Mouth cancer for clinicians part 7: cancer diagnosis and pre-treatment preparation Nicholas Kalavrezos Crispian Scully Dental Update 2024 43:1, 707-709.
Authors
NicholasKalavrezos
FRCS, FFD RCSI, MD
Consultant in Head and Neck/Reconstructive Surgery, Head and Neck Centre, University College London Hospitals, London, UK
A MEDLINE search early in 2015 revealed more than 250,000 papers on head and neck cancer; over 100,000 on oral cancer; and over 60,000 on mouth cancer. Not all publications contain robust evidence. We endeavour to encapsulate the most important of the latest information and advances now employed in practice, in a form comprehensible to healthcare workers, patients and their carers. This series offers the primary care dental team in particular, an overview of the aetiopathogenesis, prevention, diagnosis and multidisciplinary care of mouth cancer, the functional and psychosocial implications, and minimization of the impact on the quality of life of patient and family.
Clinical Relevance: This article offers the dental team an overview of diagnosis, diagnostic and pre-treatment procedures.
Article
Nicholas Kalavrezos Professor Crispian Scully
Mouth cancer theoretically should be largely preventable or detectable at an early stage. Dental training equips dentists and other dental clinicians with the best way to diagnose oral disease and the importance of the history and examination are stressed in training. The General Dental Council (GDC) recommendations for Continuing Professional Development (CPD) have long included medical emergencies, disinfection and decontamination and radiography and protection safety but, after pressure from us and others, the GDC have now added oral cancer early detection, along with legal and ethical issues, and complaints handling. There is evidence that education helps diagnostic outcomes not only of oral but also orofacial disease (Figure 1). Nevertheless, one US study showed that the diagnosis of oral lesions by dentists and dental specialists was incorrect in over 40% of cases, and over 5% of cancers were misdiagnosed.
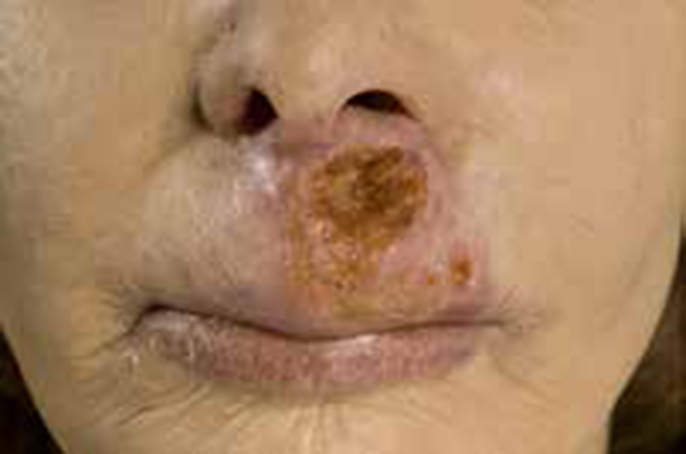
Figure 1. Basal cell carcinoma of skin.
In the UK, only 25.2% of GMPs but 54.1% of GDPs in one study felt that they had sufficient knowledge regarding detection and prevention of mouth cancer. Failure to diagnose oral cancer has led to GDC disciplinary action in the UK and already is the second highest cause of dental malpractice in the USA.
Diagnosis
Clinical diagnosis of an early cancer can be quite straightforward if the clinician has adequate level of awareness and suspicion, but potentally malignant disorders (PMDs) that are likely to transform are far more difficult to decide upon. Lesions in ‘high risk’ patient groups (Article 2) should be regarded with especial care but it is dangerous not to consider a diagnosis of cancer just because a patient is apparently not in such a ‘risk group’.
Why is early cancer diagnosis important?
Early diagnosis of mouth cancer is important mainly in order to improve the prognosis and minimize the adverse effects of treatment. Early, localized tumours with no spread to the cervical lymph nodes can be effectively treated and cured, with 5-year survival rates around 80%. When cervical lymph nodes are involved, 5-year survival falls to less than 20%.
Delayed diagnosis may also result in poor quality of life, mainly from maxillofacial deformity, disturbances in speech, mastication and swallowing. There is often still a mean delay of around 3 months during the cancer journey. Delays are associated with up to a 3-fold increase in mortality.
Diagnostic delays
Patients may delay seeking professional advice after having become aware of any oral symptom that could be linked to oral cancer, and diagnosis is often delayed by up to 6 months, even in developed countries, despite exhortations over the past 25 years to increase the index of suspicion. Delays are common in many different countries but are generally longer in:
Heavy smokers;
Heavy alcohol drinkers;
People of lower socio-economic status (SES);
Males.
The reason for a patient to be diagnosed with advanced disease can be related to delays in recognition of the disease, delayed referral to the appropriate healthcare worker, or to system delays. Late stage diagnosis is mainly because of a lack of patient awareness related to socio-economic status/education or cognitive function, rather than because mouth cancer is hard to discover. Many patients think that their symptoms of many diseases are trivial, will get better by themselves and give little thought as to whether it might be serious. Patients frequently know little or nothing about the disease.
Nevertheless, healthcare systems should endeavour to minimize delays, which may include the patient's delay in seeking medical care, limited access to a doctor or a dentist, misdiagnosis in primary care, referral delays, or mismanagement in diagnosing and treating the patient once he/she attends the referral centre. Simple, clear, fail-safe, fast-track referral schemes may diminish the delay. The identification of a ‘scheduling delay’ in mouth cancer justifies additional educational interventions aimed at the whole healthcare team as well as at dental and medical practices.
Diagnostic delays in primary care account for a minority of these cases but are potentially modifiable. Clinicians need to be aware of several different factors when assessing the risk for oral cancer, including the changing epidemiology of mouth cancer, the role of HPV and new trends in tobacco consumption, for example the increasing use of waterpipes.
Opportunistic screenings would yield earlier discovery by healthcare professionals. Dental practitioners and dental care professionals should remain vigilant for signs of PMD and oral cancer whilst performing routine oral examinations.
What is involved in clinical diagnosis?
Dental clinicians are all trained in careful inspection, examination and palpation of all the oral tissues – Conventional Oral Examination (COE) – and regional (cervical) lymph nodes. The steps in this are illustrated in Figures 2–9.
Figure 2. Examination of buccal mucosa. (Courtesy of Dr Y Hassoneh.)Figure 3. Examination of right ventral tongue mucosa. (Courtesy of Dr Y Hassoneh.)Figure 4. Examination of left tongue ventrum mucosa. (Courtesy of Dr Y Hassoneh.)Figure 5. Examination of left lingual mucosa. (Courtesy of Dr Y Hassoneh.)Figure 6. Examination of the labial mucosa. (Courtesy of Dr Y Hassoneh.)Figure 7. Examination of submental lymph nodes. (Courtesy of Dr Y Hassoneh.)Figure 8. Examination of submandibular lymph nodes. (Courtesy of Dr Y Hassoneh.)Figure 9. Examination of cervical lymph nodes. (Courtesy of Dr Y Hassoneh.)
What features are suggestive of mouth cancer?
Early mouth cancer, such as oral squamous cell carcinoma (OSCC), may be symptomless, with no pain or other symptoms. The patient may eventually notice mild symptoms, such as a persistent lesion or ulcer that does not heal within a couple of weeks. Figures 10–21 illustrate the range of clinical appearances of OSCC.
Figure 10. Lip cancer – advanced.Figure 11. Lip cancer.Figure 12. Lip cancer early ulcerated lesion.Figure 13. Early lip cancer.Figure 14. Lingual carcinoma – advanced.Figure 15. OSCC: classical ulcerated lump on lateral tongue.Figure 16. OSCC: earlier ulcerated lesion close to foliate papillae.Figure 17. Early ulcerated lesions: carcinoma in palate. (Courtesy of Scully C et al. Atlas of Oral and Maxillofacial Diseases 3rd edn. London: Informa, 2004.)Figure 18. OSCC: early lesion that has not ulcerated.Figure 19. OSCC: advanced gingival carcinoma.Figure 20. Gingival leukoplakia and carcinoma.Figure 21. OSCC.
Any single lesion that cannot be wiped off the mucosa and persists more than 3 weeks, particularly if Red, Ulcerated or a Lump, Especially with induration (a firmness on palpation) – the acronym RULE – should be regarded with suspicion and a histopathological diagnosis established by biopsy examination.
Other features that may be suggestive of OSCC are any persistent:
Red lesion (erythroplasia or erythroplakia);
Mixed red/white lesion (erythroleukoplakia);
Nodular white lesion (verrucous leukoplakia);
Lump;
Ulcer with fissuring or raised exophytic margins;
Pain or numbness;
Abnormal blood vessels supplying a lump;
Loose tooth;
Extraction socket not healing;
Induration, ie a firm infiltration beneath the lesion;
Fixation of lesion to deeper tissues or to overlying skin or mucosa;
Regional lymph node enlargement;
Dysphagia;
Weight loss.
If any of these changes are noticed, help should be sought from a dentist, doctor, or another healthcare professional without delay. The dentist is usually the person best trained in early diagnosis of mouth issues.
However, early lesions can lack these warning features. Characteristics of oral cancer in the asymptomatic early lesion (after Mashberg and Samit) include:
Granular or smooth surface 82%;
No elevation (with <1 mm) 80%;
No ulceration 85%;
No bleeding 98%;
No induration 90%.
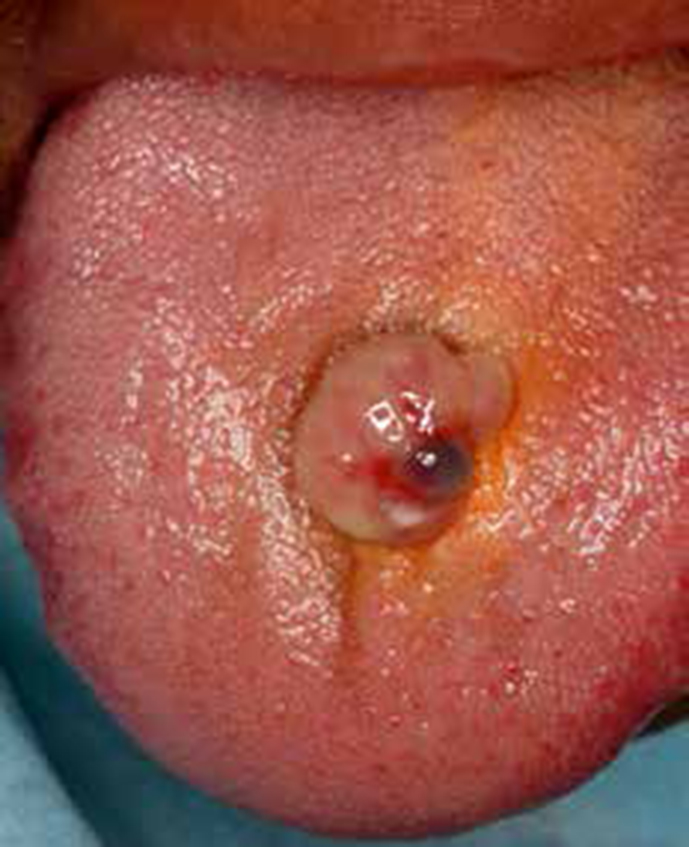
Other lesions can mimic carcinoma. Occasionally, pyogenic granulomas (Figure 22) or similar less serious lesions can clinically and histologically mimic OSCC (eg necrotizing sialometaplasia (Figure 23) or Traumatic ulcerative granuloma with stromal eosinophilia (TUGSE) (Figure 24) – benign lesions of unclear pathogeneses). The main differential diagnoses for OSCC include PMD; other malignant diseases such as lymphomas, sarcomas and metastases, which grow rapidly as opposed to a typical OSCC; salivary neoplasms (Figure 25); and chronic infections, such as syphilis, tuberculosis, or histoplasmosis.
It should also be noted that clinically differentiating PMD and OSCC from benign lesions can be taxing, even for highly trained professionals. Not uncommonly, PMD and OSCC are asymptomatic, and appear innocuous and some can be overlooked. Thus fewer than 27% of leukoplakias, a common PMD, are ever subjected to biopsy. As discussed above, even biopsy can leave cancers undetected in PMD.
As a result, some OSCC must surely mistakenly remain untreated and be left to progress to more advanced stages or cancer. A high index of suspicion is clearly indicated.
What are essential for diagnosis?
Dental practitioners and dental care professionals should always be vigilant for signs of potentially malignant disorders (PMD) and mouth cancer whilst performing routine oral examinations. Red, white, ulcerated lesions or lumps are the common presentations of OSCC. A high index for suspicion is warranted. Red oral lesions usually are more dangerous than white oral lesions. Diagnosis is from these clinical features, always supported by biopsy.
What are the essentials of physical examination?
Dental practitioners and some other clinical dental care professionals are trained in the examination (inspection and palpation) of the mouth. Dentists are trained to spot early signs of mouth cancer and can easily examine with a good dental light, dental mirror and good retraction, parts of the mouth difficult for the person or others to see, so annual examinations by a dentist, even if the person is edentulous, are advised.
All areas should be scrutinized using a good light and retraction and these are best available in a dental office. Lesions always must be palpated after inspection to detect induration and fixation to deeper tissues. Examine the entire mucosa because widespread dysplastic mucosa (field change) or a second neoplasm (see ‘Staging’) may be present. Carefully record the location of suspicious lesions, preferably on a standard topographic diagram.
As recommended (Ogden, 2013), ‘The screening of all oral mucosal surfaces should be carried out (and recorded) every time a patient attends and be practice policy (and open to audit to ensure it's done). Dentists and DCPs should identify patients who are at increased risk of mouth cancer. One way is through the use of medical history sheets that include lifestyle questions.'
Therefore, to increase the chance of early diagnosis, it is important for yearly examinations to be carried out by a clinical dental professional. The patient should be aware of what is normal for them, keep an eye out for any changes, and seek advice from a dentist or clinical dental professional or GMP if they suspect anything out of the ordinary.
Early referral to a specialist with oral surgery or oral medicine competence is advised.
Bear in mind that:
A typical malignant ulcer is hard with heaped-up and often everted or rolled edges and a granular floor.
The most common sites of mouth cancer include the lower lip, the lateral margin of the tongue, and the floor of the mouth.
Most lip cancers manifest on the lower lip at the mucocutaneous junction as a chronic small lump, ulcer, or scabbed lesion.
Intra-oral cancer can have a highly variable clinical appearance – mainly a red or white area, ulcer, lump or fissure:
- Most intra-oral cancers manifest on the middle third of the lateral margins of the tongue with an erythroplastic component and, sometimes, induration;
- Late tongue cancer may manifest as an exophytic lesion, an ulcer, or an area of superficial ulceration with induration;
- The sump area or ‘coffin corner’ at the posterior tongue/floor of the mouth is a common site for cancer but may be missed by cursory inspection; special care is needed to ensure close examination;
- The floor of the mouth is the second most common intra-oral site for cancer and more commonly is associated with leukoplakia. Most cancer arises in the anterior floor of the mouth as an indurated mass that soon ulcerates, resulting in slurring of speech;
- Carcinomas of the alveolus or gingiva are mostly seen in the mandibular premolar and molar regions, usually as a lump (epulis) or ulcer. The underlying alveolar bone is invaded in 50% of cases, even in the absence of radiographic changes, and adjacent teeth may be loose;
- Carcinomas of the buccal mucosa are mostly seen at the commissure or in the retromolar area. Most are ulcerated lumps, and some arise in candidal leukoplakias;
- Carcinomas can affect the palate or elsewhere.
Examine the teeth and periodontium in good lighting: advanced caries, periodontal disease, or periapical lesions may need early attention, especially if radiotherapy is to be used in management of a tumour.
The presenting features of mouth cancer usually relate to local effects of the primary tumour, and only occasionally to regional spread, metastatic disease, or paraneoplastic phenomena.
What are the latest oral diagnostic methods?
A Conventional Oral Examination (COE) with white light (‘incandescent light’) (visual and palpation examination) as above, still constitutes the gold standard for the diagnosis of oral pre-cancer and cancer. There is no doubt that clinician education improves the diagnostic skills and that experience counts.
However, a range of potential diagnostic aids is appearing on the market, or in the literature, and these include:
Vital (toluidine blue) staining;
Exfoliative cytology/brush biopsy;
Autofluorescence spectroscopy/imaging;
Chemiluminescent illumination;
Narrow band imaging;
Confocal microscopy.
Analysis of the evidence thus far of the adequacy of diagnostic aids has shown that there is insufficient evidence that:
Commercial devices based on autofluorescence enhance visual detection beyond a conventional visual and tactile examination;
Commercial devices based on tissue reflectance enhance visual detection beyond a conventional visual and tactile examination;
Transepithelial cytology can assess the validity of seemingly innocuous mucosal lesions.
Vital (toluidine blue) staining
Vital staining using the dye toluidine (tolonium) blue has been available for at least 50 years but is insufficiently specific or sensitive, a problem faced by virtually all such ‘aids’.
Toluidine blue staining in future may prove useful if combined with molecular studies (Article 2), which have shown:
Low malignant risk – heterozygosity for chromosome 9p;
Intermediate risk – LOH for 9p alone or LOH 9p plus either LOH for 17p or LOH for 4q;
High risk – LOH for 9p, 17p, and 4q.
Exfoliative cytology/brush biopsy
This technique of transepithelial cytology is also insufficiently specific or sensitive but in future may be used with modern techniques, such as DNA Image Cytometry (DNA-ICM), DNA analysis (aneuploidy), MALDI-ToF MS (Matrix-Assisted Laser Desorption/Ionization Time of Flight Mass Spectrometry) or Peptidome profiling.
Autofluorescence spectroscopy/imaging
Autofluorescence spectroscopy/imaging is available as, for example:
Early studies suggest promise in this area but, meantime, until the evidence base improves, Conventional Oral Examination (COE) plus biopsy, despite limitations, remains the gold standard.
What about cancer screening?
Cancer screening means testing people for early signs of cancer before they show any symptoms. At first sight it sounds an excellent and attractive proposition. However, an effective and accurate test is needed, reliable at detecting cancers but not giving false positive results in people who have no cancer, nor false negative results when cancer is present.
Screening can also be expensive; it is most cost-effective to screen people who have an increased (high) risk of developing cancer (typically older people of low SES with exposure to known cancer risk factors), but of course it is often those groups who do not avail themselves of the opportunities for early detection.
There is therefore currently no UK national screening programme for mouth cancer because these cancers are also uncommon and the Cochrane Library (2010) determined that currently there is insufficient evidence to show that a screening programme for mouth cancer can help detect mouth cancers earlier, and concluded that there is insufficient evidence to recommend screening of the general population for OSCC, either by using visual examination or adjunctive tools (eg toluidine blue, brush biopsy, fluorescence imaging) to decrease mortality. Those authors recommended regular screening by visual inspection by qualified healthcare providers for high-risk groups.
In a recent study, high-risk groups with tongue OSCC were being:
Age >80;
Widowed;
Socially marginalized;
A current smoker; or
A smoker-heavy drinker.
Risk factors in people with floor of mouth cancer were being:
Age >70; and
Socially marginalized.
Having a regular dentist was protective.
Where does mouth cancer spread?
OSCC predominantly metastasizes locally and to draining regional lymph nodes, primarily in the anterior neck. Mouth cancer often spreads to the submental and submandibular nodes. It spreads by haematogenous dissemination only late in its natural history. Extra-oral examination must therefore include cervical lymph node examination; most enlarged nodes are palpable but not visible on inspection alone.
A painless enlarged cervical lymph node may be the only presenting symptom and from 30–80% of patients with OSCC have metastases in the cervical lymph nodes at presentation, though few are as visible as shown here, which is more typical of oropharyngeal carcinoma (Figure 27).
Figure 27. Cervical lymphadenopathy.
Memorial Sloan-Kettering Cancer Center, USA developed the most widely used lymph node regional definitions. To describe the neck lymph nodes (for neck dissection to remove nodes with metastases), the neck is divided into six areas or levels, identified by Roman numerals, increasing towards the chest (Table 1).
I
Submental and submandibular triangles bounded by the posterior belly of the digastric muscle, hyoid bone inferiorly and body of mandible superiorly
II
Upper jugular lymph nodes and extends from the level of the hyoid bone inferiorly to skull base superiorly
III
Middle jugular lymph nodes from hyoid bone superiorly to cricothyroid membrane inferiorly
IV
Lower jugular lymph nodes from cricothyroid membrane superiorly to clavicle inferiorly
V
Posterior triangle lymph nodes bounded by anterior border of trapezius posteriorly, posterior border of sternocleidomastoid anteriorly and the clavicle inferiorly
VI
Anterior compartment lymph nodes from hyoid bone superiorly to suprasternal notch inferiorly. On each side the lateral border is formed by medial border of carotid sheath.
A systematic and thorough examination of the cervical lymph nodes, mouth and fauces must be performed by a clinician trained in the diagnosis of oral diseases, and a general physical examination is indicated.
Metastatic cancer most often involves the lung. Bone and liver involvement is much less common. Rarely, paraneoplastic phenomena can become evident in advanced disease stages, most commonly hypercalcaemia resulting from elaboration of a parathyroid hormone–like peptide.
What investigations may be indicated?
The diagnosis is often arrived at by a biopsy from the primary lesion or site. The principles are to:
Confirm the cancer diagnosis histopathologically;
Determine if there is malignant disease elsewhere:
-Locally (eg invasion of bone, muscles or cervical regional lymph nodes); Metastases, which initially are to cervical lymph nodes and later to liver, lungs, bone and brain. Imaging may detect abnormalities that escape clinical examination;
-Secondary primary tumours (SPTs): endoscopy and/or imaging may detect abnormalities, but there is controversy as to the cost-effectiveness for endoscopy in all cases (Table 2);
In all cases:
Lesional biopsy
In cases with severe dysplasia, or carcinoma:
Cervical lymph node biopsy;
Imaging:
- Ultrasonography
- Jaw radiography or CT
- MRI head and neck
- Chest radiography or CT
Panendoscopy;
Blood pressure;
Electrocardiogram (ECG);
Full blood picture.
In some cases:
Angiography;
Bone scans;
Doppler;
Liver function tests;
Positron Emission Tomography (PET) scans;
Psychological assessment;
Urea and electrolytes.
CT and MRI are now established as the mainstay investigations in the pre-operative evaluation, in order to:
- Delineate the extent and size of the primary cancer;
- Determine the presence, number and position of involved cervical lymph nodes;
- Search for an occult primary tumour;
- Locate a synchronous primary tumour or distant metastases.
Several studies have suggested that, to detect significant lung pathology, a chest CT is preferable to a plain chest radiograph.
Lesional biopsy
A lesional incisional biopsy is mandatory to confirm any diagnosis of cancer. A biopsy must be performed on any oral mucosal lesion suggestive of cancer, including any ulcer that does not heal within 2–3 weeks. Ideally, scans to evaluate the primary site should be performed prior to biopsy to avoid the effect of upstaging from the oedema caused by biopsy trauma, but this is rarely feasible.
Informed consent is mandatory for biopsy as for all operative procedures, particularly noting the likelihood of postoperative discomfort, the possibility of bleeding or bruising, and any possible less-transient adverse effects, such as postoperative reduction or loss of sensation. Care must be taken not to produce undue anxiety.
Biopsy is generally best performed by a specialist. Some specialists take several biopsies, and some advise that the biopsy should always be done by the surgeon. As a general rule, the biopsy should include lesional and normal tissue.
Another consideration is whether to use a scalpel or a biopsy punch. When a scalpel is used, a specimen of elliptical shape is usually taken, most commonly from an edge of the lesion, and suturing is usually needed. The punch has the advantage that the incision is more controlled, an adequate specimen is still obtained (typically 4 mm or 6 mm diameter) and suturing may not be required (Figures 28–32).
Figure 28. Scalpel and punch.Figure 29. Biopsy procedure.Figure 30. Scalpel biopsy.Figure 31. A silver nitrate application may be adequate haemostasis.Figure 32. Biopsy complete.
Only if adequate specimens and clinical data are provided can the pathologist perform optimally. Thus there is a need to identify the site in the lesion most representative of the pathology: a non-representative biopsy may delay diagnosis. Any red area should ideally be included in the specimen and, in some PMD where no obvious site can be chosen, vital staining with ‘toluidine blue’ followed by a rinse with 1% acetic acid may first be indicated to highlight the area best biopsied. Suspect areas absorb the dye preferentially and stain a deep blue. Oral carcinoma in situ and early invasive carcinoma have an affinity for toluidine blue dye and, although several false-positive results may be encountered, these can be minimized by restaining after 14 days. Toluidine blue clearly is more effective in experienced hands and when used with appropriate clinical judgment. Counterstaining with Lugol iodine solution may enhance the usefulness of toluidine blue staining.
Avoid excisional biopsies unless the lesion is small, because the procedure is unlikely to have achieved excision of an adequately wide margin of tissue if the lesion is malignant but will have destroyed clinical evidence of the site and character of the lesion for the surgeon or radiotherapist. This can be avoided by tattooing the site.
An incision biopsy means cutting a thin slice of tissue from the area to be tested. The biopsy specimen should be sufficiently large to include enough suspect and apparently normal tissue to provide the pathologist with an opportunity to make the diagnosis and not have to request an additional specimen. Most patients tolerate (physically and psychologically) one biopsy session. Depending on the size of the piece of tissue removed, some sutures may be needed. Most biopsy wounds, whether 0.5 cm (too small) or 1.5 cm long (usually adequate), heal within 7–10 days; therefore, taking at least one ample specimen is better than having to repeat the procedure. Some clinicians always take several biopsy specimens at the first visit to avoid the delay, anxiety and aggravation resulting from a negative pathology report for a patient in whom cancer is strongly suspected.
Fix biopsies in 10% formal saline (40% formaldehyde: 100 ml; sodium chloride: 9 g; distilled water: 900 ml) to prevent autolysis. The biopsy specimen container must be labelled clearly with the:
Patient's details as above;
Date and time of the procedure; and
Specimen site.
The histopathology request form should be completed with the:
Patient's details (full name, hospital or clinic number, date of birth, etc);
Date, clinic location and requesting clinician's name;
Site of biopsy (diagrams can be useful);
Clinical résumé (photographs may help);
Provisional diagnosis and dates and numbers of all previous biopsies.
It is common to have some bruising and/or soreness in the area the biopsy sample was taken from for up to a week or so afterwards. This can usually be relieved by taking a mild analgesic such as paracetamol.
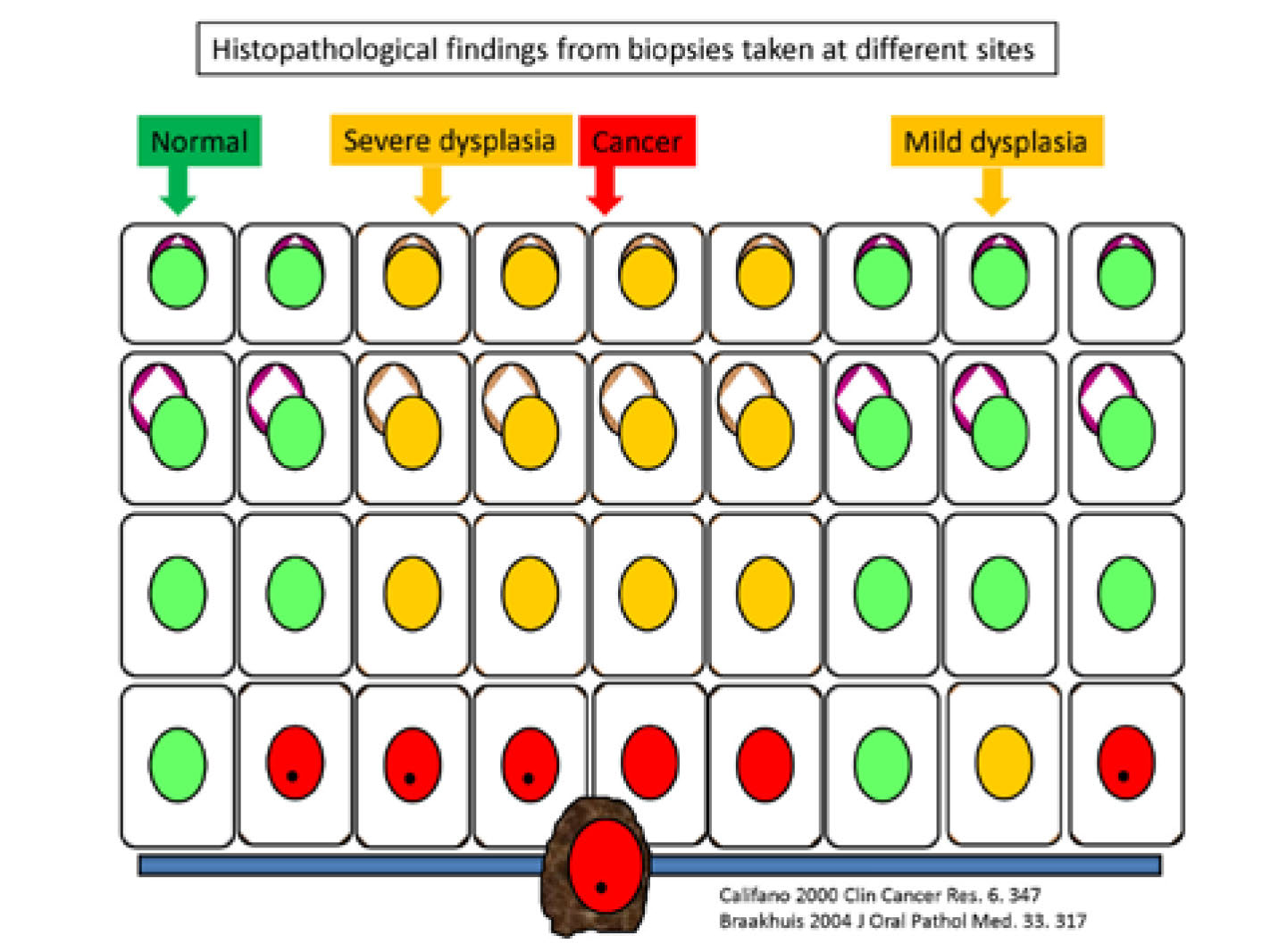
However, with the most appropriate biopsy, even the best pathologists can still err, and it is important to repeat or challenge negative results if clinically suspicious of malignancy. In any PMDs there might be a range of cells present of different malignant potential, including some that cross the epithelial basement membrane – defining the lesion as cancer (Figure 33).
Figure 33. Diagrammatic representation of composition of a clinical mucosal lesion considered potentially malignant, and possible biopsy results. Cells with green nuclei = normal; cells with orange nuclei = dysplastic; cells with red nuclei = severely dysplastic/malignant.
The histopathological interpretation of a biopsy from such a lesion could thus vary from benign to malignant, depending on the site biopsied, the histopathologists acumen, and other factors.
Lymph node biopsy
Clinical palpation of the cervical lymph nodes is necessary but is generally regarded as inaccurate (sensitivity and specificity ~60–70%), and impalpable micrometastases may be present. In practical terms, ipsilateral, firm or hard, enlarged regional lymph nodes in a patient with an obvious oral or oropharyngeal carcinoma are highly likely to include metastases.
Investigations, particularly node biopsy, are thus commonly performed. Lymph node biopsy is best performed on regional lymph nodes that are enlarged and suggestive of cancer, usually using a fine-bore needle to aspirate cells for cytologic examination, or excision biopsy. False-negative results are possible, but the primary danger of biopsy is that it may seed malignant cells. Fine needle aspiration, also called FNA, involves inserting a thin needle into the lymph node to draw out cells and fluid for histopathological analysis. Ultrasound-guided Fine-Needle Aspiration Cytology (US-FNAC) is now most favoured.
Sentinel lymph node biopsy
A Sentinel Lymph Node (SLN) is the first lymph node(s) to which cancer cells are most likely to spread from a primary tumour. A Sentinel Lymph Node Biopsy (SLNB) can be used to help determine the extent, or stage, of spread of the cancer. Because SLNB involves less extensive surgery and the removal of fewer lymph nodes than does standard lymph node surgery, the potential for adverse effects is lower.
The SLNB may be done on an outpatient basis or may require a short hospital stay. A surgeon injects either a radioactive substance, or a blue dye, or both near to the tumour to locate the position of the SLN. The surgeon then uses a device to detect radioactivity to find the SLN or looks for blue-stained lymph nodes. Once the SLN is located, the surgeon makes a small skin incision overlying the SLN and removes the node, which is then examined histopathologically. If cancer is found, the surgeon may remove additional lymph nodes, either during the same biopsy appointment or during a follow-up surgical procedure. SLNB can be done either before or after removal of the tumour.
A negative SLNB result suggests that cancer has not spread to other nearby lymph nodes or organs. A positive SLNB result indicates that cancer is present in the sentinel lymph node and may be present in other regional lymph nodes. This information can help in the staging of the cancer and in developing an appropriate treatment plan.
Examination Under Anaesthesia (EUA)
Usually a more thorough Examination Under general Anaesthesia (EUA), of the mouth and upper aerodigestive tract, is indicated to delineate the extent of the primary cancer carefully, palpate for cervical lymph node involvement and identify any synchronous primary lesions typically located in the upper aerodigestive tract (eg mouth, nose, pharynx, larynx, oesophagus).
EUA may be indicated particularly for patients with:
Tumours in the posterior tongue;
Tumours where the margins cannot be readily defined;
An enlarged cervical node but no visible primary neoplasm.
Magnetic Resonance Imaging (MRI) is also useful to detect spread locally or elsewhere.
Sentinel node biopsy, MRI, or ultrasonography of the neck (or combinations) can be used to delineate the extent of cervical node metastasis. When a cervical lymph node is positive (palpably enlarged and with metastatic disease on biopsy) without any primary site evident, a meticulous EUA might reveal the primary tumour. Positron Emission Tomography-Computerized Tomography (PETCT) fusion scan has specific value in evaluating a patient with metastatic lymph nodes and an unknown primary but, if the latter is not located by visual inspection or palpation or PET, random biopsies of the areas for most occult primary sites (nasopharynx, base of tongue, hypopharynx) may help. Biopsy of the tonsil or fossa of Rosenmuller or an ipsilateral tonsillectomy are often warranted.
Clinical examination may reveal metastasis, which initially occurs to regional lymph nodes and later to the liver, bones, and brain. Imaging and other studies may help detect metastases missed during the clinical examination (Table 2).
How are second primary tumours detected?
Second primary tumours (SPTs) are additional primary carcinomas (synchronous tumours) present in as many as 10–15% of people with OSCC or within six months after the index tumour, and are most commonly seen in the mouth in patients with gingival, floor of mouth, lingual, or buccal carcinoma (Figure 34). SPTs may also be present elsewhere in the upper aerodigestive tract (eg mouth, nose, pharynx, larynx, trachea, bronchus, oesophagus).
Figure 34. PMD with field change and several carcinomas and leukoplakias.
General examination and, possibly, endoscopy (a camera and light at one end, and an eyepiece at the other end), may therefore be indicated to detect metastases or SPTs. Metachronous SPTs are those that may develop subsequently after six months of the index tumour.
Nasoendoscopy
Nasendoscopy or laryngoscopy allows examination of all upper air passages and the pharynx. The specialist may use a local anaesthetic spray to numb the throat first and then passes a narrow, flexible telescope (nasoendoscope) up the nose and into the throat. If the specialist detects any abnormal area a biopsy from that area is indicated.
Panendoscopy
Panendoscopy utilizes a series of connected tubes used under GA to examine all upper airways, trachea, bronchi and oesophagus. It helps identify simultaneous SPTs in the oesophagus, larynx or lungs in as many as 15% of patients. More than one-third of SPTs are detectable by endoscopy at or within one year of diagnosis of the index tumour. Panendoscopy is currently only recommended for symptomatic patients or patients with primary cancers known to have a significant risk of a second (synchronous) primary tumour.
What other imaging may be helpful?
Photography
To create a photographic record is especially useful for monitoring the clinical state and site of a lesion.
In biopsy-confirmed mouth cancer the following imaging may be useful.
Jaw radiography
This may often reveal bone invasion, although it is inadequate to exclude bone invasion. Orthopantomography (rotating pantomography, OPG or OPT or Panorex scan) examines the area around the maxilla and mandible and the surrounding area.
MRI or CT scanning
MRI or CT scanning of the primary site, of the head and neck, and of suspected sites of lymph node or distant metastases can help. Head and neck CT will show the size of the cancer and any neck nodes. CT demonstrates bone well. A chest and abdominal CT may show other signs of cancer spread.
The ability of MRI to differentiate tumour tissue from normal tissue gives improved contrast resolution compared to CT. MRI scan shows soft tissue more clearly than on a CT scan but takes longer than CT. T1 weighted images carry a great deal of spatial resolution with good depiction of anatomy, while T2 weighted images are better at highlighting abnormal tissues. Many mouth cancer patients, however, have difficulty with breathing, swallowing, lying flat and keeping still and CT may be the only imaging modality which can be tolerated.
Positron emission tomography (PET) scanning
This is used to produce detailed three-dimensional images. PET scanning, when combined with computed CT, may be useful in detecting occult lymph node involvement and metastatic disease. PET scan uses a small amount of an injected radioactive drug (a radiotracer such as 18-fluorodeoxyglucose [FDG-PET]). However, PET scannng is expensive, and usually only available at some specialized centres.
Chest radiography
This is valuable for excluding synchronous SPTs and as a pre-anaesthetic check, especially in patients with known pulmonary or airway disease, and to demonstrate metastasis to lungs or hilar lymph nodes, ribs, or vertebrae.
Ultrasonography
Ultrasound can be helpful in lymph node biopsy and diagnosing swellings.
Bone scans
These show up any abnormal areas of bone. A small amount of radioactive substance is injected into an arm vein and, about 2–3 hours later, a whole body scan is taken to reveal any ‘hot spots’ (highlighted areas).
Blood vessel examination
Doppler duplex bloodflow studies are used in planning radial free forearm flaps. Angiography is used in planning lower limb free flaps.
Blood tests
Blood tests include the following:
Complete (full) blood cell count and haemoglobin;
Urea and electrolytes;
Blood group testing and cross-matching;
Liver function tests: may reveal metastases in people with advanced disease or other disease in alcohol-users;
Calcium level: raised serum levels are a poor prognostic indicator, primarily found in people with advanced disease.
What is cancer classification, staging and grading?
Terms used to describe mouth cancer may include:
‘Early’ or ‘local’ – a cancer that has not spread.
‘Locally advanced’ – a cancer that has spread to surrounding tissues or cervical lymph nodes.
‘Local recurrence’ – a cancer has returned in the same area.
‘Secondary’, ‘advanced’, ‘widespread’ or ‘metastatic’ – cancer has spread elsewhere in the body.
The most important prognostic factors in mouth cancer are site and TNM (Tumour, Node, Metastasis) stage. The TNM system describes:
The tumour size (T);
Whether the cancer has spread to the nodes (N);
Whether the cancer has metastasized (M).
OSCC should usually be staged according to the TNM classification of the International Union against Cancer (UICC), since this classification relates well to overall survival rate (ie the earlier the stage of tumour, the better the prognosis and the less complicated and mutilating is the treatment). Staging is helpful in order to:
Aid treatment planning;
Prognosticate;
Evaluate treatment results;
Facilitate information exchange between treatment centres.
TNM classification (UICC)
Primary tumour
- T0 – No primary tumour
- Tis – Carcinoma in situ
- T1 – Tumour 2 cm or smaller
- T2 – Tumour 4 cm or smaller;
- T3 – Tumour larger than 4 cm;
- T4 – Tumour larger than 4 cm and deep invasion to muscle, bone or deep structures (eg antrum).
Lymph node involvement
- N0 – No nodes
- N1 – Single homolateral node smaller than 3 cm
- N2 – Nodes(s) homolateral smaller than 6 cm
- N3 – Nodes(s) larger than 6 cm and/or bilateral
Tumour metastasis
- M0 – No metastasis
- M1 – Metastasis noted
Staging
Stage I – T1, N0, M0
Stage II – T2, N0, M0
Stage III
- T3, N0, M0
- T1, T2, T3, N1, M0
Stage IV
- T4, N0, M0
- Any T, N2 or N3, M0
- Any T, any N, any M Category M1 may be further specified
Adrenals (ADR)
Bone marrow (MAR)
Brain (BRA)
Hepatic (HEP)
Skin (SKI)
Lymph nodes (LYM)
Osseous (OSS)
Other (OTH)
Peritoneum (PER)
Pleura (PLE)
Pulmonary (PUL)
There is also a number stages system for mouth and oropharyngeal cancers which uses four main stages, but some also refer to stage 0:
Stage 0 or carcinoma in situ (CIS) – This is a very early stage cancer;
Stage 1 – This is the earliest stage of invasive cancer; it is <2 cm across and has not spread to nearby tissues, lymph nodes or other organs;
Stage 2 – This is >2 cm across, but <4 cm and has not spread to lymph nodes or other organs;
Stage 3 – Either the cancer is >4 cm but has not spread to any lymph nodes or other parts of the body, or the tumour is any size but has spread to one lymph node on the same side of the neck as the cancer. In this case, the lymph node involved is no more than 3 cm across. Stage 3 cancer may be subdivided into Stage 3a, Stage 3b and Stage 3c. A Stage 3b cancer may differ from a Stage 3a cancer in either the tumour size or if the cancer has spread to lymph nodes;
Stage 4 – This is advanced; it is divided into 3:
- Stage 4a – This has grown through the tissues around the lips and mouth-lymph nodes in the area may or may not contain cancer cells;
- Stage 4b – This is any size and has spread to more than one lymph node on the same side of the neck, or to lymph nodes on both sides of the neck, or any lymph node is bigger than 6 cm;
- Stage 4c – This has spread to other parts such as the lungs or bones.
The number stages are made up of different combinations of the TNM stages, so a Stage 1 cancer may be described as either T1, N0, M0 or T2, N0, M0.
Grading of mouth cancer
Grading refers to the cancer cell appearance under the microscope and gives an idea of how the cancer may behave. The histological grading of carcinoma represents an estimation by the pathologist of the expected behaviour of the cancer:
GX – Grade of differentiation cannot be assessed;
G1 – Well differentiated (low grade) – the cells look like normal mouth cells;
G2 – Moderately differentiated (intermediate grade) – the cells differ slightly from normal mouth or oropharyngeal cells – cells are moderately differentiated. Elongated rete pegs invading lamina propria, with keratin pearls;
G3 – Poorly differentiated (high grade) – the cells are abnormal and not much like normal mouth or oropharyngeal cells – cells are poorly-differentiated. Irregular invading rete pegs; loss of cellular cohesion;
G4 – Undifferentiated. (high grade) – the cancer cells differ from normal mouth or oropharyngeal cells – cells are undifferentiated. Sheets of invading epithelium with no obvious architecture, but severe cellular abnormalities, such as pleomorphism and hyperchromatism.
Grading is used as a prognostic indicator; well-differentiated or low-grade cancers tend to have the better prognosis, usually growing more slowly and less likely to spread than a high-grade tumour. High-grade means the cells look more abnormal and the tumours metastasize more readily.
What else is needed before cancer treatment?
The patient is prepared for major surgery particularly in terms of his/her understanding and informed consent, co-morbidities, general anaesthesia, potential blood loss and ability to metabolize drugs. Potential dental or oral problems should be addressed pre-operatively to minimize or avoid later complications (Article 13).
Talking with a person diagnosed with mouth cancer
It is difficult to find the right words to say to someone who has been diagnosed with cancer. There is no correct way to act or perfect words to say. Assuring them of your support is one of the most important things you can do. Most people with cancer do not want to face the experience alone and will need support from their healthcare team, family and friends. Bear in mind that not everyone wants to talk about their feelings: some may have other ways to express their emotions, and some just prefer to keep feelings private.
What are the potential medical/legal pitfalls?
These may include:
Failure to diagnose mouth cancer or refer appropriately;
Failure to diagnose correctly because of inadequate biopsy specimens or inadequate histopathological diagnosis;
Failure to start treatment early;
Failure to exclude complicating factors such as comorbidities, metastases, or second primary neoplasms.