Ng Y-L, Mann V, Rahbaran S, Lewsey J, Gulabivala K Outcome of primary root canal treatment: systematic review of the literature – Part 1. Effects of study characteristics on probability of success. Int Endod J. 2007; 40:(12)921-939
Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J. 2006; 39:921-930
Ørstavik D Time-course and risk analyses of the development and healing of chronic apical periodontitis in man. Int Endod J. 1996; 29:(3)150-155
Nair P On the causes of persistent apical periodontitis: a review. Int Endod J. 2006; 39:(4)249-281
Byström A, Happonen R-P, Sjögren U, Sundqvist G Healing of periapical lesions of pulpless teeth after endodontic treatment with controlled asepsis. Dent Traumatol. 1987; 3:(2)58-63
Siqueira JF, Rôças IN Present status and future directions in endodontic microbiology. Endod Topics. 2014; 30:(1)3-22
Ramachandran Nair P, Pajarola G, Schroeder HE Types and incidence of human periapical lesions obtained with extracted teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996; 81:(1)93-102
Hancock H, Sigurdsson A, Trope M, Moiseiwitsch J Bacteria isolated after unsuccessful endodontic treatment in a North American population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 91:(5)579-586
Ng Y-L, Mann V, Rahbaran S, Lewsey J, Gulabivala K Outcome of primary root canal treatment: systematic review of the literature – Part 2. Influence of clinical factors. Int Endod J. 2008; 41:(1)6-31
Gorni FG, Gagliani MM The outcome of endodontic retreatment: a 2-yr follow-up. J Endod. 2004; 30:(1)1-4
De Deus QD, Horizonte B Frequency, location, and direction of the lateral, secondary, and accessory canals. J Endod. 1975; 1:(11)361-366
Bandlish R, McDonald A, Setchell D Assessment of the amount of remaining coronal dentine in root-treated teeth. J Dent. 2006; 34:699-708
Abbott P Incidence of root fractures and methods used for post removal. Int Endod J. 2002; 35:(1)63-67
Ng YL, Gulabivala K, Mann V A prospective study of the factors affecting outcomes of non-surgical root canal treatment: part 1 periapical health. Int Endod J. 2011; 44:583-609
Andreasen JO, Munksgaard EC, Bakland LK Comparison of fracture resistance in root canals of immature sheep teeth after filling with calcium hydroxide or MTA. Dent Traumatol. 2006; 22:(3)154-156
Murray PE, Garcia-Godoy F, Hargreaves KM Regenerative endodontics: a review of current status and a call for action. J Endod. 2007; 33:(4)377-390
Darcey J, Qualtrough A Resorption: part 1. Pathology, classification and aetiology. Br Dent J. 2013; 214:(9)439-451
Tabiat-Pour S, Roberts A, Harrison R, Chapple I Restorative planning for hemisection surgery: a technique report. Perio Practice Today. 2007; 4:(3)215-219
Guidelines on CBCT for Dental and Maxillofacial Radiology.
Velvart P, Ebner-Zimmermann U, Pierre Ebner J Papilla healing following sulcular full thickness flap in endodontic surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 98:(3)365-369
Velvart P Papilla base incision: a new approach to recession-free healing of the interdental papilla after endodontic surgery. Int Endod J. 2002; 35:(5)453-460
Rubinstein RA, Kim S Short-term observation of the results of endodontic surgery with the use of a surgical operation microscope and Super-EBA as root-end filling material. J Endod. 1999; 25:(1)43-48
Kim S Modern endodontic surgery concepts and practice: a review. J Endod. 2006; 32:601-623
Kim S, Pecora G, Rubinstein R Comparison of traditional and microsurgery in endodontics. In: Kim S Philadelphia: WB Saunders; 2001
Chong B, Pitt Ford T, Hudson M A prospective clinical study of Mineral Trioxide Aggregate and IRM when used as root-end filling materials in endodontic surgery. Int Endod J. 2003; 36:(8)520-526
Torabinejad M, Chivian N Clinical applications of mineral trioxide aggregate. J Endod. 1999; 25:(3)197-205
Velvart P, Peters CI Soft tissue management in endodontic surgery. J Endod. 2005; 31:(1)4-16
Christiansen R, Kirkevang L-L, Hørsted-Bindslev P, Wenzel A Randomized clinical trial of root-end resection followed by root-end filling with mineral trioxide aggregate or smoothing of the orthograde gutta-percha root filling – 1- year follow-up. Int Endod J. 2009; 42:(2)105-114
Torabinejad M, Corr R, Handysides R, Shabahang S Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod. 2009; 35:(7)930-937
Grung B, Molven O, Halse A Periapical surgery in a Norwegian county hospital: follow-up findings of 477 teeth. J Endod. 1990; 16:(9)411-417
Modern endodontic principles part 6: managing complex situations Carly Taylor Reza Vahid Roudsari Sarra Jawad James Darcey Alison Qualtrough Dental Update 2024 43:3, 707-709.
Authors
CarlyTaylor
BDS, MSc, MFGDP, FHEA
Clinical Lecturer/Honorary Specialty Registrar in Restorative Dentistry, Dental School, University of Manchester
Clinicians are often faced with endodontic cases that are significantly more challenging than the primary root canal treatment of mature adult teeth. This paper outlines some of the common treatment modalities which can be employed in situations in which either primary treatment has failed, or there is iatrogenic damage or unusual anatomy.
CPD/Clinical Relevance: This paper will provide the reader with advice and techniques for undertaking orthograde endodontic retreatment, hemisection, endodontic surgery and management of teeth with incompletely formed roots.
Article
Primary endodontic treatment is not always successful.1 Teeth which are no longer painful but, after root canal treatment, have a persisting periapical radiolucency or draining sinus may be considered to have ‘survived’. When there is persistent periapical disease and symptoms, treatment is said to be at best unfavourable and at worst to have failed. However, when teeth become symptomatic the clinician must consider intervention, be it via root canal treatment or extraction.
It is essential to consider the time that has elapsed since the root canal treatment was undertaken; healing takes time. Though the ESE recommends monitoring for 4 years,2 evidence suggests that healing will most likely occur within two years of treatment.3 Serial radiographs are essential and patients must be counselled that a treatment may not have failed, especially if a lesion persists but has diminished in size.
Though there are many possible causes of persistent periapical pathology (Table 1), there is no method of confirming the pathology without histological examination from either apical surgery or extraction.4 When a lesion has become a true cyst or there is an extra-radicular infection, orthograde root canal treatment may not be successful.5 The clinician must therefore recognize that, in some cases, pathology may remain post retreatment, but it is impossible to predict which these may be pre-operatively! Nonetheless, in the majority of cases intra-radicular infection is the primary cause of periapical disease.6,7
Intra-radicular infection
Bacterial biofilm remains/re-established in the canal system due to inadequate cleaning/shaping/obturation, missed anatomy, iatrogenic damage, poor coronal seal, fracture, etc.
Extra-radicular infection
Bacterial biofil.m has developed on the external aspect of the root surface. These biofilms are inaccessible to conventional cleaning protocols. Re-treatment may be unsuccessful.
True cyst
Results from epithelial proliferation and is self-sustaining due to cholesterol clefts and antigens. Re-treatment may be unsuccessful.
Foreign body reaction
Materials extruded into the apical tissues stimulates chronic inflammatory response and fibrous encapsulation. Without retrieval re-treatment may be unsuccessful.
Cholesterol clefts
Formed from degrading lymphocytes, erythrocytes and cholesterol. Macrophages respond producing IL 1B resulting in osteolysis. Re-treatment may be unsuccessful.
Scar tissue
Fibrous tissue formed following apical surgery. Easily mistaken with persistent pathology. No treatment necessary.
The microbiology in failed treatment differs from case to case. In technically inadequate treatment, the bacterial colonies are polymicrobial, resembling those found pre-treatment. However, when the technical quality is perceived to be high, there is often less microbial diversity.8 Bacteriodes, Propionibacterium, Staphylococcus epidermidis and Actinomyces have all been linked to ‘refractory’ disease, in addition to fungi and E. faecalis.9 It is important to understand why these pathogens remain or how they have re-entered the tooth.
In a systematic review of the outcomes of root canal treatment, Ng et al10 concluded that endodontic treatment was more likely to fail in the following circumstances:
Pre-operative presence of periapical radiolucency;
Root fillings with voids;
Root fillings under extended greater than 2 mm from the radiographic apex or over extended obturations;
An unsatisfactory coronal restoration.
If the existing obturation has obvious technical shortcomings, such as over or under extension, poor condensation, under-preparation or there is a poor coronal seal, then it is possible that these factors can be improved upon and orthograde endodontic retreatment attempted. If there are impediments to cleaning and shaping, such as obliterations, ledges and perforations, this may explain primary treatment failure but also forewarn of difficulties in successful retreatment.11 However, if the primary endodontic treatment has been carried out to a good technical standard, then there is little room for improvement and success second time around may be less likely. Missed, additional or accessory canals not apparent in the initial diagnostic radiograph may explain the failure in these cases, highlighting the importance of parallax radiographic views during the examination.12
Retreatment
The first stage in root canal retreatment is the careful assessment of and, if necessary, the removal of existing restorations to access the canal system. Attempting retreatment through an existing restoration can be difficult: visibility is reduced and the artificial morphology of the restoration may mislead the clinician's access preparation. If there is evidence of failing restorative margins, recurrent disease or complex coronal restoration, removal of the crown is advisable. The simplest technique is to create a groove through the mid buccal aspect and extend this across the occlusal surface. Gentle torquing with a flat plastic instrument inserted into the groove will disrupt the cement and dislodge the crown. Pneumatic or slide hammer type designs may be used but are unpleasant for patients and risk damaging both core and gingival tissue. The Wam key (Wam, Aix en Provence, France) is a tool inserted into a pre-prepared slot in the buccal aspect of a crown that may lever the crown coronally. This more delicate approach may also allow the crown to be re-used but relies on the premise that the underlying core is sound. Once a crown has been removed, all diseased tissue should be removed and the tooth assessed for restorability before continuing with endodontic treatment. Absence of ferrule, minimal remaining dentine walls <1 mm in depth and width, and margins that are subgingival, should all alert the clinician that a tooth may have a poor long-term prognosis if restored, or be unrestorable. Readers are referred to papers 1 and 7 of this series and papers on a restorability index that has been developed to aid decision-making.13
Posts
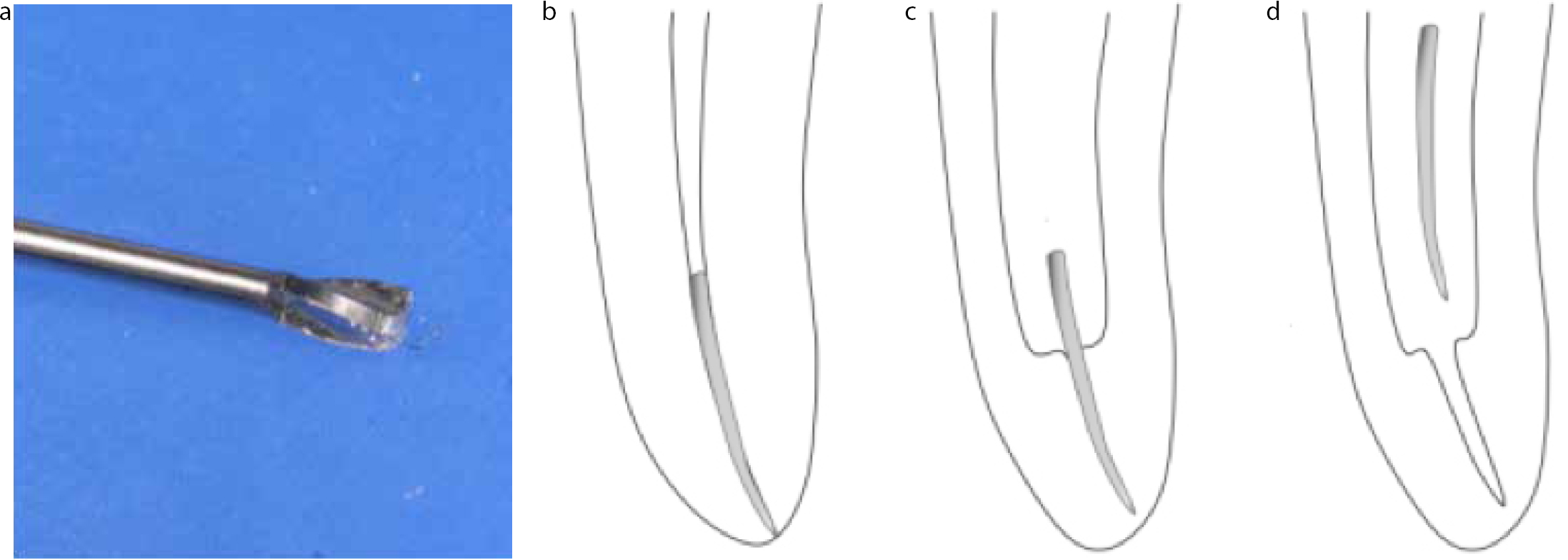
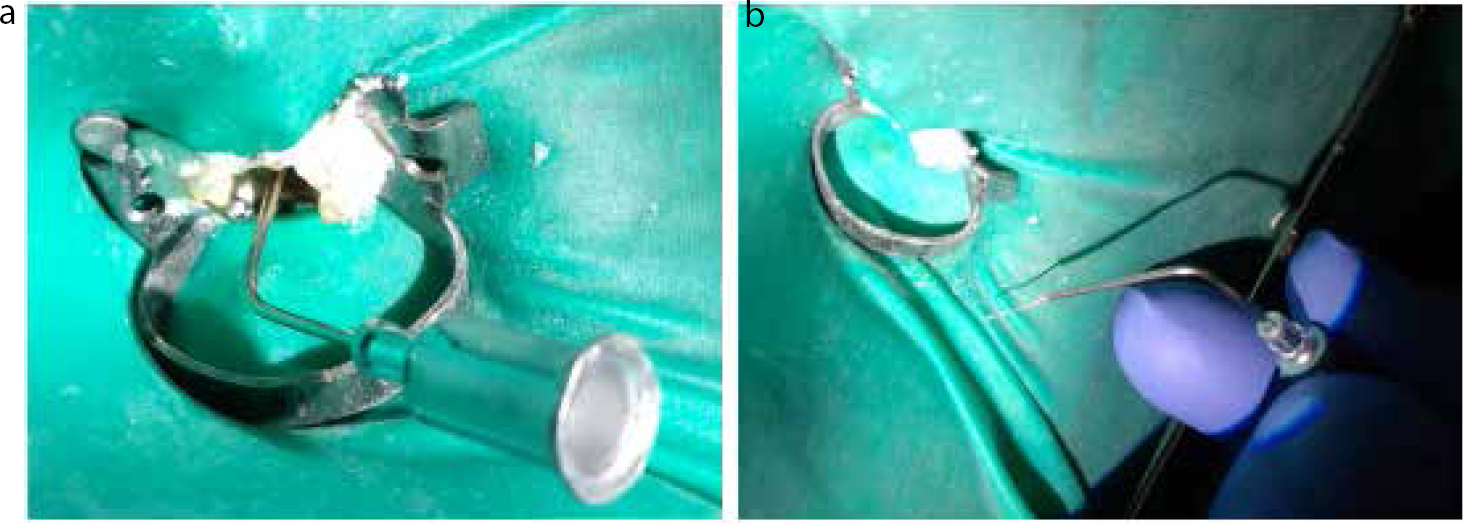
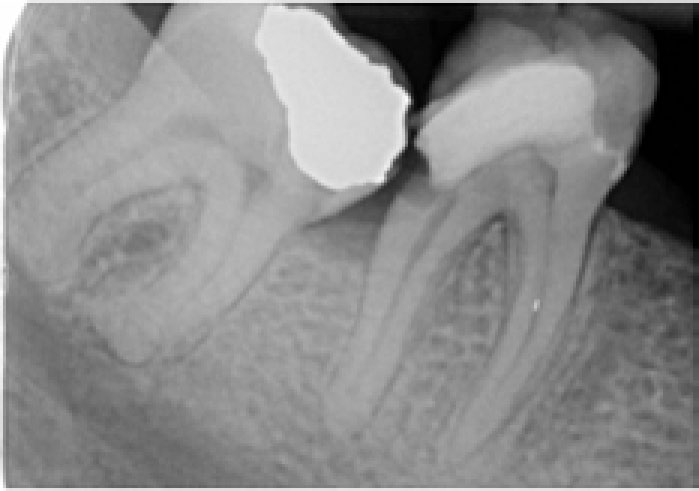
Frequently, a post is present in the canal which requires removal. Assessment of the post should be carried out prior to embarking upon treatment, as this may influence the decision to attempt orthograde retreatment or use a surgical approach. A variety of techniques are available for post removal, including ultrasonic vibration with specialized tips (Figure 1), drilling out the post (non-metallic posts) and a range of post removal kits (Figure 2). Although there is widespread belief that post removal is time consuming and often results in root fracture, Abbott demonstrated a 0.06% incidence of root fracture during 1600 post removals, using a variety of methods.14 The average time taken to remove a post was 3 minutes, although the author of this paper is an expert!
Figure 1. Ultrasonic tips used to aid the removal of posts.Figure 2. Using the Masserann post removal system. (a) Following exposure of the coronal 2 mm of the post, an estimate is made of the post diameter from the radiograph using a sizing guide. (b) The corresponding trepan is used from the kit and placed over the post head to engage the post and, if necessary, remove dentine and cement from the periphery of the post. (c) Rotational and coronal pressure dislodges the post. (d) A post-operative radiograph reveals how much tooth has been sacrificed to remove the post.
Existing gutta-percha
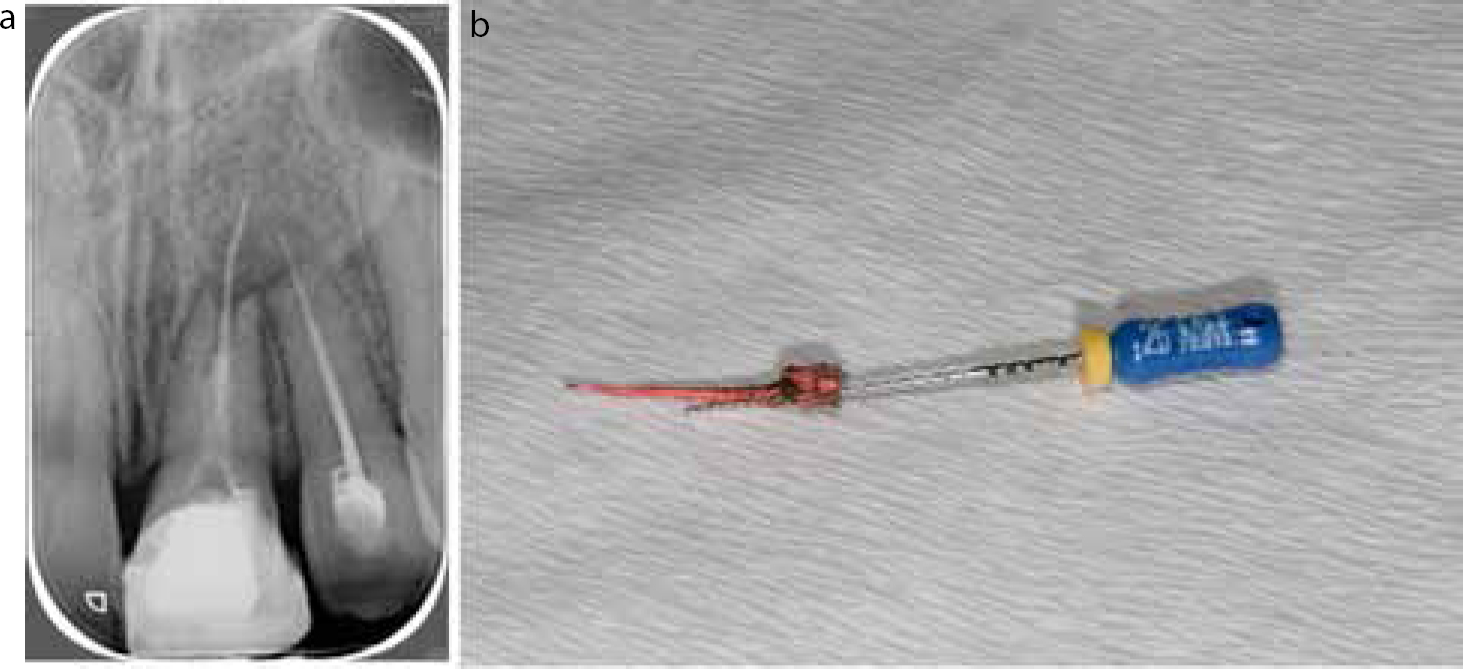
Following removal of the coronal restoration, the existing obturation material needs to be removed. This can be relatively straightforward in the case of a single cone obturation (Figure 3), or far more challenging if the gutta-percha is well condensed. Although conventional endodontic files can be used, several manufacturers have produced specific files for this, which often have deeper flutes to facilitate material removal (Figure 4). As with primary root canal treatment, it is sensible to create a glide path before using conventional rotary instruments. Gutta-percha dissolving agents, such as chloroform or oil of cajeput, may be used (Figure 5). A major shortcoming of using such products is that they smear the gutta-percha over the walls. This can hinder penetration of irrigants and thus disinfection of parts of the canal system. It is therefore sensible only to use these if the GP cannot be penetrated with instruments. If solvents are used, paper points should be placed in the canal to wick away excess solvent and softened GP.
Figure 3. The removal of single points or poorly compacted GP such as those in (a) can be relatively simple. Gently wind a Hedstrom file to engage the GP and pull coronally. (b) The GP will be removed with the file.Figure 4.
ProTaper Retreatment Files (Dentsply, Tulsa). These can be used in sequence to remove the coronal, mid and apical 1/3 root filling material more efficiently before final shaping with conventional instruments. Gates Glidden drills would be a suitable alternative for removing coronal filling.Figure 5. Solvents for removing filling materials are widely available. These include orange solvent, oil of cajeput and other proprietary brands. Endosolv E and Endosolv R are available from Septodont (Saint-Maur, France) for removing GP and resin-based filling materials accordingly. Care must be taken not to spill such solvents; they will dissolve rubber dam rapidly.
Blockages
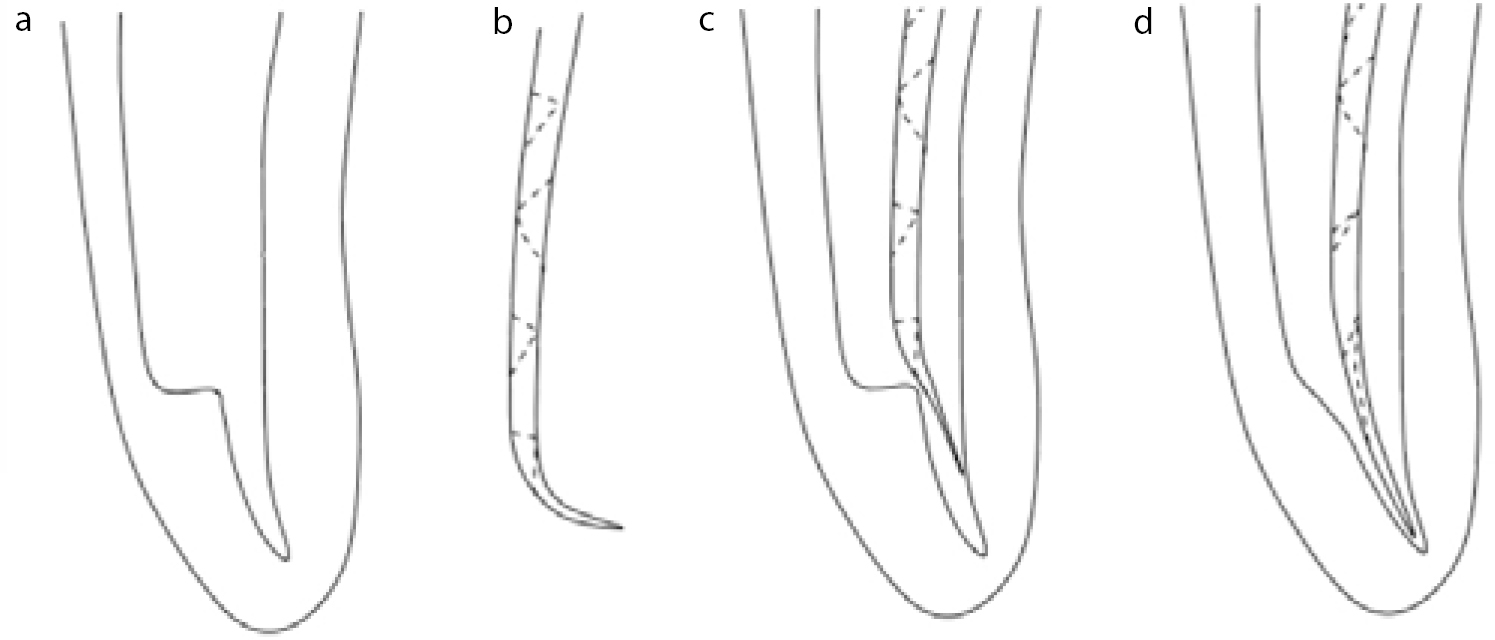
Frequently, the clinician will have to overcome previous iatrogenic damage, including the presence of zips, ledges and transportations. One useful technique for overcoming ledges is to create a sharp bend in a small hand file, using tweezers or specifically designed tools (Endo-Bender™, SybronEndo). This is then worked past the ledge and small back and forth movements are utilized to eliminate the ledge gradually before proceeding to the next size of file (Figure 6).
Figure 6.
(a) A ledge is present within this canal, impeding instrumentation to the apex. (b, c) The placement of a small bend in the tip of a file can help the clinician negotiate the instrument beyond a ledge. (d) From here larger instruments can be placed to length and the ledge slowly removed. Once the ledge has been smoothed, all instruments should have a glide path to the apex.
Separated instruments
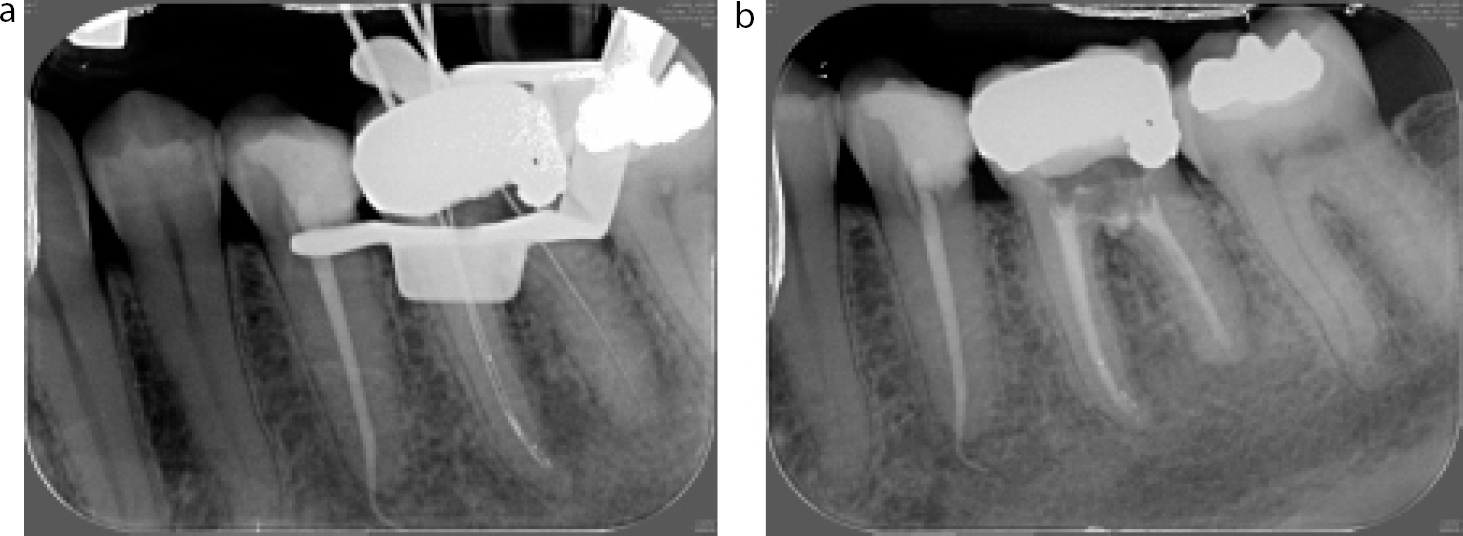
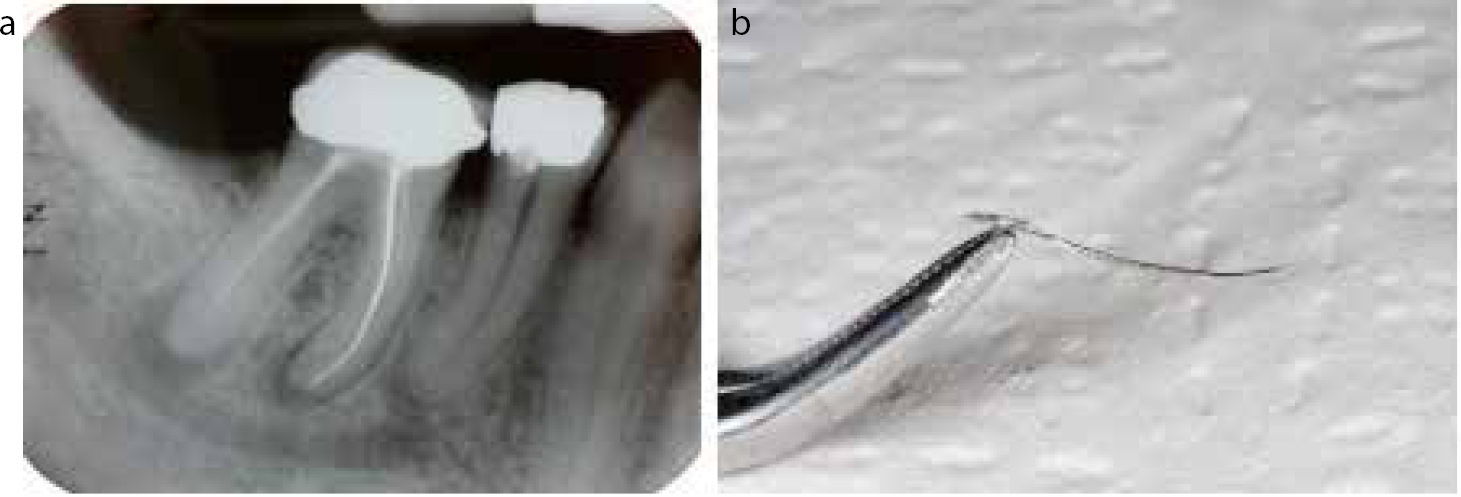
Careful assessment of fractured instruments needs to be undertaken in order to determine the location and possible material of the fractured portion. Instruments located in the coronal and middle thirds can often be retrieved, especially in straighter canals. Those instruments located in the apical third are rarely retrievable, especially in curved canals, and attempting to bypass the instrument is often the only choice (Figure 7). In a relatively straight canal, instruments may be removed simply, by using ultrasonic instruments to loosen the fragment and endodontic forceps to retrieve it (Figure 8). When the instrument lies more apically, or is ‘screwed’ into the dentine, alternative approaches may be required. One technique involves creating a coronal platform around the head of the instrument. The coronal platform can be created by drilling the tip off a Gates Glidden bur. Fine ultrasonic tips are then used to ‘trough’ around and loosen the instrument (Figure 9). The instrument can then be retrieved by various methods. These include attempting to twist two hand files around the instrument, using a syringe needle with cyanoacrylate glue applied to the tip, or introducing a hand file into the syringe to grip the instrument (Figure 10). The latter techniques can only be attempted if some of the instrument protrudes from the canal. Such techniques, however, can significantly weaken the remaining tooth structure. An operating microscope or high magnification loupes with a fibre optic light source are essential.
Figure 7.
(a) The instrument tips in the mesial canals of this LL6 can be bypassed with files. (b) The completed obturation shows good preparation and filling despite the instruments remaining in the canal system.Figure 8.
(a) The radiograph reveals there to be a silver point in one of the mesial canals of LR6. (b) Modified artery forceps and ultrasonics were used to remove the silver point from the MB of this LR6. It is important not to use ultrasonics directly on silver points as they may shatter, creating difficulties to remove retained apical portions. Stieglitz forceps are much finer and ideal for removing instruments. Every practice should have a pair.Figure 9.
(a) Following removal of the tip of this Gates Glidden, (b) it can be used around the coronal aspect of the instrument (c) to create a platform. (d) Once exposed, the separated instrument may be removed with ultrasonics.Figure 10.
(a) Cyanoacrylate (Super Glue) is withdrawn into a syringe tip carefully sized to fit over the instrument. The syringe is then placed over the instrument and left to set for 5 minutes. (b) Following this a coronal pull should dislodge the instrument. Images courtesy of Dr Omayma Madi.
Once the obstacles have been by-passed or cleared, essentially the tooth should be managed in a similar way to primary root canal treatment, in terms of cleaning, shaping and obturation. A notable deviation from the protocols may lie in the use of irrigant. Studies have shown that, in retreatment cases, the use of iodine and EDTA as adjuncts to sodium hypochlorite irrigation may be beneficial.15 However, chlorhexidine irrigation in retreatment cases has been shown to have a negative effect.15 Where significant iatrogenic damage has occurred, which may preclude the development of a continuously tapering preparation, thermoplastic obturation techniques may be required to achieve a satisfactory obturation.
Complex anatomy
The clinician may be faced with teeth exhibiting unusual anatomy. One relatively common situation is teeth with arrested root development, often following trauma. The key challenges are that:
They have thin dentinal walls of reduced length, which are prone to fracture;
There is no apical constriction, with the canal often being wider in the apical region (blunderbuss).
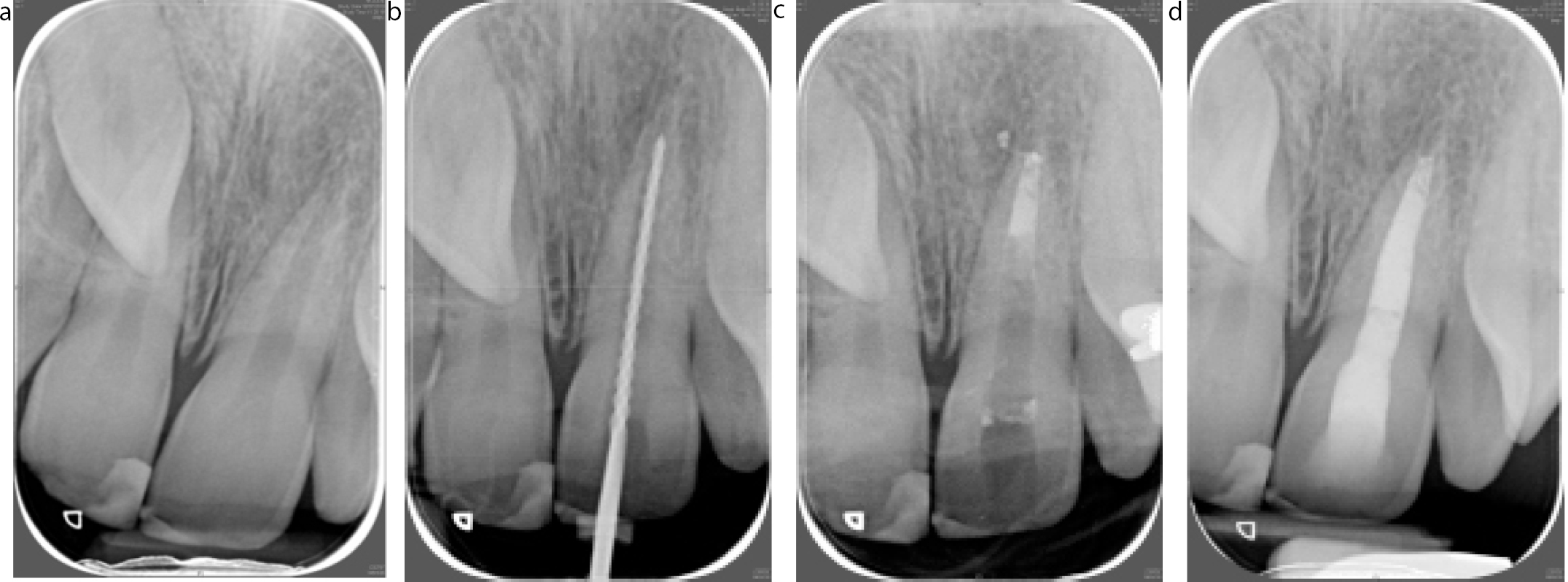
This can result in extrusion of obturation materials and the inability to obturate the canal system adequately. Traditional techniques aimed to create an apical barrier to facilitate obturation, by repeatedly placing calcium hydroxide dressings in the tooth. Limitations of this technique include long treatment time and weakening of the root dentine.16 With advances in materials, apical barriers can now be created in a single visit using mineral trioxide aggregate (MTA) or Biodentine™ (Septodont, St Maur, France) (Figure 11). More recently, regenerative techniques aimed at stimulating root development have been reported.17 Such treatments aim to not only create an apical constriction but also an increase in root length and thickness. A description of this technique and suggested clinical protocol will be discussed in the final paper of this series.
Figure 11.
(a) This non-vital UL1 has an incomplete apex. (b) Following working length determination, a 3 mm apical barrier of MTA is placed. (c, d) A radiograph confirms the MTA is well condensed and in the correct position before backfill with warm flowable GP is completed.
Resorption
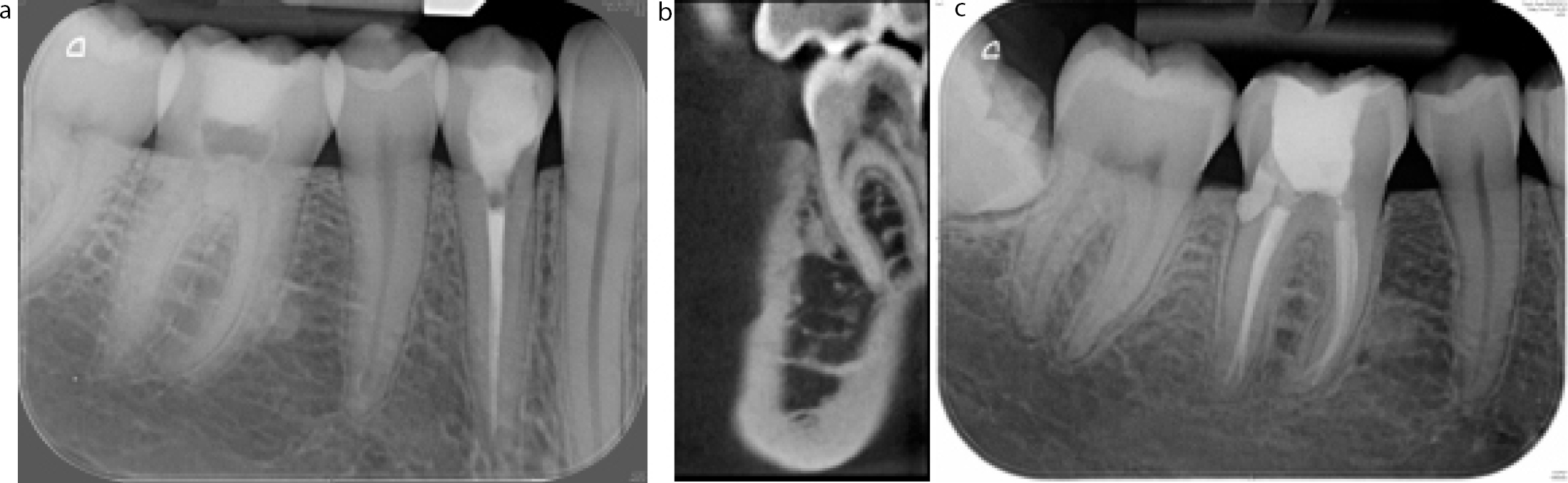
Resorptive defects can also present a challenge to endodontists. It is beyond the remit of this paper to discuss this topic in detail and readers are referred to a comprehensive paper discussing the subject.18 Despite this, internal resorptive defects may result in canal irregularities and loss of an apical constriction. Contemporary management of such cases may require many differing approaches, including the use of bioactive materials and flowable obturation materials (Figure 12).
Figure 12.
(a) The LR6 has extensive cervical inflammatory resorption. (b) The CBCT reveals the extent of the lesion. (c) Elective endodontics was performed and the resorptive cavity cleaned and filled with MTA internally.
Perforations
Primary endodontic and retreatment can result in iatrogenic damage to the tooth. From small ledges to perforations, the risk is ever present. Prevention is the best strategy, with careful access and instrumentation. If a perforation is created, there is often profuse bleeding and may be pain. It can be confirmed with an apex locator: a zero reading from the site will confirm connection with the periodontal tissues.
When assessing a perforation; large defects, increased length of time before repair and coronal location of the defect all contribute to a more uncertain prognosis for that tooth. Thus delaying repair and referring may result in poorer outcomes. Practitioners should familiarize themselves with newer materials and be prepared to repair defects at time of injury. Biologically active materials should be used to repair defects and these will be covered in paper 8 of this series.
Hemisection
Occasionally, one root of a mandibular molar tooth may not be amenable to treatment, despite the rest of the tooth and its supporting structures being relatively intact. Hemisection refers to the process of intentional removal of a root and its associated coronal tooth tissue, in an attempt to avoid complete extraction of a multi-rooted tooth. Indications for undertaking hemisection are presented in Table 2 (Figure 13). It is sometimes possible to resect the root only, leaving the clinical crown intact but, if the roots are fused, then extraction is often indicated. If root resection is planned, then careful consideration needs to be given to the likely occlusal forces as the coronal portion of the tooth will remain untouched, yet the root support is compromised.
Failed endodontic treatment/persistent periapical pathology affecting one root
Root fracture involving one root
Perforation affecting one root
Unrestorable caries affecting one root
Advanced periodontal bone loss involving one root
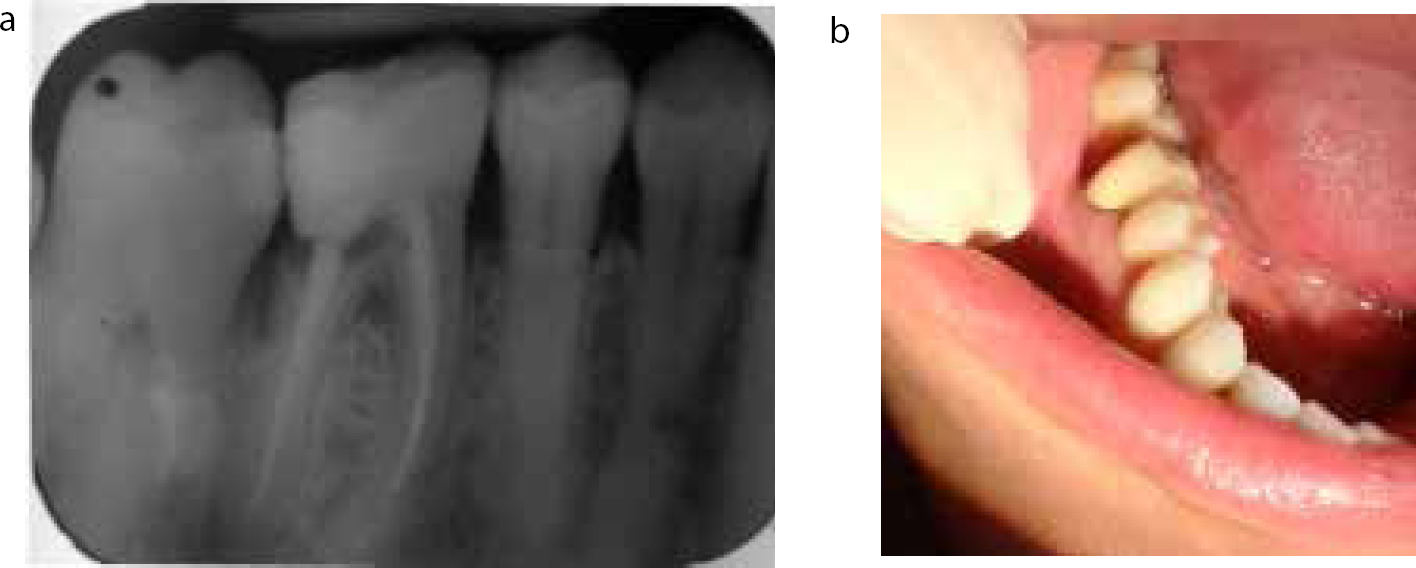
Figure 13. LR7 has extensive distal caries resulting from the mesially impacted LR8. The periodontal defect and depth of caries renders this tooth of poor prognosis. In this situation, hemisection would be a good treatment plan.
Factors which favour hemisection of a tooth are presented in Table 3. The root/s to be retained must have good periodontal bone support, ideally with no bone loss in the furcation region. The tooth should have a high furcation, otherwise it will be difficult to provide a satisfactory indirect restoration which does not impinge on the biological width and is amenable to cleaning by the patient.19 Parallax radiography is often helpful in these circumstances. The definitive restoration must be carefully planned. The occlusal table of the final restoration should be reduced to minimize the occlusal loads placed upon the tooth. The tooth may be premolarized (Figure 14) or crowned and a cantilever design adopted to maintain the original molar morphology (Figure 15). A ‘tear drop’ shaped indirect restoration, in which a wash through pontic is attached to the crown, allows easy access for patient cleaning whilst preserving proximal contacts and preventing over eruption of the opposing tooth.19
Good bone support of the remaining root
Absence of furcal bone loss
High furcation
Uncomplicated canal morphology of the remaining root favouring a successful outcome for endodontic treatment
Absence of periapical pathology of the remaining root/s
Favourable occlusal forces - absence of parafunction, tooth not involved in protrusive or excursive guidance
Presence of adjacent teeth in order to prevent drifting of the remaining tooth
Figure 14.
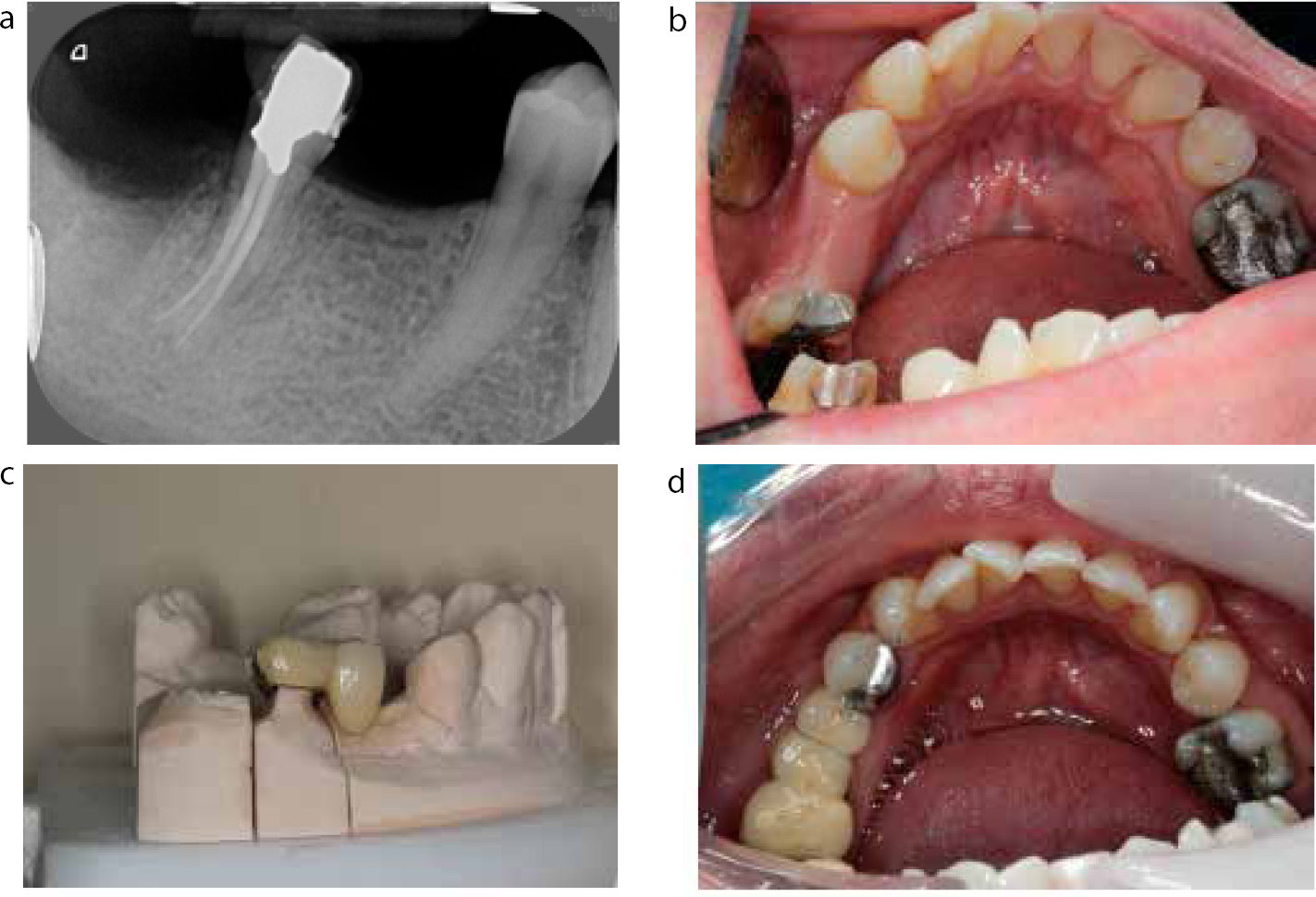
(a) Shows extensive caries around the distal margin of the restoration LR6. (b) Following amputation of the distal root of the LR6 the mesial root was premolarized.Figure 15.
(a) The distal root of the LR6 has been amputated. (b) The tooth is prepared for indirect restoration. (c) A conventional cantilevered bridge is constructed. (d) The space is partially restored with this premolar design and with an adhesive cantilever from the LR4.
Hemisection may be a technically demanding, labour intensive and costly procedure; therefore the importance of retaining the tooth and a careful assessment of its prognosis must be considered and communicated to the patient. With careful planning and technique, good outcomes can be achieved.
Clinical procedure for hemisection
Visit 1
Endodontic treatment should be carried out prior to the resection. It is not essential to clean and shape the root which is planned for removal fully, but it may be useful to enlarge the coronal portion of the canal and place some gutta-percha in the coronal third. This can be a useful landmark when sectioning takes place. Once the obturation of the roots to be retained is complete, place a corono-radicular (Nayyar) core in the tooth. Amalgam is preferred as it is easily distinguishable during sectioning and when preparing the finish line for the definitive restoration.
Visit 2
Sectioning of the tooth can be undertaken with a high-speed handpiece, using the buccal groove as a landmark. Some clinicians prefer raising a flap prior to exodontia. This allows visual and facilitates tactile confirmation that the entire furcation has been removed and that a ‘lip’ of dentine does not remain in this region (Figure 16). Preparation for the indirect restoration should be undertaken at this visit if adequate haemostasis has been achieved. Given the apical extent of the finish line, it is prudent to provide a restoration with a metal finish line to prevent over preparation and not to impinge on the biological width. If a tooth-coloured restoration is required, then buccal porcelain with a metal collar may suffice in the posterior region (Figure 17). A chairside temporary restoration can be made from a pre-operative impression.
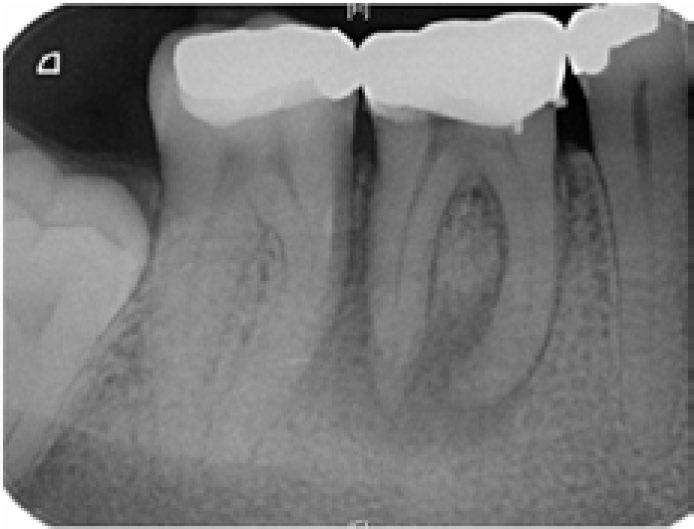
Figure 16. Hemisection of the mesial root was required. It is important to section the tooth at the highest point of the furcation and not leave a ‘lip’ of dentine.Figure 17. Crown with a metal collar which requires a less destructive labial finish line.
Endodontic surgery
Though modern endodontic surgery is significantly different from traditional approaches, the indications and contra-indications remain the same (Table 4). Most of these modifications in technique have only been made possible by the use of magnification (Table 5), ultrasonic apical preparation and bioactive materials. To understand the evolution of modern apical surgery it is essential to address each stage of the procedure.
Indications
Contra-indications
Radiographic evidence and/or symptoms of periapical periodontitis where orthograde root canal treatment is not possible owing to obstruction of the canal or the prospect that attempted orthograde treatment will jeopardize the longevity of the tooth
Local anatomy or tooth positioning prevents access to the apex
Radiographic evidence and/or symptoms of periapical periodontitis where there is material extruded beyond the apex that cannot be retrieved via an orthograde approach
Unco-operative patient
Perforation of the root or floor of the pulp that cannot be repaired from within the pulp
Medical history contra-indicates a surgical approach
Persistent periapical disease following root canal treatment where further retreatment is inappropriate
Inadequate periodontal support
Allows more precise inspection of the operating field for pathology, fractures or perforations
Facilitates the distinction between bone and root tip
Allows more precise root end amputation, apical preparation and obturation
Allows smaller osteotomy
Improves operator posture
Variable magnification may be used throughout the procedure depending upon need
Imaging
With the advent of CBCT it is possible to investigate the intricacies of the root canal system and more precisely estimate the presence and extent of disease. This can be of vital importance when establishing whether conventional non-surgical root canal retreatment is possible and, if not, the merits of a surgical approach (Figure 18). In addition, CBCT gives the clinician very accurate information on the location of roots and their relation to anatomical structures: essential when planning and consenting patients to surgery.20
Figure 18.
(a) Failed root canal treatment UL6 suggests the presence of a second mesio-buccal root. (b) CBCT reveals there to be not one but three canals within the mesio-buccal root.
Flap design
The use of a semilunar incision is contra-indicated as it does not allow good access and is prone to scarring. The full thickness mucoperiosteal flap raised from an intrasulcular incision has historically been the foundation of surgical access. Although such flaps allow good visibility, post-operative gingival recession is often a problem; furthermore, with refined surgical techniques such large flaps are no longer deemed necessary.21
The modern flaps of choice are the submarginal and papilla preservation flaps22 (Figure 19). These preserve vital coronal soft tissue allowing good repositioning of flaps without significant post-operative recession. Micro-surgical, double-sided cutting blades are available on a round handle and allow the surgeon to manoeuvre the blade like a pen with improved precision (Figure 20).
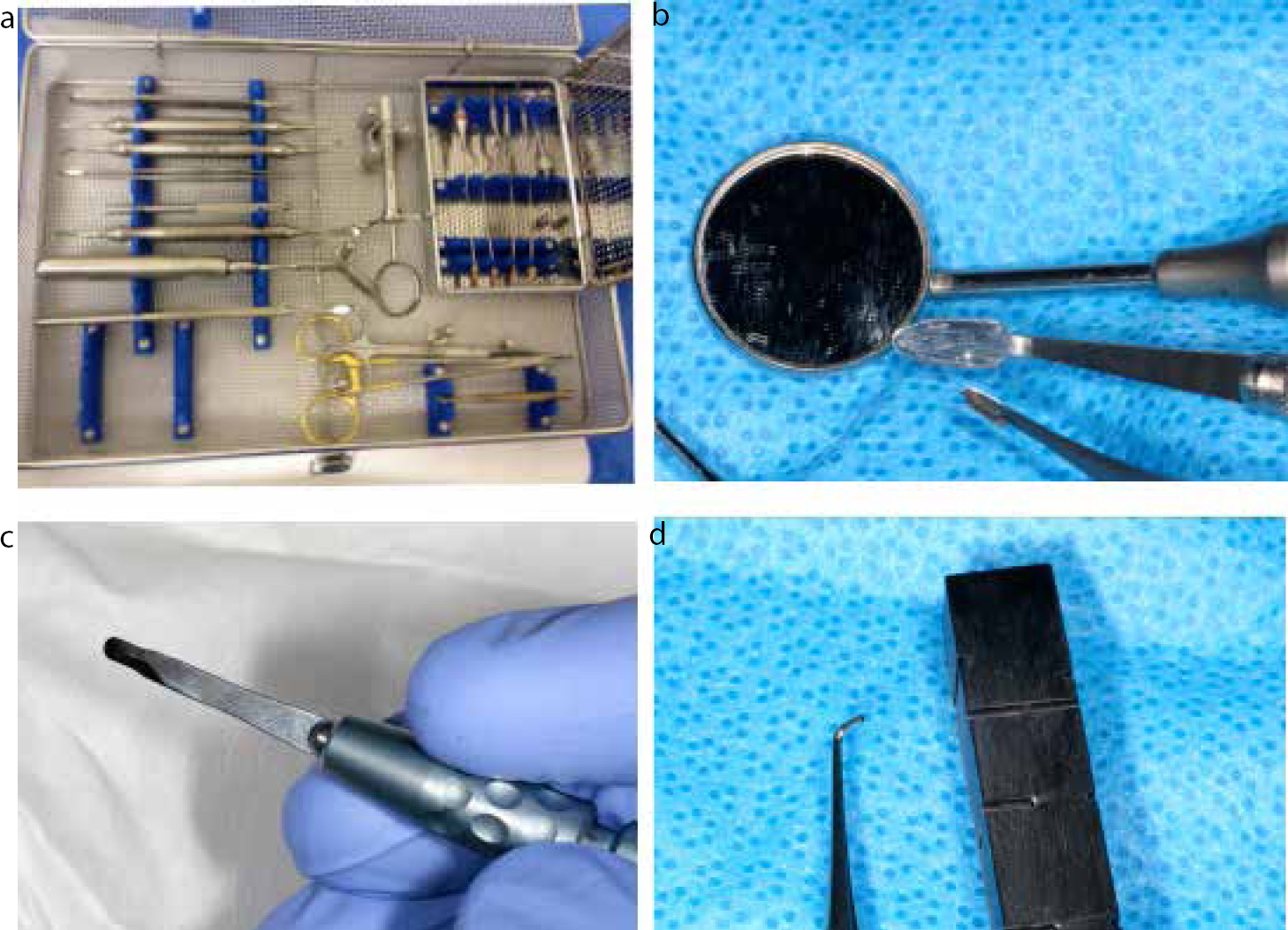
Figure 19. The sub-marginal incision was made in this case but a papilla preservation incision has also been illustrated.Figure 20. Tools in the armamentarium: (a) the full endodontic micro-surgical tray; (b) micro mirror adjacent to a regular mirror; (c) micro-surgical blade; (d) block for compacting MTA and micro-plugger for delivery and compaction of the MTA at the apex.
The submarginal incision (or Leubke Oschenbein) follows the gingival contours of the teeth but lies approximately 3 mm apical to the free gingivae, thus preserving a collar of attached gingivae. This flap design necessitates sufficient depth of attached gingivae not less than 3 mm. This may only be used if the operator is confident that the lesion does not extend so far coronally as to be inaccessible to curretage.
The papilla base preservation incision follows an intrasulcular incision mid-buccally. This technique necessitates two incisions that preserve the papilla. The first enters at 90 degrees to the gingival mucosa to a depth of 1.5 mm. The second incision (via the first) deviates towards the alveolar crest allowing the flap to be raised buccally, preserving the papilla base with a butt junction to allow optimal apposition of the flap following apicectomy and minimal scarring.
Once the flap has been lifted, careful handling will minimize trauma to the tissue and allow more favourable healing. It is good practice to ensure elevators and tissue retractors rest upon bone and not soft tissue. Some operators recommend the placement of a groove in the cortical bone into which a retractor can be placed and stabilized to minimize further trauma. This may have the added benefit of protecting vital structures, most notably, the mental nerve.
Osteotomy
Traditional osteotomies involved the removal of a large window of bone. The modern focus should be on only removing sufficient bone to allow access to the apex and enlarged if periradicular curettage cannot be easily performed (Figure 21). The use of micro-surgical instruments permit access into significantly smaller resections. Smaller osteotomies heal more quickly and minimize the likelihood that a periodontal communication may be created.23 An attempt must be made to remove all granulation tissue. Good practice demands histopathological examination of removed tissue. If such facilities are not available, the patient should be consented in advance that histological confirmation of any tissue cannot be undertaken.
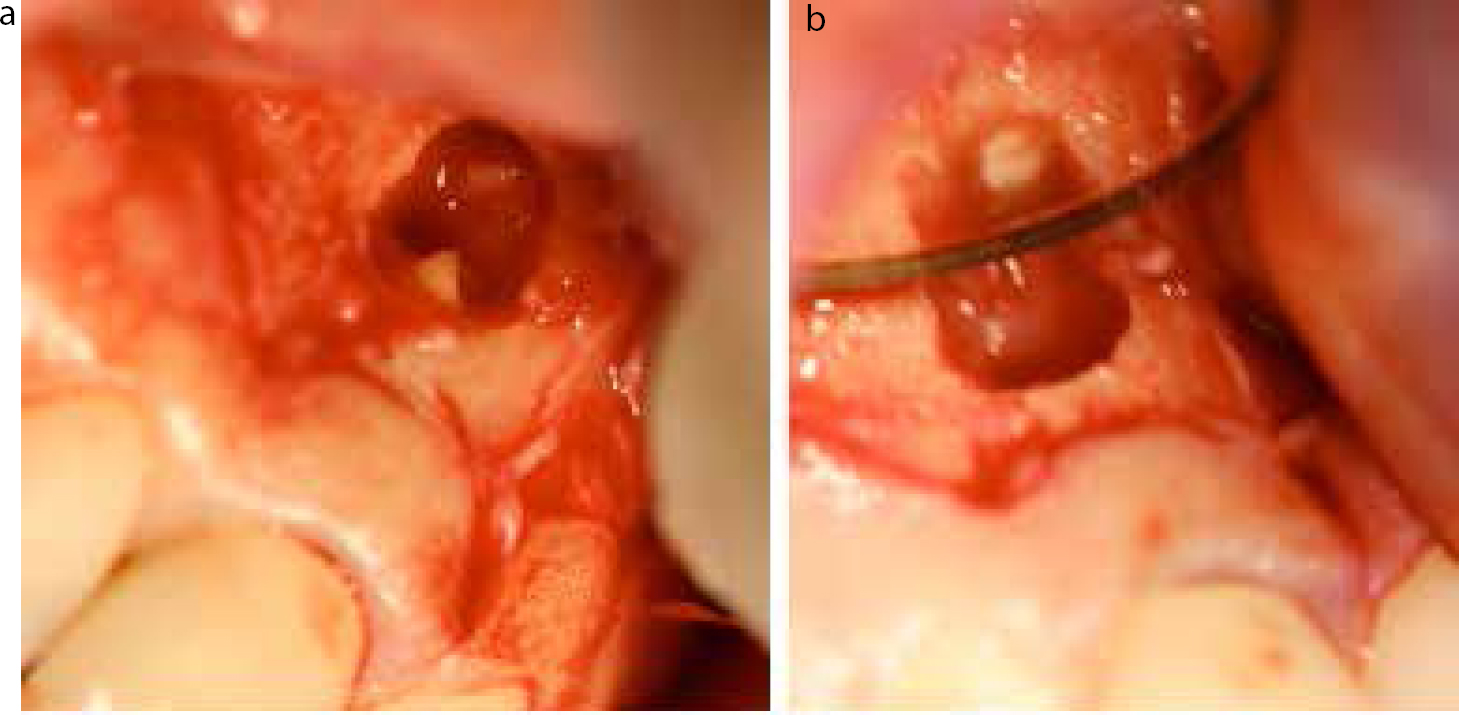
Figure 21. Maintaining a small osteotomy still permits access to the apex for preparation and promotes faster healing. (a) Demonstrates the smaller osteotomy and (b) the final obturation.
Root end preparation
As 98% of ramifications and 93% of accessory canals are found in the apical 3 mm, this remains the recommended depth of root amputation.24 The amputation should be at right angles to the root surface and not bevelled. Although surgical straight fissure burs may be used, ultrasonic units may allow a less traumatic and more precise root amputation.
The root end preparation should be performed to a depth of 3 mm and stay centred within the canal structure to avoid perforation or the creation of an undercut on the buccal aspect of the cavity preparation. The use of ultrasonic, diamond-coated, right-angle tips are recommended. These come in a variety of shapes and sizes, allowing the clinician to follow the anatomy precisely. It is essential that the root end is closely inspected, as isthmuses and second canals, if not prepared, may contain bacterial biofilm and, if left, result in failure.25
Root end obturation
Once prepared, the apical cavity must be filled. Amalgam, composite and glass ionomer are not appropriate restorative materials. The two most commonly used types of material are reinforced zinc oxide eugenols (Super EBA and IRM) and the bioactive calcium silicates (MTA, Biodentine™, Septodont, St Maur France). There may be little significant difference in outcome between the use of MTA and IRM,26 but the clinician must be aware that calcium silicates offer additional benefits that outweigh the higher financial costs: only repair occurs with IRM but, with calcium silicates, regeneration of cementum and periodontal ligament may follow.27 (Such advantages will be covered in the final paper of this series.) It is the belief of the authors that calcium silicate materials are the gold standard.
Care must be taken to ensure good moisture isolation. Techniques, such as the placement of bone waxes, haemostatic agents (ferric sulphate), resorbable agents (Surgicel®) or vasoconstrictors into the osteotomy have been advocated but, more simply, ribbon gauze carefully packed around the root tip will control bleeding. It is for this reason that local anaesthetic for periapical surgery should contain epinephrine, unless there are specific contra-indications. MTA can be difficult to handle and instruments are available to help manipulate and compact the material into the prepared cavity (Figure 22). The material should be carefully compacted to ensure three-dimensional obturation and improved peripheral seal. Once filled, the apex should be carefully inspected for voids.
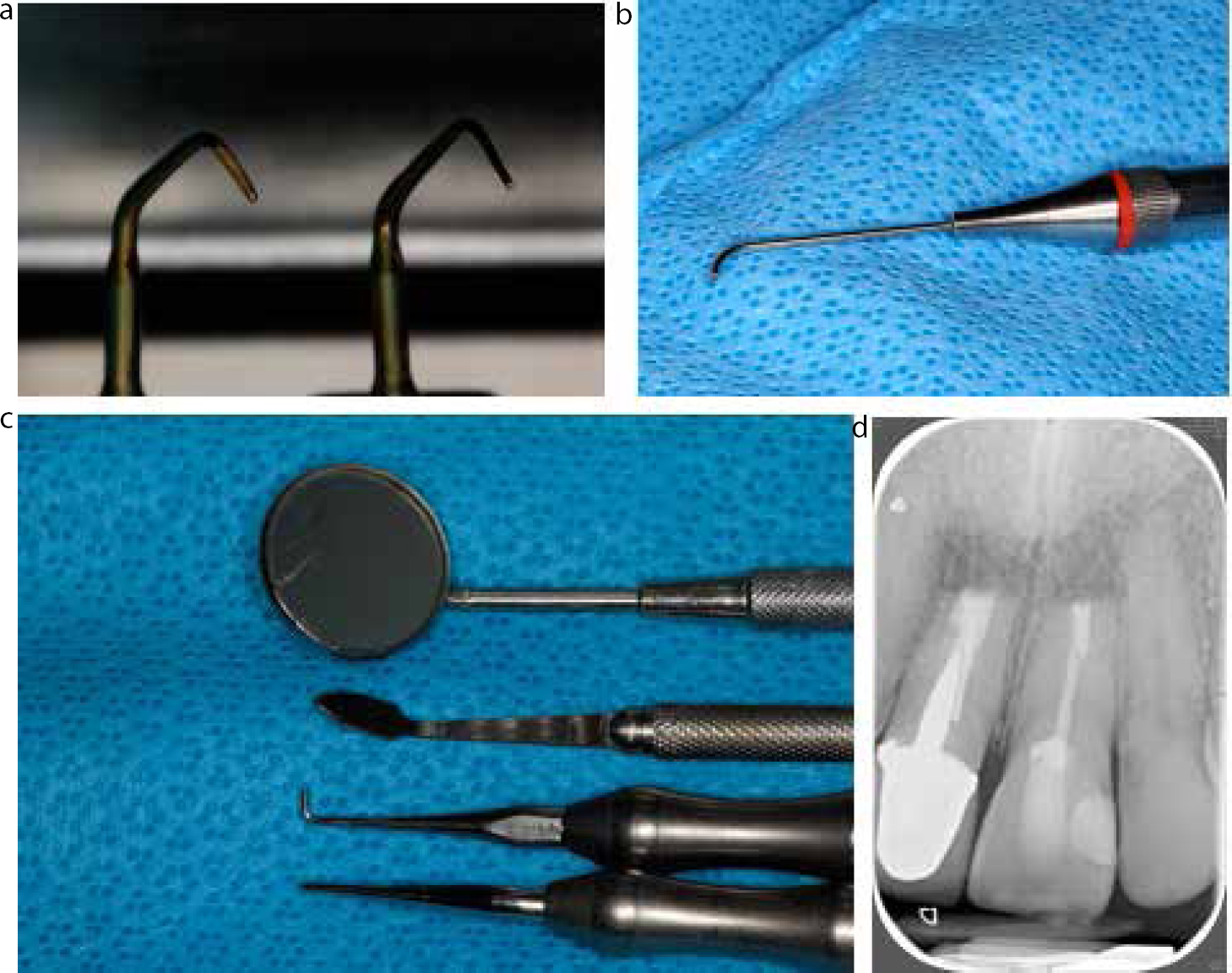
Figure 22. The use of contra-angled, diamond-coated ultrasonic tips: (a) in conjunction with dedicated MTA placement tools (MAPTM System, Dentsply, Tulsa); (b) and micro-pluggers; (c) allows precise root end preparation and MTA placement with minimal collateral damage. In this case, (d) the separated instrument UR1 could not be removed and the apical preparation was enlarged to encompass the instrument tip in MTA.
Flap closure
Monofilament sutures have replaced braided silk sutures. The latter accumulate plaque and delay healing through a wicking effect into the tissues, resulting in inflammation. The use of 5-0 and 6-0 polypropylene sutures leaves a smaller wound that heals faster. Sutures should be removed at 3–5 days.28
Success
Modern endodontic success rates have been quoted as high as 96%.29 There is some evidence that, although surgical treatment is associated with a higher short-term success, long-term success rates are not so favourable.30 This is thought to be related to the persistence of micro-organisms within the canal structure. Furthermore, success rates are significantly higher where there is evidence of good orthograde treatment.31 It is therefore imperative that the clinician should, wherever possible, attempt orthograde root canal treatment before electing a surgical approach.
Conclusion
This paper has highlighted some of the more challenging endodontic situations faced by clinicians and provided the reader with an overview of the principles, modern techniques and materials for managing them.