Yu VSH, Messer HH, Tan KB. Multiple idiopathic cervical resorption: case report and discussion of management options. Int Endod J. 2010; 44:77-85
Mueller E, Rony HR. Laboratory studies of an unusual case of resorption. J Am Dent Assoc. 1930; 17:326-334
Macdonald-Jankowski D. Multiple idiopathic cervical resorption most frequently seen in younger females. Evid Based Dent. 2005; 6
Kim PH, Leslie BH. Multiple idiopathic resorption in the primary dentition. Review of the literature and case report. Oral Surg Oral Med Oral Pathol. 1999; 88:501-555
Liang H, Burkes EJ, Fredderikson NL. Multiple idiopathic cervical root resorption: systematic review and report of four cases. Dentomaxillofac Radiol. 2003; 32:150-155
Neely AL, Gordon SC. A familial pattern of multiple idiopathic cervical root resorption in a father and son: a 22 year follow-up. J Periodontol. 2007; 78:367-371
George DI, Miller RL. Idiopathic resorption of teeth: a report of three cases. Am J Orthod. 1986; 89:13-20
Nikolidakis D, Nokou G, Meijer GJ. Cervical external root: 3 year follow-up of a case. J Oral Sci. 2008; 4:487-491
Cholia SS, Wilson PHR, Makdissi J. Multiple idiopathic external apical root resorption: report of four cases. Dentomaxillofac Radiol. 2005; 34:240-246
Von Arx T, Schawalder P, Ackerman M Human and feline invasive cervical resorptions: the missing link? Presentation of four cases. J Endod. 2009; 35:904-913
DeLaurier A, Boyde A, Jackson B Identifying early osteoclastic resorptive lesions in feline teeth: a model for understanding the origin of multiple idiopathic root resorption. J Perio Res. 2009; 44:248-257
Moody AB, Speculand B, Smith AJ Multiple idiopathic external resorption of teeth. Int J Oral Maxillofac Surg. 1990; 19:200-202
Iwamatsu-Kobayshi Y, Sato-Kuriwade S, Yamamoto T A case of multiple idiopathic external root resorption: a 6 year follow up study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 100:772-779
Kerr DA, Courtney RM, Burker EJ. Multiple idiopathic root resorption: case report and discussion of management options. Oral Surg Oral Med Oral Pathol. 1970; 29:552-565
Weltman B, Vig KWL, Fields HW, Shanker S, Kaizar EE. Root resorption associated with orthodontic tooth movement: a systematic review. Am J Orthod Dentofacial Orthop. 2010; 137:462-476
Marx RE, Garg AK. Bone structure, metabolism and physiology: its impact on dental implantology. Implant Dent. 1998; 7:267-276
Pjetursson BE, Tan K, Lang NP, Brägger U, Egger M, Zwahlen M. A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years. Clin Oral Implants Res. 2004; 15:625-642
Dental management of a patient with multiple idiopathic cervical root resorption Rahat Ali Stephen Fayle David Langley Asmaa Altaie Brian Nattress Dental Update 2024 42:7, 707-709.
Multiple Idiopathic Cervical Root Resorption (MICRR) is a rare condition. It initiates at the cemento-enamel junction of multiple teeth. The lesions continue to grow until they unite, thereby undermining the entire coronal structure of affected teeth. Its distribution can vary from a single region to the entire dentition and the number of teeth affected by resorption tends to increase as the condition is followed over time. The teeth themselves appear clinically normal. The aetiology of MICRR is unknown and it is considered to be a diagnosis of exclusion. The condition tends to be progressive. Consequently, root treatments/surgical curettage and restoration of the lesions have been unsuccessful at arresting the condition. Affected teeth are often extracted in anticipation of catastrophic fracture and have been replaced with partial or complete dentures. In this case report, we describe how a young female patient was dentally managed over 10 years and ultimately rehabilitated with dental implants.
CPD/Clinical Relevance: Patients suspected of having multiple idiopathic cervical root resorption may require specialist, multidisciplinary care and require referral to an appropriate secondary care unit for treatment planning and potential oral rehabilitation.
Article
Multiple Idiopathic Cervical Root Resorption (MICRR) is an uncommon dental condition with less than 30 cases having been reported worldwide.1 It was first reported by Mueller and Rony2 and is thought to have a predilection for affecting younger female patients.3 Most case reports have identified MICRR in the permanent dentition, however, there have been isolated cases of the condition affecting the primary dentition.4 Radiologically, it initiates at the cemento-enamel junction (CEJ) of multiple teeth. The lesions continue to grow until they unite, thereby undermining the entire coronal structure of the affected teeth.
A systematic review5 has suggested that MICRR tends to be an incidental finding on routine clinical/radiological examination. There is no apparent correlation with any other medical or dental condition. Some patients have reported an increase in tooth mobility, but it is generally asymptomatic. The cases included in the systematic review also suggested that the number of teeth affected ranged from 5 to 24 (per patient) with no predilection for any particular location or tooth. The distribution of MICRR can vary from a single region to the entire dentition1 and the number of teeth affected by resorption tends to increase as the condition is followed over time.5 It is unknown whether there is a genetic predisposition to MICRR. Given that the condition has been identified in both patients and their offspring,6 a familial pattern of inheritance may be likely.
Patients with MICRR tend to have normal alveolar bone levels and blood chemistry values.7 There is little correlation with systemic disease and the resorption tends to occur circumferentially on vital teeth. The teeth appear clinically normal. Histological examination of the resorptive sites has revealed the presence of multi-nucleated giant cells, which are indicative of osteoclastic activity.8
The aetiology of MICRR is unclear and it is generally considered to be a diagnosis of exclusion.9 It has been suggested that the condition is associated with exposure to the feline herpes virus FEHV1.10,11 However, this link is tenuous and requires further investigation.
Dental management of MICRR is difficult. The condition can spontaneously arrest. However, it can also progress to the point that the affected teeth are so undermined that they effectively decoronate themselves.5 Currently, it is not possible to predict whether MICRR will arrest or progress in any given patient. If the condition is progressive, root treatment/surgical curettage and restoration of the lesions have been unsuccessful at arresting the condition.12 Affected teeth are often extracted in anticipation of catastrophic fracture and have been replaced with dentures.13,14
In this case report, we describe how a young female patient was managed over a decade and ultimately rehabilitated with dental implants.
Clinical report
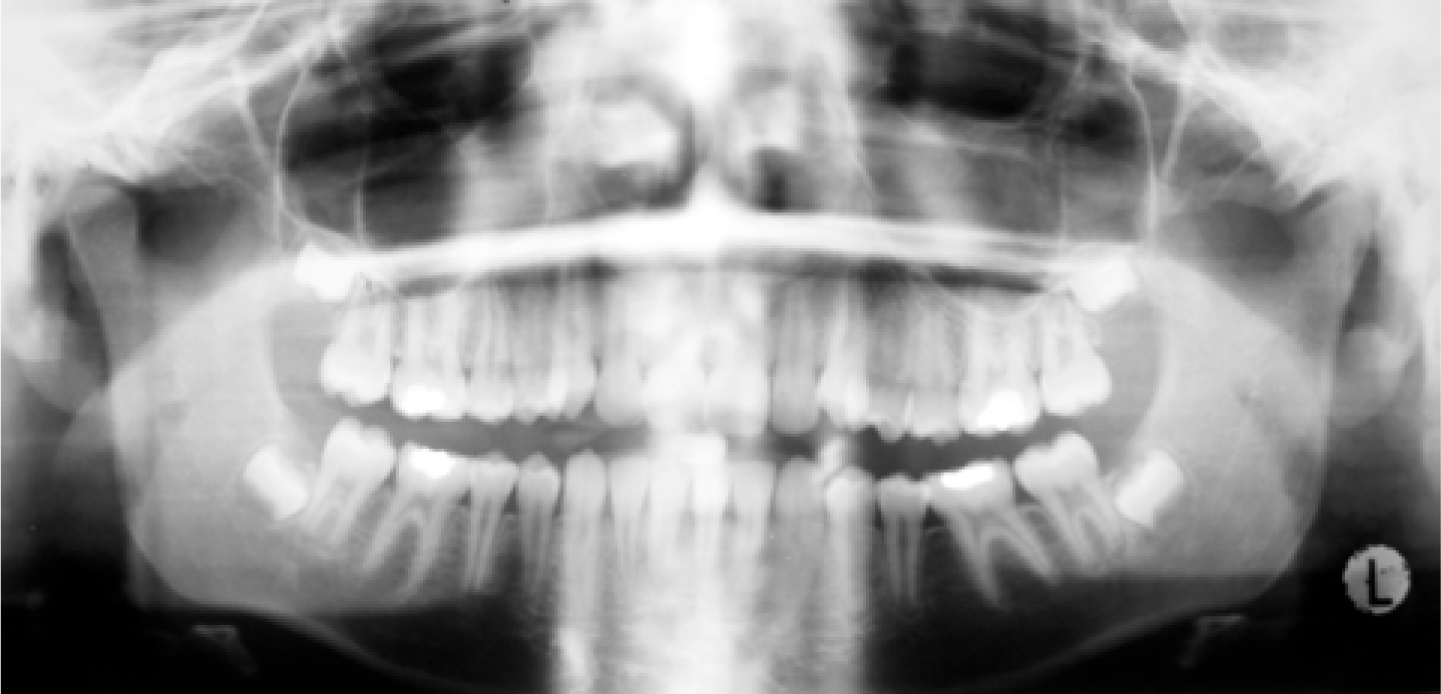
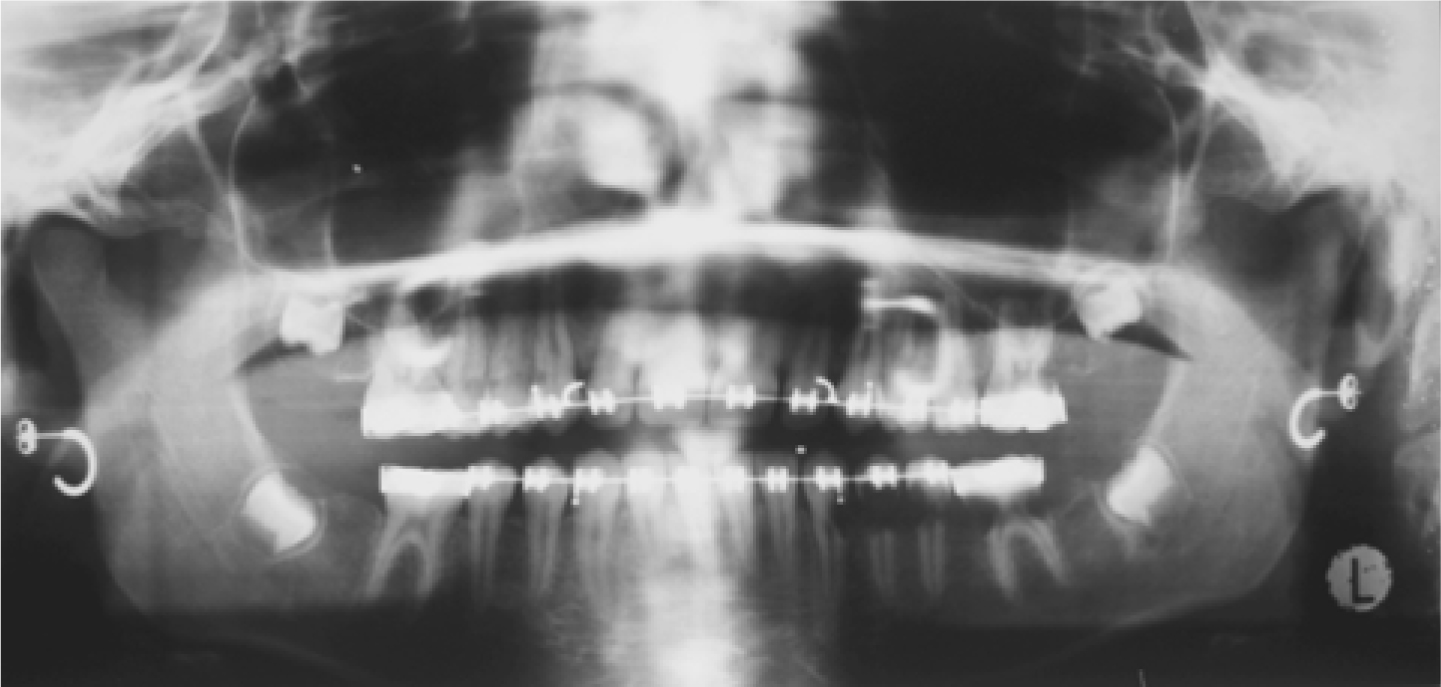
A 12-year-old patient started fixed orthodontic treatment in 2002 (Figure 1). Two years later she was referred to the Leeds Dental Institute (by her orthodontist) just before her maxillary and mandibular fixed appliances were due to be removed. A dental panoramic tomogram (DPT) revealed that LL3, LL4, LL5, LL6, UL6, UR3, UR4, UR5 and UR6 had evidence of cervical resorption (Figure 2).
Figure 1. DPT of the patient taken in 2002: pre-orthodontic treatment.Figure 2. DPT taken in 2004 during orthodontic treatment.
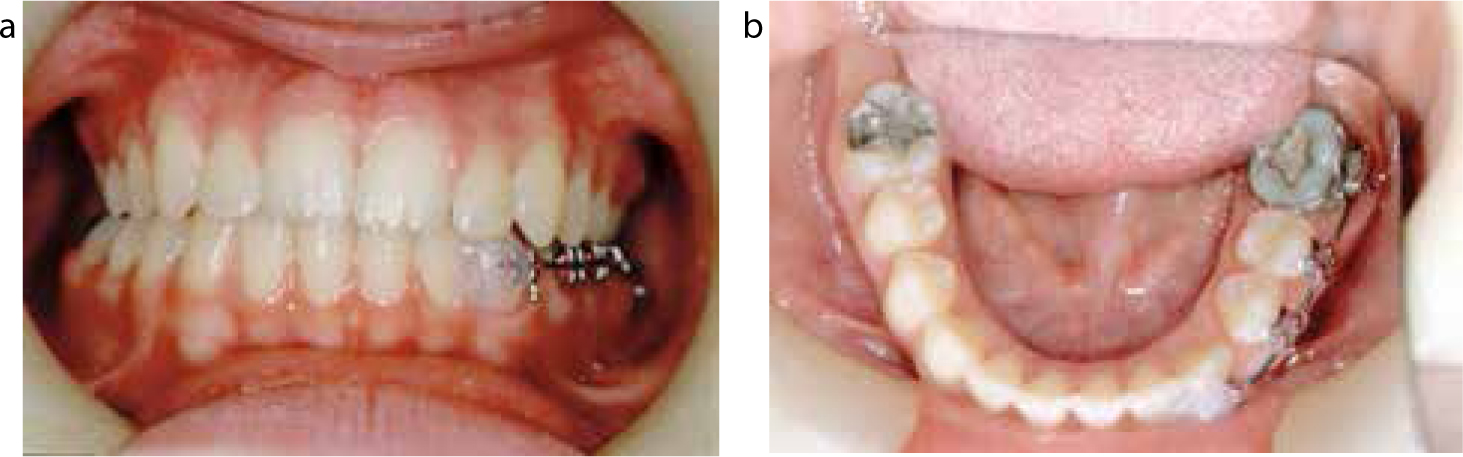
Clinically, in 2004, the patient's plaque control was very good with minimal bleeding on probing. There was no periodontal pocketing associated with any tooth in the patient's dentition or any obvious pathology (Figure 3a and b). At consultation, the patient's family enquired whether the condition was related to the fixed appliance orthodontic treatment. It is possible for apical resorption to affect teeth undergoing orthodontic tooth movement (due to excessive torquing forces).15 However, it is unlikely that the multiple cervical lesions in this patient were due to orthodontic treatment as MICRR has been known also to affect unerupted permanent teeth.1 Therefore, exposure to the oral cavity and some form of environmental insult/trauma does not appear to be a pre-requisite for the condition.
Figure 3.
(a) Labial view of the patient in 2004 after orthodontic treatment had finished. The orthodontic appliance was left in situ in the lower left quadrant to prevent the teeth from decoronating. (b) Lingual view of the patient in 2004. Notice that the teeth appear clinically free of any resorptive defect or pathology.
The crowns of the LL3, LL4, LL5 and LL6 spontaneously decoronated but the roots were left in situ to preserve bone. The remaining resorptive lesions were accessed surgically, granulation tissue was removed and the defects were restored with glass-ionomer cement by the paediatric dentistry team.
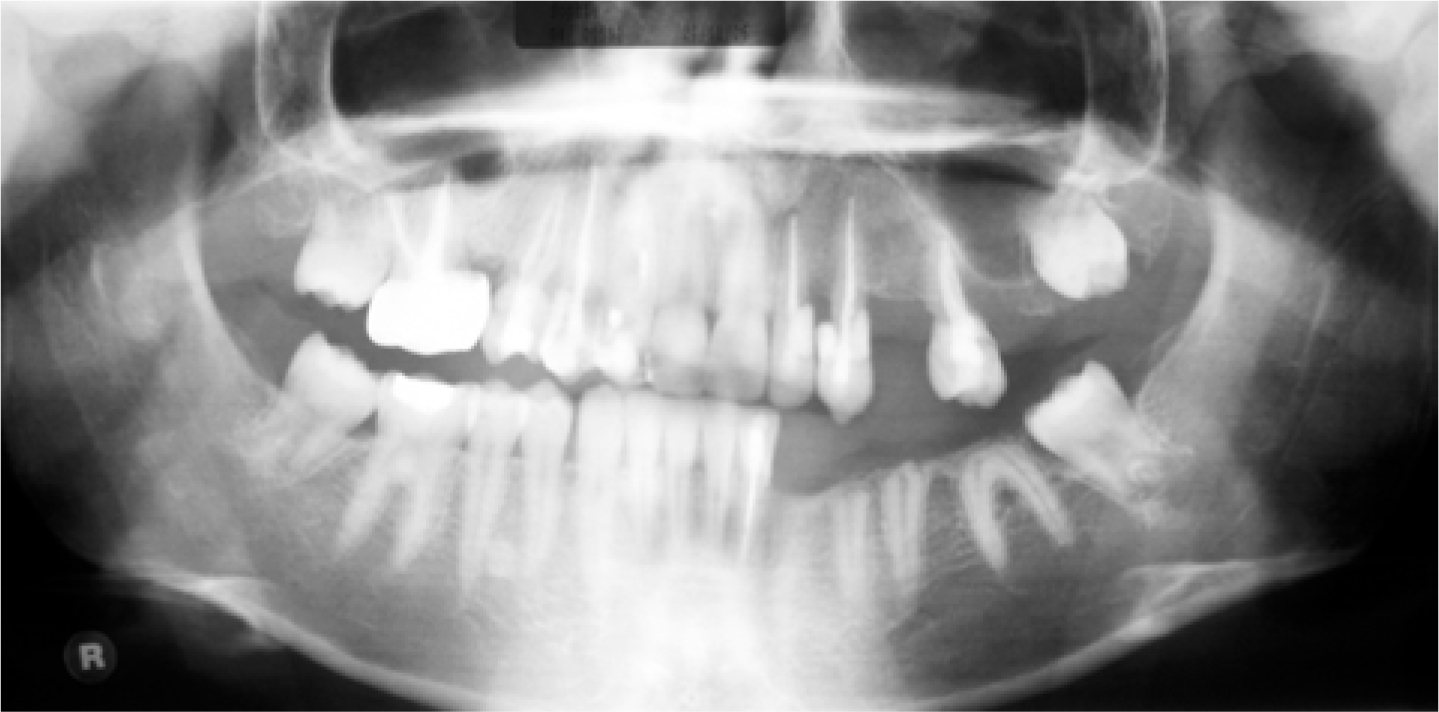
Over the next 2 years, resorptive defects occurred (and re-occurred) on the UR2, UR3, UR4, UR5, UR6, UL2, UL3, UL4, UL5 and LL2 teeth. On multiple occasions, buccal flaps were raised, the resorptive defects curetted and any granulation tissue/coronal tooth structure was sent for further investigation. The UL4, LL3 and UR4 were unrestorable and required extraction. The UR2, UR3, UR5, UR6, UL2, UL3, UL5 and LL2 teeth all required root canal therapy (RCT) as the resorptive defects extended into pulp. The lesions were again restored with GC Fuji IX GP® glass ionomer cement (GIC) by the paediatric dentistry team (Figure 4).
Figure 4. DPT taken in 2006. The teeth affected by resorptive defects have either been root-treated and restored with GIC or extracted if found to be unrestorable. (GC Fuji IX GP®: Leuven, Belgium.)
Histological examination of the granulation tissue revealed that the lesions contained multi-nucleated giant cells, which were consistent with tooth tissue resorption, as well as an associated proliferation of fibrous gingival connective tissue.
In 2006, the patient was 16 years old. It was felt that surgical curettage/repair and RCT of the affected teeth was futile as the lesions were progressive and tended to re-occur. All of the root-treated and surgically repaired teeth shown in Figure 4 started to show clinical and radiographic signs of cervical root resorption. Any further treatment provided in a similar vein would only serve as a short term measure. After joint discussion between consultants in oral/maxillofacial surgery, paediatric and restorative dentistry, it was decided to plan for an implant-based reconstruction.
The heavily restored, root treated UR6, UR5, UR3, UR2, UL2, UL3, UL5 and LL2 teeth, in addition to the LL4, LL5 and LL6 roots, were planned for extraction. A diagnostic wax-up suggested that a functional and aesthetic result could be achieved if the patient was provided with a 4-unit implant-supported bridge in the maxillary left, maxillary right and mandibular left quadrants.
The aforementioned UR6, UR5, UR3, UR2, UL2, UL3, UL5, LL2, LL4, LL5 and LL6 were removed. Radiographs suggested that insufficient bone volume was present in the maxillary left and mandibular left quadrants to allow implant placement. In 2007, the UL2, UL3 and LR2, LR3 regions were augmented with autogenous bone harvested from the patient's chin.
Three 3.3 mm diameter x 13 mm length Brånemark (Nobel Biocare UK Ltd, Uxbridge) implant fixtures were placed in the maxillary left quadrant and three more were placed in the maxillary right quadrant. Three 3.5 mm diameter x 13 mm length Astra implant fixtures (Dentsply, Weybridge, UK) were placed in the lower left mandibular quadrant. The implant system changed as a different clinician took over the patient's restorative care.
The implants were exposed and subsequently restored with 3 sets of 4 unit cement-retained metal ceramic bridges (Figure 5). The patient was satisfied with the treatment she had received at one year review.
Figure 5. (a) Labial view of the patient's 4-unit cement-retained, implant-supported bridges in the maxillary and mandibular arches in 2012. (b) Left buccal view of the patient's 4-unit cement-retained, implant-supported bridges in the maxillary arch replacing the LL2, LL3, LL4 and LL5 and the cement-retained, implant-supported bridge replacing the UL2, UL3, UL4 and UL5 teeth. (c) Right buccal view of the patient's 4-unit cement-retained, implant-supported bridge in the maxillary arch replacing the UR2, UR3, UR4 and UR5 teeth.
Discussion
Given that the MICRR has been known to cluster in families,6 the patient's parents were made aware of this and advised that their other children should attend regular dental appointments for appropriate radiographic examination. Although there are no specific guidelines on which radiographs should be taken, the authors recommend that, as a minimum, patients should have bitewing radiographs taken (in line with their caries risk). This will allow clinicians to evaluate the CEJs of the posterior teeth clearly. However, the bitewing radiographs may have to be supplemented with periapical radiographs of the anterior teeth (if they too are to be evaluated). In this patient, the lesions were identified with tomographic radiographs. Cone Beam Computerized Tomography (CBCT) scanning may have been a better imaging modality to use. Yu et al1 identified early lesions on CBCT scans that were not visible on the plain film images. Furthermore, the resorptive defects were often more extensive than the radiographs would suggest. They also reported that an interesting feature of the condition was that alveolar bone would grow into the root defects, and increase the height of the alveolus. Given that this would promote retention of bone, provision of implant-retained restorations (without grafting) may be possible for some of these patients. It is unknown whether sites of active resorption will have an adverse effect on long-term osseointegration16 and therefore implant retention and success.
Case reports have suggested that the resorptive process can be arrested with bisphosphonate medication.13 However, this may complicate the provision of implants in the future. Yu et al1 suggested a more practical protocol to manage these patients. Lesions that have been detected early can be surgically exposed and restored with glass ionomer cement. This can maintain teeth for many years. However, the condition is progressive. Providing root treatments, surgical curettage and restoration of resorptive defects only appears to play a palliative (but important) role in the management of these patients. If the defects are sub-crestal, consideration should be given to restoring the lesions with a bioactive material, such as mineral trioxide aggregate (MTA) (Dentsply, York, PA, USA) or Biodentine (Septodent, Maidstone, Kent, UK). If a lesion is supra-crestal and in the aesthetic region, composite resin should be used to restore the defect (if moisture control permits). If affected teeth can be retained with these local measures until the patient's growth is complete, alveolar bone levels will be maintained.
As resorption continues to affect larger numbers of teeth, extraction and subsequent prosthodontic rehabilitation should be planned for. In the interim phase, this may take the form of a partial denture. In the long term, the patient may need to be rehabilitated with fixed bridge work. If conventional or resin-bonded bridges are prescribed, the abutment teeth need to be carefully examined to ensure that they are free of resorptive defects. However, the patient must be warned that the abutment teeth may also develop lesions in the future and that the bridges will need regular review. Alternatively, implant-retained crowns and bridges can be provided. Such restorations appear to have a survival rate of 95% over a 5-year period.17 Although implant-retained restorations have a high survival rate, it must still be remembered that a relatively high proportion can develop complications after a period of 5 years, including fracture of the veneering porcelain (14%) and loosening or even fracture of the retaining screws (7%).17 Even if the definitive dental rehabilitation is to be implant-based, the clinician must remember that further teeth may still be lost in the future. Therefore, one must ensure that design features are incorporated to allow for the addition of further teeth. Perhaps if implant-retained bridges are provided for such patients, screw-retained frameworks should be used. This would certainly allow for easy removal, modification and even replacement should further teeth require removal. If, however, all of the teeth are extensively affected by the resorptive process, a clearance and provision of complete dentures/implant-retained overdentures may be necessary.
MICRR is not an endodontic problem. Therefore, patients should not be provided with unnecessary root fillings. They require referral to a secondary care unit for appropriate treatment planning. Furthermore, their family members should be advised to have their own dentitions assessed and monitored as the condition can cluster in families.6 MICRR is also not caused by orthodontic treatment. It is possible for apical resorption to affect teeth undergoing orthodontic tooth movement.15 However, MICRR is not caused or propagated by orthodontic treatment as the condition can be seen in unerupted permanent teeth,1 as well as in patients with no history of orthodontic treatment.4 Therefore, exposure to the oral cavity and some form of environmental stimulus does not appear to be a pre-requisite for the condition.
The restorative, paediatric and surgical dentist have very important roles to play in this multidisciplinary management with regard to treatment planning. They need to be involved early in the decision-making process. Issues regarding the prognosis of compromised teeth and methods of replacement (in both the short and long term) need to be discussed at the outset. These patients will clearly require multiple dental visits and interventions to manage their resorptive defects. Given the progressive nature of the condition, patients should be made aware of this at the beginning of their management. They should also be advised that any teeth which have not been removed will require life-long review, to ensure that they have not developed any new lesions. Although the dental management of MICRR is technically challenging and time consuming, these patients can be managed successfully using a carefully planned multidisciplinary approach.