Sun MZ, Oh MC, Safaee M Neuroanatomical correlation of the House-Brackmann grading system in the microsurgical treatment of vestibular schwannoma. Neurosurg Focus. 2012; 33
Cha CI, Hong CK, Park MS, Yeo SG. Comparison of facial nerve paralysis in adults and children. Yonsei Med J. 2008; 49:725-734 https://doi.org/10.3349/ymj.2008.49.5.725
Scully C. Oral and Maxillofacial Medicine: The Basis of Diagnosis and Treatment.Edinburgh: Churchill Livingstone; 2008
Gussen R. Pathogenesis of Bell's palsy. Retrograde epineurial edema and postedematous fibrous compression neuropathy of the facial nerve. Ann Otol Rhinol Laryngol. 1977; 86:549-558
Abdulsalam AJ, Alsairafy MA, Al-Hashel JY, Alkandari SA. Bilateral facial palsy after cosmetic filler injections: is pain really the price of beauty?. Rev Neurol (Paris). 2020; 176 https://doi.org/10.1016/j.neurol.2020.02.004
Lee JI, Kang SJ, Sun H. Skin necrosis with oculomotor nerve palsy due to a hyaluronic acid filler injection. Arch Plast Surg. 2017; 44:340-343 https://doi.org/10.5999/aps.2017.44.4.340
Bae IH, Kim MS, Choi H Ischemic oculomotor nerve palsy due to hyaluronic acid filler injection. J Cosmet Dermatol. 2018; 17:1016-1018 https://doi.org/10.1111/jocd.12498
The demand for lip augmentation has increased over the recent years. Facial palsy is not a frequently encountered presentation post cosmetic fillers, there is little literature on this. Therefore, it is important to highlight the findings of this case and to discuss the possible pathophysiology and management, should a similar case arise.
CPD/Clinical Relevance: This case report discusses an incidental finding of left-sided facial nerve palsy post lip augmentation.
Article
The demand for lip augmentation has increased over the recent years, especially for cosmetic reasons.1 Before treatment is undertaken, it is therefore important to be aware of the possible risks and complications, so if they were to arise, they can be managed appropriately. While giving history, patients may attribute their symptoms to a preceding event. It is important to differentiate whether there is causation or an association between the two, when trying to diagnose. This case report discusses an incidental finding of left-sided facial nerve palsy after lip augmentation, and its management.
Case report
A 20–year–old woman presented to the Emergency Department (ED) with left-sided facial weakness after lip augmentation. She had both her upper and lower lips augmented with Revolax (Across, Korea) filler by a beautician, Revolax being a dermal filler that contains lidocaine and hyaluronic acid.2 The patient's past medical history was unremarkable, and she had no known allergies. She had received lip augmentation with Revolax several times previously by the same beautician, with no known complications.
After the procedure, the patient experienced some difficulty moving the left side of her upper lip, which she associated with the post-procedure swelling. However, the following day, she had no movement of her upper lip on the left side. When the weakness had not resolved over the next 3 days, she attended the ED. She was seen by several doctors who were unsure of the cause and management. Subsequently, she was referred to Oral and Maxillofacial Surgery (OMFS) and was followed up in the outpatient clinic the next day.
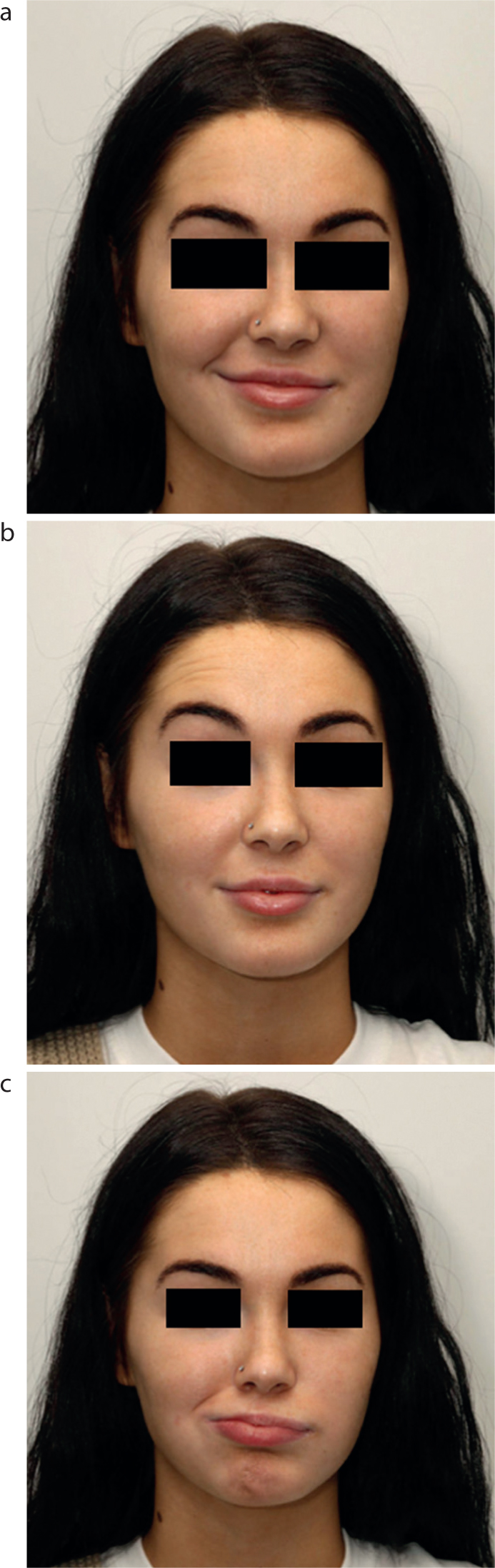
On examination, she was unable to raise her upper lip on the left side, blow her left cheek, close her left eyelid and raise her left eyebrow (Figure 1). She had good corneal protection with minimal sclera exposed on closure of the left eye. Intra-orally, no abnormalities were noted. She complained of a buzzing sound in her left ear, for which she was referred to Otorhinolaryngology (ENT). The ENT assessment showed no obvious ear pathology.
Figure 1. The patient had difficulty with various facial movements. She was (a) unable to raise the upper left side of her lip when smiling; (b) had difficulty raising her left eyebrow (note the unfurrowed left forehead); (c) and had an inability to blow out her left check (note the obliterated left nasolabial fold).
Her overall presentation correlated to House-Brackmann IV lower motor neurone (LMN) VII weakness. In this regard, the extent of facial nerve palsy is graded using House-Brackmann classification, for which there are six grades, depending on clinical presentation (Table 1).
Grade
Description
Clinical findings
I
Normal
No facial nerve weakness
II
Mild dysfunction
Slight weakness noticeable on close inspection, may have very slight synkinesis
III
Moderate dysfunction
Obvious, but not disfiguring difference between two sides. Noticeable, but not severe synkinesis or hemifacial spasm. Complete eye closure with effort
IV
Moderately severe dysfunction
Obvious weakness of disfiguring asymmetry, normal symmetry and tone at rest but unable to complete eye closure
V
Severe dysfunction
Only barely perceptible facial muscle motion, asymmetry at rest
VI
Complete paralysis
No movement
The patient had no obvious signs of viral infection and did not complain of any obvious contributory factors to facial weakness apart from the recent lip augmentation. However, it was difficult to explain how lip augmentation could have directly caused palsy of all five branches of the facial nerve on the left side. If it was an immune-mediated response to the lip filler, then both the right and left facial nerves would have been affected. Therefore, her diagnosis was of Bell's palsy.
The patient was prescribed prednisolone 40 mg, once daily for 7 days, along with Artelac Nighttime 0.2% eye gel, with the plan to follow-up in 3–4 weeks. She was advised to wear an eye patch on the left eye during sleep, to help prevent the eye from drying out.
At her 4-week review, the patient reported that she had no problems, and an examination revealed full recovery of the left-sided facial weakness (Figure 2). Her symptoms started to subside gradually after starting prednisolone, and the symptoms had completely settled by the end of third week.
Figure 2. At the 4-week review, the patient showed (a) re-establishment of a symmetrical smile; (b) ability to raise both eyebrows; and (c) could blow out both cheeks.
Discussion
Facial nerve palsy is an usual presentation after lip augmentation, and therefore it is important to highlight the findings of this case report. The cause of this sudden onset of facial palsy is not known. However, the patient was convinced that her symptoms were caused by the coincidental lip augmentation. Thorough discussion took place with the patient to explain that it is very difficult to explain how lip fillers could have caused left-sided facial palsy, and even though these events followed one another, it cannot be proved that one caused the other. As a result, the diagnosis made was Bell's palsy, a condition that is idiopathic.
Literature shows that the most common causes of facial palsy in adults are Bell's palsy, followed by infection, trauma, iatrogenesis and tumours.4
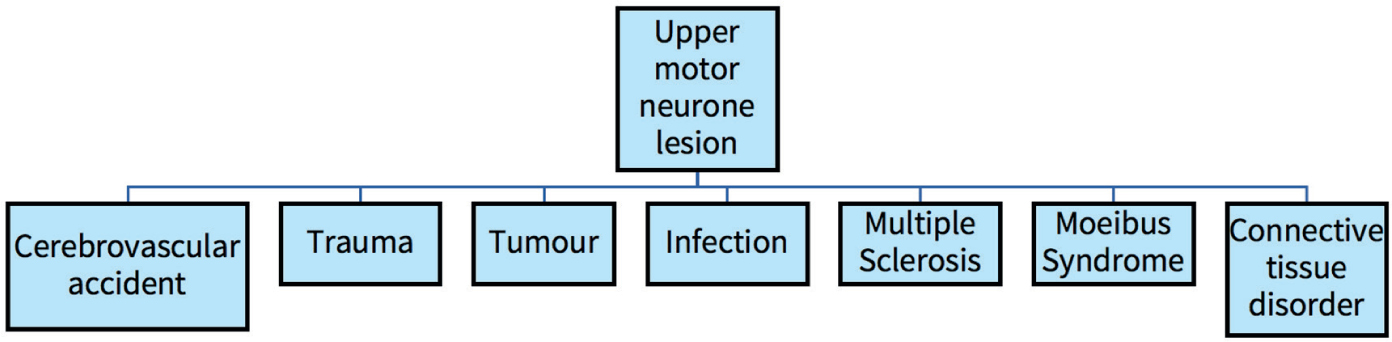
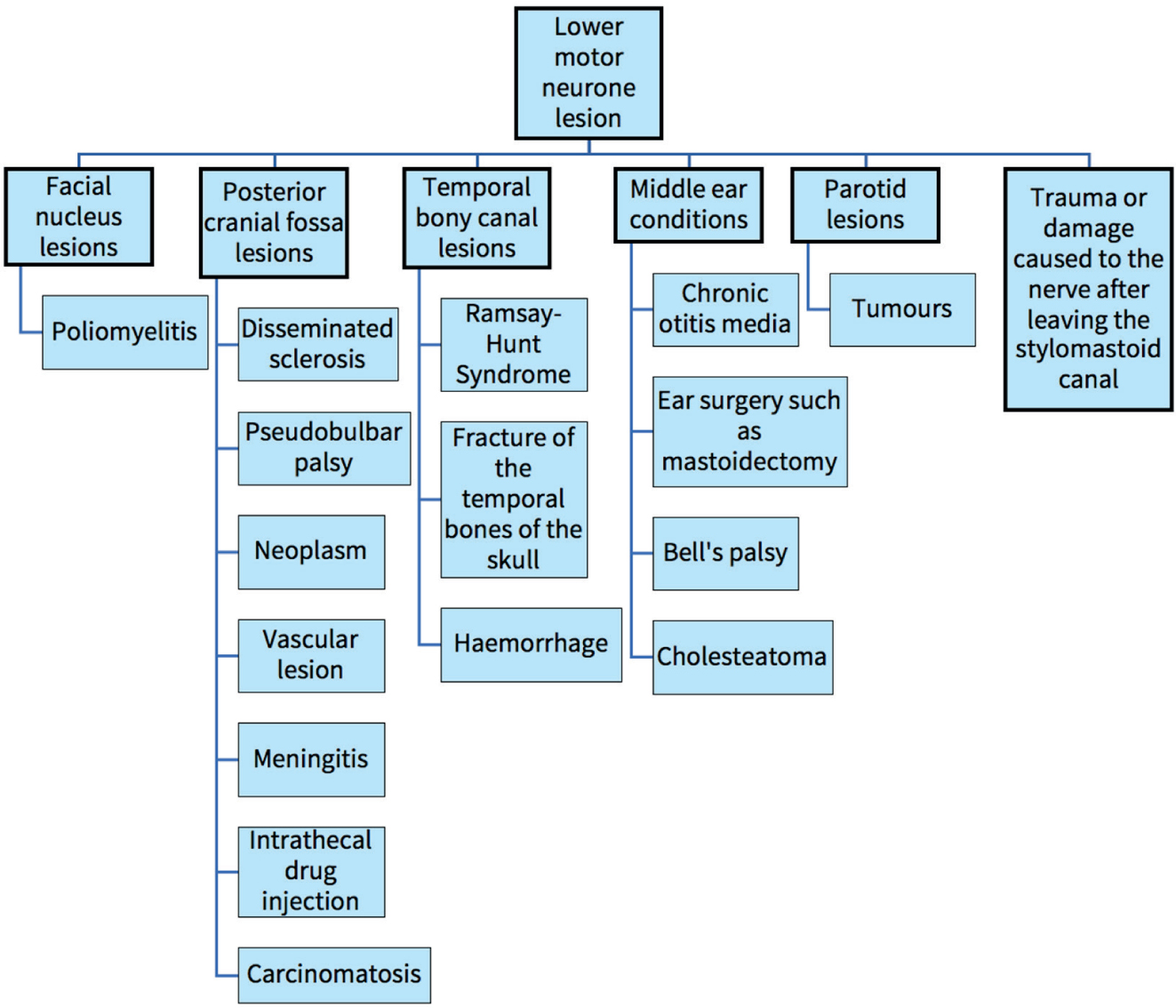
The causes of facial nerve palsy can be divided into upper or lower motor neurone lesions (Figures 3 and 4). Clinical presentation can help to distinguish between the two as there is some sparing of the frontalis and orbicularis oculi muscles for upper motor neurone palsy owing to the upper face receiving bilateral upper motor neurone innervation.5
Figure 3. The different upper motor neurone lesions.5Figure 4. The different lower motor neurone lesions.5
The patient presented with facial nerve palsy of both her upper and lower face, therefore demonstrating lower motor neurone palsy. The pathophysiology of Bell's palsy is unknown but is thought to be due to retrograde epineurial compression oedema with ischaemia of facial nerve.6 This could be through vasospasm, from any cause, along any facial nerve branch.6 Another theory is that an autoimmune response is involved in Bell's palsy.7 It could be possible that the patient developed hypersensitivity to the material over time and responded in this manner. However, it will be difficult to explain why the symptoms were only present unilaterally.
Similar clinical presentation after cosmetic filler injection has been reported, which described a patient who experienced bilateral facial nerve weakness after having dermal fillers to treat his nasolabial and marionette lines.8 Palsy of other cranial nerve branches, in particular oculomotor nerve palsy, has also been reported after the use of dermal fillers. This occurred as a result of ischaemia or occlusion of an artery, leading to nerve palsy.9,10
Conclusion
Although the pathophysiology may be unclear for this presentation, it is important to highlight uncommon presentations or complications that may occur after treatment. This can help with understanding and managing similar cases, should they arise.
It is also important to differentiate cause and association so that accurate discussions can take place with the patient, and they can have a better understanding of the condition affecting them. This may be difficult if there is little scientific literature. Therefore, further research can help to improve understanding of the pathophysiology of similar presentations.