Thompson LDR Diagnostically challenging lesions in head and neck pathology. Eur Arch Otorhinolaryngol. 1997; 254:357-366
Non-Hodgkin lymphoma – Cancer Statistics Report. 2013;
Van der Waal RIF, Huijgens PC, van der Valk P, van der Waal I Characteristics of 40 primary extranodal non-Hodgkin lymphomas of the oral cavity in perspective of the new WHO classification and International Prognostic Index. Int J Oral Maxillofac Surg. 2005; 34:391-393
Painter D Research Fellow University of York. Personal communication. 2014;
Epstein JB, Epstein JD, Le ND, Gorsky M Characteristics of oral and paraoral malignant lymphoma: a population-based review of 361 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 92:519-525
Bacon CM Extranodal lymphomas. Diagnost Histopathol. 2009; 16:82-98
Herd MK, Woods M, Anand R, Brennan PA Lymphoma presenting in the neck: current concepts in diagnosis. Br J Oral Maxillofac Surg. 2012; 50:309-313
Wulfrank D, Speelman T, Pauwels C Extranodal non-Hodgkin's lymphoma of the head and neck. Radiother Oncol. 1987; 8:199-207
Mill WB, Lee FA, Franssila KO Radiation therapy treatment of Stage I and II extranodal non-Hodgkin's lymphoma of the head and neck. Cancer. 1980; 45:653-661
Parrington SJ, Punnia-Moorthy A Primary non-Hodgkin's lymphoma of the mandible presenting following tooth extraction. Br Dent J. 1999; 187:468-470
Wolvius EB, van der Walk P, van der Wal JE Primary extranodal non-Hodgkin lymphoma of the oral cavity. An analysis of 34 cases. Oral Oncol Eur J Cancer. 1994; 30:121-125
Pazoki A, Jansisyanont P, Ord RA Primary non-Hodgkin's lymphoma of the jaws: report of 4 cases and review of the literature. J Oral Maxillofac Surg. 2003; 61:112-117
Kolokotronis A, Konstantinou N, Christakis I Localised B-cell non-Hodgkin's lymphoma of the oral cavity and maxillofacial region: a clinical study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 99:303-310
Steinbacher DM, Dolan RW Isolated non-Hodgkin's lymphoma of the mandible. Oral Oncology. 2006; 42:187-189
Eideken-Monroe B, Eideken J, Kim EE Radiologic concepts of lymphoma of bone. Radiol Clin North Am. 1990; 28:841-864
Mohren M, Markman I, Jentsch-Ullrich K, Koenigsmann M, Lutze G, Franke A Increased risk of thromboembolism in patients with malignant lymphoma: a single-centre analysis. Br J Cancer. 2005; 92:1349-1351
Segawa Y, Yasumatsu R, Shiratsuchi H Inflammatory pseudotumour in the head and neck. Auris Nasus Larynx. 2014; 41:321-324
Primary extranodal non-hodgkin lymphoma in the infra-orbital region – a diagnostic challenge Naren Thanabalan Vinod Patel Chris Sproat Mark McGurk Dental Update 2024 43:9, 707-709.
Authors
NarenThanabalan
BDS, BSc, MJDF, GDP
Specialty Dentist in Oral Surgery, Oral Surgery Department, Floor 23, Guy's Dental Hospital, London Bridge, London (naren.thanabalan3@gmail.com)
Lymphomas within the head and neck region (HNR) are relatively uncommon; however, they can mimic common odontogenic conditions leading to diagnostic delays and subsequently the implementation of treatment. We report a case of a chronic infra-orbital swelling which, following excision, was diagnosed as an extranodal low grade Non-Hodgkin lymphoma. This paper explains the mode of presentation of extranodal lymphomas in the HNR, so that dental practitioners may consider it as a potential diagnosis when presented with a lump in the HNR.
CPD/Clinical Relevance: Extranodal lymphomas presenting within the head and neck region can have a multitude of clinical presentations, which may often resemble odontogenic conditions. This can cause confusion, resulting in diagnostic delays and treatment. This case highlights the importance of being aware of the features of extranodal lymphoma in the head and neck region, and the diagnostic challenges that may be encountered.
Article
There is a wide range of conditions that can present as a lump within the head and neck region (HNR), posing diagnostic challenges.1 Unusual signs and symptoms often result in a delay in diagnosis and treatment. The main challenge for the clinician is to distinguish sinister pathology from the benign by early recognition of the cardinal features of serious disease.
Lymphomas in the HNR are difficult to diagnose as they have varied patterns of presentation and are relatively uncommon. However, they should always be considered within the differential diagnosis of a lump in the HNR, as lymphoma is the sixth most common cancer in the UK, with 12,180 new cases diagnosed in 2010; a total of 4646 people having died from the disease in 2011.2
We describe a case of a primary extranodal Non-Hodgkin lymphoma (NHL) presenting as a localized infra-orbital swelling, including the investigations leading to diagnosis and treatment.
Case report
A 75-year-old female was referred by her general medical practitioner (GMP) to the Oral Surgery department in August 2012, with a unilateral swelling bounded by the lateral border of the nose and the infra-orbital margin on the left-hand side (Figure 1).
Figure 1. Left infra-orbital region larger in comparison to the right (arrowed).
The swelling had been present for approximately 8 months, slowly increasing in size and causing an occasional ache on pressure but no spontaneous pain. There had been no systemic symptoms, nasal or visual disturbances. The patient was a well-controlled hypertensive but otherwise healthy.
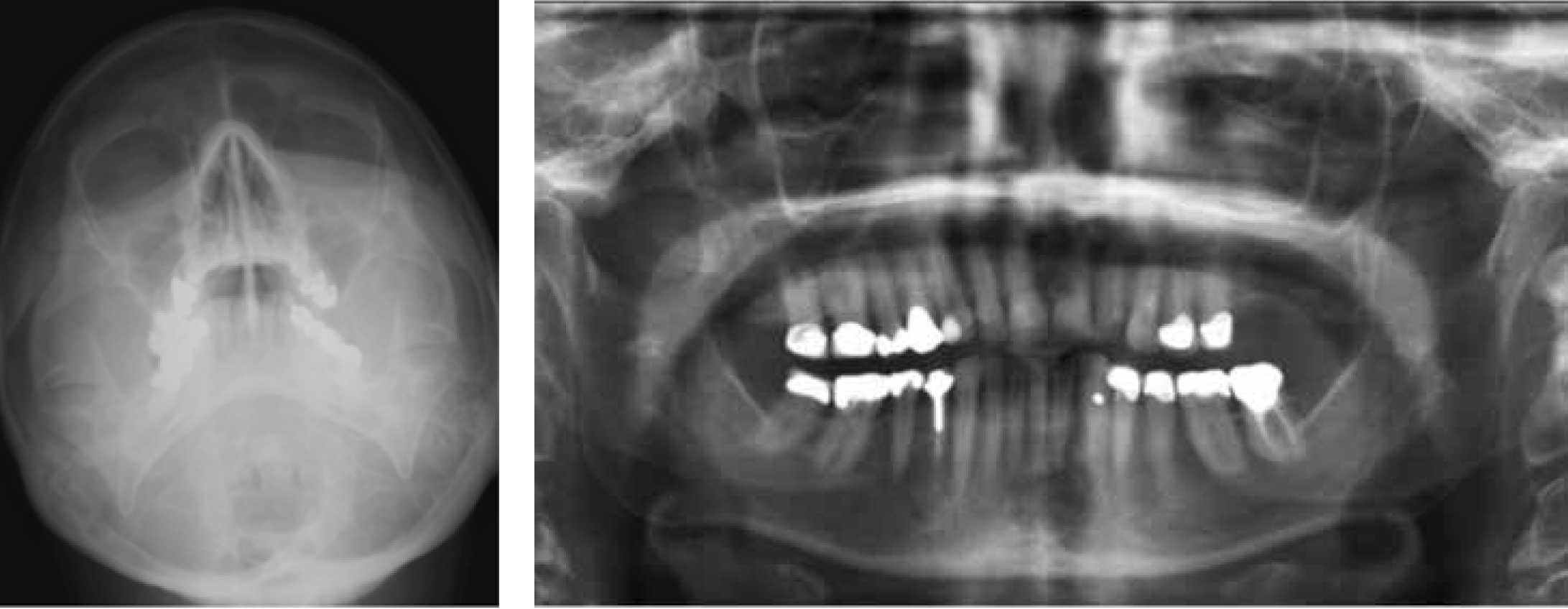
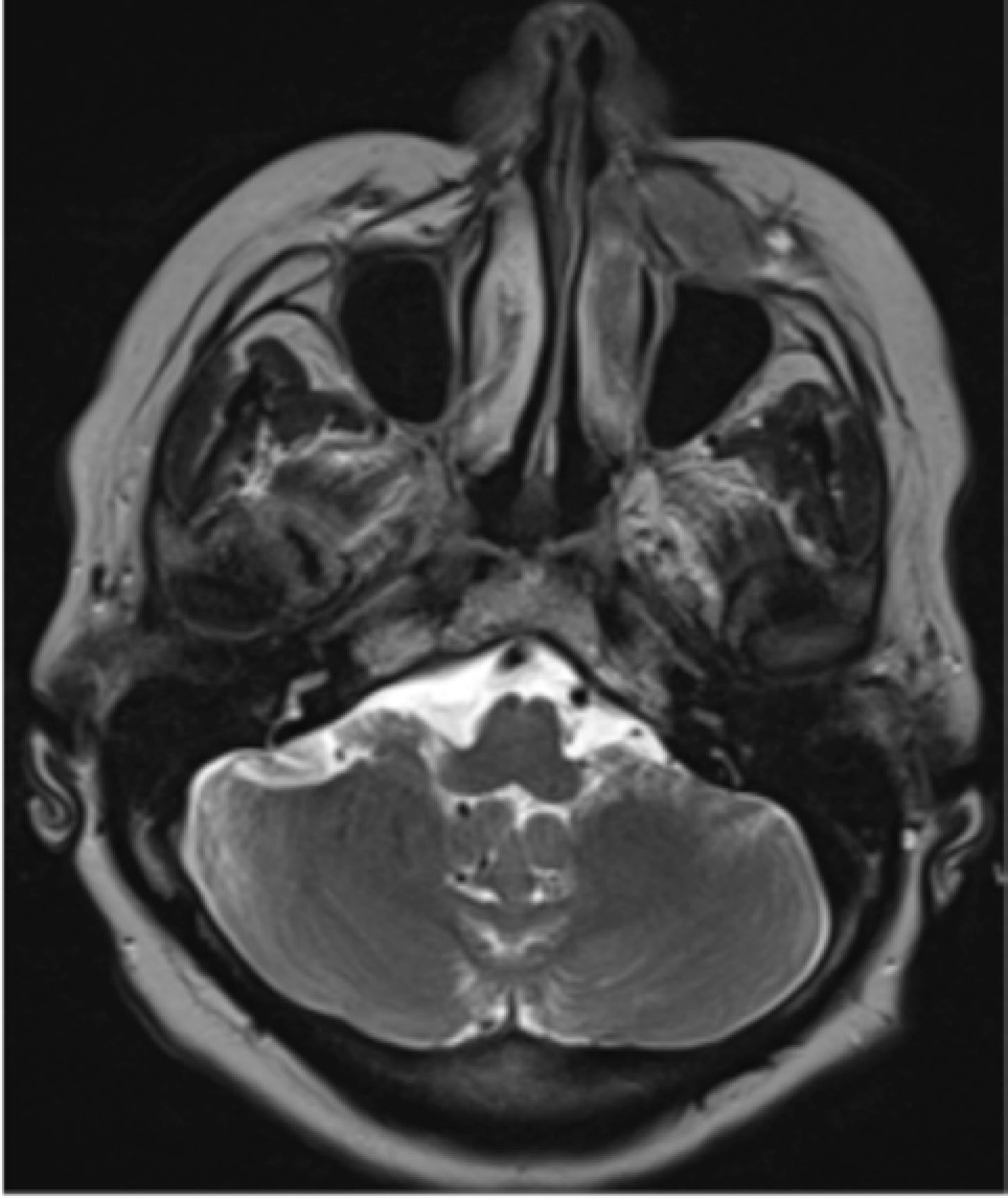
Clinical examination revealed a firm, fixed and non-tender 3x3 cm left-sided mass within the left cheek, with no associated lymphodenopathy or altered sensation related to the distribution of infra-orbital nerve. Panoramic and occipitomental plain radiographs (Figure 2) showed soft tissue swelling of the left cheek, but no evidence of bony destruction. An ultrasound scan undertaken at another hospital reported a 3 cm hypoechoic area of unknown origin. An MRI scan confirmed this and demonstrated erosion of the anterior maxillary wall (Figure 3).
Figure 2.
(a) Occiptomental view 30°. (b) Dental panoramic showing no obvious bone destruction in the left infra-orbital region.Figure 3. Axial section MRI scan showing left infra-orbital mass (solid white arrow) closely associated with the anterior wall of the antrum (dotted white arrow).
In light of the MRI report, the patient was referred to the Head and Neck Oncology Multidisciplinary team at the local hospital, and an incisional biopsy performed which was interpreted as an inflammatory pseudotumour (IPT). A PET/CT scan showed modest fluorodeoxyglucose (FDG) uptake in the soft tissue mass in keeping with inflammation rather than a tumour. Blood tests were unremarkable.
Following discussion at the multidisciplinary team meeting, the mass was surgically excised and further histological examination carried out. This revealed a Stage 1A, Grade 3A follicular lymphoma (a low grade NHL), for which the patient received adjuvant localized radiotherapy of 30 Grays (Gy).
Discussion
Lymphomas are broadly divided into Hodgkin (HL) and Non-Hodgkin (NHL) lymphomas, and are the third most common head and neck malignancy, after squamous cell carcinoma (SCC) and salivary gland tumours.3 The Haematological Malignancy Research Network (HMRN) estimates the annual incidence of NHL to be 10170 cases, with 32% in HNR, and HL to be 1120 cases, with 68% in the HNR.4 Within the HNR, lymphomas tend to present in one of two ways: most commonly as bulky, rubbery cervical lymphodenopathy with or without systemic symptoms (B symptoms). The B symptoms include night sweats, fever >38 °C and weight loss >10% body weight over 6 months, and are often associated with aggressive lymphomas.5 Alternatively, they can arise at extranodal sites, including the paranasal sinuses, salivary glands and oral cavity, either as primary or disseminated disease.6
Extranodal HL is uncommon (2–5%)7 and has two modal peaks of presentation in young adults (20–30 years) and the elderly (70–85 years).8 In contrast, 25% of NHL patients have extranodal disease, of which a disproportionate number manifest in the HNR (33%).9,10
Extranodal lymphomas of the HNR can present in a variety of clinical guises. Oral lymphomas can arise from the soft tissues or intra-osseously, and may be the first clinical sign of evolving disease in an otherwise asymptomatic patient.11 Intra-orally the common sites are the palate, vestibule and gingivae.11 The primary sign is a mass or swelling where the overlying mucosa may appear normal, ulcerated or have a red to blue discoloration.12 Lymphoma of the jaws is more prevalent in the maxilla than the mandible.13 The symptoms vary from pain, swelling, tooth mobility or resorption to parasthesia of local nerve roots.13,14,15 Gingival changes can masquerade as periodontal disease with marked erythema and hyperplasia,6 where the defining feature is the rapidly progressive nature. Radiographical features are not specific and may show localized alveolar bone loss, disappearance of the lamina dura or periradicular radiolucency.12,13 There may be buccal or lingual cortical destruction and widening of mental foramen or mandibular canal.15 Edeiken-Monroe et al16 estimated that 80% of bone lesions exhibit osteolytic erosive features and the remaining 20% show sclerotic or mixed radiographic appearances. Therefore, oral lymphomas can be reminiscent of common dento-alveolar conditions, such as periodontal or periradicular disease and osteomyelitis.12,16
Aggressive lymphomas can be identified more quickly due to their rapid progression in comparison to low grade types. Patients who have suffered an unexpected thrombo-embolic event may be investigated for occult causes at the treating hospital, as there is an increased incidence associated with higher grades of malignant lymphoma.17
The present case highlights the diagnostic dilemma posed when there is a discrepancy between the clinical and histological features. The histological diagnosis of IPT was accepted with caution owing to the clinical history and the knowledge that many lesions initially diagnosed as IPT can be reinterpreted as malignant.18 The differential diagnoses included lipoma, epidermoid cyst and low grade local dental infection. The clinical features of the soft tissue swelling were nondescriptive and difficult to interpret, although made an inflammatory cause unlikely. The cardinal clinical features in this case were bone erosion and the progressive nature of the mass, with unrelenting progression as the key feature.
Conclusion
Extranodal lymphomas have a variety of clinical presentations in the HNR, which can pose significant diagnostic challenges to both the referring general dentist and the hospital specialists. Lymphomas should be part of the differential diagnosis whenever investigating a mass in the head and neck. It is imperative for dental practitioners to be aware of the cardinal features of extranodal lymphomas in the HNR, to enable the identification of a lesion and refer for onward diagnosis and management.