Katusic S Incidence and clinical features of trigeminal neuralgia, Rochester, Minnesota, 1945–1984. Ann Neurol. 1990; 27:(1)89-95
Hall GC Epidemiology and treatment of neuropathic pain: the UK primary care perspective. Pain. 2006; 122:(1–2)156-162
Dieleman JP Incidence rates and treatment of neuropathic pain conditions in the general population. Pain. 2008; 137:(3)681-688
Koopman JS Incidence of facial pain in the general population. Pain. 2009; 147:(1–3)122-127
Devor M, Amir R, Rappaport ZH Pathophysiology of trigeminal neuralgia: the ignition hypothesis. Clin J Pain. 2002; 18:(1)4-13
Love S, Coakham HB Trigeminal neuralgia: pathology and pathogenesis. Brain. 2001; 124:(12)2347-2360
Jannetta PJ Neurovascular compression in cranial nerve and systemic disease. Ann Surg. 1980; 192:(4)518-525
Luo DS An animal model for trigeminal neuralgia by compression of the trigeminal nerve root. Pain Physician. 2012; 15:(2)187-196
Cephalalgia. 2004; 24:9-160
Zakrzewska JM Diagnosis and differential diagnosis of trigeminal neuralgia. Clin J Pain. 2002; 18:(1)14-21
Rasmussen P Facial pain. IV. A prospective study of 1052 patients with a view of: precipitating factors, associated symptoms, objective psychiatric and neurological symptoms. Acta Neurochir (Wien). 1991; 108:(3–4)100-109
Zakrzewska JM, McMillan R Trigeminal neuralgia: the diagnosis and management of this excruciating and poorly understood facial pain. Postgrad Med J. 2011; 87:(1028)410-416
Limonadi FM, McCartney S, Burchiel KJ Design of an artificial neural network for diagnosis of facial pain syndromes. Stereotact Funct Neurosurg. 2006; 84:(5–6)212-220
Rasmussen P Facial pain. III. A prospective study of the localization of facial pain in 1052 patients. Acta Neurochir (Wien). 1991; 108:(1–2)53-63
Rasmussen P Facial pain. II. A prospective survey of 1052 patients with a view of: character of the attacks, onset, course, and character of pain. Acta Neurochir (Wien). 1990; 107:(3–4)121-128
Drangsholt M, Truelove EL Trigeminal neuralgia mistaken as temporomandibular disorder. J Evid Based Dent Pract. 2001; 1:41-50
McMillan R Trigeminal neuralgia – a review of a disabling facial condition. Dent Nursing. 2011; 7:(11)618-623
Gronseth G Practice parameter: the diagnostic evaluation and treatment of trigeminal neuralgia (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the European Federation of Neurological Societies. Neurology. 2008; 71:(15)1183-1190
Zakrzewska JM, Linskey ME Trigeminal neuralgia. BMJ Clin Evid. 2009;
Cruccu G AAN-EFNS guidelines on trigeminal neuralgia management. Eur J Neurol. 2008; 15:(10)1013-1028
Moriarty O, McGuire BE, Finn DP The effect of pain on cognitive function: a review of clinical and preclinical research. Prog Neurobiol. 2011; 93:(3)385-404
Li P Clinical outcomes of 114 patients who underwent gamma-knife radiosurgery for medically refractory idiopathic trigeminal neuralgia. J Clin Neurosci. 2012; 19:(1)71-74
Academic Clinical Fellow and Honorary Teacher in Oral Medicine, Eastman Dental Hospital, University College London Hospitals NHS Trust, 256 Gray's Inn Road, London, WC1X 8LD, UK
Trigeminal neuralgia (TN) is also known as ‘tic douloureux’ (in French, ‘painful twitch’). It is a rare chronic facial pain syndrome, characterized by severe, brief, stabbing, ‘electric shock-like’ recurrent pain attacks felt in one or more divisions of trigeminal nerve innervation areas. So intense is the elicited pain that TN has a significant effect on a sufferer's quality of life, rendering many patients unable to consider a future with the ongoing threat of recurrent pain. The aim of this article is to discuss the diagnosis and management of this disabling facial pain condition.
CPD/Clinical Relevance: As general medical practitioners may struggle differentiating TN from toothache, primary care dentists have an important role in excluding odontogenic cause of pain, diagnosing TN and referring patients to a facial pain clinic for further investigations and multidisciplinary team management.
Article
Epidemiology
A detailed epidemiological study investigated the incidence and prevalence rates of TN from 1945 until 1984, and found an overall annual incidence rate of 4.7 per 100,000 in the Minnesota, USA, population. Females were affected twice as commonly as males (5.2 and 2.5 per 100,000 population per year, respectively).1 This study used strict inclusion criteria and may have missed the data of patients diagnosed in the community, thus creating an impression that TN is even less common. Two more recent studies from the UK2 and Netherlands3 found much higher annual incidence rates of 26.8 and 28.9 per 100,000 population per year, respectively. Both these studies used data from general practice research databases. However, a specialist might not have confirmed some of these patients' diagnoses. A recent study by Koopman and colleagues4 further investigated the results obtained from the general practice research database and patients with unclear TN diagnosis were reviewed by neurologists. The incidence rate of TN was found to be less than half that previously reported – 12.6 per 100,000 population. Again, females were more affected than males – 17.8 and 7.3 per 100,000, respectively.4
Aetiopathogenesis
Although the aetiopathogenesis of TN is still not absolutely clear, currently the most accepted hypothesis of TN pathophysiology is the ignition hypothesis by Devor and colleagues.5 It suggests abnormalities of afferent trigeminal neurons in either the trigeminal nerve or trigeminal ganglion that can be caused by compression or demyelination. This damage makes the neurons hyperexcitable, which means that they may generate impulses autonomously at abnormal locations. This, in turn, can cause spontaneous nerve firing lasting several seconds, so called after-discharge. After-discharge bursts can be triggered by external stimuli, such as a soft touch, however, they can occur intermittently without any obvious cause. This abnormal firing can be augmented by positive feedback from other neurons and, as a result, an increasing number of neighbouring neurons are involved by a chain reaction, resulting in the characteristic TN attack. During the burst, calcium ions enter the neuron and potassium ions leave the cell, causing hyperpolarization of the neuron and ending the firing. Post-burst hyperpolarization can last more than a minute and, in this time, the next burst cannot be triggered. This explains the refractory period between pain attacks.
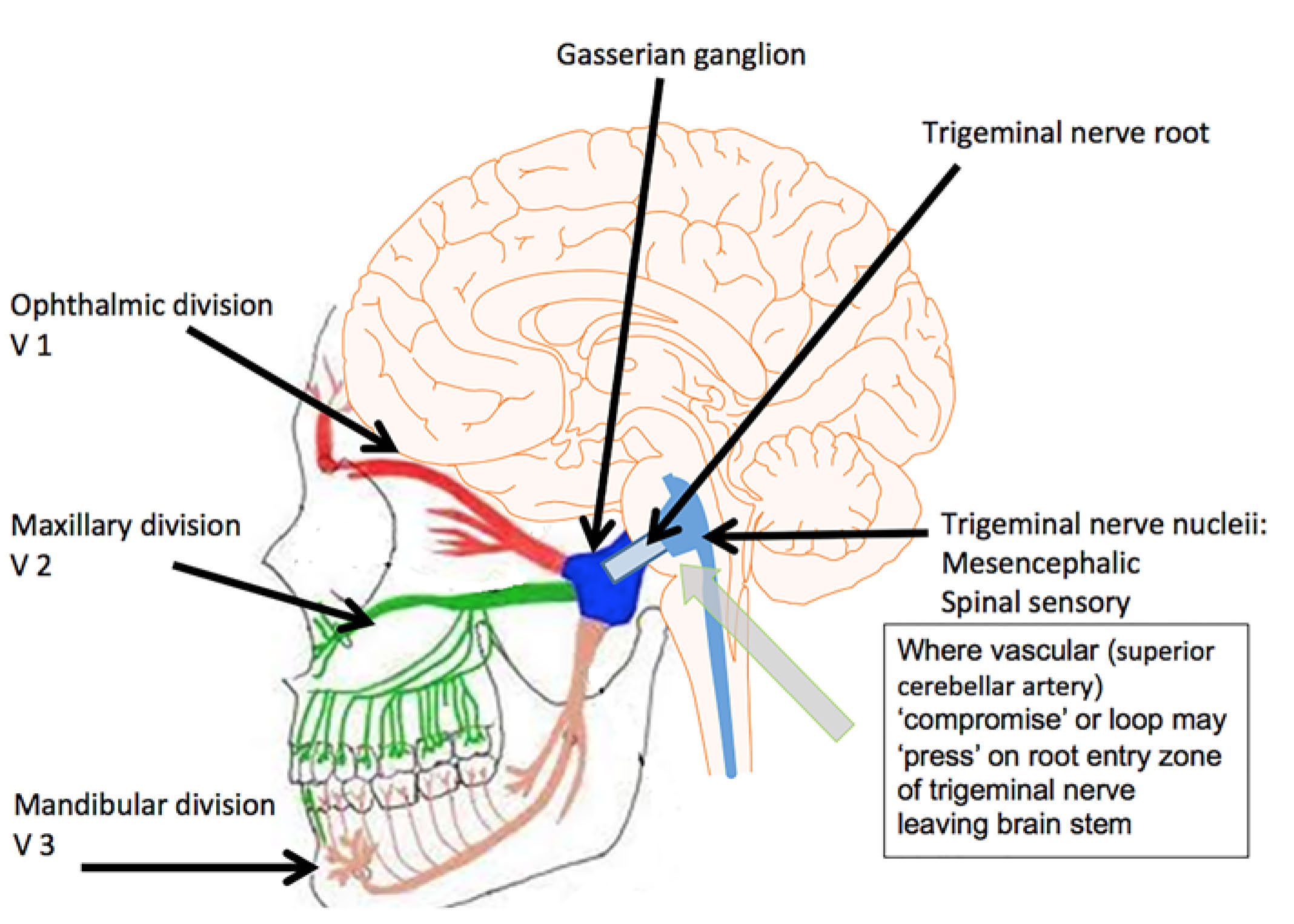
In most TN cases, there is an identifiable compression of the trigeminal nerve root (Figures 1 and 2), which is usually within a few millimetres of the nerve entry into the pons, so called root entry zone.6 Most commonly, this compression is due to of the superior cerebellar artery or vein (Figures 2 and 3). It was first described by Jannetta in 1967 and is thought to account for 80–90% of cases.7 Indeed, results from a recent animal study indicated that mechanical compression of the trigeminal nerve root induced facial pain behaviour in rats.8
Figure 1. Diagrammatic representation of the vascular compromise of the trigeminal root emerging from the brain stem.Figure 2.
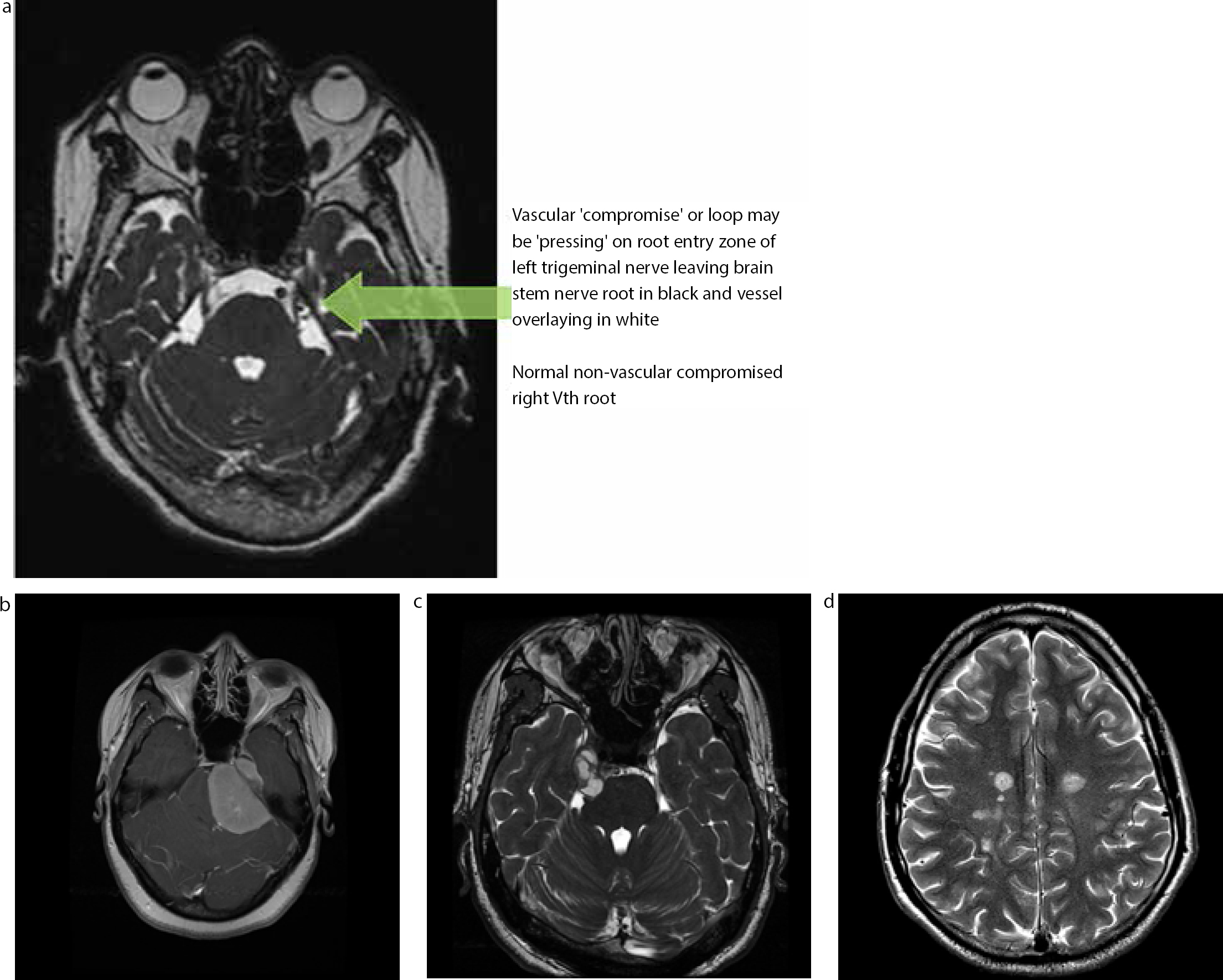
(a) Magnetic Resonance Imaging (MRI) illustrating vascular compromise of the trigeminal root. (b) MRI illustrating the petrous apex meningioma presenting with trigeminal neuralgia symptoms. (c) MRI illustrating trigeminal schwannoma presenting with trigeminal neuralgia symptoms. (d) MRI illustrating demyelination due possibly to MS, presenting with trigeminal neuralgia symptoms.Figure 3.
(a) Diagrammatic representation of microvascular decompression (MVD): TS – transverse sinus; SI – surgical incision; SS – sigmoid sinus; M – mastoid process; DG – digastric groove. (b) Microvascular decompression of the trigeminal root exiting the brain stem: non-compressive tributary of the superior petrosal vein before division (green arrow); right trigeminal nerve (blue arrow); branch of superior cerebellar artery passing medially to the trigeminal nerve (red arrows). (c) Microvascular decompression of the trigeminal root exiting the brain stem: retracted superior petrosal vein (green arrow); reveals point of compression of the trigeminal nerve by a branch of the superior cerebellar artery (red arrow) passing medially to the nerve.(d) Microvascular decompression of the trigeminal root exiting the brain stem: remnants of superior petrosal vein after cauterization and division (green arrow); decompressed trigeminal nerve (blue arrow); multiple Teflon (PTFE) grafts interposed between branch of superior cerebellar artery and trigeminal nerve (asterisks). (e) View of right retromastoid craniotomy: relaxed cerebellum after opening of cisterna magna (not seen) and drainage of CSF (green arrow); tentorium cerebelli (blue arrow); petrous bone (trigeminal nerve in this direction) (red arrow).
Other compressive lesions include vestibular schwannomas, meningiomas and various other tumours and cysts.6 In the long term this compression can cause demyelination and later remyelination of the nerve.6
Neuralgia pain can also be caused by nerve damage due to multiple sclerosis, if demyelination plaques involve the root entry zone. Accordingly, when investigating this condition these differential diagnoses must be considered and explicit request of the neuroradiologist for the MRI scan should include:
Exclusion of space occupying lesions;
Vascular compromise of Vth nerve root (right or left); and
Demyelination.
If gadolinium contrast medium is required, a recent renal profile is needed to estimate the glomerular filtration rate.
Clinical features and classification
The International Association for the Study of Pain has defined TN as ‘a sudden, usually unilateral, severe, brief, stabbing, recurrent pain in the distribution of one or more branches of the fifth cranial nerve’.9
TN is classified by the International Headache Society as ‘classical’ TN and ‘symptomatic’ (secondary) TN. In classical TN, no obvious cause can be found, other than possible trigeminal nerve compression by a blood vessel. However, in symptomatic TN, pain is caused by a benign or malignant tumour or a disease such as multiple sclerosis. Classical TN has diagnostic criteria suggested by the International Headache Society (Table 1). However, not all patients can fulfil these criteria. Therefore the term of ‘atypical’ or Type II TN is used for these patients.10
Paroxysmal attacks of facial or frontal pain, lasting from few seconds up to 2 minutes
At least 4 of the following characteristics are fulfilled:
Pain is distributed in one or more divisions of the trigeminal nerve
Sudden, intense, sharp, stabbing, superficial or burning quality
Severe intensity
Presence of trigger areas or pain can be provoked by daily activities such as talking, eating, washing the face, or brushing the teeth
Symptom-free periods between pain attacks
No neurological deficit
Pain attacks are stereotyped in individual patients
Other causes of facial pain are excluded by history, physical examination and special investigations, if required
It has been found that TN most commonly affects the maxillary or mandibular divisions of the trigeminal nerve; however, it is possible that more than one division is involved.11 The ophthalmic branch on its own is very rarely affected,1 and it is suggested that pain in the ophthalmic division only is more likely to be caused by trigeminal autonomic cephalalgia rather than TN.12 The right side of the face seems to be more often affected than the left side.11 Bilateral involvement is possible, though very rare, and often does not occur at the same time.1,11
The onset of TN is usually spontaneous; however, some patients associate it with toothache or dental treatment.13 This could be due to the fact that often TN affects the lower or mid-face region and can be mistaken for dental origin pain. It is not unusual for TN patients to have dental treatment, including root canal treatment and even extractions, before the diagnosis of TN is decided and neurosurgeons claim it can be as high as 60%.10
The pain attack starts suddenly and lasts from a few seconds to up to a few minutes.13 However, owing to the severity of the pain, it is difficult for patients to appreciate how long the pain attack lasts and to notice if there are any breaks between pain attacks. Classical TN patients are completely pain-free in between the pain attacks. However, patients with atypical TN may experience mild ache or burning background pain lasting from 30 minutes to a few hours afterwards.12 Atypical TN is diagnosed if a patient has background pain present for over 50% of the time.13 During the pain episodes the patient may have several pain attacks a day. The median length of a pain episode is about 50 days; however, it may range from one to 1,462 days.1 A small percentage of classical TN patients suffer daily pain, however, the majority experience pain-free intervals lasting from a few days even up to a few years.13
Regarding the character of pain, most patients report ‘shooting’, ‘lancinating’ or ‘cutting’ pain,14 but patients may also report less sharp pain qualities.10 It is important to listen to how patients describe their pain. The narratives used may include: ‘ice-pick’, ‘shock’, ‘electric shock-like’, ‘shooting jolts of electricity’, ‘hot knife stabbing’.15 Pain attacks may be provoked by chewing, talking, touching the face or cold. Fifty per cent of patients have noticed trigger zones, where light touch can provoke pain. These can be intra- or extra-oral triggers.16
Diagnosis and differential diagnosis
There are no objective tests available to diagnose TN. Even the criteria suggested by the International Headache Society have not been validated by comparison with other types of facial pain.10 Therefore, a good pain history is essential, and the patient's own pain description can be indicative of TN.17
A review of the past medical history and thorough examination of cranial nerves is important to exclude symptomatic TN. Nowadays magnetic resonance imaging (MRI) is usually performed in all TN patients to diagnose symptomatic TN and determine whether there is a compression of the trigeminal nerve by a blood vessel. Rarely, neurophysiological tests are performed to help to differentiate classical TN from symptomatic TN.17
Through the pain history, including questions about autonomic features (such as ipsilateral facial blushing and sweating, redness and tearing of the ipsilateral eye, watery discharge from the ipsilateral nostril) can also help to differentiate TN from trigeminal autonomic cephalalgias. It is essential to exclude the diagnosis of trigeminal autonomic cephalalgias (covered in a separate section), which often present with neuralgic symptoms within the trigeminal system but with concomitant autonomic signs. In addition, many medical practitioners are ill-equipped to differentiate TN from toothache, whereas the patient's dentist is able to clarify this early. Post traumatic neuropathy may also ‘mimic’ TN with mechanical allodynia (elicited pain on touch) in the trigeminal distribution, however, a concomitant neuropathy (numb, paraesthetic area) and a history of recent surgical intervention will differentiate post traumatic neuropathy (covered in another section of this series) from TN. Other differential diagnoses include dental origin pain, temporomandibular disorder, trigeminal neuropathic pain and chronic facial pain. Therefore, a good pain history is crucial. The dentist plays an important role in diagnosing TN by excluding dental origin pain, such as pulpitis, and they are often the first healthcare professional to see them. It is often more difficult to diagnose in the early stages as Drangsholt and Truelove have shown.17
Pain impact
TN is a debilitating facial pain condition that often significantly affects a patient's quality of life. As it is often misdiagnosed,4 patients may not receive the appropriate treatment in time. Patients may undergo unnecessary, costly and invasive dental treatment,10 or even surgical procedures to the maxillary sinus or temporomandibular joint. Even after the correct diagnosis is made, patients may still suffer significant distress.18 Patients often suffer from depression, which can be improved after successful surgical treatment of TN.12 Patients often feel they live in isolation with their pain and feel depressed and fearful that pain may increase. One patient described daily life: ‘I spend my waking hours trying to overdose, screaming and crying for relief. Emotions? Suicidal at worst and depressed at best.'16 Even patients who are in remission may remain anxious and stressed that pain may recur or the treatment may stop working.18
Management
There are several medical and surgical methods available for management of TN. Although TN is considered to be a manageable pain condition, the treatment can be challenging and not always completely successful. It has been recommended that once carbamazepine, the first line drug, is no longer effective, patients should be referred to the secondary care sector. Departments that see these patients include oral medicine, oral and maxillofacial surgery, headache neurology, pain clinics and some neurosurgery clinics. The Trigeminal Neuralgia Association, a support group for patients, can provide advice based on the experiences of their members. They also have a list of professionals in different areas on their website.
Medical management
There are several Cochrane systematic reviews and practice guidelines available outlining pharmacological management of TN.19 Unfortunately, there are only a few high-quality, randomized, controlled trials published, and most of the studies are small and from a single centre research.
First line medications
For many years carbamazepine has been considered the gold standard treatment for TN symptoms.20 It can be very effective and may provide complete pain relief within days. In the British National Formulary (BNF) carbamazepine is currently the only drug licensed for the treatment of TN and can be prescribed by dentists. Owing to possible severe side-effects, it should be initially prescribed at a low dose and gradually increased up to therapeutic level. Prior to prescribing carbamazepine, a patient's medical and drug history must be updated as carbamazepine interacts with several other medications. Possible interactions should be checked with the most recent edition of BNF. Common side-effects include drowsiness, dizziness, constipation and abdominal discomfort; however, it can cause serious neurological, hepatic and haematological side-effects as well as electrolyte disturbance.18 Therefore, it is advisable to monitor full blood count, renal and liver profile.
Second line medications
Oxcarbazepine has been suggested as a second line treatment for TN symptoms. Although there is consensus that it is an effective treatment for TN,20 it is not licensed for management of TN. Oxcarbazepine does not use a liver cytochrome system, therefore it seems to be better tolerated than carbamazepine.21 However, there could be allergic cross-reactions between these drugs.
Lamotrigine is often used in patients who are unable to tolerate carbamazepine, however, it has to be increased slowly to avoid side-effects, therefore its use in acute TN is limited.20 There is consensus that baclofen can be effective in the treatment of symptomatic TN.20 Other drugs occasionally used for the treatment of TN include phenytoin, clonazepam, sodium valproate, gabapentin, pregabalin and topimarate. All these medications have to be used with caution as they all can cause serious side-effects (Table 2).
Can be combined with carbamazepine, beware doses above 300 mg daily as can cause significant adverse events
Sodium valproate
No
600–1200 mg
Abdominal discomfort, weight gain, thrombocytopenia, hepatic and neurological disturbance
Check liver function before prescribing.Monitor full blood count, liver and renal function
Pregablin
No
300–600 mg
Drowsiness, tiredness
One long-term cohort study had positive results
Surgical management
Decision if and when the patient needs a surgical treatment for the TN is not easy to make. Currently, there are no clear guidelines which may assist clinicians with this decision as there is insufficient evidence suggesting at what point during TN clinical course a surgical intervention should be undertaken.22 However, it has been suggested that patients with TN poorly controlled with medications may prefer a surgical treatment early.22 It has been suggested that a surgical treatment option should be discussed with a neurosurgeon early, preferably when the patient is not in acute pain, as later the patient's cognitive function might be affected by pain or medications, which would affect the process of gaining informed consent.12 Furthermore, there is strong evidence showing some degree of cognitive impairment in patients suffering from chronic pain.23
There are several surgical treatment options available (Table 3). They could be divided into three groups, depending on the targeted level of the trigeminal nerve:
Peripheral level – distally to the Gasserian ganglion (eg procedures to infra-orbital and inferior dental nerves);
Base of skull level – Gasserian ganglion procedures;
Intracranial level – posterior fossa operations to the root entry zone.
Up to 50% suffer temporary or permanent masticatory problems after balloon inflation
Intracranial operations:
■ Gamma knife surgery
69% pain free after 1 year, 52% after 3 years
Nil
9-37% some facial numbness, 6-13% troublesome sensory loss and paraesthesias
Pain relief can be delayed
■ Microvascular decompression
90% pain relief, 73% pain free after 10 years
0.2-1%
4% major problems (CSF leaks, infarct, haematoma), 11% aseptic meningitis, 7% sensory loss, 10% ipsilateral hearing loss
Major neurosurgical procedureMorbidity is lowest in high volume unitsVery high satisfaction
Peripheral interventions
These techniques involve the blocking or destruction of trigeminal nerve branches distally to the Gasserian ganglion, such as cryotherapy, neurectomy, radiofrequency thermocoagulation, alcohol injection, phenol injection or peripheral acupunture. Although morbidity associated with these procedures is low, 50% of patient experience recurrence of pain within one year.22
Gasserian ganglion procedures
These techniques involve percutaneous cannulation of foramen ovale and damaging the trigeminal ganglion or root with temperature (radiofrequency thermocoagulation), chemicals (glycerol injection) or mechanical compression (balloon inflation). These procedures have extremely low mortality, but morbidity is higher than with peripheral techniques. A small percentage of patients develop troublesome dysaesthesia or corneal numbness. About 12% of patients suffer post-operative discomfort, such as burning and aching.22 About 90% of patients experience immediate pain relief, and 68–85% are pain free after one year. At 5 years, 50% of patients after radiofrequency thermocoagulation are pain free.22
Intracranial operations
These techniques are focused on the trigeminal root in the posterior fossa. Gamma knife surgery is currently the only non-invasive technique. It aims a focused beam of radiation at the trigeminal nerve root. There is a delay between the procedure and pain control, and patients may need to wait several weeks or months for complete pain relief, but 55–97% of patients will achieve satisfactory pain relief.24 Unfortunately, the recurrence of pain is common, and about 52% are pain free after 3 years.22 Common complications involve delayed facial numbness21 and troublesome sensory loss and paraesthesias. Nevertheless, 88% of patients are satisfied with treatment outcome.22
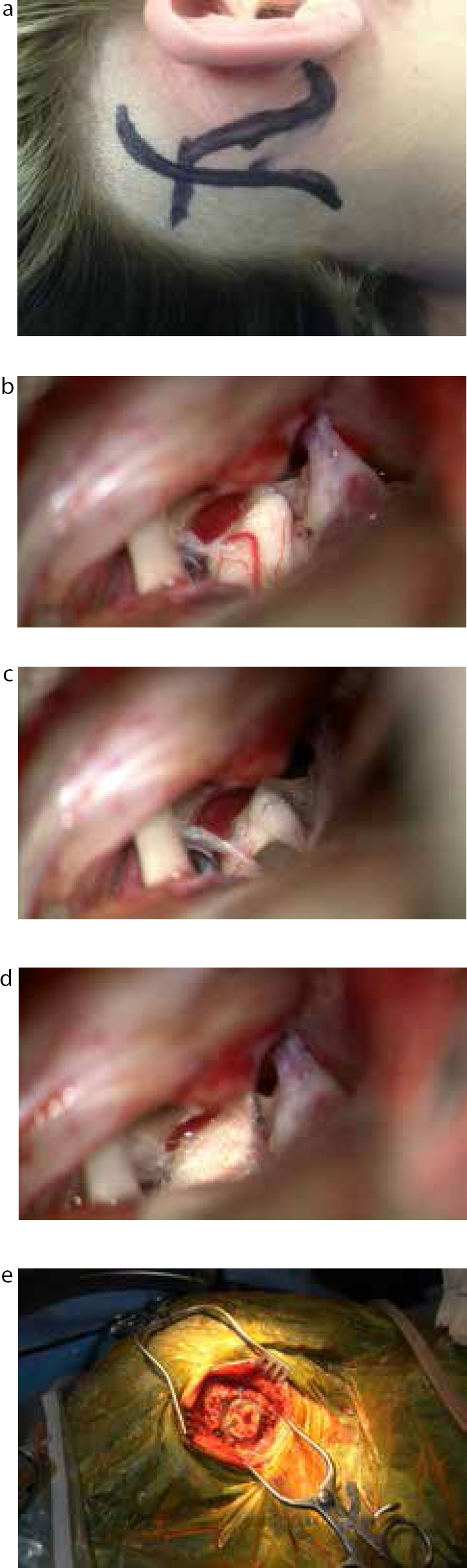
Microvascular decompression (MVD) is the preferred surgical option, if the patient is fit enough, when medical management is ineffective. MVD is a major neurosurgical operation that involves craniotomy to identify and isolate the vessels compressing the trigeminal nerve accessed via the mastoid (Figure 4). This procedure aims to preserve the trigeminal nerve. Ninety percent of patients achieve pain relief, and about 73% are still pain free after 5 years.22 Patients with classical TN have better long-term pain relief than patients with atypical TN (76% vs 56% being pain free at 10 years, respectively).25 Mortality is estimated at 0.2–0.5%, which is low,22 but it rises up to 1% for patients over 75 years.25 Postoperative complications can be serious – 4% have cerebrospinal fluid leak, infarcts or haematomas, but 11% have aseptic meningitis. Sensory loss occurs in 7%, but up to 10% may experience ipsilateral hearing loss.22
Figure 4.
(a) Incision for MVD. (b) Left Vth nerve compressed. (c) Groove in left Vth nerve where vessel released. (d) Left Vth nerve decompressed with PTFE. (e) Closure of bur hole access post auricular with bone graft.
There are now support groups for TN patients available, such as Trigeminal Neuralgia Association UK. They organize regular conferences, where patients can gain more knowledge about their condition and available treatment options, as well as meet other patients with the same diagnosis and healthcare professionals with particular interest in TN. There is also written information available to improve patients' understanding of their condition and to help them to cope with living with pain (Table 4).
Patient support group in the UK
Written information for patients
Trigeminal Neuralgia Association UK PO Box 234, Oxted RH8 8BE, UK http://www.tna.org.uk
Weigel G. Striking BackTrigeminal Neuralgia Association Gainesville, Florida, 2000
Zakrzewska JM. Insight Facts and Stories behind Trigeminal NeuralgiaTrigeminal Neuralgia Association, Gainesville, Florida, 2006
Information also available on TNA UK website http://www.tna.org.uk
Brain and spine foundation booklet on face pain Available on http://www.brainandspine.org.ukISBN 978-1-901893-60-1
Summary
Although TN is a rare severe chronic facial pain disorder, characterized by usually unilateral, sudden, brief, subbing, severe, recurrent pain attacks in the distribution area of one or more branches of the trigeminal nerve, one of the pressing issues regarding its diagnosis is that general medical practitioners may often mistake common toothache for TN and thus treat patients inappropriately with antepileptic drugs. The diagnosis, in which the dentist plays a key and important role, is clinically based on a thorough pain history and clinical examination. MRI is usually performed to exclude symptomatic TN and to determine possible nerve compression by a vessel. It is essential that the TN diagnosis is clear and not confused with some trigeminal autonomic cephalalgias. Previous confusion may explain the poor response to medical and surgical treatments for presumed TN.
There are different medical and surgical treatments available, with microvascular decompression having the highest success rate. Owing to the debilitating effect on a patient's quality of life, it is important to have multidisciplinary team management, including support from clinical psychologists. There are TN patient support groups available to help patients better understand and cope with their condition.