Fagerstad A, Lundgren J, Arnrup K. Dental fear among children and adolescents in a multicultural population – a cross-sectional study. Swed Dent J. 2015; 39:109-120
London: HSCIC; 2015
Soares FC, Souto G, Lofrano M, Colares V. Anxiety related to dental care in children and adolescents in a low-income Brazilian community. Eur Arch Paediatr Dent. 2015; 16:149-152
de Menezes Abreu DM, Leal SC, Mulder J, Frencken JE. Patterns of dental anxiety in children after sequential dental visits. Eur Arch Paediatr Dent. 2011; 12:298-302
Colares V, Franca C, Ferreira A, Amorim Filho HA, Oliveira MC. Dental anxiety and dental pain in 5- to 12-year-old children in Recife, Brazil. Eur Arch Paediatr Dent. 2013; 14:15-19
Davidovich E, Pessov Y, Baniel A, Ram D. Levels of stress among general practitioners, students and specialists in pediatric dentistry during dental treatment. J Clin Pediatr Dent. 2015; 39:419-422
London: HSCIC; 2014
London: DOH; 2013
London: DOH; 2012
Pearse RM, Moreno RP, Bauer P Mortality after surgery in Europe: a 7 day cohort study. Lancet. 2012; 380:(9847)1059-1065
London: NICE; 2010
Millar K, Asbury AJ, Bowman AW A randomised placebo-controlled trial of the effects of midazolam premedication on children's postoperative cognition. Anaesthesia. 2007; 62:923-930
Somri M, Parisinos CA, Kharouba J Optimising the dose of oral midazolam sedation for dental procedures in children: a prospective, randomised, and controlled study. Int J Paediatr Dent. 2012; 22:271-279
Kaufman E, Weinstein P, Sommers EE, Soltero DJ. An experimental study of the control of the gag reflex with nitrous oxide. Anesth Progr. 1988; 35:155-157
Paterson SA, Tahmassebi JF. Paediatric dentistry in the new millennium: 3. Use of inhalation sedation in paediatric dentistry. Dent Update. 2003; 30:350-358
Foley J. The way forward for dental sedation and primary care?. Br Dent J. 2002; 193:161-164
Davies CHM, Roberts G.London: RCS(Eng); 2008
London: IACSD; 2015
Averley PA, Lane I, Sykes J, Girdler NM, Steen N, Bond S. An RCT pilot study to test the effects of intravenous midazolam as a conscious sedation technique for anxious children requiring dental treatment – an alternative to general anaesthesia. Br Dent J. 2004; 197:553-558
Newton JT, Shah S, Patel H, Sturmey P. Non-pharmacological approaches to behaviour management in children. Dent Update. 2003; 30:194-199
Greenbaum PE, Turner C, Cook EW, Melamed BG. Dentists' voice control: effects on children's disruptive and affective behavior. Health Psychol: official journal of the Division of Health Psychology, American Psychological Association. 1990; 9:546-558
McKnight-Hanes C, Myers DR, Dushku JC, Davis HC. The use of behavior management techniques by dentists across practitioner type, age, and geographic region. Pediatr Dent. 1993; 15:267-271
Carson P, Freeman R. Tell-show-do: reducing anticipatory anxiety in emergency paediatric dental patients. Int J Health Promot Educ. 1998; 36:87-90
Allen KD, Stark LJ, Rigney BA, Nash DA, Stokes TF. Reinforced practice of children's cooperative behavior during restorative dental treatment. ASDC J Dent Child. 1988; 55:273-277
Weinstein P, Nathan JE. The challenge of fearful and phobic children. Dent Clin N Am. 1988; 32:667-692
Wilson S, Cody WE. An analysis of behavior management papers published in the pediatric dental literature. Pediatr Dent. 2005; 27:331-338
Melamed BG, Weinstein D, Hawes R Reduction of fear-related dental management problems with use of filmed modelling. J Am Dent Assoc. 1975; 90:822-826
Armfield JM, Heaton LJ. Management of fear and anxiety in the dental clinic: a review. Aust Dent J. 2013; 58:390-407
Wright GZSP, Gardner DE.London: Elsevier Health Sciences; 1987
Aitken JC, Wilson S, Coury D, Moursi AM. The effect of music distraction on pain, anxiety and behavior in pediatric dental patients. Pediatr Dent. 2002; 24:114-118
Miller AC, Hickman LC, Lemasters GK. A distraction technique for control of burn pain. J Burn Care Rehabil. 1992; 13:576-580
Foertsch CE, O'Hara MW, Stoddard FJ, Kealey GP. Treatment-resistant pain and distress during pediatric burn-dressing changes. J Burn Care Rehabil. 1998; 19:219-224
Sharar SR, Miller W, Teeley A Applications of virtual reality for pain management in burn-injured patients. Expert Rev Neurother. 2008; 8:1667-1674
Miller K, Rodger S, Kipping B, Kimble RM. A novel technology approach to pain management in children with burns: a prospective randomized controlled trial. Burns: journal of the International Society for Burn Injuries. 2011; 37:395-405
Jeffs D, Dorman D, Brown S Effect of virtual reality on adolescent pain during burn wound care. J Burn Care Res: official publication of the American Burn Association. 2014; 35:395-408
Guinot Jimeno F, Mercade Bellido M, Cuadros Fernandez C Effect of audiovisual distraction on children's behaviour, anxiety and pain in the dental setting. Eur J Paediatr Dent: official journal of the European Academy of Paediatric Dentistry. 2014; 15:297-302
Prabhakar AR, Marwah N, Raju OS. A comparison between audio and audiovisual distraction techniques in managing anxious pediatric dental patients. J Ind Soc Pedodont Prevent Dent. 2007; 25:177-182
Ram D, Shapira J, Holan G, Magora F, Cohen S, Davidovich E. Audiovisual video eyeglass distraction during dental treatment in children. Quintessence Int. 2010; 41:673-679
Nuvvula S, Alahari S, Kamatham R, Challa RR. Effect of audiovisual distraction with 3D video glasses on dental anxiety of children experiencing administration of local analgesia: a randomised clinical trial. Eur Arch Paediatr Dent. 2015; 16:43-50
Hoge MA, Howard MR, Wallace DP, Allen KD. Use of video eyewear to manage distress in children during restorative dental treatment. Pediatr Dent. 2012; 34:378-382
Bentsen B, Wenzel A, Svensson P. Comparison of the effect of video glasses and nitrous oxide analgesia on the perceived intensity of pain and unpleasantness evoked by dental scaling. Eur J Pain–London. 2003; 7:49-53
Zhang G, Hou R, Zhou H Improved sedation for dental extraction by using video eyewear in conjunction with nitrous oxide: a randomized, controlled, cross-over clinical trial. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012; 113:188-192
Chew LC, King NM, O'Donnell D. Autism: the aetiology, management and implications for treatment modalities from the dental perspective. Dent Update. 2006; 33:70-83
Mazurek MO, Wenstrup C. Television, video game and social media use among children with ASD and typically developing siblings. J Autism Dev Disord. 2013; 43:1258-1271
Wilson KE. Overview of paediatric dental sedation: 2. Nitrous oxide/oxygen inhalation sedation. Dent Update. 2013; 40:822-829
Could video glasses contribute to behaviour management in the 21st century? Abdullah Casaus Biraj Patel Laura Brown Kristian Coomaraswamy Dental Update 2024 44:1, 707-709.
Authors
AbdullahCasaus
Academic Clinical Fellow in Paediatric Dentistry, Department of Paediatric Dentistry, King's College Hospital (a.casaus@nhs.net)
Dental fear in the paediatric population can be a significant barrier to providing optimal dental care. Pharmacological management techniques utilized to manage anxiety, such as conscious sedation and general anaesthesia, are expensive and require specialized equipment with additional staff training. With recent advances in technology, video glasses are an economic and novel distraction technique that may aid in improving behaviour management and facilitate dental treatment.
CPD/Clinical Relevance: Nervous children may find difficulty in accessing care owing to their inability to co-operate and accept dental treatment. This paper describes an innovative technique that may aid the clinician in overcoming this barrier.
Article
Paediatric dental anxiety in the UK
The dental team play a pivotal role in making a child's visit to the dentist a positive experience. It is often necessary to adapt communication and behaviour management techniques in order to ensure patient comfort and compliance. Apprehension towards dental treatment, however, can impede the provision of care and affect a child's long-term outlook on dentistry.1
In the Child Dental Health Survey of 2013, the prevalence of anxiety in the UK was assessed. Overall, 14% of 12-year-olds and 10% of 15-year-olds were found to suffer from extreme dental anxiety. Higher anxiety levels of 21% and 17% were reported in 5- and 8-year-old children, respectively. In regards to gender differences, boys seem to report less dental anxiety compared to girls, which may be due to a reluctance in describing their dental fear. Unsurprisingly, the administration of local anaesthetic elicited the highest anxiety scores in both the 12- and 15-year-old age groups.2
Anxiety, oral health and dental staff stress
It is essential that dental phobia is appropriately managed owing to its impact on a child's oral health. Anxiety is common in children who irregularly attend the dentist and miss several appointments.3 This cohort of children exhibit increased caries morbidity or DMFT (Decayed Missing or Filled teeth) scores.4 Additionally, children with higher anxiety levels tend to suffer more dental pain compared to co-operative children.5
It is not only patients that suffer as a consequence of their dental phobia. Levels of stress can be elevated in the operating practitioner whilst undertaking dental treatment in a nervous child. This may affect rational thought and can be associated with significant health risks in the long term.6
General anaesthesia
Currently in the UK general anaesthesia is a commonly used pharmacological technique to manage insufficient co-operation in children. In 2013–2014, 46,500 children and young people in England under 19 years of age were admitted to hospital as a result of dental caries. The numbers are highest in the 5–9 year-old age category in which there has been a 14% rise in admissions since 2010–2011.7 These children placed on exodontia lists are a considerable financial burden costing taxpayers £30 million in 2012/13,8 with an average cost of £673 per child.9
In addition, dental treatment under general anaesthetic can be a distressing experience and, unfortunately, is accompanied in a healthy individual by approximately a 1:100,000 risk of suffering a life-threatening complication.10
Conscious sedation
Conscious sedation techniques aim to tackle dental anxiety by depressing the central nervous system with the administration of drugs. However, this differs from a general anaesthetic as verbal contact is maintained during treatment and a significant margin of safety exists to prevent the loss of consciousness.11
Oral pre-medication and sedation
Oral pre-medication can involve a small dose of oral sedative to help relieve anxiety prior to a dental visit. This is not routinely prescribed in children as its effects are unpredictable and cannot be titrated. Side-effects, such as nausea, vomiting, behavioural disinhibition and, in severe cases, respiratory depression and arrest may occur.12 However, a pre-operative sedative is sometimes warranted to facilitate the induction process by allowing cannulation and reducing the need for physical intervention.13
Inhalation sedation
Nitrous oxide is frequently employed in paediatric dentistry to alleviate anxiety. A titrated mix of nitrous oxide in oxygen delivered via a nasal hood has been reported to aid in undertaking dental treatment successfully by its ability to depress a patient's gag reflex and facilitate prolonged treatment.14 Nitrous oxide may be favoured over general anaesthesia in medically compromised children as it is not metabolized and therefore has a fast onset, quick recovery and, most importantly, is generally safe to use in this cohort.15 On the other hand, it is not generally available in primary dental care. Expensive equipment, maintenance costs and additional staff training,16 without the incentive to be financially compensated under the current NHS contract, deter general dental practitioners from its use.
Intravenous sedation
In complex cases where inhalation sedation is not suitable, intravenous sedation is a viable alternative method of facilitating behaviour management. It can also be utilized in situations where a general anaesthetic cannot be justified, such as the elective extractions of healthy teeth for orthodontic reasons.17 This technique is only indicated in young people over 12 years old. In a primary care setting, the use of a single drug administered intravenously is advised.18 However, it is not routinely available outside a hospital setting due to specific training requirements of teams, risks of administering midazolam or propofol, and the perceived difficulty of cannulation in children.19 These requirements call for the need of a specialist/consultant in paediatric dentistry and a consultant in anaesthesia competent in sedation for dentistry for assessment and treatment in a facility equivalent to an NHS Acute Trust in England.18
Non-pharmacological techniques
Children acquire strategies to aid in coping with new situations and experiences when growing up. Attending the dentist can be a daunting and difficult experience in which these coping strategies are not sufficient.20 A non-pharmacological approach employed by the dental team can acclimatize the patient and tailor the dentist–patient interaction to gain compliance and relieve anxiety. A wide range of practices are available in managing poor behaviour. The use of multiple approaches personalized to an individual child is recommended in order to reinforce good behaviour and build rapport.21
Voice control
This technique aims to influence a patient's co-operation by the alteration of voice volume and rate of speech. It has proved useful in poorly attentive children as authority can be established simply, therefore resulting in improved co-operation. It is also successful in reducing disruptive behaviour without producing long-term negative effects.22
Tell-show-do
This simple method is routinely utilized by the dental team to familiarize children with dental procedures quickly.23 It involves: Tell – an explanation which is age appropriate to the patient;
Show – demonstrating the procedure or equipment; and
It has been demonstrated to reduce anxiety significantly in paediatric patients and speed up the acclimatization process.25
Positive reinforcement
This approach consists of improving compliance by rewarding the child to reinforce desired behaviours and treatment outcomes. Pleasing items such as stickers, toys and badges can be utilized to reinforce good habits in a dental setting.26 However, praise through non-verbal communication and tone of voice can have a substantial impact on the behaviour-shaping process.27
Modelling
The influence of a family member, friend or peer should not be underestimated in order to improve the co-operation of a child. An older family member exhibiting appropriate behaviour in the dental chair can be beneficial in reducing dental fear and promote appropriate conduct.28 Studies have demonstrated that live model filming and videos can also encourage good conduct. To be effective, it must display a similar age of the child to be targeted with praise of the required behaviour (Figure 1).29
Figure 1. Modelling can also involve a soft toy to demonstrate dental treatment and improve patient compliance.
Systematic desensitization
This process aims to aid a child in overcoming a specific fear via repeated contacts and a gradual increase in stimulus. Relaxation techniques are integrated into the desensitization sessions in children that can identify their fear and communicate it verbally.30
Distraction
This technique aims to shift children's attention away from unpleasant stimuli, thereby reducing disruptive behaviour. Examples of these include stretching the lip when administering local anaesthetic and asking patients to ‘wiggle’ their feet when taking impressions or radiographs. Verbal distraction throughout the appointment can permit treatment to be carried out without children reacting to the known stimulus.31 Audio distraction has also been proposed and, although proven successful in adults, it has had inconsistent results in managing a child's dental anxiety.32
Research in audio-visual distraction
The medical field was the first to introduce audio-visual distraction to undertake treatment on children suffering from burn injuries.33 These patients are a difficult group to manage owing to their need for multiple dressing changes that are painful and can cause behavioural distress.34 Potent pharmacological analgesic intervention is insufficient due to physiological tolerance of, and dependence on, opioid medication.35 In this cohort of children, studies have shown that audio-visual distraction consisting of video games36 and virtual reality37 can supplement pharmacological behaviour management techniques successfully. In regards to dentistry, this behaviour management technique has increased in popularity in recent years. As a result of its simplicity, further research has been undertaken into its application for dental patients. It has been stated that there can be a significant improvement in behaviour during dental treatment. However, pain and physiological measurements are unaffected by this treatment modality.38 When assessing the success of different non-pharmacological behaviour management techniques, audio-visual distraction is more effective in alleviating paediatric dental anxiety compared to audio distraction alone.39
Video glasses in dentistry
Several technological methods have been introduced in the dental setting to improve a child's behaviour. Audio-visual distraction in the form of television, video games and virtual reality have been utilized. These devices have several disadvantages when applied to dentistry which include:
Occupying space;
Distracting the dental team;
Producing unpredictable reactions from the child; and
Video glasses are a simple and immersive audio-visual distraction tool that seems to overcome the limitations that exist with alternative technological devices. They consist of glasses with incorporated twin high resolution LCD displays which cover the full field of vision and in which sound is provided through headphones. The video glasses can be easily connected to an output device in order to allow for patient choice of a wide range of videos (Figure 2). However, there are limitations to video glasses. Some models may not provide sufficient eye protection and it is contra-indicated in children that suffer from epilepsy elicited by flashing images.
Figure 2. Vuzix® WrapTM 1200DX video glasses with light shield, input device and disposable headphones.
There is limited evidence available to support the use of video glasses, however, small studies have suggested that they may be effective in supporting the administration of local anaesthesia41 and undertaking restorative treatment in children.42
In comparison to pharmacological behaviour techniques, the use of video glasses has shown early promise. No paediatric studies have been undertaken however, in an adult randomized control trial, there was no significant difference between inhalation sedation and video glasses in its effect on perceived pain in patients diagnosed with chronic periodontitis undergoing periodontal therapy.43 It has been proposed that video glasses can be used as an adjunct to relative analgesia.44 Nonetheless, caution is advised owing to the loss of eye and verbal contact during treatment under conscious sedation.
Clinical application of video glasses
In the experience of the authors, there are several clinical scenarios in which video glasses are invaluable in the management of phobic children and allow treatment to be completed without impacting negatively on their compliance.
Patients with Autistic Spectrum Disorder (ASD)
Introducing conventional behaviour management techniques in this group of children can be complicated owing to their lack of understanding, communication difficulties and apprehension in accepting an invasion of their personal space.45 Distraction techniques can overwhelm these children due to sensory issues regarding tactile and auditory stimulus. Although this is true, autistic spectrum disorder children spend significantly more time watching television and playing video games compared to siblings.46 Taking advantage of their compulsive behaviour can be the breakthrough needed to initiate dental treatment (Figure 3).
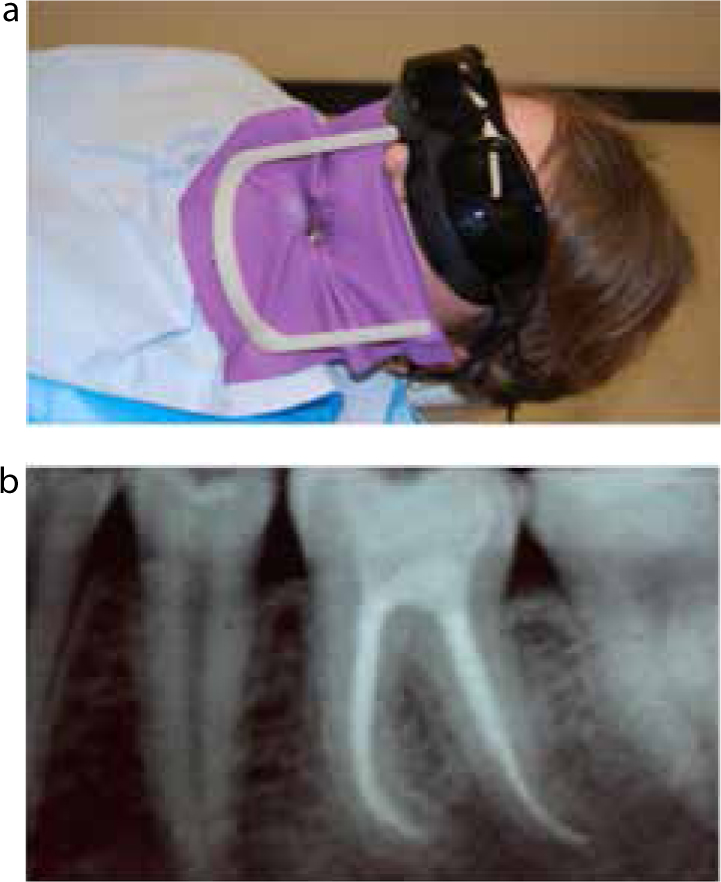
Figure 3.
(a, b) 15-year-old with Asperger's syndrome requiring molar endodontic therapy of the LL6.
Young children
This age group may struggle to receive high quality dental care owing to their short attention spans and inability to tolerate lengthy treatment appointments. Furthermore, parents may be reluctant to consent to treatment under general anaesthesia because of the risks of this procedure and the frequent need to extract all carious primary teeth in order to prevent a repeat general anaesthetic (Figure 4).
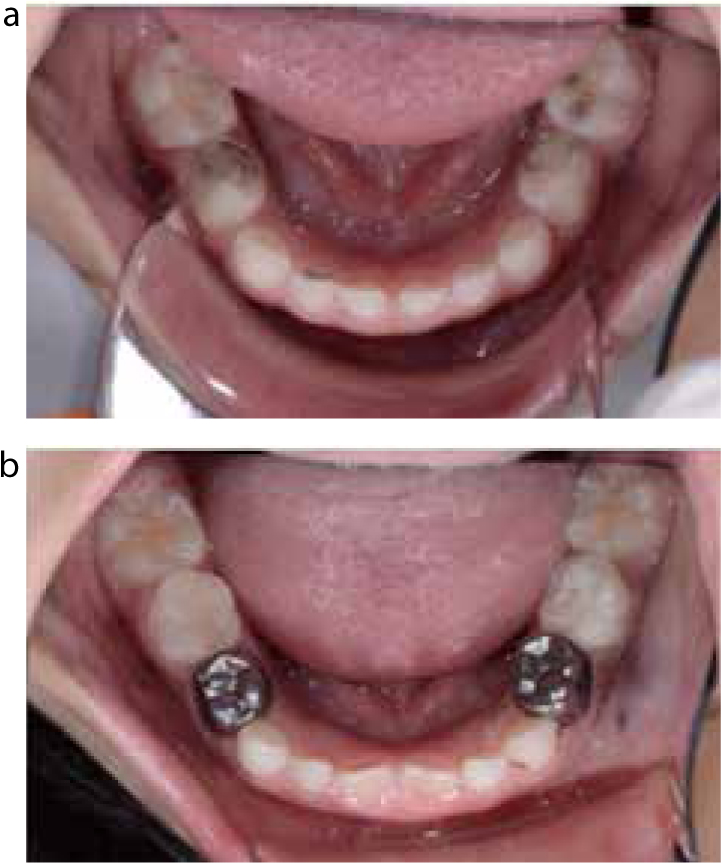
Figure 4.
(a, b) A 5-year-old girl managed by video glasses to undertake pulpal therapy and placement of preformed metal crowns.
Management of dental trauma
A traumatic injury to the incisal teeth can be a harrowing experience for both child and parent. It also may be his/her first experience of receiving invasive dental treatment. Providing timely, appropriate dental care and ensuring that it is a positive experience is paramount to safeguarding the prognosis of injured teeth. Further appointments are always necessary which may also include orthodontic, restorative and surgical treatment. Video glasses have the potential to distract the child sufficiently in order to complete complex therapy (Figure 5).
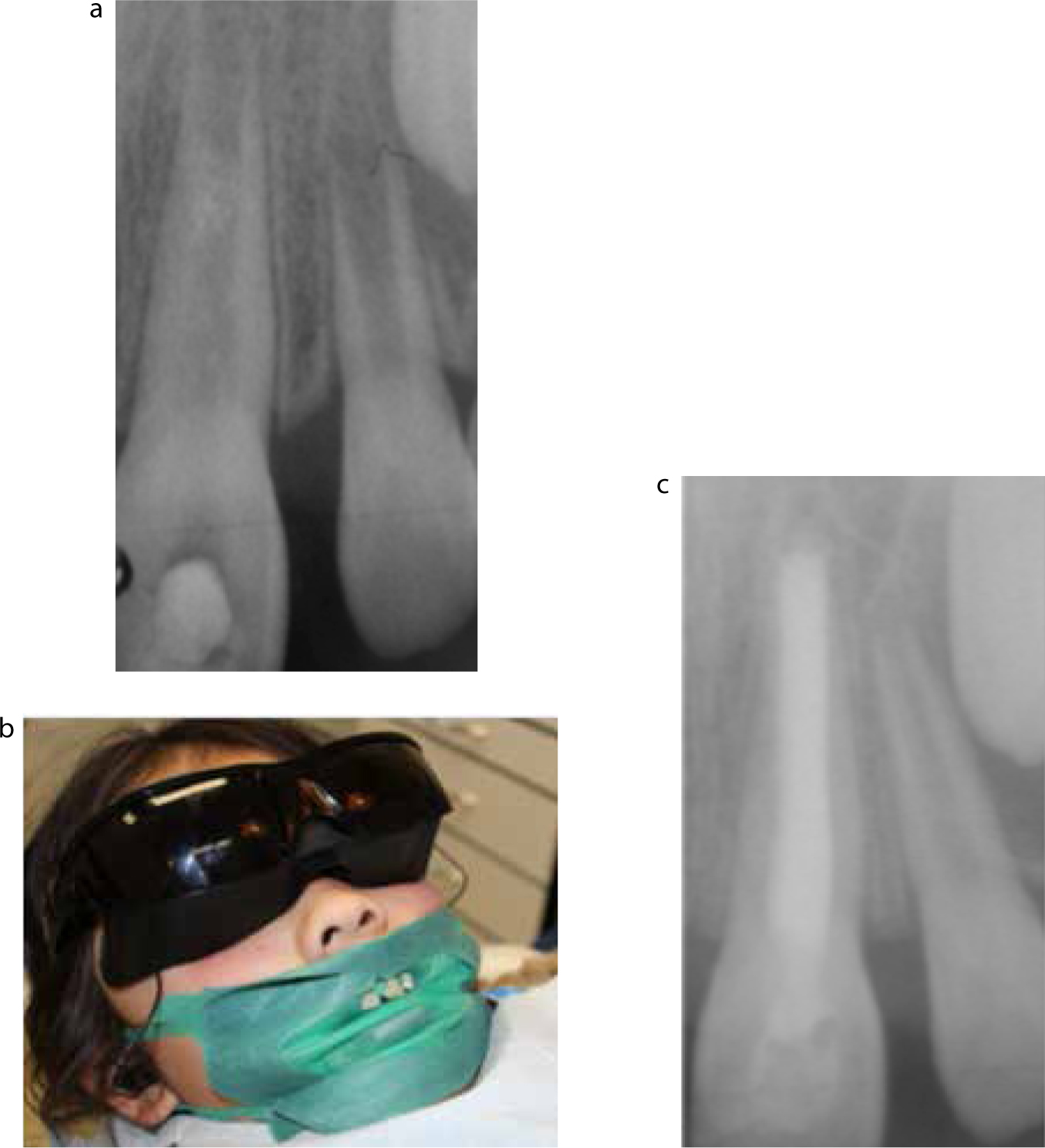
Figure 5.
(a–c) An 8-year-old girl with an enamel-dentine fracture and loss of vitality of the UL1. Apexification was achieved using Mineral Trioxide Aggregate (MTA) and obturated with gutta-percha.
An alternative technique to inhalation sedation?
Video glasses have the potential to be an effective substitute for inhalation sedation in children where it is unavailable, compliance is insufficient or where it is medically contra-indicated. Inhalation sedation is not advisable in children that are mouth breathers, have blocked noses, suffer from chronic respiratory disease and have had a medical procedure involving utilization of intracranial gases.47 Inhalation sedation can impair access to the anterior maxillary region due to the nasal hood that delivers the gas. Video glasses do not impede access to the anterior region in children who require behavioural support to improve compliance (Figure 6).
Figure 6. A 5-year-old girl showing the restriction of access to the anterior maxilla via the nasal hood, which is not a concern when utilizing video glasses.
Conclusion
In the last decade, video glasses technology has evolved to deliver a more immersive entertainment experience by improving the user interface and quality of the audio-visual reproduction. Video glasses are a novel and possibly cost-effective tool in dentistry that can aid in overcoming barriers to help nervous patients accept dental treatment. There is a paucity of data for this treatment modality in the literature. Despite the plethora of non-pharmacological behaviour management techniques available, video glasses stand out as a potential way of effectively supporting paediatric patients and allowing the successful delivery of their care.
Declarations
The authors declare no conflict of interest or any support from the manufacturers of the video glasses.