Masood M, Masood Y, Newton TJ Methods of qualitative research in dentistry: a review. Dent Update. 2010; 37:326-336
Fardal Ø Research in a dental practice setting. Dent Update. 2004; 31:423-430
GDC. 2015.
American Dental Association. 2013.
Dawes M, Summerskill W, Glasziou P Sicily statement on evidence-based practice. BMC Med Educ. 2005; 5
Cochrane Collaboration. 2015.
Gibson CJ Critical appraisal: a template to evaluate scientific literature. Dent Update. 2008; 35:414-417
Bateman G, Burke FJT, Saha S A guide to the appraisal of research: 1. the nature of research. Dent Update. 2009; 36:495-501
Maudsley G, Strivens J ‘Science’, ‘critical thinking’ and ‘competence’ for Tomorrow's Doctors. A review of terms and concepts. Med Educ. 2000; 34:53-60
Lodi G, Figini L, Sardella A, Carrassi A, Del FM, Furness S Antibiotics to prevent complications following tooth extractions. Cochrane Database Syst Rev. 2012;
Rasines AM, Veitz-Keenan A, Sahrmann P, Schmidlin P, Davis D, Iheozor-Ejiofor Z Tooth-colored resin fillings compared with amalgam fillings for permanent teeth at the back of the mouth. Cochrane Database Syst Rev. 2014;
Burke FJT, Mackenzie L, Sands P Dental materials – what goes where? Class I and II cavities. Dent Update. 2013; 40:260-274
‘Half of eight-year-olds have tooth decay’. 2015.
If your child has tooth decay, you must be a terrible parent. 2015.
Public Health England. Delivering better oral health: an evidence-based toolkit for prevention. 2014.
Marinho VCC, Worthington HV, Walsh T, Chong L Fluoride gels for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2015;
Yaacob M, Worthington HV, Deacon SA Powered versus manual toothbrushing for oral health. Cochrane Database Syst Rev. 2014;
Chapple I, Gilbert ABerlin: Quintessenz Verlag; 2010
Smith GCS, Pell JP Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials. Br Med J. 2003; 327:(7429)1459-1461
Carlsson G Some dogmas related to prosthodontics, temporomandibular disorders and occlusion. Acta Odontol Scand. 2010; 68:313-322
Kanno T, Carlsson G A review of the shortened dental arch concept focusing on the work by the Käyser/Nijmegen group. J Oral Rehabil. 2006; 33:850-862
Witter DJ, Creugers NH The shortened dental arch concept and its implications for oral health care. Community Dent Oral Epidemiol. 1999; 27:249-258
Balas EA Information systems can prevent errors and improve quality. J Am Med Inform Assoc. 2001; 8:398-399
Spallek H, Song M, Polk D Barriers to implementing evidence-based clinical guidelines: a survey of early adopters. J Evid Based Dent Pract. 2010; 10:195-206
Philstrom BL, Barnett ML Design, operation and interpretation of clinical trials. J Dent Res. 2010; 89:759-772
This article informs readers of a method of implementing evidence-based dentistry in practice. Following these steps, practitioners should be able to use this skill in an efficient manner. The importance of evidence-based dentistry and its relevance to situations encountered in everyday practice is also highlighted.
CPD/Clinical Relevance: This article highlights a series of steps to be followed by practitioners to ensure that treatment provided is supported by the most recent, good quality evidence.
Article
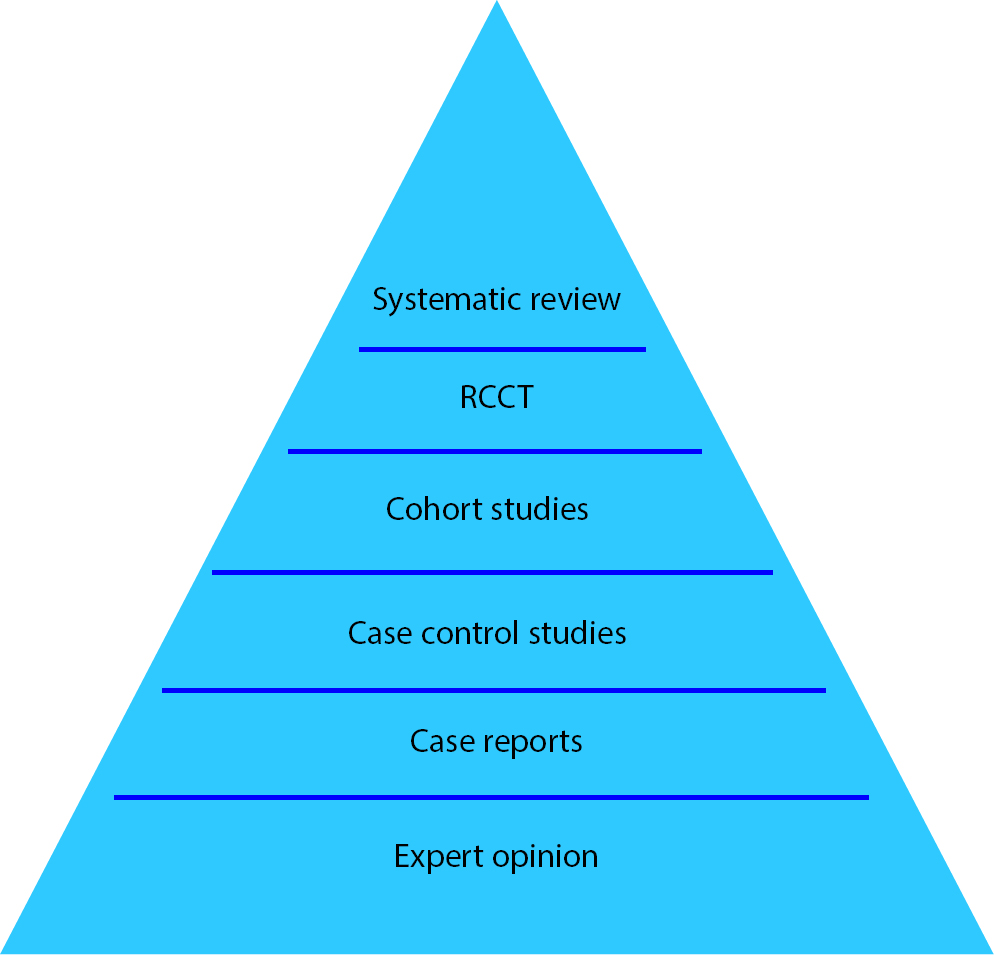
The dental community requires good quality, evidence-based research in order to enable patients to receive the best possible care available. In this regard, research methodology may either be quantitative or qualitative in its approach.1 Quantitative-based examples include durability of restorations or the effect of interventions on the success of clinical treatments. The other style of research is qualitative, which aims to interpret, measure and enumerate trends.1 There is a hierarchy of articles ranging from case reports and review articles up to the ideal study, which is a randomized controlled clinical trial (RCCT).2 A systematic review is where the authors review, in a structured way, a series of RCCTs on a similar topic, while a meta-analysis undertakes analysis of common data on a subject. The hierarchy of clinical findings is often displayed as a pyramid where the base is made up of the lowest form of evidence and the tip displays the highest form of research (Figure 1).2
Figure 1. Hierarchy of articles.
Clinical cases and cohort studies may be well received by practitioners owing to their interest level and the straightforward nature of the report. A report of a randomized clinical trial or a meta-analysis review is more demanding to read and assimilate. These reports often contain a plain English or bottom line conclusion to assist the busy practitioner in obtaining the information in a timely manner. It is the responsibility of the dental practitioner to keep up-to-date with advances in the literature and to use this information to improve the quality of care of their patients. The use of evidence will assist in the most up-to-date treatments being used.
This article aims to guide clinicians on how to go about implementing evidence-based practice with their patients. Case studies are used to demonstrate how to implement evidence-based dentistry (EBD) in everyday practice.
Current knowledge on evidence-based dentistry (EBD)
The general dental council (GDC) expects that registrants are able to:
‘…explain, evaluate and apply the principles of an evidence based approach to learning, clinical and professional practice and decision making.’
However, there may be confusion about what constitutes EBD.3 There is the temptation to believe that simply reading journal articles counts towards practising EBD when, in reality, it is more complex than this. The American Dental Association defines evidence-based dentistry as:
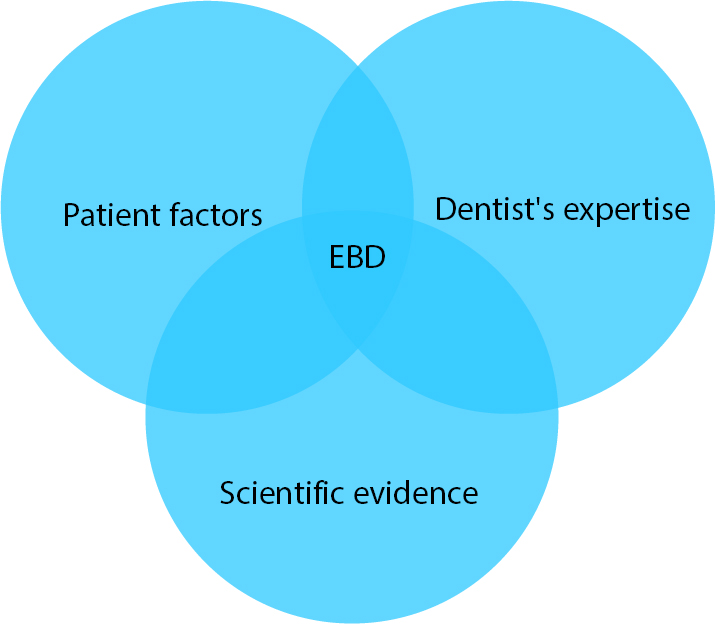
‘…an approach to oral health care that requires the judicious integration of systematic assessments of clinically relevant scientific evidence, relating to the patient’s oral and medical condition and history, with the dentist's clinical expertise and the patient's treatment needs and preferences.'4
The three key points from this definition are the use of scientific evidence, the clinician's expertise and the patient's needs and preferences (Figure 2).4 Therefore, there are steps that have to be taken by the clinician after gaining information to be able to carry out an evidence-based approach to professional practice (Figure 3). In this regard, much published work on evidence-based dentistry has focused on how to appraise literature critically and less on how the knowledge gained should be utilized by the dental professional.
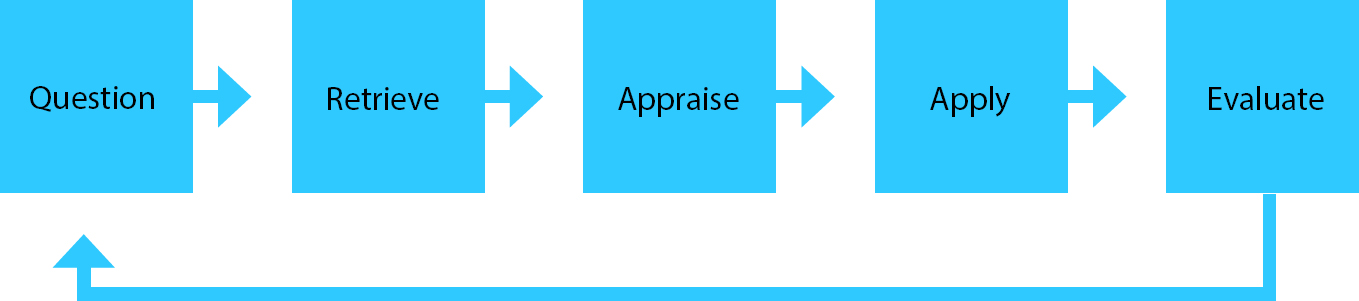
Figure 2. The constituents of evidence-based dentistry.Figure 3. The steps taken to implement evidence-based dentistry in practice.
There are five steps that the clinician should consider when reviewing a clinical intervention:5
Question: form a question that needs to be answered that is based on the patient's problem.
Retrieve: access available evidence.
Appraise: critically appraise the information accessed.
Apply: use the results found and act on them to provide treatment in practice.
Evaluate: assess performance.
The case studies discussed in this paper have used information retrieved from the Cochrane Library. The Cochrane Collaboration is an international organization involved in providing healthcare information, often in the form of reviews of RCCTs.6 Many leading members of the dental profession are involved in carrying out the research and reviews in order to provide accessible evidence that has minimal bias, is relevant and is of a high quality.6 The Cochrane Library was used to obtain information for the case studies in this paper as healthcare professionals are able to access the library easily. Not only this, but the systematic reviews used in the case studies are reviews of RCCTs, which is the ideal type of study to be using in EBD.
From the framework above, Step 3, critical appraisal, requires the clinician to assess the truth, validity and probability of the study to ensure that it is applicable to the clinical situation.7 Carrying out this step allows the clinician to have confidence when carrying out a treatment plan that relies on research findings. There is a vast array of literature dedicated to instructing clinicians on how to carry out a critical appraisal and the reader is referred to these.7,8 Systematic reviews will have carried out a critical appraisal on the studies included and usually provide a statement on the quality of evidence provided by the research findings.
Step 4 requires the clinician to carry out critical thinking: this involves using the information deemed to be suitable from Step 3.9 It is here that the clinician assesses possible outcomes from implementing treatment proposed in relation to the patient's desires and individual medical, social and dental history.9 The clinician must also use his/her own experience in treating past cases to provide a final list of treatment options to the patient.9 Ultimately, the patient makes the final treatment decision but, by using this framework, dental professionals can ensure that patients will be provided with treatment options based on sound evidence.
EBD case study – prescribing antibiotics post extraction
A clinician considering preventing post-operative complications following tooth extraction by prescribing antibiotics may use the steps above to help reach a decision on how best to manage patients (Figure 4).10 The question to be answered would be: ‘are antibiotics effective in preventing complications following tooth extraction?'10 Using the Cochrane Library, a systematic review on this topic was located which states that the risk of infection following extraction of a wisdom tooth in a healthy young individual is 10%, but rises to 25% in patients who are sick or immunocompromised.10 Overall, on average, it was found that 12 people would have to be treated with antibiotics to prevent one infection and 38 people would need to be treated with antibiotics to prevent one case of dry socket.10 Against this, for every 21 people treated with antibiotics, an adverse effect was likely and this was more likely than for patients who were not given antibiotics.10 Step 3 requires the clinician to appraise the evidence: 18 studies were used with a total of 2456 participants.10 The participants were either given antibiotics or a placebo post extraction, all of which were carried out by oral surgeons.10 However, many of the studies were shown to have poor design and reporting and 13 of the 18 studied were assessed to have high bias.10 The results indicate that, for a healthy patient, the benefits of prescribing antibiotics do not outweigh the drawbacks but, at Step 4, the clinician also needs to think more broadly; what are the wider implications of carrying out this treatment? This would allow the clinician to realize that there is also the conflicting interest of bacterial resistance being created by widespread antibiotic usage.10 It is the responsibility of clinicians to reflect on their previous experience of patients attending with post-operative infection or dry socket: how many patients did this affect? How was the infection subsequently resolved? Only then will clinicians be able to make decisions about whether the benefits of avoiding infection in patients outweighs the risk of antibacterial resistance.10 The subsequent treatment is carried out and the clinician is expected to evaluate his/her decision and use this to help influence future treatment decisions.
Figure 4. Antibiotics may be prescribed to patients post extraction to prevent post-operative complications.
EBD case study – tooth-coloured filling vs amalgam restorations in posterior teeth
A decision often facing a dentist in general practice is whether to use composite resin or amalgam restorations in posterior teeth. Following the framework above, the question to be answered would be ‘should composite resin or amalgam be used to carry out a restoration in the posterior tooth?' A literature search reveals a Cochrane Oral Health Group review.11 In this analysis, seven RCCTs met the criteria for the review and these were selected for use.11 It may be argued however that, although thousands of papers on posterior composites did not meet the strict criteria for inclusion in this review, they may well have contained important information that would be of use. Not only this, but two of the RCCTs included restorations placed in children and, although important, this is not the group in which the majority of restorations are placed.11 The rapid development of dental materials such as composites often does not provide sufficient time for their clinical use to be fully evaluated. This is also demonstrated in the Cochrane review. Five of the RCCTs were published before 1990 and, even though the results suggest that amalgam restorations had lower failure rates than resin, resin-based materials are continuously evolving and there is evidence to show that the physical properties of composites have improved.11,12 In this case, using the Cochrane review in isolation could lead the clinician to overlook the advances that have been made in resin materials and this highlights a major shortcoming of the Cochrane review: only RCCTs are used, while the majority of clinical studies in dentistry are cohort studies.
Other factors unrelated to the study design would have to be taken into consideration in order for the clinician to be carrying out EBD. Factors such as: the size of the cavity, the surface to be filled, and other restorations placed in the tooth would also have to be considered. The patient's medical history would have to be checked to ensure that they have no allergies to the metals contained in the amalgam mixture intended to be used. Not only this, the patient's preferences would also have to be taken into consideration.
EBD case study – preventing tooth decay in children and adolescents using fluoride gels
Caries in primary teeth is a topic that has recently generated much media interest.13,14 A common method of preventing caries is by the use of topical fluoride applied to the surfaces of teeth.15 The use of fluoride in the water supply has received a great deal of negative press and so clinicians are expected to answer questions from concerned parents about the safety of fluoride in order to gain informed consent. If a child attends the clinic and is assessed to be at high risk of caries, the dentist may propose the application of topical fluoride on the surfaces of the dentition (Figure 5). In the scenario above, the parent or carer may be worried about the possible toxic effects of fluoride. Their question highlights a Cochrane review comparing the use of fluoride gels in children and adolescents compared to the use of a placebo or no treatment in preventing caries.16 Step 3, appraisal of the review, shows that over 28 studies are included and over 9000 children were treated.16 The studies ran from 1 to 4 years and took place in various cities around the world.16 Importantly, the quality of the evidence was deemed to be ‘low’ for the deciduous dentition and ‘very low quality’ for the evidence on the adverse effects.16 On the other hand, the evidence for the permanent dentition was assessed to be of moderate quality.16
Figure 5. A typical set-up of the materials needed to apply fluoride varnish.
The results showed that, on average, there was a 28% reduction in decayed, missing or filled permanent teeth and a 20% reduction in decayed, missing and filled deciduous teeth.16 The review found little evidence on the negative effects from topical fluoride gel administration and further research was suggested in this area, especially as children often swallow the gel.16 At Stage 4, applying the information gained, the clinician would need to assess the patient's compliance: what is the likelihood of the patient swallowing the fluoride gel? If there is a high chance, what alternatives can be offered? Each patient will have a different tolerance but all parents and carers should be given the same information with regards to possible toxic effects. It is the duty of the clinician to relay up-to-date information to patients; inevitably further research will always be needed in certain areas but the clinician providing treatment must utilize current knowledge until further information is gained. As in the previous scenarios, once treatment has been provided the outcome must be evaluated; was the majority of the gel swallowed? At recall appointments, how many new cavities have been formed? Reflecting on these outcomes will help inform future treatment of similar situations.
EBD case study – powered vs manual toothbrushing for oral health
Delivering oral hygiene instruction often raises the question of whether an electric toothbrush is more effective in removing plaque compared to a manual toothbrush. This is often an important discussion for patients as the information determines whether they invest in a new toothbrush. The question often proposed by patients being: ‘is a powered toothbrush more effective than a manual toothbrush?' A literature search would reveal a systematic review carried out by the Cochrane Oral Health Group on this topic.17 The review involved both adults and children. However, the studies were short term, lasting at least 4 weeks.17 Overall, 56 trials met the inclusion criteria but were at varying degrees of bias.17 The information was assessed to be of moderate quality and the review found that powered toothbrushes provide a statistically significant reduction of plaque in both short and long term.17 This was quantified by suggesting that this equated to a 6% decrease in gingivitis with the Löe index and a 11% reduction in the Silness index.17 It is important to note, however, that periodontal disease is multifactorial and patients differ in their susceptibility to it.18 This means that the reduction in plaque may have a greater importance to a patient who has a predisposing factor to the disease, such as diabetes, again highlighting the importance of taking the patient's medical history into account.18 Delivering this information alone may persuade some to invest in a powered toothbrush, while others may prefer to try other techniques to improve their oral hygiene. It is the responsibility of clinicians to determine what type of toothbrush patients use and if they are using any adjuncts to improve their oral hygiene. They can then advise patients on how they can improve but the ultimate decision to buy any new products or change their frequency of brushing is up to the patient. Upon review, clinicians would be able to determine if there has been an improvement in oral hygiene and whether, for the patients who decided not to invest in a powered toothbrush, other adjuncts are just as successful. For patients who did invest in a powered toothbrush, clinicians may be interested to know how quickly they adapted to using it and if this varies with patient age. This could then influence the advice that clinicians deliver to other patients. The review highlighted that, although powered toothbrushes were used, there was variation in the type of movements they carried out. This is an area that requires further investigation to determine the most effective type of movement for removal of plaque which can then be used to help patients improve their oral hygiene.
Discussion
Evidence-based practice can be implemented by following the 5 Steps outlined previously. Clinicians are to use their own expertise and experience to help inform their decisions to help provide the best treatment for their patients. The vast array of research being carried out in any one specialty may be overwhelming and there is the temptation to rely on one source of evidence, for example; the Cochrane Collaboration. However, as the resin vs amalgam case study illustrated, the strict regulations ensuring that only RCCTs are included in the review leave us at risk of missing important information that other studies, such as cohort studies, show. In reality, there are very few RCCTs in dentistry owing to the time and cost involved. This means that systematic reviews carried out are on the small number of RCCTs produced. Cohort studies, comprising the majority of clinical survival studies, are rejected as they may show both selection and reporting bias.19 The exclusion of cohort studies in systematic reviews can result in many important findings not being relayed to clinicians, giving a skewed image of results. Randomized controlled clinical trials are the highest form of evidence but there are other important studies that will inform the clinician and, if interpreted with care, add to the knowledge base.
Using research to inform treatment planning can seem daunting for clinicians who have used alternative techniques that have worked adequately throughout their careers. In dentistry, many procedures are accepted and carried out on patients without having a strong evidence base. It has been suggested that these procedures should be called ‘dogmas’ as they are based on beliefs that are accepted as being true even when this has not been supported by evidence.20 Once formed, dogmas can allow clinicians to fall into the routine of carrying out and accepting procedures as a ‘gold standard’ without questioning alternatives which may provide better outcomes for the patient.
One example of how a dogma has been challenged is the concept of the shortened dental arch.21 A literature review demonstrates that a shortened dental arch ‘comprising anterior and premolar teeth in general fulfil the requirements of a functional dentition’.21,22 It is now accepted that a shortened dental arch can provide a patient with a good quality of life and is generally adequate for function. Following the definition proposed by the American Dental Association for evidence-based dentistry, when the shortened dental arch is considered for a patient, the patient's functional needs and preferences must be taken into account and the patient must be informed of teeth that will not be replaced.5,21 Unfortunately, changes like this take time to be accepted in practice. One estimate indicates that it can take up to 17 years for research to take effect and be implemented in clinical practice.23 Not only this, but practitioners are faced with other barriers which prevent them from implementing evidence-based dentistry in their practices.24
Firstly, healthcare providers may be unable to access research that is of good quality and relevant to their particular case.24 This is especially true as RCCTs are difficult and costly to design and so it is unlikely that there will be one that caters to every clinical situation.25 Not only this, but the time taken to run RCCTs means that, by the time the results are produced, the materials or practices in question have already been superseded.
Furthermore, within each practice, practitioners may not feel confident carrying out an alternative procedure based on evidence if colleagues are not routinely carrying out EBD.24
Lastly, even with the best intentions on behalf of the dental professional, the final treatment decision is made by the patient. This is often influenced by cost and information gained from other sources, such as the internet.23
General dental practitioners may be reluctant to use evidence in their practices but the case studies provided show how evidence can be used to improve the quality of treatment given to patients. With the continued demand for good quality, relevant research will drive the focus of research projects to ensure that a constant flow of new evidence is accessible to practitioners. The challenge for the dental community will be deciding whether to base EBD on RCCTs only or by relying on a combination of RCCTs and clinical studies. The latter requires clinicians to be able to appraise each individual piece of literature independently. This is no easy task after a busy clinic and the need for this may be questioned, especially when it seems that existing practices are adequate.
Conclusion
Evidence-based dentistry can be implemented in an efficient manner but difficulties arise when deciding on the type of study required to confirm clinical findings. The randomized controlled trial will be the ‘gold standard’ but some clinical techniques may only be gold-plated when subjected to this form of evidence. There is a strong argument that, in everyday practice, cohort studies will provide relevant clinical information.