Loomans B, Opdam N, Attin T Severe tooth wear: European Consensus Statement on Management Guidelines. J Adhes Dent. 2017; 19:111-119 https://doi.org/10.3290/j.jad.a38102
Sun K, Wang W, Wang X Tooth wear: a cross-sectional investigation of the prevalence and risk factors in Beijing, China. BDJ Open. 2017; 3 https://doi.org/10.1038/bdjopen.2016.12
Liu B, Zhang M, Chen Y, Yao Y. Tooth wear in aging people: an investigation of the prevalence and the influential factors of incisal/occlusal tooth wear in northwest China. BMC Oral Health. 2014; 14 https://doi.org/10.1186/1472-6831-14-65
Poyser NJ, Briggs PF, Chana HS The evaluation of direct composite restorations for the worn mandibular anterior dentition – clinical performance and patient satisfaction. J Oral Rehabil. 2007; 34:361-376 https://doi.org/10.1111/j.1365-2842.2006.01702.x
Al-Khayatt AS, Ray-Chaudhuri A, Poyser NJ Direct composite restorations for the worn mandibular anterior dentition: a 7-year follow-up of a prospective randomised controlled split-mouth clinical trial. J Oral Rehabil. 2013; 40:389-401 https://doi.org/10.1111/joor.12042
Robb ND, Smith BG, Geidrys-Leeper E. The distribution of erosion in the dentitions of patients with eating disorders. Br Dent J. 1995; 178:171-175 https://doi.org/10.1038/sj.bdj.4808695
al-Hiyasat AS, Saunders WP, Sharkey SW The abrasive effect of glazed, unglazed, and polished porcelain on the wear of human enamel, and the influence of carbonated soft drinks on the rate of wear. Int J Prosthodont. 1997; 10:269-282
Mehta SB, Francis S, Banerji S. A guided, conservative approach for the management of localized mandibular anterior tooth wear. Dent Update. 2016; 43:106-112 https://doi.org/10.12968/denu.2016.43.2.106
Rupawala A, Musani SI, Madanshetty P A study on the wear of enamel caused by monolithic zirconia and the subsequent phase transformation compared to two other ceramic systems. J Indian Prosthodont Soc. 2017; 17:8-14 https://doi.org/10.4103/0972-4052.194940
Beddis HP, Durey K, Alhilou A, Chan MF. The restorative management of the deep overbite. Br Dent J. 2014; 217:509-515 https://doi.org/10.1038/sj.bdj.2014.953
Milosevic A, Burnside G. The survival of direct composite restorations in the management of severe tooth wear including attrition and erosion: a prospective 8-year study. J Dent. 2016; 44:13-19 https://doi.org/10.1016/j.jdent.2015.10.015
Ahmed KE, Murbay S. Survival rates of anterior composites in managing tooth wear: systematic review. J Oral Rehabil. 2016; 43:145-153 https://doi.org/10.1111/joor.12360
Burke FJT, Lucarotti PSK. The ultimate guide to restoration longevity in England and Wales. Part 4: resin composite restorations: time to next intervention and to extraction of the restored tooth. Br Dent J. 2018; 224:945-956 https://doi.org/10.1038/sj.bdj.2018.443
Lucarotti PSK, Burke FJT. The ultimate guide to restoration longevity in England and Wales. Part 9: incisor teeth: restoration time to next intervention and to extraction of the restored tooth. Br Dent J. 2018; 225:964-975 https://doi.org/10.1038/sj.bdj.2018.1025
Milosevic A. Direct placement composite: the treatment modality of choice to restore the worn or eroded dentition in primary dental care. Prim Dent J. 2016; 5:25-29 https://doi.org/10.1177/205016841600500301
Gulamali AB, Hemmings KW, Tredwin CJ, Petrie A. Survival analysis of composite Dahl restorations provided to manage localised anterior tooth wear (ten year follow-up). Br Dent J. 2011; 211 https://doi.org/10.1038/sj.bdj.2011.683
Redman CD, Hemmings KW, Good JA. The survival and clinical performance of resin-based composite restorations used to treat localised anterior tooth wear. Br Dent J. 2003; 194:566-572 https://doi.org/10.1038/sj.bdj.4810209
Hemmings KW, Darbar UR, Vaughan S. Tooth wear treated with direct composite restorations at an increased vertical dimension: results at 30 months. J Prosthet Dent. 2000; 83:287-293 https://doi.org/10.1016/s0022-3913(00)70130-2
Edelhoff D, Sorensen JA. Tooth structure removal associated with various preparation designs for anterior teeth. J Prosthet Dent. 2002; 87:503-509 https://doi.org/10.1067/mpr.2002.124094
Smales RJ, Berekally TL. Long-term survival of direct and indirect restorations placed for the treatment of advanced tooth wear. Eur J Prosthodont Restor Dent. 2007; 15:2-6
Milosevic A. The survival of zirconia based crowns (Lava) in the management of severe anterior tooth wear up to 7-years follow-up. Oral Biol Dent. 2014; 2
Hansen TL, Schriwer C, Øilo M, Gjengedal H. Monolithic zirconia crowns in the aesthetic zone in heavy grinders with severe tooth wear. An observational case-series. J Dent. 2018; 72:14-20 https://doi.org/10.1016/j.jdent.2018.01.013
Burke FJT. Survival rates for porcelain laminate veneers with special reference to the effect of preparation in dentin: a literature review. J Esthet Restor Dent. 2012; 24:257-265 https://doi.org/10.1111/j.1708-8240.2012.00517.x
Rinke S, Lange K, Ziebolz D. Retrospective study of extensive heat-pressed ceramic veneers after 36 months. J Esthet Restor Dent. 2013; 25:42-52 https://doi.org/10.1111/jerd.12000
Beier US, Kapferer I, Burtscher D, Dumfahrt H. Clinical performance of porcelain laminate veneers for up to 20 years. Int J Prosthodont. 2012; 25:79-85
Mehta SB, Banerji S. The prevention of tooth wear. Dent Update. 2020; 47:813-820
Burke FJT. Information for patients undergoing treatment for toothwear with resin composite restorations placed at an increased occlusal vertical dimension. Dent Update. 2014; 41:28-38 https://doi.org/10.12968/denu.2014.41.1.28
Blum IR, Lynch CD, Wilson NH. Factors influencing repair of dental restorations with resin composite. Clin Cosmet Investig Dent. 2014; 6:81-7 https://doi.org/10.2147/CCIDE.S53461
Yoshiyama M, Sano H, Ebisu S Regional strengths of bonding agents to cervical sclerotic root dentin. J Dent Res. 1996; 75:1404-1413 https://doi.org/10.1177/00220345960750061201
Kwong SM, Cheung GS, Kei LH Micro-tensile bond strengths to sclerotic dentin using a self-etching and a total-etching technique. Dent Mater. 2002; 18:359-369 https://doi.org/10.1016/s0109-5641(01)00051-3
Wang J, Song W, Zhu L, Wei X. A comparative study of the microtensile bond strength and microstructural differences between sclerotic and Normal dentine after surface pretreatment. BMC Oral Health. 2019; 19 https://doi.org/10.1186/s12903-019-0899-x
Mandibular anterior tooth wear, while sometimes simple to manage, can present a restorative challenge. The evidence on management of worn lower anterior teeth is limited to small case series because the majority of the literature in this field is focused on outcomes in the maxillary arch. This article discusses the presentation and available treatment techniques to manage mandibular anterior tooth wear from a summary of the existing literature and the authors' own experiences.
CPD/Clinical Relevance: Mandibular anterior tooth wear can be challenging to manage.
Article
A Johanna Leven
Tooth wear in mandibular anterior teeth is a common clinical finding and may be a natural physiological process. However, excessive tooth wear can occur as a result of pathological causes. The proportion of patients suffering with premature tooth surface loss has increased over time.1 In terms of their proportion, lower incisors are the smallest teeth and, as such, have a reduced surface area for restoration, but at the same time can be heavily involved in excursive tooth movement, particularly in protrusion. After molars, it is reported that mandibular incisors have the most extensive tooth wear with an average of 1.5 mm lost over 60 years.1 However, a recent study of a Chinese population showed that mandibular incisors were, in fact, the most frequently worn tooth.2 This is likely to be due to incisors being the first teeth to erupt, often being retained longer than posterior teeth in older patients and are, therefore, present in the mouth longer.3 Achieving both a functional and aesthetic result for lower anterior restorations can be a demanding and technique sensitive. A range of treatment options is available, from more conservative composite restorations to full coverage crowns. The choice of treatment modality must be balanced against the remaining tooth structure, removal of additional tooth structure and patient need.
Composite is generally considered to be the treatment modality of choice in the UK for the worn lower incisor, but the evidence base for this is limited.4,5 Many papers discuss survival of anterior composites with mandibular and maxillary composites grouped together, often focusing on maxillary restorations. It is therefore difficult to assess the true survival of mandibular incisor and canine composite restorations. Composite is reported as having good success rates, but often is stated to be a reasonable short-to medium-term restoration, which begs the question of what is the long-term solution.
A review of the literature relating to restoration of worn mandibular anterior teeth and their management is discussed.
Aetiology of tooth wear in mandibular anterior teeth
Various patterns of tooth wear are observed on lower anterior teeth and the cause is often multifactorial. Loss of vertical crown height is typically seen in attritive tooth wear, particularly in patients with an edge-to-edge incisal relationship. Frequently, the incisal edges have matching wear facets on the opposing dentition, which is indicative of a parafunctional habit (Figure 1). Bruxism can result in substantial tooth structure loss over time, leaving limited coronal height for restoration.
Figure 1. Matching wear facets seen on maxillary and mandibular teeth in a patient with a parafunctional habit.
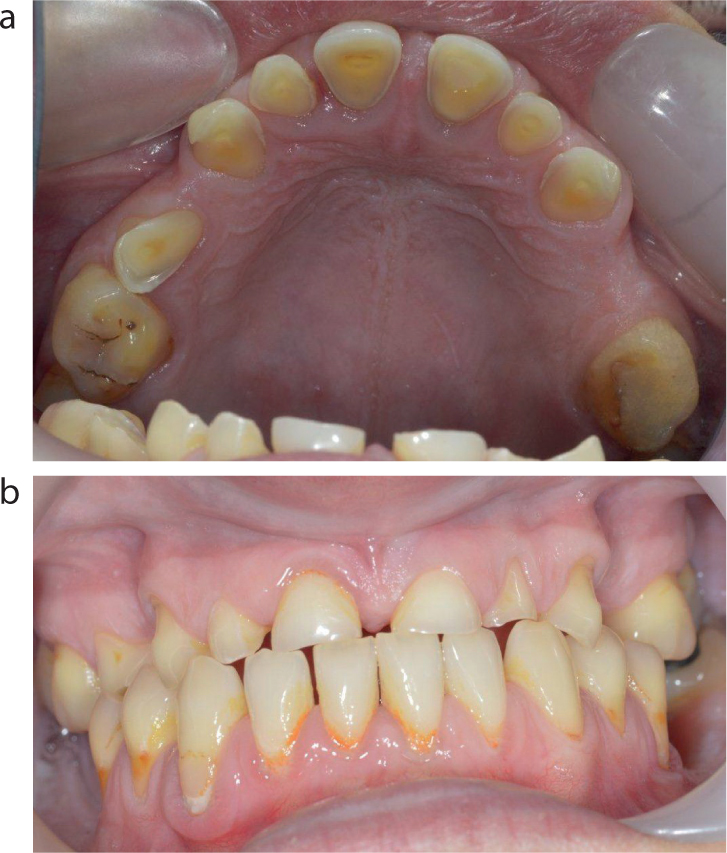
Erosion often presents with incisal edge cupping defects on the incisors and canines where the softer dentine has worn more rapidly than the surrounding peripheral enamel. In general, these cases are straightforward to restore with direct composite conforming to the patient's occlusal vertical dimension (Figure 2). Mandibular anterior teeth are often spared from intrinsic and extrinsic acid attack by the presence of the tongue and salivary buffering, which offers protection (Figure 3).6
Figure 2. Erosive wear of mandibular anterior teeth showing incisal pitting with peripheral enamel halo.Figure 3.
(a, b) Patient who had bulimia nervosa for many wears. Maxillary dentition severely worn while the mandibular teeth remain intact.
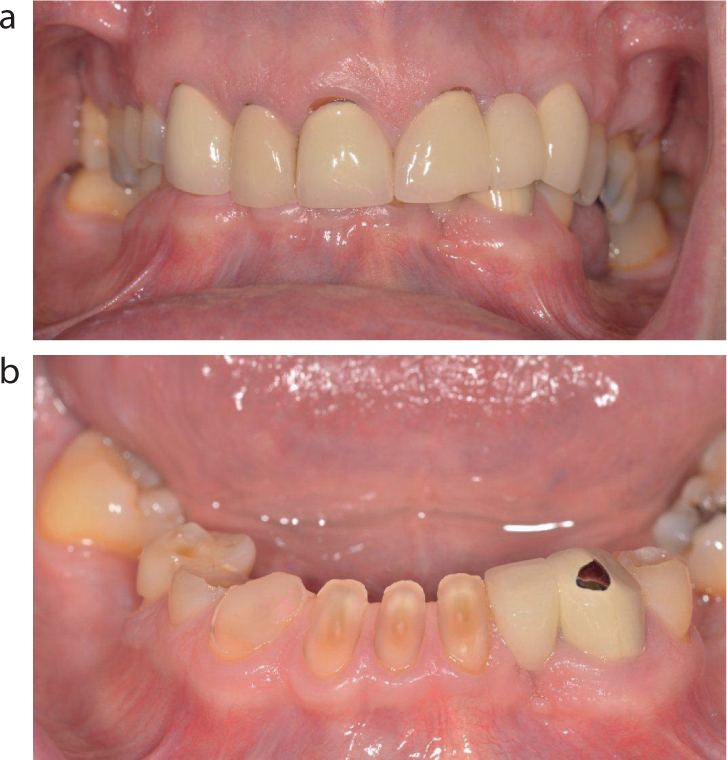
Abrasion commonly presents in the cervical region as a result of overzealous tooth brushing; however, unusual incisal wear patterns due to abrasive factors, such as chewing on pens, fingernails and legs of spectacles, are occasionally observed. Lower anterior teeth may be susceptible to abrasion where unglazed or unpolished porcelain restorations oppose the mandibular teeth and can lead to very severe wear, particularly in patients who also have a high consumption of acidic beverages (Figure 4).7,8 As well as managing the mandibular arch, consideration may have to be given to replacing the maxillary crowns to a metal or unglazed polished monolithic ceramic palatal surface.9
Figure 4.
(a, b) Severe tooth wear of the mandibular anterior teeth in the presence of opposing metal ceramic crowns with unpolished porcelain on the palatal surface.
Lower incisors experience significant shearing forces in the presence of a deep overbite in patients with a Class II division II incisal relationship. This can lead to severe wear, particularly in the presence of parafunction or acid attack, and make such worn teeth very challenging to restore. Labial wear of mandibular incisors can be associated with a traumatic overbite, which may cause additional soft tissue trauma of the labial mucosa, which gradually worsens as further tooth surface loss occurs. This mucosal trauma can be acutely painful for patients (Figure 5). This can be a challenging group of patients to manage: treatment may range from localized direct composites to full mouth rehabilitation using a reorganized occlusion at an increased vertical dimension. Orthodontic treatment may offer an alternative to reduce the overbite, but this can be technically difficult and orthognathic surgery may also required in cases with severe skeletal discrepency.
Figure 5.
(a, b) Patient with a Class II division II incisal relationship and traumatic overbite. The patient had wear facets on the mandibular anterior teeth and gingival recession with trauma to the labial mucosa. Indentation of the upper left central incisor is visible on the mandibular labial mucosa.
Evidence is equivocal to suggest that a lack of posterior support may contribute to anterior tooth wear and premature restoration failure. Replacement of missing posterior teeth may be helpful to restore the occlusal vertical dimension and provide posterior support with either fixed restorations or a removable denture in long-span spaces.10 Anecdotally it is reported that patients increasingly rely on incisors and canines for mastication, which can result in tooth wear that is worsened in the presence of parafunction.11 Smith et al, however, found no clinical significance between the number of missing posterior teeth and tooth wear of anterior teeth.12
Xerostomia is a significant risk factor for tooth wear because of the loss of salivary buffering.2 Tooth wear on mandibular anterior teeth, similar to the rest of the dentition, is, however, commonly affected by multifactorial causes. Numerous risk factors must therefore be controlled for prevention and successful treatment. Identifying the aetiology of the wear as far as possible is vital in tailoring preventive advice and interventions for patients. In cases of mild tooth wear, where monitoring is the most appropriate treatment option, successful prevention will be pivotal in delaying the restorative cycle.
Restoration of worn mandibular anterior teeth
There are numerous studies reviewing survival and success of various types of restorations, but few include survival of these restorations in tooth wear patients, particularly for those with a parafunctional habit. Papers discussing anterior teeth mainly focus on maxillary teeth, therefore there is limited evidence regarding restoration of mandibular anterior teeth specifically.
Composite restorations
A systematic review of anterior composite survival by Ahmed and Murbay in 2015 included only five studies.13 These studies were of small patient cohorts (the largest being 31 patients) and the studies were found to be considerably heterogeneous, making meta-analysis impossible. The review found survival rates of over 90% at 2.5 years and over 50% at 5 years for direct composite.
A prospective randomized controlled trial included in the systematic review by Ahmed reported a success rate of 85% at 7 years for direct composite restorations of the lower anterior teeth.5 This paper was a 7-year follow up of the same cohort of patients described in the 2007 paper by Poyser et al,4 who identified the most common forms of ‘failure’ to be marginal breakdown and staining. This was a small study in which 15 patients were followed up; however, this is the only study looking specifically at mandibular anterior composite survival in tooth wear patients of which the authors are aware. Milosevic and Burnside's11 prospective study of composite survival in a cohort of 164 patients with 1010 restorations followed up over 33.8 months did break down the survival at the tooth level. Although not statistically significant, analysis showed a higher percentage of failures in the lower arch (9.6%) compared to the upper arch (6%); however, most restorations were placed in the maxillary arch.10,11 Conversely, Burke and Lucarotti14 reported that mandibular incisor composite restorations perform slightly better than maxillary incisors in terms of time to re-intervention in a study that analysed data from payment claims submitted from dental practitioners to the Dental Practice Board in England.14
Risk factors for failure of composite are reported as: male gender, which is likely to be due to increased occlusal forces compared to females;15 older age, which may be attributed to increased sclerotic dentine reducing bond strengths;16 and incisal relationship. However, the evidence is equivocal on this. Studies have reported differing higher failure rates in Class I, Class II division II and Class III, edge-to-edge incisal relationships.12,17–19
Crowns
Full-coverage crowns are hard to justify for lower incisors in particular because they are already diminutive teeth and preparation for metal–ceramic and all-ceramic crowns are reported to result in 63% and 72% tooth structure removal, respectively.20 This is exceptionally destructive on an already worn tooth. Lucarotti and Burke 15 reported that, although crowns and veneers had increased time to re-intervention compared to composite, at 15 years, 25% of crowned incisors required extraction compared to 16% for resin composite and 7% for veneers. A study comparing the survival of composites and full-coverage crowns in patients with advanced tooth wear found that survival rates at 10 years was 62.0% and 74.5%, respectively.21 In reference to anterior restorations, composite was reported to have a 58.9% survival compared to a 70.3% survival of crowns at 10 years. The authors reported that the most common cause of failure of composite was bulk fracture, which could be easily remedied with replacement or repair, whereas the incidence of pulpal problems leading to extractions or endodontic treatment was higher in patients receiving crowns. The authors attributed this finding to the more destructive preparation of the tooth.21
Evidence for the use of zirconia crowns in anterior tooth wear is limited to case series. Milosevic reported the estimated mean survival time of 161 zirconia-based crowns placed on maxillary and mandibular anterior teeth in 30 individuals to be 74 months, with a higher incidence of debond or delamination of layered surface ceramic reported in cases of attrition and bruxism.22 Hansen et al reported success in a small cohort of bruxist patients with anterior tooth wear treated with monolithic zirconia. Patients were followed up after 1–3 years and 94.1% had no chipping or bulk fracture at review.23 Dentine-bonded crowns, sometimes referred to as full-coverage porcelain veneers, require reduced preparation compared to conventional crowns and may have some application in non-parafunctional patients, but careful patient selection is essential. In cases of erosion or attrition, Burke reported on 48 dentine-bonded crowns prospectively followed up for 4 years and observed a failure rate of 6%; however, only four crowns were placed on lower incisors.24
Veneers
Ceramic veneers may be useful in cases of labial wear provided there is adequate peripheral enamel for bonding. In a non-tooth wear cohort, Rinke reported equal survival rates of ceramic veneers in maxillary and mandibular incisors at 36 months, the survival rate according to Kaplan–Meier analysis was 95.1%.25 Lucarotti and Burke found that veneers in incisor teeth perform more favourably than other restorations, such as crowns and composite, in terms of time to extraction of the tooth.15
Beier et al26 reported the estimated survival of porcelain laminate veneers in maxillary and mandibular anterior teeth as 93.5% at 10 years and 82.93% at 20 years with statistically significant higher failure rates found in bruxist patients with the hazard ratio for bruxism reported as 7.74. Success rates of veneers can be improved in parafunctional patients with good patient compliance in wearing occlusal splints to protect the restorations.27
Composite build up technique
The composite build up technique is detailed thoroughly in several papers.4,8,12,28 Either a lingual silicone stent to incrementally build up composite, or a full-coverage stent with injection moulding of composite is used. A lingual stent is used particularly when dual shade composite is needed to layer the composite restorations to replicate enamel translucency. While aesthetically superior results can be achieved, this is dependent on clinician skill because this is a more technically demanding technique. The injection moulding technique using a translucent full coverage stent often works well for lower anterior teeth as aesthetics are generally not as critical as in the maxillary anterior teeth; however, very satisfactory results are still achieved with this technique. The difficulty of controlling contact points is one of the main drawbacks in using the injection moulding technique owing to the excess composite flash that can flow on to adjacent teeth, and so more time will be needed to polish the proximal surfaces of the restorations. Care should be taken to ensure the embrasure spaces are blocked out with polytetrafluroethylene (PTFE) tape, Wedjets (Coltene, Alstätten, Switzerland), or similar to ensure these areas are left cleansable with interdental brushes or floss. In circumstances where there is insufficient incisal enamel to which to bond, consideration should be given to extending the composite onto the lingual or labial enamel to take advantage of an increased surface area for more predictable bonding. Where only labial wear is present, a labial translucent guide, rather than a full-coverage guide, can be helpful because this allows the wax-up to easily be transferred, but allows for excess composite to be removed on the lingual aspect prior to curing (Figure 6).
Figure 6. Composite restoration of lower anterior teeth, which, pre-operatively, had labial wear. Injection moulding technique with a labial stent was used.
Composite is weak in thin section, and a minimal thickness of 1.5–2.0 mm is required, particularly in cases where the Dahl technique is used to increase the vertical dimension on the composite restorations.29,30 Where tooth wear is mild, it may be best to monitor the wear and avoid the cycle of restoration maintenance, especially when patients have no dentine hypersensitivity or significant aesthetic concerns.
Lower anterior teeth are often restored as part of a wider treatment plan to manage generalized tooth wear. However, when only one or two mandibular incisors require restoration, composite should ideally have only light occlusal contact or be kept slightly out of contact. This can help protect the restorations, particularly in patients with a parafunctional habit (Figure 7).
Figure 7. Patient had issues with lower central incisor composites debonding, therefore restorations were kept slightly out of contact when replaced, and patient was provided with an occlusal splint for night wear.
Patients should be provided with full coverage occlusal splints to protect the teeth and restorations from further wear, although patient compliance with wearing splints does vary.4 There is no strong evidence to support the use of hard stabilization splints over soft splints in the non-temporomandibular joint dysfunction patient to prevent further tooth wear. It has been reported that hard stabilization splints may reduce unwanted tooth movement;31 however, cost and clinician skill may not make this feasible. From the authors' experience, not all patients are compliant in wearing hard stabilization splints and may find soft or bilaminar splints more acceptable. Ultimately, the decision on splint type should be made on an individual patient basis.
Repair/replacement of failed composite
Composite restorations will fail in time, either with minor chipping, complete fracture or debond. Replacement or repair of these restorations can be more than just technically demanding as patients may have lost confidence in the material, particularly if there has been repeated debond. It is therefore essential at the treatment planning stage to emphasize to patients that the composite will require maintenance and replacement, and this should be expected, particularly in patients with a bruxism. It should be explained that composite failure, while frustrating generally, has less severe consequences than indirect restorations, which can result in catastrophic failure more frequently leading to tooth loss.14 Incidentally, Dental Update published an information leaflet for patients undergoing resin restorations in the management of tooth wear, which is available in the issue archives.32 If the composite restoration fails early in the restorative cycle, this may be due to technical errors, such as inadequate moisture control, but care should be taken to reassess the occlusion. Excursive movements in particular should be assessed because heavy occlusal contact can often be the reason for premature failure. Ideally, there should be shared contact in protrusion on the lower incisors. Minor fractures can often be simply polished rather than rebuilt. If there is limited coronal tooth structure, composite might be used as an initial measure, but premature or repeated failure, particularly in severe wear, may suggest the need for alternative treatments, such as surgical crown lengthening or prosthetic replacement with an overdenture.
If composite is to be repaired, Blum et al33 advocate the use of a CoJet sandblaster (3M ESPE, Seefeld, Germany) to tribochemically coat the surface of the remaining composite, followed by application of a silane primer and adhesive bonding agent. Alternatively, a fine grit diamond or tungsten carbide bur can be used on exposed tooth tissue and composite substrate prior to bonding, to remove the salivary pellicle and create a fresh surface for bonding, followed by acid etching prior to bonding. It is recommended to use the same bonding system and composite as the original restoration; however, that may not always be feasible. Resin bond strength of non-carious sclerotic dentine is reported to be significantly lower than that of normal dentine. Older patients may, therefore, experience more composite failure.34,35 An in vitro study by Wang et al found that pre-treatment using 35% phosphoric acid for 30 seconds and 5% or 10% sodium hypochlorite for 60 seconds resulted in significantly higher microtensile bond strengths in sclerotic dentine.36
Ideally, the patient or dentist will have retained the laboratory wax-up and stents used during the initial composite rehabilitation making replacement much easier. It is suggested that composites are replaced or repaired as they fracture or debond, and not allow several to fail before replacement, because this may lead to general failure of the composite rehabilitation as the remaining restorations can become more heavily loaded in the occlusion leading to a snowball effect of failing restorations.
Conclusion
Management of mandibular anterior tooth wear cases can be very challenging and these patients generally have high maintenance burdens, particularly patients with parafunctional habits. There is limited available evidence on management of worn mandibular anterior teeth. Direct composite restorations have the distinct advantage of being conservative to tooth structure and do not result in significant damage to the residual tooth structure when composites fail. However, composite does require significant maintenance and that is something patients must be fully informed about and consented for to avoid frustration for both patient and clinician. Repair and replacement of composite should be expected and anticipated. The reality is that there are no ideal long-term solutions for worn lower anterior teeth, and repeated composite restoration is, at present, the management of choice for many patients. In the authors' experience, when planned carefully and carried out to a high standard, composite can be a predictable and conservative treatment modality. Indirect restorations should be used with caution because, although the initial maintenance is lower, the failures can be catastrophic, particularly in the presence of parafunction, and teeth can ultimately be rendered unrestorable. Before embarking on rehabilitation of worn mandibular anterior teeth, clinicians must inform patients of the risks and repeated maintenance involved with proposed treatment and every attempt should be made to control patient risk factors to prevent further tooth wear.