El-Kamah GY, Fong K, El-Ruby M, Afifi HH, Clements SE, Lai-Cheong JE, Amr K, El-Darouti M, McGrath JA. Spectrum of mutations in the ANTXR2 (CMG2) gene in infantile systemic hyalinosis and juvenile hyaline fibromatosis. Br J Dermatol. 2010; 163:208-234
Thomas JE, Moossavi M, Mehregan D. Juvenile hyaline fibromatosis: a case report and review of the literature. Int J Dermatol. 2004; 43:785-789
Hakki SS, Ataoglu T, Avunduk MC, Erdemli E, Gunhan O, Rahman N. Periodontal treatment of two siblings with juvenile hyaline fibromatosis. J Clin Periodontol. 2005; 32:1016-1021
El-Maaytah M, Jerjes W, Shah P, Upile T, Murphy C, Ayliffe P. Gingival hyperplasia associated with juvenile hyaline fibromatosis: a case report and review of literature. J Oral Maxillofac Surg. 2010; 68:2604-2608
Murray J. Three peculiar cases of molluscum fibrosum in children. Medico-Chirurg Trans. 1873; 38:235-253
Kitano Y, Horiki M, Aoki T, Sagami S. Two cases of juvenile hyaline fibromatosis: some histological, electron microscopic and tissue culture observations. Arch Dermatol. 1972; 106:877-883
El-Kamah GY, Mostafa M. Heterogeneity and atypical presentation in infantile systemic hyalinosis with severe labio-gingival enlargement: First Egyptian report. Dermatol Online J. 2009; 15:(5)
Nofal A, Sanad M, Assaf M, Nofal E, Nassar A, Almokadem S, Attwa E, Elmosalamy K. Juvenile hyaline fibromatosis and infantile systemic hyalinosis: a unifying term and a proposed grading system. J Am Acad Dermatol. 2009; 61:695-700
Juvenile hyaline fibromatosis: impact of periodontal care on quality of life and a patient perspective Zehra Yonel Sabrina Parmar Iain LC Chapple Dental Update 2024 42:7, 707-709.
Authors
ZehraYonel
BDS, MFDS RCS(Ed), FHEA
Department of Periodontology, Birmingham Dental Hospital, St Chad's Queensway, Birmingham B4 6NN, UK
Juvenile hyaline fibromatosis (JHF) is a rare autosomal recessive inherited condition presenting early in life and characterized by the accumulation of hyaline-like tissue in the skin as well as various organs. Gingival overgrowth is a significant oral manifestation. This paper highlights how early and essential periodontal intervention may be necessary to improve mastication and subsequent weight gain, and to eliminate pain and improve the patient's quality of life. Here we highlight the key features of this condition and demonstrate how appropriate surgical management can have a significant impact on a patient‘s wellbeing.
CPD/Clinical Relevance: Juvenile hyaline fibromatosis has a significant impact on patient wellbeing and it is therefore important that clinicians are able to recognize the condition and ensure that patients receive appropriate care and management.
Article
Juvenile hyaline fibromatosis (JHF) is a rare autosomal recessive inherited condition. Impaired collagen synthesis is thought to be the major underlying mechanism behind JHF1, with mutation in the gene encoding the capillary morphogenesis protein 2 (ANTXR2/CMG2) implicated in the development of this disease.2
The condition is characterized clinically by the following features:
The oral complications of JHF extend to limited mouth opening due to joint contracture, difficulty eating and maintaining oral hygiene and a negative impact on speech due to the gingival overgrowth.
Approximately 70 cases of JHF have been reported in the literature to date5 and, owing to the rarity of the condition, debate regarding its exact pathogenesis is ongoing.
The condition was first described in 1873 by Murray, who described it as ‘Molluscum fibrosum’ in children’.1,6 Several terms have subsequently been used to describe the condition and, in 1972, Kitano et al first used the term ‘Juvenile hyaline fibromatosis’, which is the most commonly used term in the literature today.3,7
Infantile systemic hyalinosis (ISH) is a more severe condition which presents clinically with many of the same characteristics as JHF but with additional systemic features, such as deposition of hyaline material in skin, gastrointestinal tract and skeletal muscle.8 ISH is usually identified soon after birth and those with the condition rarely survive beyond two years of age.2,8
Owing to the numerous similarities between JHF and ISH, this has led to many authors, including the authors of this article, to believe that both JHF and ISH are a spectrum of the same disease process. Nofal et al suggest that the conditions are different expressions of the same disorder because, in addition to the similarity of clinical features, the two conditions also have identical histopathological and ultra-structural findings and a similar gene mutation.9 They suggested that a more appropriate terminology would be ‘hyaline fibromatosis syndrome’, which could be further divided into mild, moderate and severe subtypes.9
Case presentation
A 20-year-old male was initially referred to the Periodontal Department at Birmingham Dental Hospital in July 2008 from Ear Nose Throat (ENT) and Maxillofacial colleagues because of the complex oral management he required. The patient was wheelchair-bound with skin lesions, which were particularly prominent on the ears and nose. He also had marked gingival overgrowth. At the point of referral, his mouth opening was limited such that surgical management under general anaesthesia was not appropriate. It was deemed more suitable that his oral care be managed in a specialist periodontal environment (Figure 1).
Figure 1. Limited mouth-opening and extent of gingival hyperplasia.
Upon initial presentation, the patient's mouth opening was limited to approximately 30 mm and he was unable to chew. The maxillary overgrowth was such that the maxillary teeth appeared displaced palatally. Access to the retro-molar fossa for inferior alveolar nerve block local anaesthesia was extremely limited, with the pterygomandibular raphae just being visible. There was limited elasticity in the cheeks and the patient complained of waking with blood on his pillow (Figures 2 and 3).
Figure 2. Extent of palatal overgrowth.Figure 3. Improvement in gingival condition post-surgery.
The preliminary proposed treatment plan involved staged surgical procedures anteriorly to de-bulk the gingival overgrowth and facilitate exposure of the teeth for mastication. Due to the vascularity of the tissue, it was thought that local anaesthesia would be relatively short-lived. The patient had never experienced local anaesthesia intra-orally and, given the ‘cardboard-like’ consistency of the intra-oral local anatomy and sulcus to inject into, the gingival surgery was initially conducted in the lower incisor region only. If the patient was comfortable, a similar procedure was planned for the upper incisor region and, if this proved successful, then an attempt would be made to reduce the posterior overgrowth and de-bulk the hard palate.
The patient was also being treated for his temporomandibular joint dysfunction (TMJD) to improve mouth opening, though with limited success.
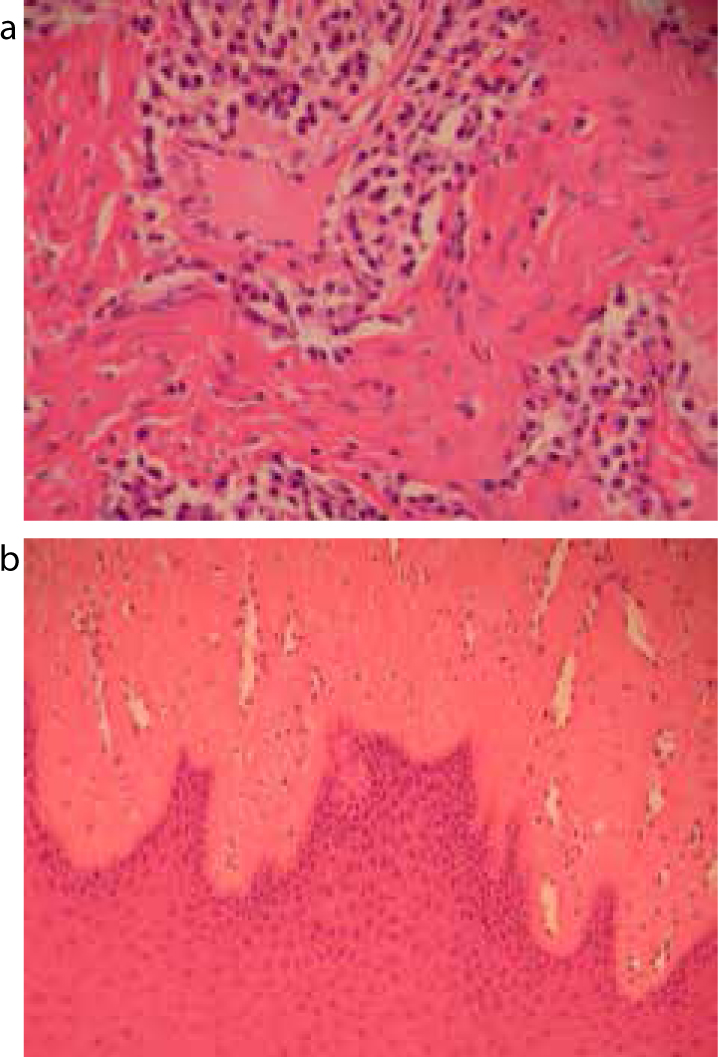
The histopathological report of the excised gingival tissue revealed that the mucosa was covered by parakeratinized squamous epithelium which was acanthotic and hyperplastic. The underlying corium was fibrous, hyperplastic and contained a florid lymphoplasmocytic infiltrate. In places there were sheets of densely hyalinized stroma in which there were fibroblasts present. These latter areas are typical of JHF. The diagnosis of JHF and fibro-epithelial hyperplasia was confirmed, the latter being most likely caused by chronic inflammation (Figure 4).
Figure 4.
(a, b) Histological appearance of JHF.
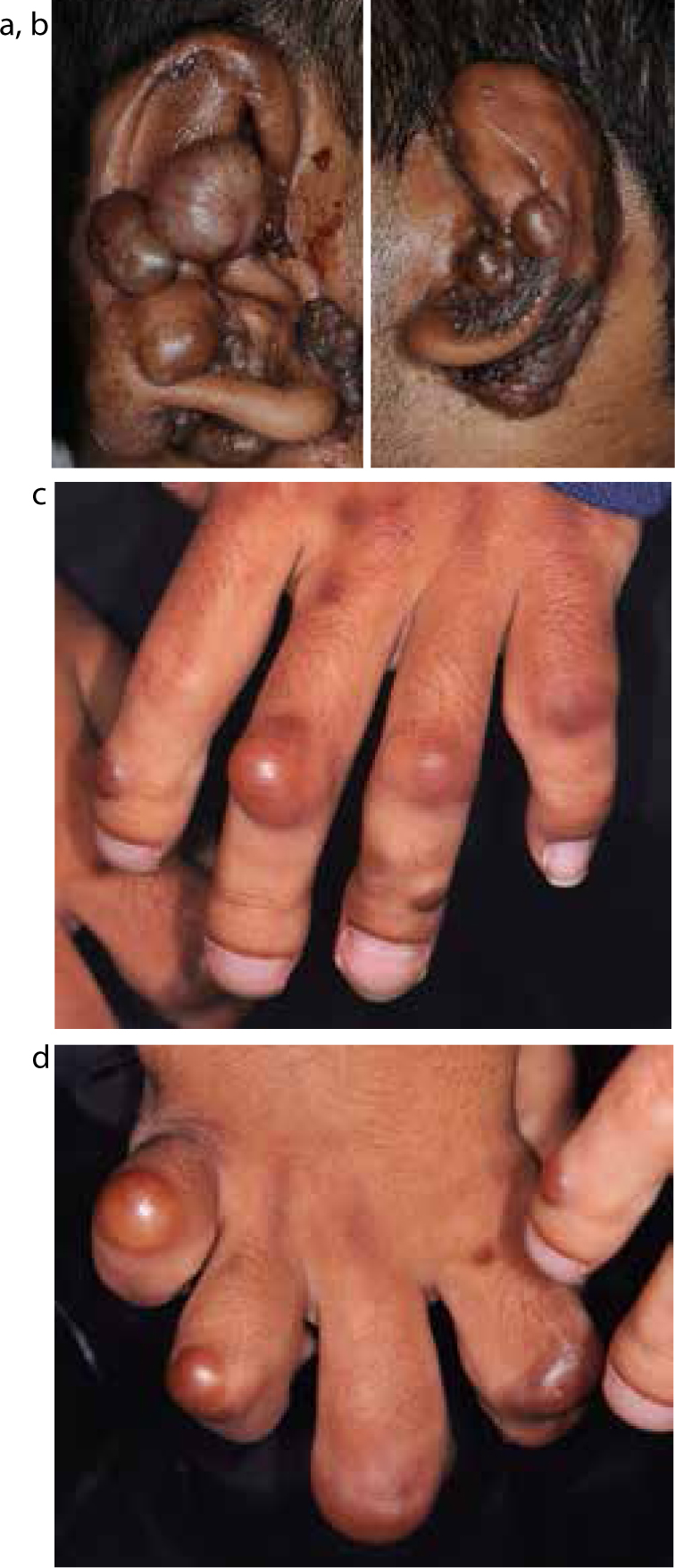
As well as being treated within the Birmingham Dental Hospital for management of his gingival overgrowth and TMJD, the patient was also under the care of ENT, who undertook surgery to ease the discomfort caused by multiple ear nodules in 2011 (Figure 5). Furthermore, in 2011, the patient was treated by the Rheumatology Department to manage his progressive skeletal deformity, particularly related to an increasing scoliosis concave to the right, with flexion contractures to the knees, hips and elbows. Both shoulders had limited mobility, and the right shoulder in particular showed no movement at all. There were also nodules over his fingers and bulbous enlargement of the thumbs (Figure 5). His hip rotation was limited, with hips flexed at 90 degrees, and there were longstanding deformities of the ankles and feet. A history of pressure sores to the heels and back were also reported.
Figure 5.
(a, b, c, d) Nodules to hands and ears.
The patient coped well with the local anaesthesia, as this was acutely painful when administered and he coped well psychologically, given that he had never previously experienced local anaesthesia.
In 2012, the patient returned to the Periodontal Department and was limited to a liquid diet as he was unable to swallow or chew food due to recurrence of his gingival overgrowth and reduced mouth-opening as a result of the TMJD. The patient reported shortness of breath and being aware of a decline in breathing capacity. Further gingival surgery was performed to facilitate improved function and ability to eat.
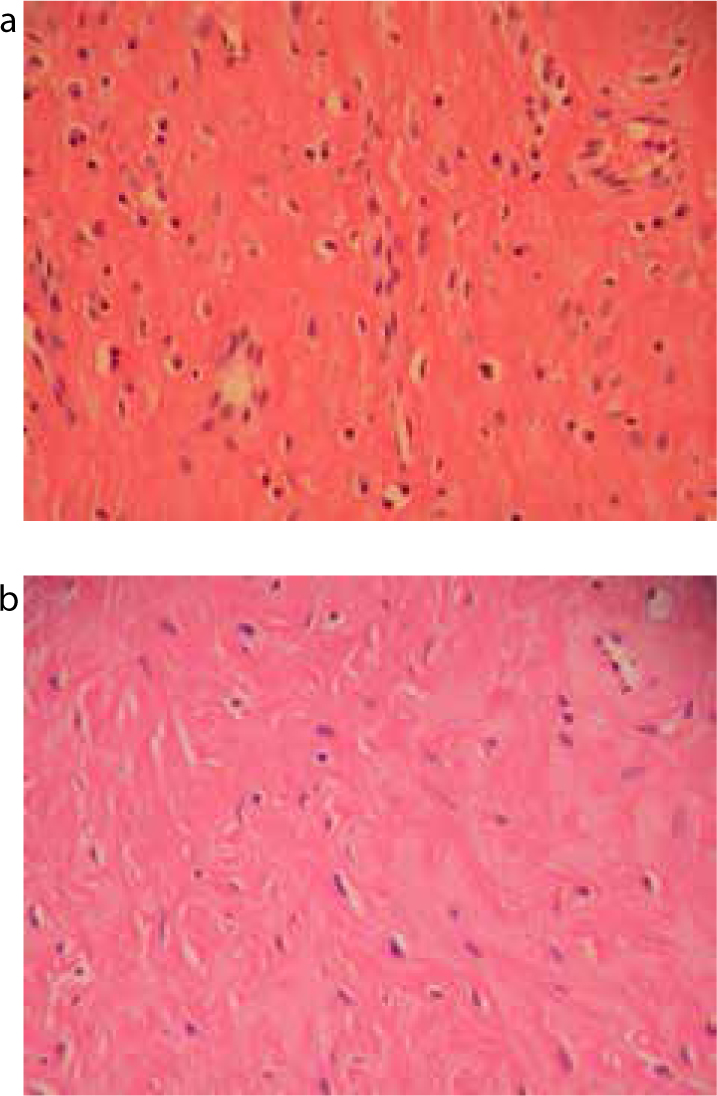
Further samples were sent for histopathological report from the palatal and buccal tissue in the maxillary arch. The underlying sub-mucosal architecture had been replaced by fibromatosis showing extensive hyaline change. The appearance was entirely consistent with JHF and there was associated chronic inflammation (Figure 6 a and b).
Figure 6.
(a, b) Histological appearance of JHF.
In 2013, the patient returned to the Periodontal Department and, over the previous six years, various surgical procedures had been conducted to uncover the patient's teeth which had been buried by overgrowth of gingival tissue (Table 1). Diathermy loops were employed to uncover the palate to reduce the risk of haemorrhage that would be difficult to control as a result of limited intra-oral access. However, surgery was progressively more challenging due to the patient's limited mouth-opening.
Timeline of Surgical Procedures within Birmingham Dental Hospital
Year
Treatment
2008
Gingivectomy lower canine to canine
2008
Gross de-bulking of upper premolar to premolar
2009
Buccal and lingual gingival re-contouring to expose LL4, LL5, LL6 and Gross scale
2009
Excision of overgrown tissue buccal and lingual of LR3, LR4, LR5, LR6
2009
Excisional biopsy of buccal swelling LL6, LL7
2010
Surgical de-bulking of UL7 and LR7
2011
Excision of excess tissue LL2, LL3
2011
Maximum opening recorded as 17 mm between UL1 and LL1
2011
Excised excess tissue at UL4, UL5, UL6
2011
Gingivectomy UL4 to UR4
2013
Referral to Oral Surgery Department for extraction of lower first premolar which was lingually in-standing and causing trauma when eating
2013
Excision of gingival tissue to expose LL6 and UR7, UR6, UR5, UR4, UR3 to expose the teeth and scale of teeth was conducted
2013
Assessed within TMJ Clinic for assessment of TMJD
2014
Awaiting results from CT and MRI scan of TMJD
The major concerns at this point were that, as mouth-opening continued to deteriorate, the patient would be unable to eat and would require a PEG (percutaneous endoscopic gastrostomy). Also with mouth-opening, at less than 17 mm, access to perform surgery and maintaining his airway would be compromised. Referral was therefore made to maxillofacial colleagues within the TMJD clinic of Birmingham Dental Hospital. Wooden sticks and jaw exercises had already been attempted to improve jaw opening, but with little benefit, and therefore further suggestions for management of the trismus were requested.
Patient's reflections
‘My name is Shyam Chandegra and I suffer with a condition called systemic hyalinosis. The condition affects my joints, muscles and causes excessive tissue growth on my fingers and ears. The condition also causes my gums to overgrow which has resulted in me having numerous minor surgeries at the dental hospital. At first it was very difficult for me to chew any solid food due to my teeth being covered by the overgrowth and so it was very difficult for me to partake in family meals. But now, after having some repeated surgery, I can honestly say it has benefited me in such a way that I feel more independent because I am able to go out with friends and family to restaurants. Also, it has made my speech more clear, which helps me a lot as I'm an ambassador for Acorns Hospice for which I undertake numerous tasks which entails speaking in front of different organizations.’
Discussion
This report demonstrates how periodontal intervention, as part of an ongoing care pathway and multidisciplinary team approach, helped improve this patient's quality of life with an otherwise debilitating disease.
Initial management was conservative in order to enable the patient to cope with his first dental injection and with advanced dental surgery. A staged surgical approach was planned in order to establish feasibility of surgical intervention as a treatment modality, given the potential for haemorrhagic sequelae and the surgical challenges faced by the operator (ILC). It was also deemed important to consider patient factors and whether the patient could tolerate or, indeed, desired multiple surgical procedures. The difficulty faced by the operator included that of very limited access due to the patient's marked trismus. Likewise, gaining suitable levels of anaesthesia for patient comfort, and also ensuring airway patency were important considerations.
The patient tolerated the surgery extremely well, and was reviewed regularly and often instigated the process of further surgical procedures as and when he felt they were required. His positive attitude and excellent tolerance to surgical therapy has led to a very smooth communication pathway between himself, his family and the surgical team and a very good mutual understanding of his requirements and the limitations of surgical management. The removal of excess tissue in the posterior region of the oral cavity played an important role in maintaining airway patency. The positive impact of the surgery on the patient's functional and psycho-social wellbeing is evident from his personal reflection of the care offered. Prior to surgical intervention the patient was limited to a liquid diet; the surgery has thus had an impact on his nutritional state and general quality of life.
Conclusion
JHF is a rare condition with fewer than 70 reported cases in the literature (Appendix) and it is therefore important to report information about the condition, how it presents and possible interventions and management strategies in order to aid with diagnosis and management should a patient with similar clinical manifestations of the condition present in the future.
Despite the many symptoms the patient reported due to the condition, including spinal deformity, joint contractures and skin nodules, the provision of early dental management as part of a multidisciplinary team approach had a significant impact on his day-to-day life and greatly contributed to improving the patient's quality of life.
Obituary
Shyam Chandegra sadly passed away on 20th January 2015 aged 27 years; after this manuscript was accepted. Shyam was a truly inspirational young man with an incredibly positive attitude towards life. He worked tirelessly for the Acorn's Children's Hospice as an ambassador and also composing his own music from his wheelchair and met MPs in the House of Commons to speak about health and social care provision and also presented in the House of Lords. For a young man his achievements were huge – Shyam was awarded the Medal of Admiration in Wheelchair Hockey by HRH The Prince of Wales in 2014 and he was personally honoured by the Mayor of Birmingham, receiving a Highly Commended award for being the ‘Pride of Birmingham’. Such an award is only presented to those remarkable individuals who show compassion to society and a hunger to make a difference to peoples’ lives. His father contacted me after he passed away to share Shyam's thanks for the care my team provided for him over many years and the positive impact this had on his quality of life……this from his hospital bed the night before we lost him. There are few people who make me feel so incredibly humble as this amazing young guy did, and we all miss him very much.