Eyrich GK, Baltensperger MM, Bruder E, Graetz KW Primary chronic osteomyelitis in childhood and adolescence: a retrospective analysis of 11 cases and review of the literature. J Oral Maxillofac Surg. 2003; 61:(5)561-573
Prasad KC, Prasad SC, Mouli N, Agarwal S Osteomyelitis in the head and neck. Acta Otolaryngol. 2007; 127:(2)194-205
Eckman MH, Greenfield S, Mackey WC, Wong JB, Kaplan S, Sullivan L Foot infections in diabetic patients. Decision and cost-effectiveness analyses. JAMA. 1995; 273:(9)712-720
Marx RE Chronic osteomyelitis of the jaws. Oral Maxillofac Surg Clin North Am. 1991; 3:367-381
Bevin CR, Inwards CY, Keller EE Surgical management of primary chronic osteomyelitis: a long-term retrospective analysis. J Oral Maxillofac Surg. 2008; 66:2073-2085
Koorbusch GF, Fotos P, Goll KT Retrospective assessment of osteomyelitis. Etiology, demographics, risk factors, and management in 35 cases. Oral Surg Oral Med Oral Pathol. 1992; 74:149-154
Hudson JW Osteomyelitis of the jaws: a 50-year perspective. J Oral Maxillofac Surg. 1993; 51:1294-1301
Aitasalo K, Niinikoski J, Grenman R, Virolainen E A modified protocol for early treatment of osteomyelitis and osteoradionecrosis of the mandible. Head Neck. 1998; 20:411-417
Bevin CR, Inwards CY, Keller EE Surgical management of primary chronic osteomyelitis: a long-term retrospective analysis. J Oral Maxillofac Surg. 2008; 66:2073-2085
Lucchesi L, Kwok J Long term antibiotics and calcitonin in the treatment of chronic osteomyelitis of the mandible: case report. Br J Oral Maxillofac Surg. 2008; 46:400-402
Lee L Inflammatory lesions of the jaws, 4th edn. Missouri: Mosby; 2000
Montonen M, Kalso E, Pylkkaren L Disodium clodronate in the treatment of diffuse sclerosing osteomyelitis (DSO) of the mandible. Int J Oral Maxillofac Surg. 2001; 30:313-317
Suei Y, Taguchi A, Tanimoto K Radiographic evaluation of possible etiology of diffuse sclerosing osteomyelitis of the mandible. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997; 84:571-577
Beretta-Piccoli BC, Sauvain MJ, Gal I, Schibler A Synovitis, acne, pustulosis, hyperostosis, osteitis (SAPHO) syndrome in childhood: a report of ten cases and review of the literature. Eur J Pediatr. 2000; 159:594-601
Eckardt JJ, Wirganowicz PZ, Mar T An aggressive surgical approach to the management of chronic osteomyelitis. Clin Orthop Relat Res. 1994; 298:229-239
van Merkesteyn JP, Groot RH, van den Akker HP, Bakker DJ, Borgmeijer-Hoelen AM Treatment of chronic suppurative osteomyelitis of the mandible. Int J Oral Maxillofac Surg. 1997; 26:450-454
Kim S, Jang H Treatment of chronic osteomyelitis in Korea. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 92:394-398
Marx RE Chronic osteomyelitis of the jaws. In: Laskin D, Strass R Philadelphia: Saunders; 1992
Bamberger DM Osteomyelitis. A commonsense approach to antibiotic and surgical treatment. Postgrad Med. 1993; 94:177-182
Kovrey ME, Perrott DH, Kaban LB The use of rigid internal fixation in mandibular fractures complicated by osteomyelitis. J Oral Maxillofacial Surg. 1994; 52:1114-1119
Mehra P, van Heukelom E, Cottrell DA Rigid internal fixation of infected mandibular fractures. J Oral Maxillofacial Surg. 2009; 67:1046-1051
A pathological fracture of the mandible due to osteomyelitis following a full dental clearance Preeti Jauhar Thomas Handley Nicholas Hammersley Dental Update 2024 43:2, 707-709.
Authors
PreetiJauhar
BDS, MFDS RCPS(Glasg)
Monklands Hospital, Airdrie, Lanarkshire, Scotland, UK
Orofacial infections following dental extractions are a common referral to an oral and maxillofacial department as an emergency, especially when combined with swelling and limited mouth opening. The case presented demonstrates a rare complication of chronic suppurative osteomyelitis with bilateral pathological fractures of the mandible, which occurred following a staged dental clearance.
CPD/Clinical Relevance: Dental extractions are one of the most common treatments carried out by oral surgeons and general dental practitioners. This case highlights a rare but encountered complication of routine oral surgery and demonstrates when it is necessary to make an immediate referral to the local oral and maxillofacial surgery unit.
Article
Case report
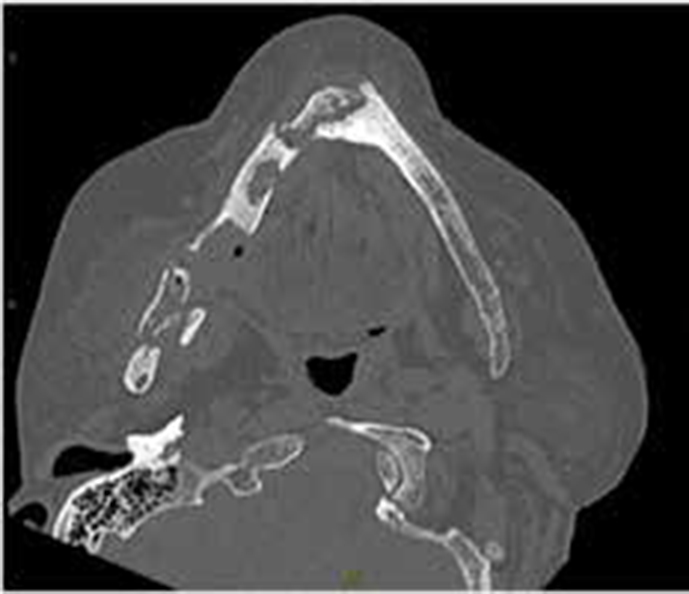
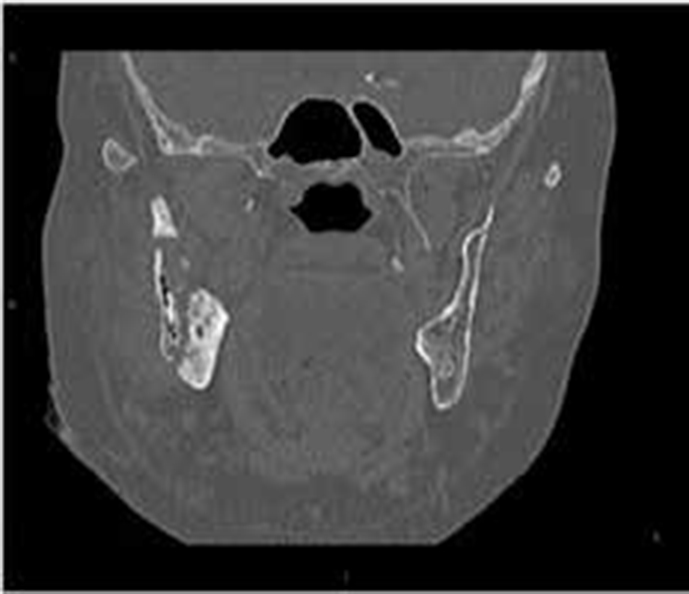
A 58-year-old female patient presented at an oral and maxillofacial outpatient clinic with a nine-month history of pain, swelling and draining fistulas at the right angle of mandible and submental region. This was following a staged full dental clearance by her general dental practitioner. A 10-week course of oral antibiotics had already been prescribed without resolution of symptoms or signs. On presentation she was afebrile with a normal pulse rate and blood pressure. She had a swollen right face, trismus and suppurative infection draining from these fistulas (Figure 1); there was no palpable lymphadenopathy. Intra-orally there were draining fistulas present on the alveolar mucosa of the right body of the mandible and mobility of the mandible was present at the right angle and symphysis. Radiographic examination was carried out with an OPT but, due to patient factors, a diagnostic image was unachievable and CT imaging was undertaken. This revealed gross destruction of the right ramus and symphysis of the mandible, associated pathological fractures and multiple sequestrae with pockets of gas in the soft tissues in keeping with infection. The coronoid and condylar processes, as well as the proximal body of mandible, were noted to be markedly sclerotic on the right-hand side with a lamellar type periosteal reaction. These features were felt to be consistent with a diagnosis of chronic suppurative osteomyelitis (Figures 2–5). A white cell count, CRP and bone profile were normal.
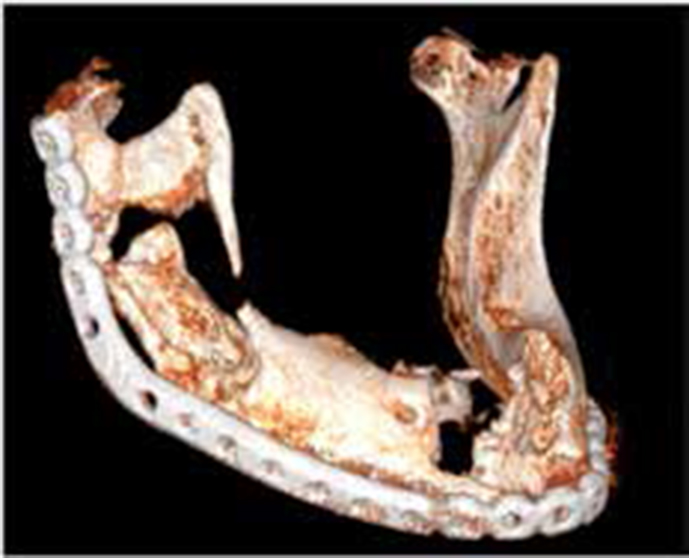
Figure 1. Draining sinuses at the right submandibular and submental regions.Figure 2. CT axial images demonstrating the pathological fractures and sequestration.Figure 3. CT coronal reformat showing bony destruction of the right ramus of mandible.Figure 4. CT coronal reformat showing bony destruction and sequestration at the mandibular symphysis.Figure 5. 3D reconstructed image of the pathological fractures of the mandible.
Her past medical history was significant and included severe rheumatoid arthritis, steroid-induced osteoporosis, major depression, hypertension, severe peripheral vascular disease with a left below knee amputation and she was therefore wheelchair-bound, peptic ulcer disease, and continued MRSA colonized venous ulceration. Current medications included prednisolone, clopidogrel, omeprazole, mirtazapine, atenolol, furosemide and amilodipene. There was a history of allergy to penicillin and rifampicin. She was an ex-smoker with a 30-pack year history and she drank moderate levels of alcohol.
The patient was immediately admitted to clinic and commenced on intravenous vancomycin and metronidazole on the advice of microbiology clinicians and investigations performed to assess her suitability for surgical intervention. Her clopidogrel was stopped and she was placed on low molecular weight heparin. Whilst waiting for surgery, swabs from the draining fistulas revealed a growth of Strep. milleri sensitive to the prescribed antibiotics.
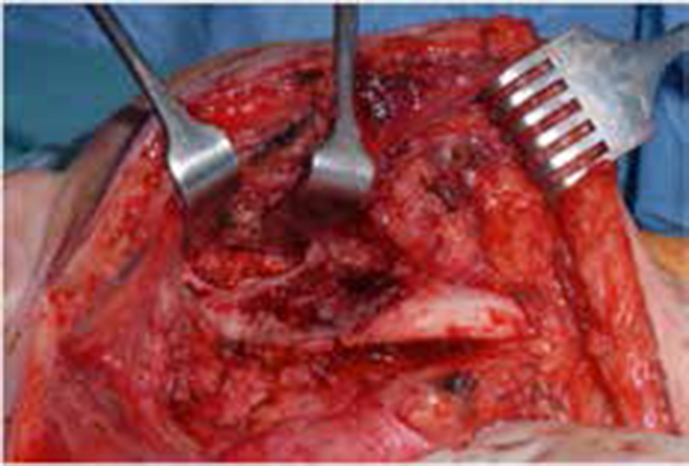
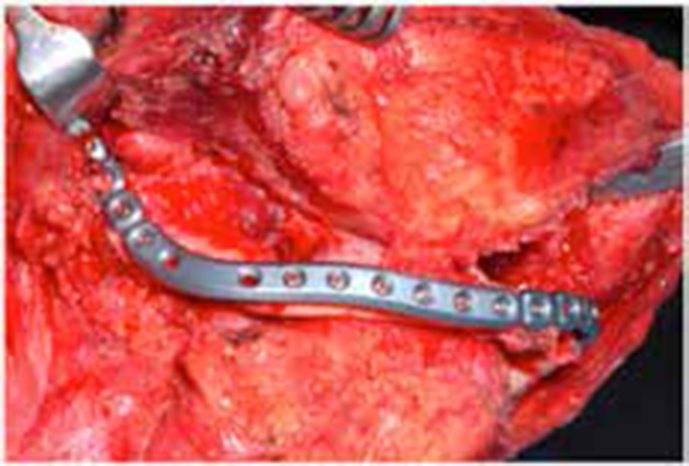
Following the initial management and surgical work-up, the patient underwent surgical debridement of the fracture sites via an extra-oral approach. Necrotic bone was debrided back to healthy bleeding bone (Figure 6), the fistulas were excised and rigid internal fixation was applied to the mandible in the form of a preformed 2.5 mm reconstruction plate with bicortical locking screws (Figures 7 and 8). The intra-oral fistulas were excised and closed primarily and a nasogastric tube was placed to enable enteral nutrition whilst the intra-oral wounds healed. Pathological and microbiology specimens taken at the time of surgery confirmed the clinical diagnosis and sensitivities. The antibiotics were continued for a further four weeks intravenously and the patient was then discharged from hospital. Follow-up of the patient has demonstrated excellent wound and fracture healing with no further complications.
Figure 6. Intra-operative view of the right ramus of mandible osteomyelitis.Figure 7. Rigid internal fixation in situ following thorough surgical debridement and fracture reduction.Figure 8. 3D reconstructed image of the postoperative CT following debridement and internal fixation.
Discussion
This case demonstrates some of the typical features of chronic suppurative osteomyelitis (secondary chronic osteomyelitis), a rare but well documented potential complication of chronic odontogenic infections which general dental practitioners may encounter.
Osteomyelitis is an inflammatory process involving cortical and cancellous bone. In the maxillofacial skeleton the mandible is the most frequently affected bone.1 It occurs most commonly in the mandible due to the dense, poorly vascularized cortical plates and a single blood supply from the inferior alveolar neurovascular bundle.2
The majority of the time a bacterial focus is identified as a source of infection, however, occasionally in some cases no clear aetiology is found. In modern day practice, osteomyelitis more often presents as a chronic condition and is more commonly associated with debilitated, immunosuppressed or medically compromised patients.3
Classification
Using the nomenclature discussed by Eyrich et al,1 acute and chronic osteomyelitis are differentiated arbitrarily on time: the acute process occurs up to one month after the onset of symptoms and chronicity is beyond this point.4
Chronic osteomyelitis is often further subdivided into primary chronic osteomyelitis (PCO) and secondary chronic osteomyelitis (SCO). PCO is a non-suppurative chronic inflammation of unknown aetiology which starts insidiously, with no acute phase. SCO is defined as chronic osteomyelitis that develops secondarily to an acute phase, with the presence of suppuration, sequestration, abscess and fistula formation at some stage during the disease process, occurring as a result of a defined, infectious aetiology.5
Aetiology
Osteomyelitis of the jaw is a relatively uncommon inflammatory disease in developed countries.6 It usually affects adults and is relatively rare in children. The incidence of the disease has dramatically decreased with modern day antimicrobials and improvements in medical and dental care.7,8 The primary cause of chronic osteomyelitis of the jaws is infection by odontogenic micro-organisms.7 It may also arise as a complication of dental extractions and surgery, maxillofacial trauma and the subsequent inadequate treatment of a fracture, and/or irradiation to the mandible.9 Predisposing factors include autoimmune disease,10 trauma11 and other conditions affecting the vascularity of the bone, such as radiation, malignancy, osteoporosis, osteopetrosis, and Paget's disease. Systemic factors that cause concomitant alteration in host defences, such as diabetes, steroids and malnutrition, profoundly influence the course of osteomyelitis.12
The jaws are unique from other bones in the body by the presence of teeth which create a direct pathway for infectious agents to invade bone by means of caries and periodontal disease.13 Oral bone appears to be particularly resistant to infection despite its exposure to oral flora.14 This further reiterates the rarity of the mandible developing osteomyelitis.
Infection spreads into the marrow spaces of the mandible, resulting in an inflammatory reaction. There is a decrease in the blood supply to the area as there is tissue necrosis and suppuration leading to the development of pus within the bone marrow spaces. The infection can extend through cortical bone, involving the periosteum and resulting in the creation of a collection of necrotic bone submerged in pus. Chronic suppuration will lead to the formation of intra-oral or extra-oral fistulas.
Presentation
Acute osteomyelitis is characterized by a virulent infection with intense pain, tenderness, inflammation, swelling, erythema and limited mouth opening. If, however, the bacteria are less virulent, the symptoms can differ and mimic an acute and prolonged alveolar osteitis, making it difficult to diagnose and thus treat. In its chronic form, features include fistula tract formation, bony sequestration and even pathological fracture.
Imaging
Imaging modalities in investigating this disease process include plain radiography in the form of a dental panoramic radiograph, however, due to the number of differential diagnoses, further imaging should be sought. This is usually in the form of conventional or cone beam CT, which will reveal in detail the extent of bone and soft tissue involvement. Bone resorption is the prominent feature with an osteolytic pattern. Sclerotic areas may be seen around the osteolytic area, particularly in long-standing lesions. There may be a periosteal reaction, which is usually lamellated, and appears as a thin, faint, radio-opaque line adjacent to the surface of the bone. A radiolucent band separates the new periosteal bone from the bone surface. If the process occurs repeatedly, an 'onionskin' appearance is observed.15 In the early stages of the disease process, MRI T1 weighted images are more useful at detecting marrow changes as inflamed tissue creates low signal intensity in the normally bright signal of fat contained in the marrow.3 MRI may also be helpful in disease monitoring.16
Differential diagnosis
The differential diagnoses in cases of insidious onset should include malignant and benign entities, as discussed by Eyrich et al.1 The benign lesions should include ossifying and non-ossifying fibroma. The malignant causes which should be considered are Ewing's sarcoma, osteosarcoma, chondrosarcoma, primary oral malignancies and metastatic disease (Table 1).
Differential Diagnosis
Clinical Features
Radiological Features
Diagnosis
Osteosarcoma
Pain, swelling, paraesthesia, loss of sensation, increased mobility of teeth, trismus - patients tend to be middle-aged
Irregular; ‘sun-ray appearance’ - trabeculae of bone radiate perpendicularly around the lesion
Imaging and biopsy
Osteoradionecrosis
Pain, non-healing tissue, history of radiotherapy or bisphosphonate use
Irregular, moth-eaten, minimal evidence of healing
Imaging and biopsy
Osteomyelitis
Intra-oral or extra-oral sinus, pain, swelling, pyrexia, malaise, trismus, paraesthesia of teeth, increased mobility of teeth Patients tend to be at extremes of age
Irregular; moth-eaten, sclerosis of surrounding bone, sequestra of bone
Imaging and biopsy
Squamous cell carcinoma
Non-healing tooth socket, indurated, rolled edges, swelling, increased mobility of teeth, paraesthesia, decreased mobility of adjacent tissues
Irregular, bony destruction and invasion, displacement of teeth
Imaging and biopsy
Ossifying fibroma (cemento-ossifying fibroma)
Painless swelling, slow-growing mass in bone
Radio-opaque associated with root of a tooth and a radiolucent margin
Biopsy - excisional for treatment and for confirmation of diagnosis
Ewing’s sarcoma
Pain, swelling, mucosal ulcers, displacement and increased mobility of teeth
Non-specfic features, may mimic an infectious process or a malignancy. Moth-eaten destructive radiolucency of the medullary bone with expansion and destruction of the cortex
Biopsy and imaging
Chondrosarcoma
Pain, swelling, increased mobility of teeth
Radiolucency - well or poorly circumscribed, varied appearance, may be multi-locular and contain calcifications
Biopsy - histological confirmation for diagnosis
Metastatic disease
Swelling, increased mobility of teeth, displacement of teeth, paraesthesia
Moth-eaten, ragged edges, radiolucent
Further imaging, biopsy - depending on disease progression
Pathogenesis
The widely documented difficulty in managing this condition reflects the pathogenesis, which is thought to be due to the relatively avascular and ischaemic nature of the infected area and sequestrum, thus producing an area of lowered oxygen tension that antibiotics cannot penetrate. The lowered oxygen tension impairs the bacteriocidal activities of polymorphoneutrophils and converts a previously aerobic infection into one that is anaerobic. The diffusion rate of antibiotics into the dead bone is so low that, regardless of the external concentration, adequate penetration is impossible. This may lead to ineffective antibiotic concentrations at the site of infection, despite adequate therapeutic serum concentrations.17 Early diagnosis of this destructive infection can reduce the need for surgical therapy and allow for the prevention of major complications. These include sepsis, gross mandibular destruction, pathological fractures and, in its chronic form, recurrence.
Treatment
Management in this case entailed a course of antibiotics in combination with aggressive surgical debridement. This is consistent with published protocols.7,18,19 It has been suggested that the minimum duration of antibiotic therapy to treat CSO is two weeks.20 However, it has also been suggested by Bamberger21 that a minimum of four weeks is indicated. Fracture treatment requires rigid fixation; traditionally methods of treatment for pathological fractures include external fixation and inter-maxillary fixation. However, there is increasing evidence for the use of rigid internal fixation in the treatment of infected fractures.22,23 Adjuvant treatments available include ozone gas or hyperbaric oxygen therapy,3 but these are reserved for persistent cases where standard treatment has failed, or in cases with already impaired vascularity.
Conclusion
This case is an example of when simple dental treatment can result in significant complications and morbidity. Early diagnosis of this destructive infection can reduce the need for surgical therapy and allow for the prevention of major complications. These include sepsis, gross mandibular destruction, pathological fractures and, in its chronic form, recurrence. The main reason for delayed diagnosis is as a result of a general lack of awareness of this condition, its risk factors and its presenting features.
This case had significant risk factors for the development of osteomyelitis as well as a characteristic clinical presentation. The diagnosis was missed, unfortunately, and treated with repeated courses of antibiotics for what was thought to be a simple ‘slow to respond’ post-operative infection. This led to significant progression in the disease process and significant morbidity.
Long-term close follow-up will be necessary to ensure that there is no recurrence of the infection or complications arising from the treatment carried out.