A MEDLINE search early in 2015 revealed more than 250,000 papers on head and neck cancer; over 100,000 on oral cancer; and over 60,000 on mouth cancer. Not all publications contain robust evidence. We endeavour to encapsulate the most important of the latest information and advances now employed in practice, in a form comprehensible to healthcare workers, patients and their carers. This series offers the primary care dental team, in particular, an overview of the aetiopathogenesis, prevention, diagnosis and multidisciplinary care of mouth cancer, the functional and psychosocial implications, and minimization of the impact on the quality of life of patient and family.
Clinical Relevance: This article offers the dental team an overview of oral potentially malignant disorders.
Article
Nicholas Kalavrezos Professor Crispian Scully
Some mouth cancers are preceded by clinically obvious potentially malignant disorders (PMDs); most are probably not and arise in clinically apparently normal mucosa. Nevertheless, molecular changes must precede histopathological and clinically detectable lesions. Risk factors for the PMD are generally those as for OSCC (Articles 3, 4, 5).
What are potentially malignant disorders?
Some mouth cancers are preceded by clinically obvious potentially malignant disorders (PMDs). There is a range of PMDs known but the most important recognized are erythroplakia (erythroplasia), leukoplakia, lichenoid lesions, actinic cheilitis and submucous fibrosis (Table 1 and Figures 1–9; see also Article 7) and many cancers are associated with such lesions (especially in South-East Asian people).
Of course PMDs, although regarded as early lesions in possible progression to malignancy, may well, in molecular terms, be rather ‘late’ (Article 1) in that several genetic changes may be present with no clinical signs detectable.
Oral cancer itself in the initial clinically detectable stage is often a red or red and white area without symptoms, so it can be very difficult to differentiate PMDs from early cancers and both are rarely painful. The initial PMD lesions are usually solitary and asymptomatic when they are small and thus, in the early stages, it is quite possible to make a misdiagnosis. Lesions of oral cancer can range from a few millimetres, to several centimetres diameter in the more advanced cases. In advanced cancers, there is often a red or red and white single lesion, ulcer or lump with irregular margins which are rigid to touch (indurated) and there may be pain, especially in the tongue and floor of the mouth lesions. These are easier to recognize: the RULE is to look out for a single lesion of 3 or more weeks’ duration, especially a:
Red and/or white lesion;
Ulcer;
Lump;
Especially when in a combination, or if indurated (firm on palpation).
Such lesions should be regarded with suspicion, and urgent biopsy arranged. If people notice any of these changes, they should seek help from their dentist, doctor, or another healthcare professional without delay.
The risk of malignant transformation in the PMD varies enormously but, over a 5–10 year period, is approximately as follows:
Potentially malignant lesions are initially usually symptomless, so any symptoms should raise the index of suspicion of malignant change.
What is the natural history of PMDs?
The natural history of PMDs is not absolutely clear and, though the risk of malignant development is not reliably predictable, it is greatest in:
Older patients;
Females;
Never-users of tobacco;
PMDs that are:
-non-homogeneous;
-on the lateral and ventral tongue, floor of the mouth and retromolar/soft palate complex;
-large lesions covering several intra-oral subsites; or
-of long duration.
Factors predictive of future malignant transformation may also include factors discussed below, such as:
Epithelial dysplasia;
Expressions of P53 tumour suppressor protein;
Changes involving chromosomes 3p or 9p termed ‘loss of heterozygosity,’ or LOH;
Chromosomal polysomy;
History of cancer in the upper aerodigestive tract.
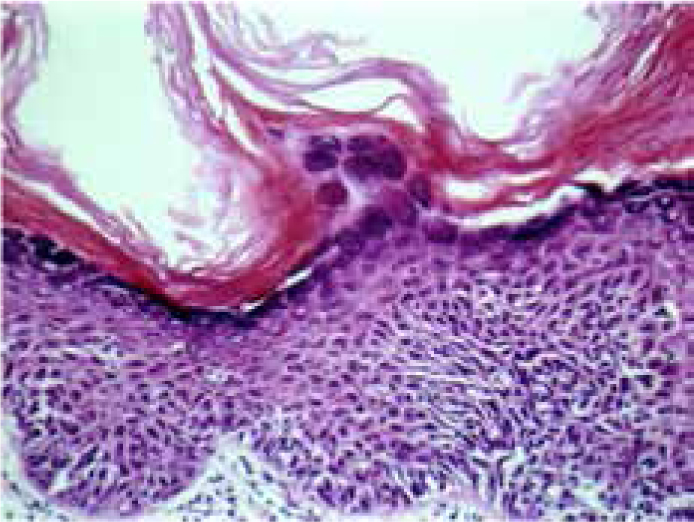
Epithelial dysplasia (from Greek dys = poor and plasia = a moulding) is a term describing the combination of disorderly maturation and disturbed cell proliferation seen in OSCC and in some PMDs (and in some benign disorders) (Figure 10).
Figure 10. Epithelial dysplasia – a predictor of transformation.
Epithelial dysplasia is usually graded as mild, moderate or severe, depending on the extent of the abnormality seen. This grading process is subjective, but it is still the single most useful tool for prediction of the behaviour of abnormal epithelium. A total of 148 male patients with oral PMDs in Taiwan were studied with a mean follow-up period of 38 months. The malignant transformation rate was highest in subjects diagnosed with oral epithelial dysplasia. In this group the transformation ate was 7.62 per 100 people per year. The anatomical site of PMDs was the only statistically significant variable associated with malignancy: higher for tongue lesions than with buccal lesions. A UK study of 1357 patients with biopsy-confirmed oral PMDs showed the most common PMD to be lichen planus/lichenoid reactions. Among all PMDs, 15% had epithelial dysplasia. Thirty-five patients developed OSCC over the follow-up period (2.6%). Patients with severe dysplasia had a higher risk of transformation to oral cancer compared to those with no dysplasia. A significant trend over dysplasia grades was evident. Transformation to oral cancer was also associated with increasing patient age.
Dysplasia on biopsy examination is thus one of the main histological features that appears to precede the onset of malignancy and it appears to be the most predictive marker for malignant potential in current use. Cellular atypia is the main feature of dysplasia and the rate of malignant changes can be as high as 36% when moderate or severe dysplasia is present.
Sadly, a number of studies have shown that the reliability of dysplasia grading and histopathological examination cannot be guaranteed; pathologists can differ in their diagnosis one from another and even the same pathologist can sometimes give a different opinion at different times (a phenomenon common with some other diagnostic procedures in healthcare). Furthermore, some potentially malignant lesions on initial biopsy have shown no serious pathology but have, on excision, been shown to contain cancers in up to 10%. Also, the clinically normal mucosa at lesional margins may actually harbour alterations at the molecular level, contributing to the persistence/recurrence of the lesion, or to subsequent OSCC.
Because of such uncertainties, much effort has gone into identifying the genetic changes that underlie mouth cancer and to find biomarkers such as DNA ploidy (aneuploidy), and changes in the p53, and loss of heterozygosity (LOH) in chromosomes 3p, 9p, 4q or 17p that might better predict malignant change (Article 1). Malignant transformation of the involved epithelium is a culmination of constant exposure to carcinogens and an accumulation of genetic alterations. Molecular aberrations have been identified in oral premalignant mucosal lesions, which increase in number as lesions progress toward malignancy. Loss of heterozygosity at 9p21 is thought to be an early event, identified in hyperplastic lesions. Mutations in the tumour-suppressor genes p53 and Rb are common in tobacco-related premalignant and malignant lesions. Most HPV-related oropharyngeal head and neck cancers carry wild-type Rb and p53. Evidence now supports the role of the viral oncoproteins E6 and E7 in the development of HPV malignancy through inactivation of p53 and Rb gene products.
However, despite considerable progress in such molecular biology, there is still no single marker or set of markers that reliably predict malignant transformation in an individual patient, although the presence of dysplasia and of other changes, such as these genetic changes, are suggestive.
The extent or grade of dysplasia is currently the accepted reference method by which the malignant potential is gauged to predict malignant transformation, but many specialists now believe that seeing severe dysplasia is often tantamount to a diagnosis of early carcinoma, since the epithelial basement membrane may well be breached even when not detected in the biopsy specimen submitted for histopathological examination. Detection of dysplasia thus suggests early intervention hopefully to reduce future malignant transformation.
Dysplasia grading is widely used to assess risk of transformation, despite limited data on predictive value. DNA ploidy analysis has been proposed as an alternative. A retrospective study of conventional dysplasia grading was conducted on 1,401 patients. DNA ploidy analysis was conducted on a subset of 273 patients and results correlated with clinical information, pathologic diagnosis and outcome over 5–15 years. Malignant transformation occurred in 12% and, of these, 63% of pre-existing index lesions had aneuploidy, whereas it was present in only 16% of patients not developing carcinoma. Epithelial dysplasia correlated with DNA ploidy status. The overall positive predictive value for malignant transformation by DNA aneuploidy was 38.5% (sensitivity 65.2% and specificity 75%), and by severe dysplasia grade 39.5% (sensitivity 30% and specificity 98%). DNA diploid and tetraploid status had negative predictive value of 90–96%.
Combining DNA ploidy analysis with dysplasia grading seems to give a higher predictive value than either technique alone. Each of three traditional dysplasia grades (mild, moderate, severe) predicts a significantly different risk of carcinoma development and time to transformation. DNA ploidy analysis had equivalent predictive value and also detected additional risk lesions in the absence of histological evidence of dysplasia.
Future directions are hopeful and are leading to increased reliability of prognostic factors, most of which rely on molecular studies under development. Newer markers suggestive of transformation potential in potentially malignant disorders include:
Cancer history positive;
Chromosomal polysomy [ploidy];
Loss of chromosomal heterozygosity (LOH);
-High risk – LOH for 9p, 17p and 4q
-Intermediate risk – LOH for 9p alone or LOH 9p plus either LOH 17p or LOH 4q
-Low risk – LOH for chromosome 9p only;
p53 protein expression.
What is the recommended management of patients with PMDs?
Management of patients with PMD is a controversial issue because of the above observations and since there is no reliable evidence base. Certainly, a biopsy and a histologic examination are required because dysplasia may precede malignant changes, and a specialist opinion is advised.
Sadly, the evidence base on which treatment is based is also not ideal. Cessation of smoking habits appears to result in some lesions regressing or resolving, so possible aetiological factors should be removed, and an observation of 2–4 weeks seems acceptable to observe any possible regression.
It is not possible yet to define the risk of malignant transformation of a PMD reliably, nor to predict the effects of any interventions reliably. Oral dysplasia shows a significant rate of transformation to cancer, related to grade, and may be decreased significantly but not eliminated by excision. This suggests the need for excision and continued surveillance. Lesions that are not excised demonstrate considerably higher transformation rate than those that are excised. Therefore, rather than so-called ‘watchful waiting’ of PMDs, it is probably best to remove all oral erythroplasias/leukoplakias, if feasible, especially if there is epithelial dysplasia on biopsy. Surgery may have a beneficial effect, but there is little evidence that this will reliably reduce the risk of later recurrence, or malignant transformation of PMDs, at the same or another site. Thus, despite a lack of solid evidence, surgical resection still remains considered the best practice, regardless of histologic grade.
The most commonly used modalities are surgical excision or CO2 laser excision so that the specimen can be sent for histopathological examination. Laser fulguration or ablation does not permit the examination of the whole lesion and, bearing in mind the above comments, would seem less desirable. For widespread lesions, photodynamic therapy (PDT) may sometimes be considered (see below).
The evidence from systematic reviews is that medical therapies are not reliably effective: topical anticancer agents, such as podophyllin or bleomycin or retinoids, have only temporary efficacy, and perhaps their best indication is when the location or extent of the lesion prevent adequate surgical removal. Medical measures that lessen the size, extent or histopathological features of dysplasia within PMD are also associated with a risk of adverse effects.
Recurrence rates after any form of treatment may be up to 30%, probably mainly depending on the duration of follow-up. The efficacy of continuous follow-up of PMD patients is virtually unknown. There is also neither evidence base nor absolute consensus as to the optimum review interval or protocol for other PMDs.
Fully informed consent is crucial, all the uncertainties being discussed with the patient. Management of PMDs is not informed by high level evidence but consensus supports targeted use of biopsy and histopathological assessment. The management of biopsy-proven dysplastic lesions thus favours:
Advice to avoid or reduce known carcinogens, eg tobacco, alcohol and betel;
Surgical excision when the size of the lesions and the patient's function allow;
Long-term surveillance.
Erythroplakia (erythroplasia)
Red oral lesions are usually far more dangerous than white lesions. Erythroplasia is a red and often velvety lesion which, unlike leukoplakias, does not form a plaque but is level with, or depressed below, the surrounding mucosa; 75–90% prove to be carcinoma or carcinoma in situ or show severe dysplasia. Histopathologically, erythroplasia typically shows at least moderate or severe dysplasia. Epithelial dysplasia is in general regarded as the most important indicator of the malignant potential.
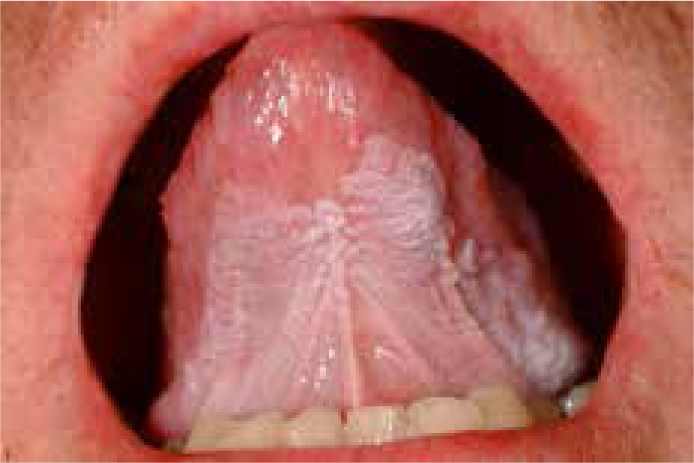
Erythroplasia mainly affects patients of either gender in their sixth and seventh decades, is usually related to tobacco and alcohol use, and typically involves the floor of the mouth, ventrum of the tongue, or the soft palate. Defined as a ‘fiery red patch that cannot be characterized clinically or pathologically as any other definable disease’ (Figure 1), it is usually a solitary lesion. In some, there is a mixture of red and white changes, when the lesion is categorized as ‘erythroleukoplakia’ (Figure 2) or ‘non-homogeneous’ or ‘speckled’ leukoplakia.
Since the majority of erythroplasias will undergo malignant transformation, they need to be removed by surgery, either by cold knife (scalpel) or by laser excision, but there are no reliable data about the prognosis or recurrence rate. Photodynamic therapy (PDT) has also been used to manage patients with erythroplasia, a high success rate (66–95%) having been claimed.
Leukoplakia
A workshop co-ordinated by the WHO Collaborating Centre for Oral Cancer and Precancer agreed that the term leukoplakia should be used to recognize ‘white plaques of questionable risk having excluded (other) known diseases or disorders that carry no increased risk for cancer’. Currently, the term leukoplakia therefore implies a diagnosis by exclusion (eg of lichen planus, candidosis). By definition, the term excludes non-premalignant entities, such as frictional keratosis or smokers keratosis.
White oral lesions usually result from increased keratinization or candidosis and, in contrast to erythroplasia, are mostly neither malignant nor pre-malignant. Leukoplakia is much more common than erythroplasia and it is also associated mainly with tobacco and alcohol. Leukoplakia can appear as:
Homogeneous leukoplakia (flat, thin, uniform white in colour);
Non-homogeneous leukoplakia – these are more dangerous and are either:
-white-and-red (‘erythroleukoplakia’), that may be either irregularly flat (speckled)
-nodular, or
-verrucous – proliferative verrucous leukoplakia (PVL) is a special subtype of verrucous leukoplakia, characterized by multifocal lesions, and a very high malignant transformation rate.
Oral white lesions almost always demonstrate hyperkeratosis, but the presence of epithelial dysplasia is far more unpredictable. The term leukoplakia is used irrespective of the presence or absence of epithelial dysplasia. The prevalence of malignant transformation in leukoplakias ranges from 3–30% over 10 years; homogeneous leukoplakias are only very occasionally premalignant, but speckled or verrucous leukoplakias are more likely to be premalignant. An annual malignant transformation rate of about 1 – 2% over 10 years is probably a realistic figure for leukoplakias overall. However, in dysplastic leukoplakias the malignant transformation may reach 30%.
There are certain other indicators that may help predict malignant change:
Of non-homogeneous type;
Containing epithelial dysplasia;
Of long duration;
In non-smokers;
In females;
On the tongue and/or floor of the mouth;
Of size >200 mm2;
With DNA aneuploidy.
However, it is not possible at present reliably to predict which lesions will progress to carcinoma, or to be absolutely certain that a lesion has malignant potential or not. Indeed, some lesions which, on initial biopsy, have shown no serious pathology have, on excision, been shown to contain cancers in up to 10%.
Despite considerable progress in molecular biology, there is still no single marker or set of markers that reliably predicts malignant transformation of leukoplakia in an individual patient, although the presence of dysplasia and other changes, such as genetic changes, particularly DNA ploidy, in the tumour suppressor gene p53, and loss of heterozygosity (LOH) in chromosomes 3 and 9 are suggestive.
Thus, possible aetiological factors should be removed, and an observation of 2–4 weeks seems acceptable to observe any possible regression. There is also no scientific evidence that treatment with any manner of interventions prevents the development of OSCC. Since some lesions which, on initial biopsy, have shown no serious pathology but have, on excision, been shown to contain cancers in up to 10%, it is probably best to remove the whole of all oral leukoplakias, if feasible, especially if there is epithelial dysplasia on biopsy, rather than any so-called ‘watchful waiting’. Excision biopsy does not prevent malignant transformation (primary prevention), but it does promote early diagnosis of cancer (secondary prevention) and is thus indicated for all lesions, where possible. The most commonly used treatments are surgical excision or CO2 laser excision (not ablation, which denies the feasibility of histopathological examination). The excision specimen must be sent for histopathological examination. For widespread leukoplakias, PDT may be considered, but results are typically less satisfactory, perhaps because the keratinized surface does not facilitate penetration by photosensitizer.
The rate of recurrence after CO2 laser resection varies from around 7–70%, with malignant transformation occurring in 7–14%. Continuous smoking after surgical removal and widespread lesions are poor prognostic indicators.
The evidence from systematic reviews is that medical therapies are not reliably effective: topical anticancer agents, such as podophyllin or bleomycin or retinoids, have only temporary efficacy, and perhaps their best indication is when the location or extent of the lesion prevent adequate surgical removal.
The efficacy of continuous follow-up of oral leukoplakia patients is unknown. If there is any change causing concern, particularly the development of a lump, a specialist opinion should be obtained.
Nevertheless, recurrence rates after any form of treatment may be high, probably mainly depending on the duration of follow-up. Despite these facts, fewer than 27% of leukoplakias are subjected to biopsy. As a result, many must surely be left to ‘watchful waiting’ and may presumably progress to more advanced stages, or cancer.
Lichen planus/lichenoid lesions
Oral lichen planus (OLP) is regarded as a potentially malignant disorder with an annual malignant transformation rate usually <0.5%. The evidence is weak but transformation may occur in any clinical type and may be more common in lichenoid lesions and on the tongue.
Unfortunately, there are no strategies known to prevent this malignant transformation and, although continuous follow-up of patients is advised, any evidence of benefit is questionable. NICE guidelines clearly state that patients with oral lichen planus/lichenoid lesions should be monitored for oral cancer as part of the routine dental examination. If there is any change causing concern, particularly the development of a lump, a specialist opinion should be obtained.
Actinic cheilitis
Actinic cheilitis (actinic keratosis of lip, solar keratosis, solar cheilosis; from the Greek aktino = rays and cheili = lips) is common in sun-overexposed individuals, and is essentially a sunburn, but chronic actinic cheilitis is a PMD. Seen mainly in older men, chronic actinic cheilitis is most common in Caucasians from the tropics. Particularly at risk are people whose lifestyles include much time spent outdoors, especially farmers, sailors, fishermen, windsurfers, skiers, mountaineers, golfers, etc. Sun ultraviolet light UVB can damage particularly the lower lip vermilion. Other forms of radiation, including arc-welding, can occasionally cause similar damage. Actinic cheilitis may rarely be an early manifestation of xeroderma pigmentosum or part of the syndrome of actinic prurigo.
The lip in chronic actinic cheilitis may become dry and scaly and wrinkled with grey to white changes. Lesions may appear as an isolated smooth or scaly, friable patch or can involve the entire lip, later becoming palpably thickened with small greyish white plaques. Eventually, nodules may form, which may evolve into OSCC in about 10%. Immune defects (including immunosuppression in organ transplant recipients) also predispose chronic actinic cheilitis to malignant transformation.
Prevention is advised, especially in high-risk individuals, by avoiding midday sun exposure, wearing broad-brimmed hats, and using adequate sunscreens.
Management of chronic actinic cheilitis is required both to relieve symptoms and to endeavour to prevent OSCC. Removal of premalignant epithelium is best achieved by topical chemo-exfoliants (eg trichloroacetic acid, 5-fluorouracil, bleomycin, 3% diclofenac in 2.5% hyaluronic acid gel, 5% imiquimod), or by photodynamic therapy (PDT), or laser or scalpel surgery. Vermilionectomy using the W-plasty technique appears to give the best cosmetic results and remains the gold standard.
Chronic actinic cheilitis carries a potential for malignant development, necessitating regular monitoring, perhaps every six months, which can be carried out by the general practitioner.
If there is any change causing concern, particularly the development of a lump, a specialist opinion should be obtained.
Submucous fibrosis
Oral submucous fibrosis (OSMF) is a chronic disorder seen only in people who chew betel products. The basic issue in OMSF appears to be an increase in submucosal collagen, for which there may be some genetic predisposition.
OSMF can affect the oral and sometimes pharyngeal mucosa, and develops insidiously, usually diffusely, often initially presenting with oral burning sensations. It is most obvious when characterized by tightening of the buccal, and sometimes palatal and lingual mucosae, especially when causing trismus. Symmetrical fibrosis in the cheeks, lips, tongue or palate appears as vertical bands running through the mucosa, and restricted oral opening. There is also epithelial atrophy and sometimes frank erythroplasia or leukoplakia, There can be oesophageal fibrosis and, if the palatal and paratubal muscles are involved, conductive hearing loss may appear because of functional stenosis of the Eustachian (pharyngo-tympanic) tube.
Diagnosis is often fairly obvious from the clinical features, and a history of betel chewing and often of slowly increasing trismus. Diagnosis can be confirmed if necessary by biopsy, and haematology often reveals coexistent anaemia.
Management is first to stop areca nut exposure, and correct any nutritional deficiencies. There is no reliably effective treatment, though the restricted opening responds best to physiotherapy to stretch the fibrous bands.
The evidence base is weak but medical therapies tried range from topical medication (eg with COX-2 inhibitors); to intralesionally injected medicaments such as corticosteroids, collagenase, or hyaluronidase; to systemic medication with lycopene or pentoxifylline. Surgical therapies range from laser release to band excision or split skin, radial forearm or other flap repairs.
What are the potential medical/legal pitfalls with PMD?
Failure to diagnose or refer correctly;
Failure to diagnose correctly because of inadequate biopsy specimens or inadequate histopathological diagnosis;
Failure to start early treatment;
Failure to exclude complicating factors such as co-morbidities, metastases, or second primary neoplasms.