Huber B [100 years of allergy: Clemens von Pirquet – his idea of allergy and its imminent concept of disease.]. Wien Klin Wochenschr. 2006; 118:(19–20)573-579
Munir Pirmohamed, James S, Meakin S Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients. BMJ. 2004; 329:(7456)15-19
Ellis AK, Day JH Diagnosis and management of anaphylaxis. Can Med Assoc J. 2003; 169:307-312
Egner W, Gawkrodger DJ The national survey of adverse reactions to dental materials in the UK: a preliminary study by the UK Adverse Reactions Reporting Project. Br Dent J. 2004; 196:471-477
Tichy M, Karlova I Allergic contact dermatitis and changes in the frequency of the causative allergens demonstrated with patch testing in 2008–2012. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2015; 159:480-488
Are metal fillings ruining our health?. Daily Mail.
Wrangsjö K, Swartling C, Meding B Occupational dermatitis in dental personnel: contact dermatitis with special reference to (meth) acrylates in 174 patients. Contact Dermatitis. 2001; 45:158-163
Nathanson D, Lockhart P Delayed extraoral hypersensitivity to dental composite material. Oral Surg Oral Med Oral Pathol. 1979; 47:329-333
Kanerva L, Turjanmaa K, Estlander T, Jolanki R Occupational allergic contact dermatitis caused by 2-hydroxyethyl methacrylate (2-HEMA) in a new dentin adhesive. Dermatitis. 1991; 2:(1)
Drucker AM, Pratt MD Acrylate contact allergy: patient characteristics and evaluation of screening allergens. Dermatitis. 2011; 22:98-101
Kanerva L, Jolanki R, Estlander T Allergic contact dermatitis from non-diglycidyl-ether-of-bisphenol-A epoxy resins. Contact Dermatitis. 1991; 24:293-300
Polydorou O, Trittler R, Hellwig E, Kümmerer K Elution of monomers from two conventional dental composite materials. Dent Mater. 2007; 23:1535-1541
Pulgar R, Olea-Serrano MF, Nivillo-Fertrelli A Determination of bisphenol A and related aromatic compounds released from bis-GMA-based composites and sealants by high performance liquid chromatography. Environ Health Perspect. 2000; 108:21-27
McGinley EL Summary of: Dental composite materials and renal function in children. Br Dent J. 2014; 216:80-81
Björkner B, Niklasson B, Persson K The sensitizing potential of di-(meth) acrylates based on bisphenol A or epoxy resin in the guinea pig. Contact Dermatitis. 1984; 10:286-304
Stanislawski L, Lefeuvre M, Bourd K TEGDMA-induced toxicity in human fibroblasts is associated with early and drastic glutathione depletion with subsequent production of oxygen reactive species. J Biomed Mater Res. 2003; 66:476-482
Stewart DE The changing faces of somatization. Psychosomatics. 1990; 31:153-158
Raja AS, Lindsell CJ, Bernstein JA The use of penicillin skin testing to assess the prevalence of penicillin allergy in an emergency department setting. Ann Emerg Med. 2009; 54:72-77
Mirakian R, Ewan PW, Durham SR BSACI guidelines for the management of drug allergy. Clin Exp Allergy. 2009; 39:43-61
Schmalz G Research Summary: Who is responsible for reporting adverse reactions?. Br Dent J. 2004; 196
Andreasson H, Boman A, Johnsson S On permeability of methyl methacrylate, 2-hydroxyethyl methacrylate and triethyleneglycol dimethacrylate through protective gloves in dentistry. Eur J Oral Sci. 2003; 111:529-535
Adverse reactions to dental materials are not an uncommon occurrence, although hypersensitivity has gained much renewed interest in light of public concerns over the safety of dental materials. Hypersensitivity can affect both patients and dental professionals and may manifest as either allergic contact dermatitis or stomatitis. Methacrylic monomers, such as MMA, EGDMA, TEGDMA and Bis-GMA, have been documented as causative allergens, however, little has been documented on the risk of such monomers in composites and bonding agents. The purpose of this article is to examine the current evidence and aspects of hypersensitivity to resin composites and bonding systems that are relevant within a dental setting.
CPD/Clinical Relevance: In the dental profession, dental materials have historically been documented as a cause of hypersensitivity. However, there remains little recent evidence on such reactions. The aims of this article are to highlight both the risk of hypersensitivity to dental composites and resin-bonding agents and the importance of reporting adverse reactions appropriately.
Article
The word ‘allergy’ was introduced by Clemens Von Pirquet in 1906,1 although the definition of this frequently used term remains inconsistent. The general consensus appears to define ‘allergy’ as an adverse hypersensitivity reaction mediated by immunological reactions that the body has to particular substances. The incidence of adverse drug reactions accounts for 6.5% of hospital admissions.2 Hypersensitivity reactions have been demonstrated to affect patient attitude towards treatment, quality of life and such adverse drug reactions are reported even to result in death in 0.15% cases.2
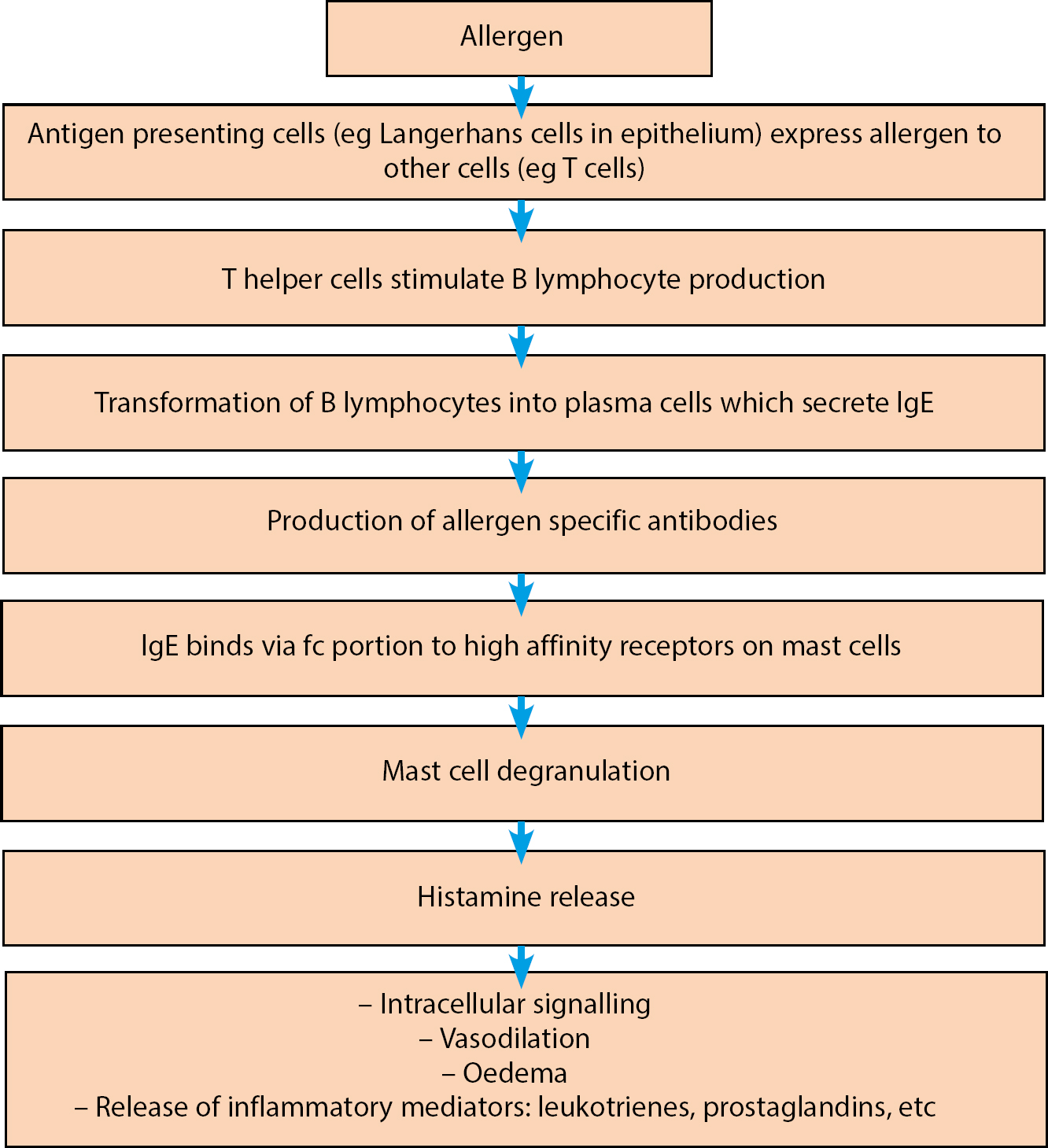
Figure 1 explains the immune response to an allergen. The body's immune response is complex and it is beyond the scope of this article to explain these in depth. The immune response is usually biphasic, with an early and late phase occurring in some cases.
Early phase: within 15 minutes, immediate response;
Late phase: 4–12 hours after exposure to allergen, delayed response.
Figure 1. Summary of immunological response to an allergen.
Anaphylaxis has been documented to occur between 5 minutes to 2 hours after exposure to an allergen. However, the second phase may occur after an asymptomatic period of up to 8 hours.3
In summary, an allergy is a type of hypersensitivity reaction requiring prior exposure to the allergen. The Gel and Coombs classification of hypersensitivity (Table 1) is widely published and illustrates the types of hypersensitivity.4 It is important to appreciate that hypersensitivity reactions are not limited to patients and may affect anyone. Dental professionals are regularly exposed to materials which pose a risk of sensitization. Re-exposure to an allergen marks a stronger and more memorable reaction, known as sensitization, whereby the signs and symptoms of allergy become clinically apparent.
Adverse reactions to dental materials are not an uncommon occurrence owing to the vascular nature of the oral environment. The potential of materials to leach out into oral tissues is both advantageous (eg fluoride release in glass ionomer cement) and disadvantageous. Common allergens include local anaesthetics, chlorhexidine, colophony, base metal materials and amalgam. The causative agents and adverse reactions depend on the nature of exposure. For example, glove allergies often affect dental staff whereas dental technicians are at greater risk of acrylic resin allergy.4 Moreover, nickel allergy has been shown to be the most common contact allergy, with 15.4% of reported cases.5
The introduction of resin composite in the 1950s marked the launch of a new era of restorative dentistry. The safety of dental amalgam is regarded as a ‘hot topic’ within dentistry, often facing widespread criticism.6 As a result, some countries have taken to adopting an amalgam-free approach to dental care, therefore increasing demand on manufacturers. Composite usage is not only limited to direct restorations, but also indirect restorations, luting cements, fissure sealants and orthodontics.
Resin-bonding agents are widely used in dentistry and include bonding direct and indirect restorations, dentine desensitizers, pulp capping and immediate dentine sealing. Resin-bonding agent formulations vary, however, the common constituents are usually phosphoric acid, Bis-GMA, 2-HEMA, water, ethanol, dimethacrylate and acetone (Table 2). Adhesion to dental hard tissues involves preparation of the cavity with a procedure of etching, priming and bond application. Over time this procedure has developed with new generations of bonding systems, however, three-step bonding systems are often viewed as the ‘gold standard’ owing to the high bond strength achieved as a result.
Inorganic Fillers
Organic Resin Matrix
Silane Coupling Agent
QuartzCeramicSilicaBa-AI-Si
Monomers (mono, di and trifunctional):
- Bis-GMA (bisphenol-A glycidyldimethacrylate)
- UDMA (urethane dimethacrylate)
Viscosity controllers:
-TEGDMA (triethylene glycol dimethacrylate)
- MMA (methyl methacrylate)
- EGDMA (ethylene glycol dimethacrylate)
Photoinitiators
- Diketone
- Camphoriquinone
Y-mpts (methacryloyloxypropyltrimethoxysilane)
Components of dentine-bonding agents are as follows:
Etchant – commonly 37% phosphoric acid (others include: 3% nitric acid, 10% maleic acid). Etchant primarily acts by decalcifying intertubular and peritubular dentine and dissolving the smear layer, thus creating a scaffold for micromechanical retention and resin tag formation.
Primer – often contains HEMA within a carrier such as acetone or ethanol. Primer is applied to the etched tooth surface and acts as a bridge between hydrophobic resin and hydrophilic dentine.
Bond – involved in the formation of resin tags and the hybrid layer, a key feature of resin-bonding agents. Bonding resin usually consists of Bis-GMA, dimethacrylate resin and methacrylate monomers.
The oral cavity is extremely vascular with many protective host defences in place, such as stratified squamous epithelium and the buffering action of saliva. Similarly, the skin has protective mechanisms in place, however it is more susceptible to hypersensitivity reactions such as contact dermatitis.
Routes of allergens into the oral cavity vary and may be classified as follows:
Oral mucosa
– contact stomatitis;
Skin
– contact dermatitis
– irritant
– allergic;
Tooth
– dentine
– pulp.
The majority of allergies caused by resins are related to monomers, particularly low molecular weight monomers such as TEGDMA. Such monomers are present within the organic resin matrix (Table 2) and are commonly eluted. Research has also suggested causative allergens are epoxy resins and acrylates.7 Delayed type IV hypersensitivity reactions have been reported as a reaction to epoxy resins.8 2-HEMA is a hydrophilic monomer based on methacrylic acid. It has often been reported as a common allergen owing to its high sensitizing potential.9 Interestingly, its use is not limited to the dental environment, and extends to include extra-ocular contact lenses and various drug delivery systems.9
Monomers have been demonstrated as a cause of occupational and non-occupational allergic contact dermatitis. MMA has been demonstrated to be of low toxicity, but is recognized as a skin sensitizer present in a variety of dental materials.10 Consistent with this are the findings of Kanerva and co-workers who reported cases of contact dermatitis of fingertips, thus raising concerns over clinical techniques practised (eg placement of bonding agents on gloves).11
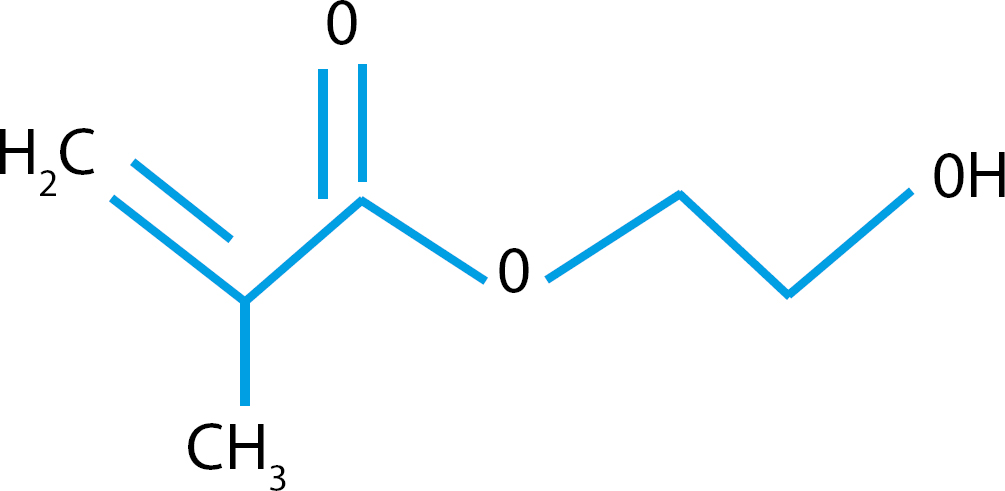
Concern also exists over the potential of monomer leaching due to the incomplete nature of the resin composite polymerization process. Evidence suggests a degree of monomer release and leakage from composite restorations, particularly when uncured, due to mechanical stresses (eg mastication and erosion).12 Bisphenol A (BPA) (Figure 2), a precursor involved in the synthesis of Bis-GMA, is prone to degradation by salivary esterases.13 The potential adverse healthcare effects of BPA are not limited to the oral and dermal tissues: recently concern has been expressed over the effect of bisphenol A on renal function in children, although this has been reported as inconclusive.14
Figure 2. Chemical structure of Bisphenol A.
Additionally, Bis-GMA, a major component of resin composites, has been reported as a common allergen. Bis-GMA is a rigid epoxy acrylate also known as Bowen's resin. The highly viscous nature of this in acrylate results in greater polymerization shrinkage stresses which are detrimental to the integrity of the restoration. As a result viscosity controllers, such as TEGMDA, UDMA and EGDMA, are often added to increase filler loading and reduce polymerization shrinkage. Bis-GMA has a high sensitizing potential, which has been demonstrated in guinea pigs.15 This being said, it is often the low molecular weight monomers which have the potential to cause allergy. TEGDMA is an example of this: it has been reported as a cause of toxicity of gingival and pulpal fibroblasts.16
Given the potential risk of hypersensitivity of resin composites and bonding agents, it is important as dental professionals to have an understanding of diagnosis and management of hypersensitivity. A problem that often exists is the wide spectrum of clinical signs and symptoms with which a patient may present. Furthermore, evidence suggests an element of somatization of allergies;17 often an inherent fear results in some patients labelling a psychological fear as an allergy. It is therefore of paramount importance to differentiate between a true allergy and perception of an allergy. In reality, less than 10% of patients who reported an allergy to penicillin have been demonstrated to suffer from a true allergy.18
The recognition of hypersensitivity
Patients who are at a perceived higher risk of hypersensitivity may be identified at the initial appointment through detailed history-taking.
The salient features of history-taking are commonly:
Medical history
– History of asthma, hay fever, dermatitis and childhood eczema
– Concomitant disease – HIV, EBV, CMV;
History of allergies including frequency, duration and severity of symptoms;
Exacerbating factors (eg particular season, known triggers, environmental factors);
It is important to be up-to-date with medical emergencies and to be able to identify the common features of hypersensitivity (Table 3).
Local
Systemic
- Swelling
- Necrosis
- Burning mouth syndrome
- Mucositis
- Ulceration
- Intra-oral vesiculations
- Pruritis
- Lichenoid reactions
- Urticarial rash (wheal and flare)
- Angiodema
- Anaphylaxis
- Bronchospasms
- Laryngeal oedema
- Prutitis or pruritis
- Oedema
Following acute management of the hypersensitive patient, it is vital to investigate the causative allergen which may necessitate referral to secondary care.19 Measurement of tryptase levels is recommended; serum tryptase release is characteristic of mast cell degranulation therefore it is a diagnostic marker of anaphylaxis.19
Other investigations include:
Skin prick test;
Intradermal test;
Epicutaneous patch testing;
Drug provocation;
Radioallergosorbent test (RAST).
Patient-centred discussions are vital to ensure that patients are fully informed of the nature of their allergies and the effect of such on their dental treatment. This is an important factor in the consent process as the patient may be limited in material choices and treatment options. It is also important to appreciate the risk of material cross-reactivity which may limit treatment choice (eg MMA in denture-based acrylics).
Reporting adverse reactions
The introduction of new generation materials is beneficial, however, the safety of dental materials is not guaranteed. Whilst materials are subject to premarket biocompatibility testing, this may not ascertain complete safety. Post market surveillance is therefore critical as part of a monitoring process. The reporting of adverse drug reactions via the Yellow Card Adverse Drug Reactions Scheme is currently in use, however, this includes only drug and anesthetic reactions, not all dental materials. The Medicines and Healthcare Regulatory Agency (MHRA) has systems in place to report adverse reactions to medical devices.
The Adverse Reactions Reporting Project (ARRP) was set up by the NHS to develop an evidence base of reactions.4,20 Dental professionals, particularly dental practitioners, are ideal candidates to help report adverse reactions to the ARRP in order to obtain a clear picture of the nature of adverse reactions.
The ARRP categorizes reactions as below:
A mild reaction is one requiring only dental treatment;
A moderate reaction is one where the signs and symptoms are significant and the affected person needs specialist referral;
A severe reaction is one that leads to death or is life-threatening, causing serious deterioration in health or where emergency treatment is required.
Prevention
Safe handling of resin composites and bonding systems is critical due to the risk of occupational health hazards. Dental nurses in particular are exposed to a multitude of materials, therefore appropriate training in material handling is of paramount importance. Ideally, due to the increasing clinical use of personal protective equipment, the incidence of contact dermatitis should be relatively low. However, conversely, this appears to be increasing.21 Glove selection is therefore a critical factor, as was demonstrated by Andreasson et al.21 General protection and hygiene measures are therefore important: handwashing must be undertaken before and after each patient contact. Moreover, it is important to ensure adequate ventilation and safe storage of materials to limit monomer exposure. Emergency medical equipment must be checked and staff familiarized and trained in medical emergencies. Patient exposure to free monomers may be reduced with the placement of rubber dam, tight matrix band systems, incremental layer techniques, effective light curing protocols and the use of high volume suction.
Conclusion
Although there remains limited evidence on the association of composites and bonding agents to hypersensitivity reactions, this article aims to highlight the need to consider the potential of hypersensitivity to such materials. In particular, monomers such as 2-HEMA, Bis-GMA, BPA and TEGDMA have been identified as common causative allergens.
The pressure on dental manufacturers to create new materials remains but it is of equal importance to appreciate the associated risk of adverse reactions to such materials. Reliable monitoring systems are required to ensure dental material safety after market release, to enable an accurate picture to be created of the nature of adverse reactions.
The dental team probably takes the safety of resin composites for granted but has an important role to play in the management of patients with known hypersensitivity and prevention remains of paramount importance. The clinician must always balance the risks and benefits of material usage and communicate with relevant specialists as the management of hypersensitivity requires a multidisciplinary approach. It is also important to appreciate the need to refer on to an appropriately qualified professional (eg dermatologists) if it is felt necessary as patient safety and best interests remain key.
Finally, the authors place a great emphasis on the appropriate reporting of adverse reactions to the MHRA and Adverse Reactions Reporting Project (ARPP).