Georgaklis C. Difficult case types: Part 1. A discussion of adult short-term orthodontics. Dentistry Today. 2012; 31:84-87
Vicéns J, Russo A. Comparative use of Invisalign by Orthodontists and General Practitioners. Angle Orthodontist. 2010; 80:425-434
Djeu G, Shelton C, Maganzini A. Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American Board of Orthodontics objective grading system. Am J Orthod Dentofacial Orthop. 2005; 128:292-298
Maini A. Short-term cosmetic orthodontics for general dental practitioners. Br Dent J. 2013; 214:83-84
Simon M, Keilig L, Schwarze J Treatment outcome and efficacy of an aligner technique – regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health. 2014; 14
Badran S. The effect of malocclusion and self-perceived aesthetics on the self-esteem of a sample of Jordanian adolescents. Eur J Orthod. 2010; 32:638-644
Cunningham S, Hunt N. Quality of life and its importance in orthodontics. J Orthod. 2001; 28:152-158
Gazit-Rappaport T, Haisraeli-Shalish T, Gazit E. Psychosocial reward of orthodontic treatment in adult patients. Eur J Orthod. 2010; 32:441-446
Miller KB, McGorray SP, Womack R A comparison of treatment impacts between Invisalign aligner and fixed appliance therapy during the first week of treatment. Am J Orthod Dentofacial Orthop. 2007; 131:(302)e1-e9
Nedwed V, Miethke R. Motivation, acceptance and problems of invisalign patients. J Orofacial Orthopaed. 2005; 66:162-173
Mizrahi E. Risk management in clinical practice. Part 7. Dento-legal aspects of orthodontic practice. Br Dent J. 2010; 209:381-390
Brace yourself. Riskwise UK. 2012; 42:14-15
Chate R. Short-term orthodontics: high profitability and low risk. Br Dent J. 2014; 217
Ireland A, Willmot D, Hunt N. An introduction to dento-legal issues and risks in orthodontics. Br Dent J. 2015; 218:197-201
Sandy J, Ireland T. Orthodontics: a themed issue. Br Dent J. 2015; 218
Marques L, Freitas N, Pereira L Quality of orthodontic treatment performed by orthodontist and general dentists. Angle Orthod. 2012; 82:102-106
Kravitz N, Kusnoto B, BeGole E How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am J Dentofacial Orthop. 2009; 135:27-35
Malik OH, McMullin A, Waring DT. Invisible Orthodontics Part 1: Invisalign. Dent Update. 2013; 40:203-215
Kuncio D, Maganzini A, Shelton C Invisalign and traditional orthodontic treatment postretention outcomes compared using the American Board of Orthodontics Objective Grading System. Angle Orthod. 2007; 77:864-869
Ali SAAH, Miethke HR. Invisalign®, an innovative invisible orthodontic appliance to correct malocclusions: advantages and limitations. Dent Update. 2012; 39:254-260
Lang G, Alfter G, Göz G Retention and stability – taking various treatment parameters into account. J Orofacial Orthop. 2001; 63:26-41
Chate R. Truth or consequences: the potential implications of short-term cosmetic orthodontics for general dental practitioners. Br Dent J. 2013; 215:551-553
Kirschen R. Letters to the Editor: Short-lived benefits. Br Dent J. 2013; 214
Fleming P, Springate S, Chate R. Myths and realities in orthodontics. Br Dent J. 2015; 218:105-110
Kacer K, Valiathan M, Narendran S Retainer wear and compliance in the first 2 years after active orthodontic treatment. Am J Orthod Dentofacial Orthop. 2010; 138:592-598
Pratt M, Kluemper T, Lindstrom A. Patient compliance with orthodontic retainers in the postretention phase. Am J Orthod Dentofacial Orthop. 2010; 140:196-201
Ackerman M, Thornton B. Posttreatment compliance with removable maxillary retention in a teenage population: a short-term randomized clinical trial. Orthodontics. 2011; 12:22-27
Sun J, Yu Y, Liu M. Survival time comparison between Hawley and clear overlay retainers: a randomized trial. J Dent Res. 2011; 90:1197-1201
Taner T, Aksu M. A prospective clinical evaluation of mandibular lingual retainer survival. Eur J Orthod. 2012; 34:470-474
Schneider E, Ruf S. Upper bonded retainers. Angle Orthod. 2011; 81:1050-1056
Booth F, Edelman J, Proffit W. Twenty-year follow-up of patients with permanently bonded mandibular canine-to-canine retainers. Am J Orthod Dentofacial Orthop. 2008; 133:70-76
Johnston C, Littlewood S. Retention in orthodontics. Br Dent J. 2015; 218:119-122
Lyotard N, Hans M, Nelson S Short-term postorthodontic changes in the absence of retention. Angle Orthod. 2010; 80:1045-1050
Darcey J, Qualtrough A. Resorption: part 1. Pathology, classification and aetiology. Br Dent J. 2013; 214:439-451
Sandy J. Northcroft Memorial Lecture 2006: The future of specialist training. J Orthod. 2007; 34:177-184
Patel S. An orthodontic registrar's life: spinning many plates. Br Dent J. 2015; 218
O'Brien K, Spencer J. A viewpoint on the current status of UK orthodontic education and the challenges for the future. Br Dent J. 2015; 218:181-183
Rock W, O'Brien K, Stephens C. Orthodontic teaching practice and undergraduate knowledge in British dental schools. Br Dent J. 2002; 192:347-351
The limitations of short-term orthodontics and why we still need specialists – a review of the current literature Sana Luqmani Dental Update 2024 44:1, 707-709.
Authors
SanaLuqmani
BDS(Hons), MJDF RCS(Eng), MSc
General Dental Practitioner, ConfiDental Clinic, 359 Ewell Road, Surbiton, KT6 7BZ, UK (sluqmani@hotmail.com)
Short-term orthodontics (STO) serves to align anterior teeth. It has become popular in cosmetic dentistry as an alternative to destructive veneers and lengthy conventional orthodontics. The aim of this article is to raise awareness of the clinical limitations of STO and highlight some of the difficulties encountered with orthodontic retention. It also gives an overview of accredited training available to dentists who wish to develop their orthodontic skills.
CPD/Clinical Relevance: Greater awareness of the clinical limitations of short-term orthodontics will aid GDPs in appropriately selecting their cases and obtaining informed consent from patients. In addition, the article serves as encouragement for those GDPs wishing to develop their orthodontic skills and pursue further accredited training.
Article
Short-term orthodontics (STO) is a cosmetic treatment that aims to enhance a patient's smile by aligning his/her anterior teeth. It is provided predominantly by General Dental Practitioners (GDPs) and is offered privately to adults as a quicker and less destructive alternative to conventional orthodontics or veneers. It has been an accepted treatment modality in the United States of America for over a decade1 and has recently gained popularity in the United Kingdom. Dentists are increasingly practising STO and the range of available STO appliances is presently greater than ever.
The first STO system to be brought to the market was Invisalign in 1997; Align Technology initially intended its use only by orthodontists but due to great success and demand, two years later made it also accessible to GDPs.2 Soon, other companies such as Inman Aligner, Six Month Smiles and Fastbraces followed suit.
Being a cosmetically motivated treatment, STO addresses malalignment of incisors and canines only, the so-called ‘social six’. It does not aim to correct imperfections in the posterior occlusion or change the Angle's class; rather, it is designed for simple anterior malocclusions in the adult patient with a fully developed jaw. The tooth movements achieved are predominantly tipping motions,3,4 but in some cases bodily movements can also be produced.5 The appliances are characteristically inconspicuous and may be of fixed or removable nature. Aesthetically acceptable results can typically be obtained in less than 6 months.4
In order to provide STO, dentists are not required to possess any postgraduate qualifications in orthodontics. The relevant training is usually acquired in short-course format over 2–3 days and is delivered by the commercial companies which supply the respective orthodontic appliance. In addition to technical aspects of the respective appliance, case selection and treatment planning, dentists are also taught how to market STO. Typically, the instructors on these courses are primary care dental practitioners without any university-accredited qualification in orthodontics.6 Exceptions are Quick Straight Teeth (QST) and Intelligent Alignment Systems (IAS) Academy who do include specialist orthodontists as instructors on their courses.
Benefits of STO
An online survey conducted on behalf of the British Orthodontic Society in 2010 revealed that 45% of adults in the UK were unhappy with the appearance of their teeth; 20% would have considered orthodontics to improve their smile.7 However, adult patients were often reluctant to accept conventional orthodontics owing to the lengthy treatment period and were much more willing to accept the compromise offered by STO: shorter treatment times whilst only those teeth visible in the smile line were aligned.4
Tooth alignment in adults has been shown to improve self-esteem8 and quality of life post-treatment.9,10 A prospective cohort study conducted in 2007 on 60 adult patients showed that treatments such as Invisalign were less frequently associated with pain (p < 0.0001) and overall negative impact on quality of life during treatment (p < 0.0001) when compared with conventional fixed appliance therapy.11 Another survey confirmed that 89% of patients undergoing Invisalign treatment were satisfied with the progress of their treatment.12
Limitations of STO
Together with the rise in popularity of STO, unfortunately there has also been increasing focus on cases of litigation in orthodontics. Between 2005 and 2010, 2.9% of cases presented to the General Dental Council (GDC) committee for professional misconduct were in relation to orthodontic treatment.13 More specifically, in 2010, 20% of all malpractice cases reported to Dental Protection Limited were due to STO treatments, of which 80–90% were performed by GDPs.14 Earlier data were sought for comparison but found to be unavailable.
In response to the above figures, sceptical members of the British Orthodontic Society (BOS) have made anecdotal claims suggesting that most GDPs had not been adequately trained in orthodontics and were therefore unable to foresee inaccuracies in tooth movements and manage situations where teeth were being moved into inherently unstable positions.15,16,17 In a study of 60 orthodontic cases, it was found that GDPs with no specialist training did indeed achieve significantly poorer treatment outcomes than specialists.18
In addition, other authors have highlighted the technical limitations of STO. Kravitz et al showed that Invisalign was only able to achieve a mean of 41% accuracy on planned anterior tooth movements.19 Refinement of the end result was often required with supplementary aligners and auxiliaries such as elastics.20 Moreover, a comparative retrospective study on patients treated with Invisalign (n = 11) and conventional fixed appliance therapy (n = 11) by an operator with postgraduate orthodontic qualifications revealed that Invisalign was more frequently associated with relapse following a retention period of 12 months. Both treatment groups were matched for complexity of their cases, and all treatments were performed by a single clinician.21 The small sample size in this study does not allow reliable conclusions to be drawn. However, it does suggest that the nature of tooth movements achieved with STO were inherently less stable than those achieved with conventional orthodontics. A recently published paper on the nature and effects of Invisalign confirms that root paralleling could not be achieved with this treatment modality, leading to decreased stability of the end result.22 Interestingly, another study demonstrated an association between short orthodontic treatment times and higher relapse rates.23 Maini therefore correctly stressed the importance of lifelong retention following STO with a bonded wire or removable clear overlay retainer (COR).4
This heavy reliance upon permanent retention has caused serious concern amongst several specialist orthodontists.24,25 Fleming et al argued that bonded retainers did not effectively resist soft tissue pressures and were therefore unable to prevent relapse in some cases.26 In addition, studies have shown that bonded retainers suffered from high failure rates whilst patient compliance with removable retainers was often poor.
Removable retainers
A questionnaire-based study of 1,200 adolescent patients demonstrated that 3 months into the retention period only 69% wore their removable retainers as instructed by their orthodontist. At 2 years, the compliance rate decreased to 45% and 20% of patients did not wear their retainers at all after 2 years, despite instructions for continued life-long wear at night.27 In another survey of patients aged between 8 and 72 years, Pratt et al showed that the older the patient, the less compliant he/she was with retainer wear in the first 6 months.28 This is particularly relevant to STO where the vast majority of patients are aged 20 or older. Moreover, it is speculated that the above quoted figures are in actual fact an under-estimation of true compliance rates as patients have been shown to over-represent their retainer wear in self-reported compliance studies.29
In addition to patient-related factors, it is thought that broken and lost retainers may contribute to poor compliance rates. A randomized control trial demonstrated that 31% of all upper and 49% of all lower CORs fractured within the first year of retention, and that 27% and 22%, respectively, were lost within 12 months.30 Added together, these figures would suggest that a relatively high percentage of patients were inadequately retained after one year. However, this is not clear from the result of the study as the authors examined only the survival of original retainers issued at the end of active treatment; repairs and replacement retainers were not followed up.
Bonded retainers
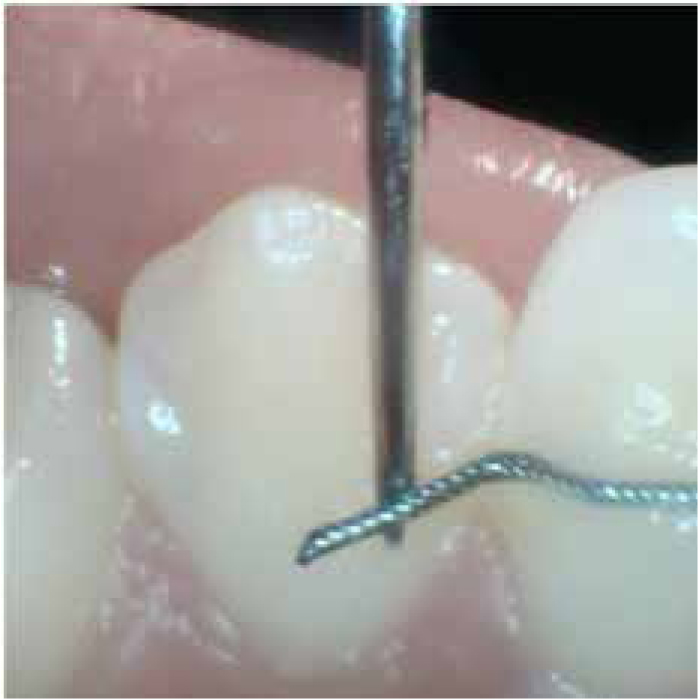
The use of bonded retainers is more common following STO, but their efficacy has also been criticized. Taner and Aksu showed that 37.9% of lower bonded wires had partially detached, fractured or completely debonded within 6 months.31 In a retrospective study of upper bonded wire retainers, 58.2% had failed over 8 to 42 months. Failure rates were higher for inexperienced operators and, interestingly, canine-to-canine retainers were the most likely to fail;32 this is the retainer design most commonly used with STO. In a long-term follow-up study of mandibular canine-to-canine bonded retainers, 25% of patients no longer had their retainers in place at a 20-year recall. Of those that were still present, 38% had required repairs on one or more occasions (Figure 1).33
Figure 1. Partially detached bonded retainers can remain undiagnosed unless carefully checked with a probe at routine examination.
Relapse
The consequence of inadequate retention is orthodontic relapse; return of the post-treatment result to the original malocclusion.34 A short-term follow-up study of 30 subjects treated with a fixed appliance showed that relapse of lower incisor crowding could occur in as little as 4 weeks in the absence of retention.35
Should a patient experience relapse and then opt to undergo a repeat course of STO, there may well be not only a financial but also a biological cost. Repeatedly exposing teeth to tipping forces, such as those predominant in STO,4 has been associated with external cervical root resorption.36
Orthodontic training for GDPs
Health Education England is now increasingly offering orthodontic study days for GDPs. These study days are led by specialists and provide guidance on how to manage the limitations of STO. Emphasis is placed on the importance of anticipating possible complications and adequately informing patients as part of the consent process, as well as recognizing when to seek help from a specialist. The rising popularity of STO-themed study days was reflected by the findings of a recent study conducted by the author of this article. A total of 376 GDPs in East Sussex were surveyed about their experience of providing STO, of which 53 (14%) responded. Despite this very low response rate, the survey did provide some statistically significant results: 60% (n = 6) of GDPs who were providing STO expressed an interest in additional clinical support from their local orthodontist in the form of seminars, study groups and one-to-one advice. Amongst those respondents not performing STO, the most commonly stated reason for not wishing to provide the service was a lack of orthodontic knowledge and training (n = 24, 57%). Specialist orthodontists remain the best trained individuals to treat malocclusions, especially those that are more complex and require extractions. It is their role exclusively to manage the non-adult patient and those requiring orthognathic surgery.
Specialist orthodontic training
In order to become a specialist orthodontist in the UK, dentists must undergo a minimum of three years of full-time postgraduate study at an accredited university.37 Teaching is delivered in the form of lectures, practical and technical sessions, seminars, tutorials and self-directed learning. In addition, students are required to work in specialist registrar posts at teaching hospitals and regional units where their clinical practice is supervised by consultant orthodontists.38 The syllabus is part of a national curriculum produced by the Specialty Advisory Committee in Orthodontics and has been approved by the GDC. It consists of 34 modules and covers topics such as normal and abnormal facial growth, diagnosis and treatment planning, biological principles of tooth movement and, importantly, limitations of orthodontic treatment.39 Specialist registrars must also participate in the delivery of undergraduate teaching and work together with maxillofacial surgeons and restorative dentists to provide multidisciplinary care. Throughout their training, postgraduate students are assessed by means of case presentations, written, oral and clinical examinations. Furthermore, it is a mandatory requirement to undertake an independently led research project and submit a dissertation of 15,000–18,000 words. Upon successful completion of specialist training, dentists are awarded with either a Master of Science (MSc) or Master of Clinical Dentistry (MClinDent) degree in orthodontics.40,41,42 This degree then makes them eligible to sit a two-day examination for Intercollegiate Membership in Orthodontics (MOrth) which, once acquired, finally facilitates inclusion on the GDC's specialist register.
Diploma in Primary Care Orthodontics
For GDPs who would like to pursue their interest in orthodontics without arduous specialist training, in 2007 the Faculty of General Dental Practitioners (FGDP) introduced a diploma in Primary Care Orthodontics.43 This consisted of a three-year part-time training programme held in London and Manchester.44 The syllabus was developed together with Dr Iain Hathorn, then chairman of the BOS, and set a national standard for orthodontic patient care in general dental practice. The programme comprised a total of 1,200 learning hours and was delivered in the form of lectures, distance learning and clinical supervision in the workplace which may either be in a primary care or hospital setting.45 Trainees were assessed by the FGDP and Royal College of Surgeons throughout the three years and by means of a final examination at the end of their training.46
Successful completion of the diploma led to accreditation as a Dentist with Special Interest (DwSI) in Orthodontics.
Unfortunately, this course has now been discontinued by the FGDP.
Conclusion
Short-term orthodontics is a useful tool in the armamentarium of the GDP who is interested in cosmetic dentistry. For many patients it is a viable alternative to veneers and conventional orthodontics. However, clinicians must recognize its limitations and be aware of the limitations of their training. GDPs who wish to develop their orthodontic skills and treat more complex cases at present only have the option of undergoing specialist training. The author of this article would strongly welcome the re-introduction of the Diploma in Primary Care Orthodontics with a focus on STO. This would enable GDPs to further their interest in orthodontics at an accredited institution without the need for arduous specialist training.