bjorvatn K. The geographic distribution of fluoride in surface and groundwater in Ethiopia with an emphasis on the Rift Valley. Sci Total Environ. 2006; 367:182-190
Severe fluorosis treated by microabrasion and composite veneers Philippa Hoyle Lyndsey Webb Peter Nixon Dental Update 2024 44:2, 707-709.
Authors
PhilippaHoyle
BChD(Hons), MJDF RCS(Eng), MPros RCS(Ed)
Specialty Registrar in Restorative Dentistry, Department of Restorative Dentistry, Charles Clifford Dental Hospital, 76 Wellesley Road, Sheffield S10 2SZ, UK (philippahoyle1@hotmail.co.uk)
Dental fluorosis results from excessive intake of fluoride either from water resources or products in early childhood. It results in varying degrees of discoloration and pitting of the teeth. This article aims to highlight the conservative management techniques available for managing the aesthetic impact of fluorosis and highlights what can be achieved conservatively with the use of adhesive dentistry.
CPD/Clinical Relevance: Fluorosis can have a huge impact on dental aesthetics, depending on its extent. This in turn can affect a patient's confidence and daily life immensely. In the past, severe fluorosis may have been managed in a more destructive manner with indirect restorations.
Article
Dental fluorosis results from the excessive consumption of fluoride during tooth development. The free fluoride ions disrupt normal enamel mineralization by decreasing the free calcium ion concentrations in the newly mineralized matrix, therefore interfering with the proteases responsible for degrading the matrix proteins during the maturation phase of amelogenesis.1 The retained matrix proteins inhibit crystal growth and result in enamel that is porous and hypomineralized at the time of eruption.1,2 Fluoride has a cumulative effect on enamel formation and its effect depends upon the total fluoride intake, the timing and duration of exposure.1
As the severity of fluorosis increases so does the porosity and fluoride content of the sub-surface enamel, resulting in increased extrinsic staining. Severely affected teeth are more at risk of mechanical surface breakdown. There is a range of fluorosis severity depending upon the extent of porosity.1
Historically, fluorosis has been treated using a variety of techniques. It has been previously suggested that the management of dental fluorosis is dependent upon its severity.2,3 Suggested treatment options include:
Bleaching;
Micro/macroabrasion;
Composite restorations;
Veneers;
Full crowns.
Generally, the literature describes more destructive techniques, such as veneers or full coverage crowns being used for masking the appearance of severe fluorosis. The more conservative approaches are more commonly used for treatment of mild to moderate forms of fluorosis.2,3,4,5,6
Case series
Three siblings presented, one brother aged 17 years, and two sisters aged 18 and 14 years-old. The family had originated from Nazareth, a town in the Ethiopian Rift Valley. All three siblings complained of discoloured teeth, in particular their upper anteriors. They had no other symptoms. They reported living in Nazareth for a number of years prior to becoming teenagers. There were no relevant medical histories. They reported no childhood illnesses or medications. There was no relevant family history. All three siblings had experienced bullying whilst at school in the UK due to the appearance of their teeth.
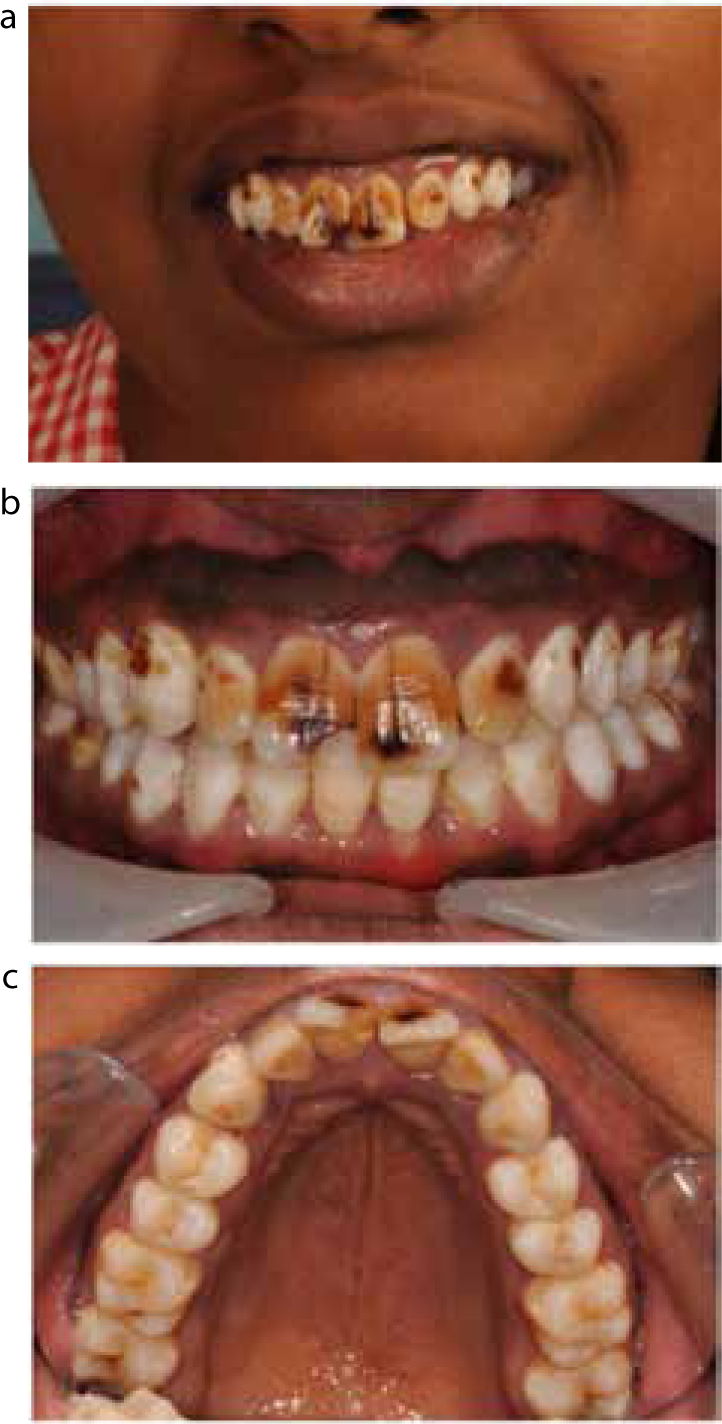
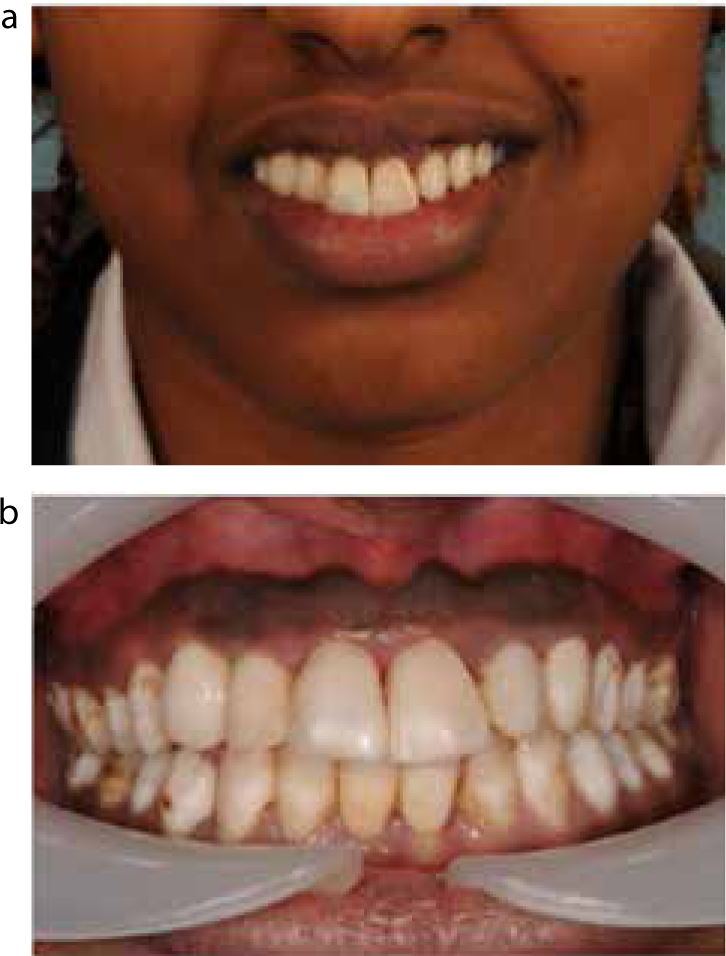
A clinical examination revealed dark brown, mottled staining and pitting, affecting mostly the buccal aspect of upper anterior teeth. There were also white and brown lesions affecting the remaining teeth to a lesser extent. (Figures 1–3).
Figure 1.
(a–c) Patient 1 prior to treatment showing dark brown discoloration of the severe fluorosis affecting the labial aspect of the upper anterior teeth.Figure 2. Patient 2 prior to treatment showing the extent of the brown/black discolorations.Figure 3.
(a–c) Patient 3 prior to treatment emphasizing the relatively unaffected palatal aspects of the teeth.
The diagnosis made was severe dental fluorosis. Patient 1 had LR1 missing due to previous trauma. Patient 3 had an uncomplicated enamel-dentine fracture to the UR1 and periapical periodontitis affecting UL2 due to previous trauma.
Arrangements were made for the patients to be seen by a member of staff for microabrasion and direct composite veneers to improve the appearance of their upper anterior teeth. The gap in the lower anterior region in Patient 1 was restored with two resin-retained bridges. Root canal treatment of UL2 on Patient 3 was also completed.
For these cases microabrasion was completed using Opalustre (Ultradent products, 505 West, 10200 South, South Jordan, Utah, 84095, USA). This contains hydrochloric acid and silicone carbide particles in a gel form. Included in the system is a specialized abrasive rubber cup (Figure 4).
Figure 4. Equipment required for microabrasion with the use of Opalustre. Caulking agent, Dry Dam, Wedjets, Opalustre gel and specialized polishing cup, slow speed hand piece and Bifluorid varnish.
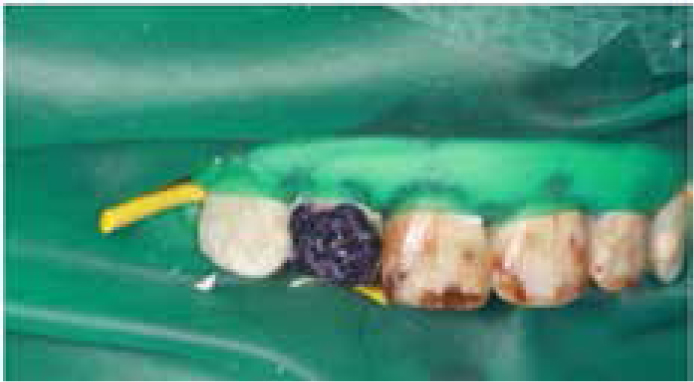
No local anaesthetic was administered in order to help gauge any sensitivity. The teeth to be treated were isolated using a caulking agent (Oraseal®) around the gingival margins (Figure 5) and then rubber dam placed over the top and secured with rubber wedjets (Figure 6). The Opalustre gel was then applied to one tooth at a time using the specialized rubber cup at slow speeds to prevent splattering (Figures 7 and 8). Each application was carried out for 10 seconds and washed thoroughly after each interval with water. This was repeated up to ten times per tooth. Fewer cycles were completed if sensitivity developed. Further polishing with soflex discs can be used on more significant discoloration. A clear fluoride varnish (Bifluorid, Voco, Cuxhaven, Germany) was then applied (Figures 9 and 10). The patients were then reviewed after the teeth had fully rehydrated at least 24 hours after treatment. Owing to the severity of the discoloration, two cycles of microabrasion were required for each case to allow final coverage with composite.
Figure 5. Caulking agent placed around the buccal and palatal gingival margins.Figure 6. Dry dam in place and secured with wedjets.Figure 7. Application of Opalustre gel to the tooth.Figure 8. Use of specialized slow speed brush.Figure 9. Immediately post microabrasion. Note: The initial appearance is affected by the dehydration from being isolated by the rubber dam.Figure 10. Application of clear fluoride varnish.
The patients were reviewed at least two weeks post microabrasion to allow for rehydration of the enamel and for the assessment of how effective the microabrasion had been6 (Figures 11 and 12). Owing to the presence of remaining discoloration, pitting and the poor aesthetic contour of some of the teeth, it was decided that direct composite veneers should be placed.
Figure 11. Patient 1: 2 weeks post microabrasion.Figure 12. Patient 2: after microabrasion.
Composite veneers were placed using a hybrid composite (Miris 2, Coltene Whaledent). The use of a composite with layering properties allows for customized coverage of discoloration defects and a natural result. Opaquers are also available for masking darker discoloration, although none was needed in these cases. Subtle bevel finishing lines at the margins within enamel were placed to reduce ledges at the composite-tooth margin and to allow for a more seamless colour transition (Figures 13–15).6
Figure 13.
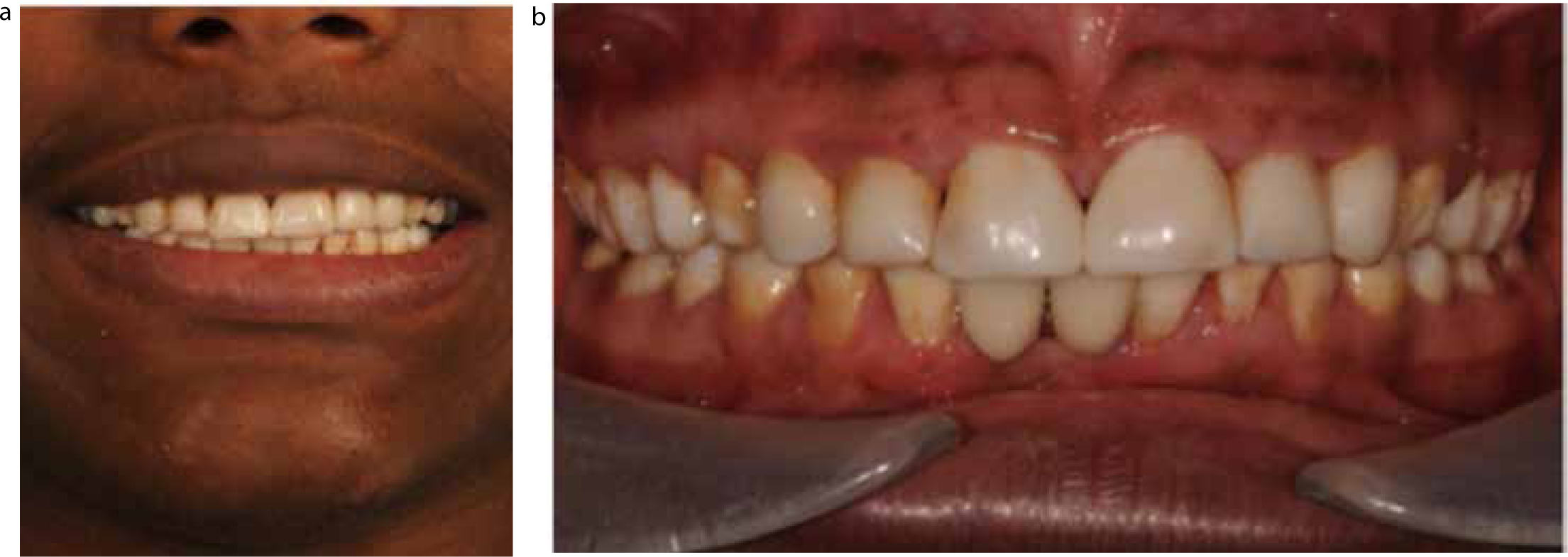
(a, b) Patient 1: post composites and resin-retained bridges.Figure 14.
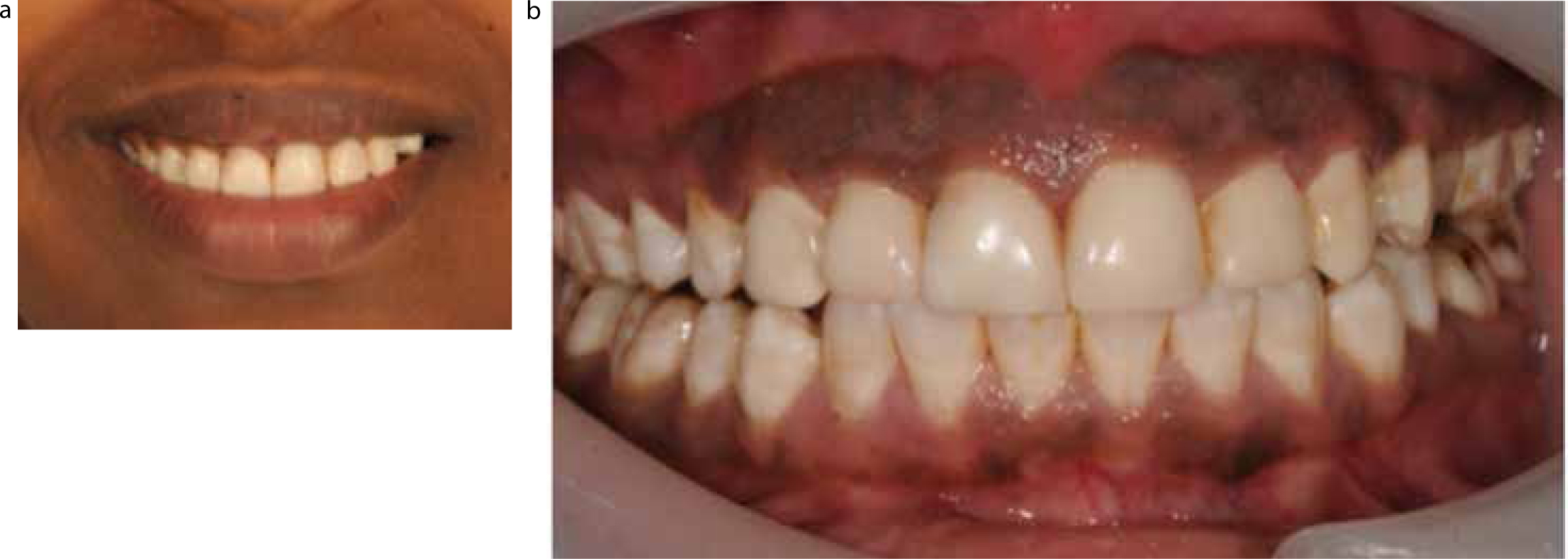
(a, b) Patient 2: post composite placement.Figure 15.
(a, b) Patient 3: post composite placement.
Discussion
Dean's Fluorosis Index, proposed in 1942, suggested the following different classifications of severity based on clinical appearance:
Normal with smooth, glossy, pale creamy-white translucent surface;
Questionable, showing a few white flecks or white spots;
Very mild forms presenting as small opaque white areas, covering less than 25% of the tooth surface;
Mild forms with white areas covering less than 50% of the tooth surface;
Moderate forms affecting all the tooth surfaces, with the presence of some brown staining;
Severe forms with all the tooth surfaces being affected, pitting and brown staining.
The Thylstrup and Fejerskov Index utilizes diagnostic criteria and a scoring system to classify the severity of fluorosis with greater sensitivity and more emphasis on histological changes.7,8
Fluoride has had a positive impact, reducing its prevalence and incidence of dental caries over the past few decades. In developed countries this is largely due to the widespread use of fluoride dentifrices. This has led to an increase in incidence of mild and very mild forms of fluorosis.7 In his early studies, Dean estimated that a water fluoride level of 1.0 ppm led to a 10% prevalence of mild or very mild fluorosis in permanent teeth.8 There is a large range in the prevalence data across the world, ranging from 7.7%–69% in fluoridated communities, and from 2.9%–42% in non-fluoridated communities.7
Fluoridated water is a well-recognized risk factor of fluorosis.7 Fluoride is found in water supplies both naturally and in an artificial capacity (either in organized fluoridation programmes or through pollution).9
The mean fluoride content in drinking water in the East African Rift Valley has been found to be 10 mg-F/L. The World Health Organization guidelines upper limit is 1.5 mg-F/L. This high naturally occurring fluoride content is thought to be due to the fact that the area is still an active volcanic region. The volcanic rocks, particularly in the young basalt, contain high concentrations of fluoride and fluorapatite. The prevalence of dental fluorosis in the Ethiopian Rift Valley ranges from 70%–100% with 35% being affected by the severe form.
Skeletal fluorosis is endemic in the area for those that consume water with fluoride levels of more than 4 mg-F/L for over 10 years. The most common incapacitating neurological complication of crippling skeletal fluorosis is cervical radiculo-myelopathy.10
In all three cases here, microabrasion was initially used to reduce the staining and discoloration, making the defects easier to camouflage. Microabrasion was described in 1986 and has been well documented as a conservative technique for the management of intrinsic superficial discoloration defects, attributed to disruption of mineralization.4
Microabrasion is indicated for superficial defects such as hypoplasia of traumatic or developmental origin, decalcification associated with orthodontic brackets and white and brown discoloration from fluorosis. Contra-indications include intrinsic discoloration, tetracycline staining, Amelogenesis Imperfecta and Dentinogenesis Imperfecta.4,6
Enamel microabrasion is the use of simultaneous erosion and abrasion to remove the superficial enamel. It is intended to remove between 50–200 µm of enamel.6 This enamel removal is pressure dependant, and careless application of this technique can be destructive.
Hydrochloric acid (18%) is used most commonly for microabrasion. Most often it is combined with a granular substance to create a slurry. Phosphoric acid (18% or 35% in the form of dental acid-etch) has also been used to a lesser extent. Alternative techniques such as air/particulate abrasion and macroabrasion with the use of fine diamond burs or multi-bladed tungsten carbide burs have also been described.4,6
In some cases, vital bleaching techniques have been used prior to composite placement. At home bleaching has been described using soft-plastic, vacuum-formed night guards, either with or without reservoirs, in conjunction with 10% carbamide peroxide. The patient, usually on a nightly basis, uses these for 2–6 week periods. Other regimens have been suggested, including using the guard for several days as much as possible, changing the bleaching gel on a 3–4 hourly basis to achieve a quicker result. But this usually just results in increased sensitivity and does not achieve quicker or better results.
If bleaching is to be used in combination with composites, it is sensible to allow a two-week delay before composite placement to allow both for shade regression and for any residual oxygen to diffuse away, as it is thought to have a detrimental effect on composite bonding.5,6 Owing to the very dark discoloration of the teeth here, no bleaching was undertaken for these cases.
Conclusions
This case series demonstrates that a conservative restorative approach can be used to mask even severe fluorosis. Consideration of such techniques in treatment planning is required to reduce the biological cost of using more traditional methods.