Aldred MJ, Savarirayan R, Lamande SR, Crawford PJM. Clinical and radiographic features of a family with autosomal dominant amelogenesis imperfecta with taurodontism. Oral Dis. 2002; 8:62-68
Seow WK. Clinical diagnosis and management strategies of amelogenesis imperfecta variants. Pediatr Dent. 1993; 15:384-393
Aldred MJ, Savarirayan R, Crawford PJM. Amelogenesis imperfecta: a classification and catalogue for the 21st century. Oral Dis. 2003; 9:19-23
Fritz GW. Amelogenesis imperfecta with multiple impactions. Oral Surg Oral Med Oral Pathol. 1981; 51:460-462
Collins MA, Mauriello SM, Tyndall DA, Wright JT. Dental anomalies associated with amelogenesis imperfecta: a radiographic assessment. Oral Surg Oral Med Oral Path Oral Radiol Endod. 1999; 88:358-364
Williams SA, Ogden AR. Failure of eruption associated with anomalies of the dentition in siblings. Pediatr Dent. 1988; 10:130-135
Rowley R, Hill FJ, Winter GB. An investigation of the association between anterior open bite and amelogenesis imperfecta. Am J Orthod. 1982; 81:229-235
Sundell S. Hereditary amelogenesis imperfecta. I. Oral health in children. Swed Dent J. 1986; 10:(4)151-163
Ooya K, Nalbandian J, Koikura T. Autosomal recessive rough hypoplastic amelogenesis imperfecta. A case report with clinical, light microscopic, radiographic, and electron microscopic observations. Oral Surg Oral Med Oral Path Oral Radiol Endod. 1988; 65:449-458
Macedo GO, Tunes RS, Motta ACF, Passador-Santos F, Grisi MM, Souza SLS, Palioto DB, Taba M, Novaes AB. Amelogenesis imperfecta and unusual gingival hyperplasia. J Periodontol. 2005; 76:(9)1563-1566
Seow WK, Hackey D. Preeruptive resorption of dentin in the primary and permanent dentitions: case report. Pediatr Dent. 1996; 18:67-71
Korbmacher HM, Lemke R, Kahl-Nieke B. Progressive preeruptive crown resorption in autosomal recessive generalized hypoplastic Amelogenesis imperfecta. Oral Surg Oral Med Oral Path Oral Radiol Endod. 2007; 104:(4)540-544
Davidovich E, Kriener B, Peretz B. Treatment of severe pre-eruptive intracoronal resorption of permanent second molar. Pediatr Dent. 2005; 27:74-77
Seow WK, Lu PC, Mcallan LH. Prevalence of pre-eruptive intracoronal dentin defects from panoramic radiographs. Pediatr Dent. 1999; 21:332-339
Guinta JL, Kaplan MA. “Caries-like” dentin radiolucency of unerupted permanent tooth from developmental defects: case report. J Pedod. 1981; 5:249-255
Seow WK. Pre-eruptive intracoronal resorption as an entity of occult caries. Pediatr Dent. 2000; 22:370-375
Ignelzi MA, Fields HW, White RP, Bergenholtz G, Booth FA. Intracoronal radiolucencies with unerupted teeth. Case report and review of literature. Oral Surg Oral Med Oral Path Oral Radiol Endod. 1990; 70:214-220
Savage NW, Gentner M, Symons AL. Preeruptive intracranial radiolucencies: review and report of a case. ASDC J Dent Child. 1998; 65:36-40
Amelogenesis imperfecta with coronal resorption: report of three cases Shannu K Bhatia M Lindsay Hunter Paul F Ashley Dental Update 2024 42:10, 707-709.
Authors
Shannu KBhatia
BDS, MDS, MFDS RCS(Eng)
Specialist Registrar in Paediatric Dentistry, Paediatric Dentistry Unit, Cardiff University Dental Hospital, Heath Park, UK
Clinical Reader and Honorary Consultant in Paediatric Dentistry, Dental Health and Biological Sciences, Wales College of Medicine, School of Dentistry, Heath Park, Cardiff CF14 4XY, UK
Senior Lecturer/Honorary Consultant and Programme Director, Department of Paediatric Dentistry, Eastman Dental Institute, 256 Gray's Inn Road, London WC1X 8LD, UK
Intracoronal resorption of the permanent dentition in cases of amelogenesis imperfecta (AI) is a rare finding which poses an added complication to the already complex management of this condition. This paper presents three cases of AI associated with delayed eruption of permanent teeth in which asymptomatic intracoronal resorption occurred.
CPD/Clinical Relevance: This paper highlights the fact that teeth affected with amelogenesis imperfecta may undergo asymptomatic intracoronal resorption which is only identifiable radiographically.
Article
Amelogenesis Imperfecta (AI) is a group of relatively rare inherited defects that affect the quantity and/or quality of enamel formation. The disorder is generalized, predominantly affecting all teeth in both primary and permanent dentitions. The prevalence of AI is known to vary by population, ranging from 1:700 to 1:14000.1 Its mode of inheritance can be autosomal dominant, autosomal recessive or X-linked. Sporadic cases, representing spontaneous mutation, may also present.2
AI arises as a result of genetic alteration associated with the process of formation and maturation of enamel.3 Alterations occurring at different levels of enamel formation and maturation result in clinically different presentations. To date, 14 different types of AI have been identified on the basis of genetic pattern, clinical and radiological features, and histological changes.4 In the classifications most commonly used by clinicians, the main types of AI are initially described phenotypically as hypoplastic or hypomineralized; hypomineralized AI can be further sub-classified into hypocalcified and hypomaturation types, with hypocalcified being a more severe type. A combination of hypoplasia and hypomineralization can also be observed in some patients with AI.
Despite the observation that AI results from disorders in the genes involved in enamel formation and maturation, a variety of non-enamel manifestations also occur in association with the disorder. Those reported in the literature include:
Resorption of the crowns of permanent teeth is an uncommon finding not widely reported in the dental literature. Here we report three cases of AI (summarized in Table 1) presenting to the Unit of Paediatric Dentistry at the Eastman Dental Hospital (UCLH Foundation Trust, London) in which intracoronal resorption associated with delayed eruption and gingival overgrowth presented as a feature of AI.
Case 1
Case 2
Case 3
Phenotype
Hypoplastic
Hypoplastic
Hypocalcified
Mode of transmission
Autosomal dominant
Recessive trait?
Autosomal dominant
Medical history
Precocious pubertyThymic enlargementMyopia
Nil relevant
ADHD
Number of teeth with intracoronal resorption
Two
One
One
Affected teeth
Maxillary1st permanent molars
Maxillary left1st permanent molar
Mandibular right2nd permanent molar
Stage of eruption
UneruptedDelayed eruption
UneruptedDelayed eruption
UneruptedDelayed eruption
Associated symptoms
Asymptomatic
Asymptomatic
Asymptomatic
Extent of lesion
Pulpal involvement
Pulpal involvement
Pulpal involvement
Outcome
Extracted
Extracted
Endodontic treatment
Case 1
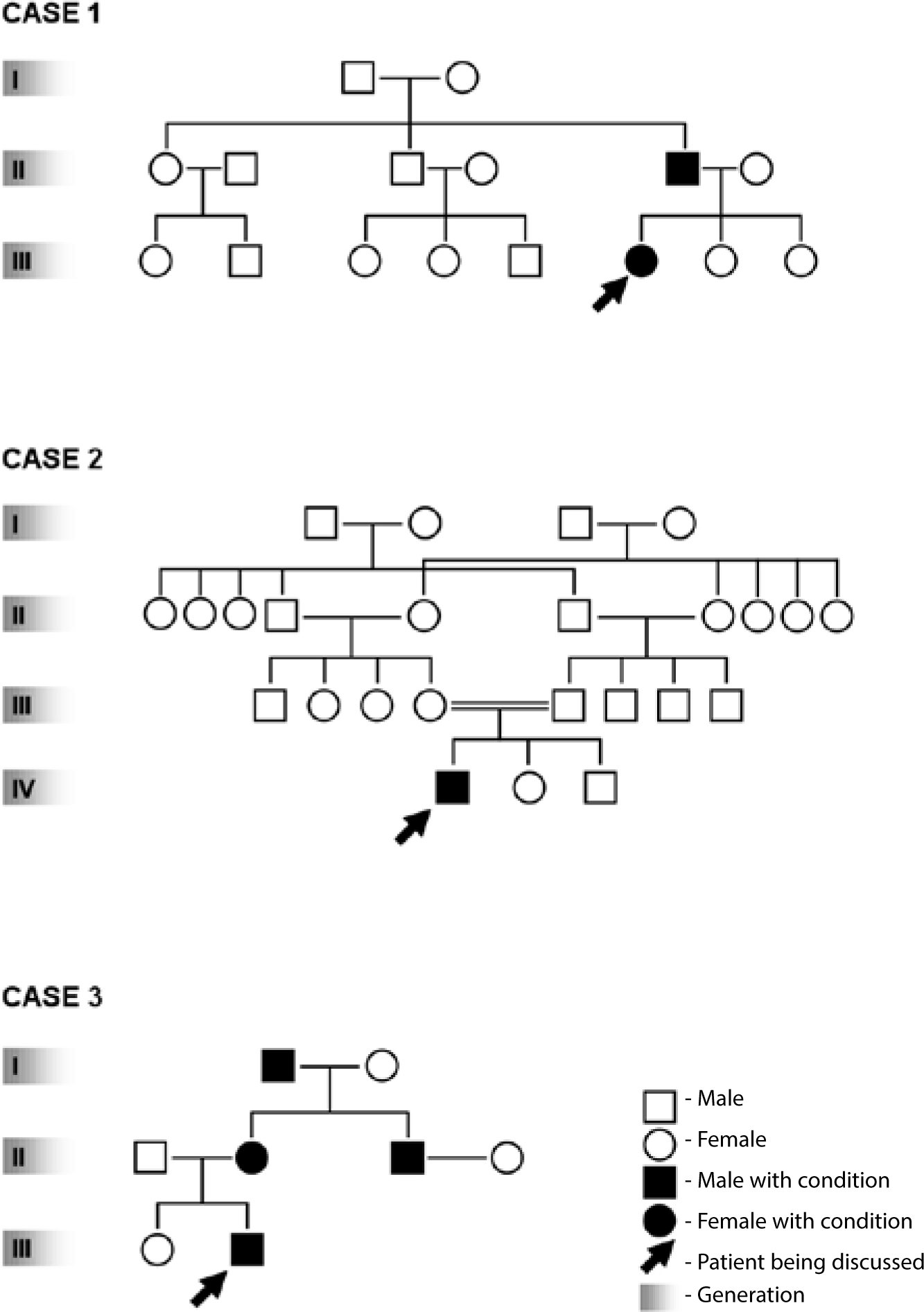
A 6-year-old female (CB) was referred for the management of AI. It was reported that her father had suffered from a similar dental condition and that all his teeth had been extracted at an early age. CB had two sisters, one of whom was affected by AI. This family history is illustrated in Figure 1. A comprehensive medical history revealed that CB suffered from myopia and thymic enlargement; she subsequently developed precocious puberty. No syndrome had been identified.
Figure 1. Family history of reported cases.
The crowns of CB's teeth were pitted but of normal colour. The enamel appeared thin, the cusps being pointed. The entire primary dentition was affected and, as they erupted, it became evident that the permanent teeth were similarly affected by AI. There was a notable delay in the eruption of the permanent teeth. At 10 years of age the occlusal surfaces of the maxillary first molars were mostly obscured by gingival tissue. A panoramic radiograph taken at this time shows delayed eruption of teeth, with no evidence of resorption of molars at this age (Figure 2).
Figure 2. Panoramic radiograph of CB at 10 years of age with no signs of resorption of the permanent molars.
CB was reviewed a year later. The maxillary first permanent molars were still not fully erupted (Figure 3) and a panoramic radiographic examination (Figure 4) suggested that the partially erupted maxillary first permanent molars were undergoing coronal resorption. Impaction of the unerupted maxillary right canine was also noted. In order to investigate the condition of the maxillary right first permanent molar further, the gingival tissue overlying this tooth was excised. The occlusal defect was found to be deep and the overlying fibrous gingival tissue continuous with the pulp. In view of this unusual finding, it was deemed that the maxillary first permanent molars were of poor prognosis. After a specialist orthodontic opinion, extraction of the maxillary first permanent molars, maxillary first premolars and mandibular left first permanent molar was advised, their loss being incorporated into a long-term orthodontic treatment plan. These teeth were extracted under general anaesthesia.
Figure 3. Intra-oral view of CB at 11 years of age showing gingival overgrowth and delayed eruption of first permanent molars. The maxillary anteriors have been restored with composites.Figure 4. Panoramic radiograph of CB at 11 years of age showing coronal resorption of maxillary first permanent molars.
The impacted maxillary right canine was subsequently exposed surgically under local anaesthetic and a bracket bonded to facilitate its guidance into occlusion. The second permanent molars which, at 14 years of age showed delayed eruption, were also surgically exposed under local anaesthesia. At operation, these teeth exhibited severe occlusal hypoplasia and were initially dressed with glass-ionomer. Following healing of the surgical site, these surfaces were restored with nickel chrome onlays. CB has since been kept under regular review.
Case 2
An 8-year-old male (AA) was referred by his general dental practitioner regarding excessive wear of his primary incisors. There was no previous family history of any similar condition and AA had two siblings whose teeth appeared normal. This family history is illustrated in Figure 1.
Clinical examination revealed AA to be in the mixed dentition with generalized marked wear of the primary teeth. The teeth were smooth and yellow in colour. In addition, the lower permanent central incisors appeared diminutive. The partially erupted maxillary left first permanent molar exhibited rough pitted enamel and a deep occlusal defect. The mandibular first permanent molars and maxillary right first permanent molar were unerupted and covered by fibrous gingival tissue. Radiographically, while all permanent teeth were present, there was evidence of delayed eruption. Intracoronal resorption of the partially erupted maxillary left first permanent molar was noted on a panoramic radiograph (Figure 5). Following consultation with a specialist in orthodontics, a decision was made to extract both maxillary first permanent molars. At operation, the mandibular first permanent molars and upper central incisors were surgically exposed. Stainless steel crowns were placed on the second primary molars to provide space anteriorly, thus enabling the provision of aesthetic composite restorations. AA will be kept under regular review to monitor the eruption of the second permanent molars.
Figure 5. Panoramic radiograph OPT showing resorption of maxillary left first molar.
Case 3
A 14-year-old male (SS) was referred by his general dental practitioner regarding management of AI, his chief complaints being in relation to aesthetics and sensitivity. A comprehensive medical history revealed that SS suffered from mild attention deficit hyperactivity disorder (ADHD). There was a clear family history of AI, SS's brother, mother, uncle and maternal grandparent all being affected. This family history is illustrated in Figure 1.
Clinical examination revealed delayed eruption of the second permanent molars and the presence of an anterior open bite. SS's oral hygiene was noted to be poor. The gingival tissues overlying the partially erupted second permanent molars appeared hyperplastic. Panoramic radiographic examination showed no evidence of intracoronal resorption at this stage (Figure 6).
Figure 6. Panoramic radiograph at this stage shows no evidence of coronal resorption.
SS's initial treatment included the provision of oral hygiene and scaling and polishing. Aesthetics and function were improved by the placement of composite veneers on the maxillary anteriors and nickel-chrome onlays on the erupted first permanent molars. A decision was made to monitor the second permanent molars until full eruption, restoring them with occlusal onlays when feasible. On review one year later, the mandibular right second permanent molar had not fully erupted (Figure 7). A decision was made to expose its coronal surface by excising the overlying gingival tissue. As in case 1, an extensive area of intracoronal resorption was seen, the gingival tissue appearing continuous with the dental pulp. Following consultation with a specialist in endodontics, a decision was made to attempt to treat the tooth endodontically. This treatment is currently ongoing.
Figure 7. Periapical radiograph showing coronal resorption in the mandibular second permanent molar.
Discussion
As stated previously, AI is a group of inherited defects of dental enamel formation that show both clinical and genetic heterogeneity. Genetic alteration at different levels of enamel formation and maturation result in clinically different presentations. In the reported cases, cases 1 and 2 exhibited a hypoplastic form of AI, while case 3 exhibited a hypocalcification variant.
Most of the reports of pre-eruptive resorption in the dental literature affect the permanent dentition. Usually a single tooth is affected;12 mandibular premolars and molars being the most frequently reported teeth.13 In all 3 cases reported here, intracoronal resorption was noted in permanent molar teeth before they had emerged into the oral cavity. Two cases exhibited resorption of a single tooth, but one had resorption of two teeth. Although aggressive in nature, intracoronal resorption tends to be asymptomatic, usually being identified only on radiographic examination. The presentation of all three cases conformed to this observation.
It has been recommended that surgical exposure of unerupted teeth be carried out as soon as resorption is detected radiographically in order to prevent progress of the lesion into the pulp.14,15 Although this recommendation was followed in the reported cases, the resorption was extensive and the pulp was already involved in two of them.
The pathogenesis of the lesions present in these three cases is unclear. The dental hard tissues of permanent teeth do not normally undergo resorption, though this may occur as a result of inflammatory conditions, mechanical stimulation or neoplastic processes. In the intracoronal resorption of unerupted teeth, the lesions are often located within the dentine-enamel junction, in the occlusal aspect of the crown. Indeed, they are often referred to as pre-eruptive caries.16 It has been suggested that the retentive nature of the cavitated lesion favours caries development, and the lesion becomes distinguishable as a carious lesion once it is exposed to the oral cavity.17 While nearly half of the lesions extend to more than two-thirds of the dentine width,14 it is not certain whether they remain stable or enlarge.
Local factors may play a role in the aetiology of this condition, the following having been implicated:
Periapical inflammation of a primary precursor; and
Developmental defect due to inclusion of uncalcified enamel matrix.13,18,19
In a SEM study carried out on unerupted third molars by Owens and co-workers, ameloblasts rather than multinucleated cells were implicated in the idiopathic external resorptive process. It was suggested that resorptive activity of, and by, enamel epithelium may explain the coronal origin of the resorption and its progression into pulp.20
The intracoronal resorption in the reported cases could be due to defective mineralization of the teeth affected with AI, leading to exposed dentinal tubules. This may have led to inflammation of the pulp and, in turn, external resorption of the crown. Alternatively, these features could be attributed to premature degeneration of the reduced enamel epithelium which covers the crown of unerupted teeth.
Conclusion
Intracoronal resorption of permanent teeth is a rare but a significant finding in AI. Prompt intervention is necessary to limit the damage and restore the tooth. Elective endodontics should be started in suitable cases; alternatively, extraction may be considered, the affected teeth being incorporated into an orthodontic treatment plan. Both specialist orthodontic and endodontic input is of benefit in treatment planning. Further research is needed in relation to the aetiopathogenesis of this unusual condition.