Anderson JA, Brewer A, Creagh D Guidance on the dental management of patients with haemophilia and congenital bleeding disorders. Br Dent J. 2013; 215:497-504 https://doi.org/10.1038/sj.bdj.2013.1097
Escobar MA, Brewer A, Caviglia H Recommendations on multidisciplinary management of elective surgery in people with haemophilia. Haemophilia. 2018; 24:693-702 https://doi.org/10.1111/hae.13549
Collins PW, Liesner R, Makris M Treatment of bleeding episodes in haemophilia A complicated by a factor VIII inhibitor in patients receiving emicizumab. Interim guidance from UKHCDO Inhibitor Working Party and Executive Committee. Haemophilia. 2018; 24:344-347 https://doi.org/10.1111/hae.13495
Knight T, Callaghan MU. The role of emicizumab, a bispecific factor IXa- and factor X-directed antibody, for the prevention of bleeding episodes in patients with hemophilia A. Ther Adv Hematol. 2018; 9:319-334 https://doi.org/10.1177/2040620718799997
Mahdi AJ, Obaji SG, Collins PW. Role of enhanced half-life factor VIII and IX in the treatment of haemophilia. Br J Haematol. 2015; 169:768-776 https://doi.org/10.1111/bjh.13360
Oldenburg J, Mahlangu JN, Kim B emicizumab prophylaxis in hemophilia A with inhibitors. N Engl J Med. 2017; 377:809-818 https://doi.org/10.1056/NEJMoa1703068
Muto A, Yoshihashi K, Takeda M Anti-factor IXa/X bispecific antibody ACE910 prevents joint bleeds in a long-term primate model of acquired hemophilia A. Blood. 2014; 124:3165-3171 https://doi.org/10.1182/blood-2014-07-585737
Kruse-Jarres R, Callaghan MU, Croteau SE Surgical experience in two multicenter, open-label phase 3 studies of emicizumab in persons with hemophilia A with inhibitors (HAVEN 1 and HAVEN 2). Blood. 2017; 130 https://doi.org/10.1182/blood.V130.Suppl_1.89.89
An update for general dental practitioners on a new medication for the management of patients with haemophilia A Stephanie Fenesan Bella Madan Najla Nizarali Dental Update 2024 49:6, 707-709.
Authors
StephanieFenesan
BDS, BSc(Hons), AKC, MSc, MSCD RCS Ed
Specialty Trainee in Special Care Dentistry, Department of Sedation and Special Care Dentistry, Guy's Dental Institute, Guys and St Thomas' NHS Foundation Trust
Specialist in Sedation and Special Care Dentistry, Department of Sedation and Special Care Dentistry, Floor 26 Tower Wing, Guy's Hospital, London Bridge, London SE1 9RT, UK
Emicizumab is a new medication used in the treatment of people with haemophilia A and there is little in the current literature providing guidance for dental treatment. It is important to risk assess dental procedures appropriately according to their bleeding risk and to liaise closely with the patient's haematology team. This article provides an overview of emicizumab, its mechanism of action and implications for dental treatment, as well as examples of surgical management plans provided by the haemophilia team.
CPD/Clinical Relevance: It is important to liaise closely with the patient's haemophilia team to ensure provision of safe dental treatment.
Article
Emicizumab (Hemlibra) is a relatively new prescription medication administered to people with haemophilia A and used for routine prophylaxis to prevent or reduce the frequency of bleeding episodes. Haemophilia is a congenital bleeding disorder in which there is a deficiency of clotting factors. Haemophilia A is a sex-linked recessive condition that results in a deficiency of clotting factor VIII and accounts for approximately 85% of haemophilia cases, affecting approximately 1:10,000, with over 8400 people registered with haemophilia A in the UK.1 People with haemophilia A can present on a spectrum of severity as mild, moderate or severe, depending on the level of clotting factor VIII present (Table 1).
Degree of haemophilia
Factor VIII present (%)
Clinical features
Severe
<1
Frequent spontaneous bleeds, severe bleeding problems, bleeds into muscles or joints
Moderate
2–5
May have spontaneous bleeds, will produce symptoms of abnormal bleeding
Mild
6–40
Bleed after trauma or surgery
Carrier
Factor level can vary
Can show mild symptoms
Conventional treatment for haemophilia A depends on the severity of haemophilia and the factor VIII percentage present, and aims to increase the levels of factor VIII. This can be carried out prophylactically if known surgical intervention is planned, and adjusted according to the procedure required, or in response to bleeding caused by trauma. This could include the use of desmopressin (desamino-8-D-arginine vasopressin or DDVAP), which acts to release bound factor VIII and increase plasma levels. However, this is only suitable for patients with mild or moderate haemophilia A and not suitable for patients with severe haemophilia A because they will not have bound factor VIII available to be released.
An additional option is replacement of factor VIII by using factor VIII concentrate from either recombinant factor VIII or from fresh frozen plasma. However, approximately one-third of patients with severe haemophilia A may develop antibodies to factor therapy, also known as inhibitors, which renders the replacement factor VIII useless. If this occurs, then by-passing agents, such as recombinant activated factor VIIa (rFVIIa), such as NovoSeven, or activated prothrombin complex concentrate (aPCC), such as factor VIII inhibitor bypassing agent (FEIBA), are indicated.
Anti-fibrinolytic agents may also be used singularly in patients with mild haemophilia or in combination with other options in patients with moderate or severe haemophilia. This includes the use of tranexamic acid, which competitively inhibits the activation of plasminogen to plasmin and inhibits fibrin clot lysis.
Additionally, adjustments to treatment or additional precautions may need to be implemented to prevent or minimize bleeding risk, such as avoiding the use of inferior alveolar blocks or avoiding dental extractions if possible. Local haemostatic measures should be undertaken if extractions are unavoidable, and these include placing topical haemostatic agents and suturing post-operatively as well as planning the timing for appointments to allow for the management of any prolonged post-operative bleeding.
Most patients with haemophilia can be seen in general practice for check-ups and for non-invasive procedures; however, liaison with the patient's haemophilia team is crucial.3,4 Patients who require more invasive treatment, such as extractions, may be referred to a specialist centre. A more comprehensive guide to the management of patients with haemophilia and congenital bleeding disorders is described by Anderson et al.2 This article discusses the more recent introduction of emicizumab and its implications for dental management.
Emicizumab
Emicizumab (Hemlibra) is a relatively new medication that can be prescribed for routine prophylaxis to prevent or reduce the frequency of bleeding episodes for patients with haemophilia A.5 It was approved for use in patients with haemophilia A with an inhibitor in July 2018, and for those without an inhibitor, in September 2019.1 Emicizumab is a monoclonal antibody that is capable of recognizing and simultaneously binding to two distinct antigenic targets simultaneously, thus making it a bispecific antibody. It is able to bind to factors IXa and X to activate factor X in the absence of factor VIII and is, therefore, not affected by inhibitors.6
In the UK, emicizumab can only be prescribed by comprehensive care haemophilia centres and requires special approval from the NHS for each patient for whom it is prescribed. Patients are initially given a subcutaneous loading dose of 3.0 mg/kg weekly, for 4 weeks. This is followed by a maintenance dose dependent on the patient's total body weight, either once a week or once every 2 weeks due to its long half-life of approximately 28 days.1
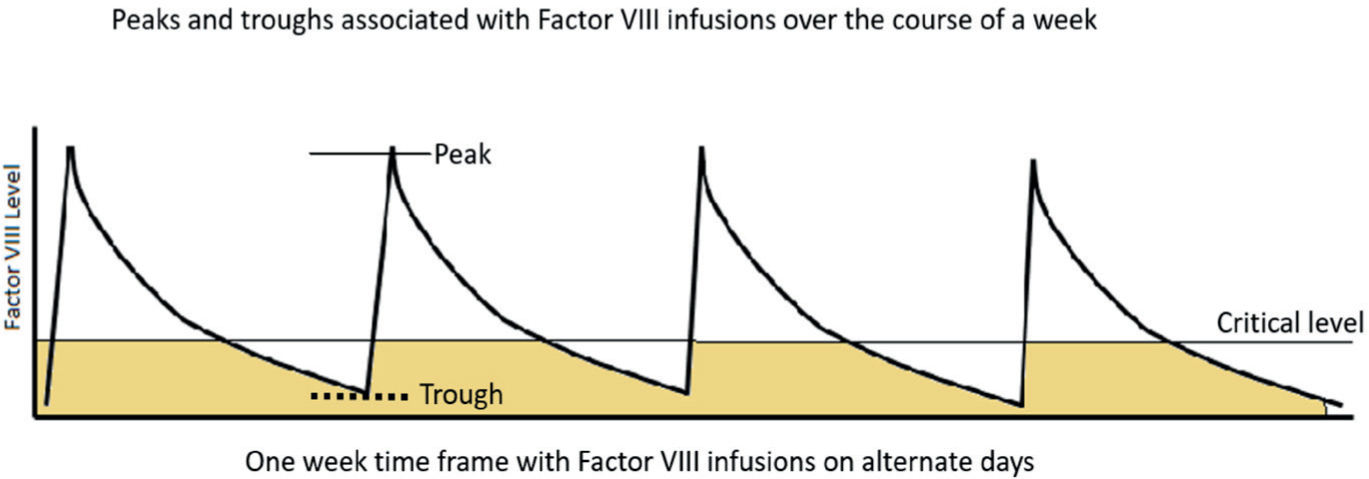
Owing to the longer half-life of emicizumab, more stable concentration levels are maintained, therefore avoiding the peaks and troughs associated with factor VIII replacement therapy (Figure 1).
Figure 1. Displaying the peaks and troughs when factor VIII is administered on alternate days. When the level of factor VIII falls below the critical level, there is an increased risk of spontaneous bleeding for the patient.7
In clinical trials it has been shown that emicizumab can be used for people with factor VIII antibodies alongside rFVIIa (NovoSeven). However, the trials have shown that use of emicizumab alongside aPCC has been associated with thrombotic microangiopathy, venous thrombosis and skin necrosis.8,9 Therefore, it is not advisable to use aPCC, such as FEIBA, while a patient is on emicizumab and first-line treatment, if there is a bleed, should be recombinant factor VIIa.5 For less severe mucosal bleeds, tranexamic acid alone may be sufficient. However, if a patient taking emicizumab requires major surgery there are few data available in the literature regarding this at the time of writing, and the UK Haemophilia Centre Doctors Organisation (UKHCDO) suggests the use of by-passing agent recombinant factor VIIa (NovoSeven).5
Dental management
Risk assessment is crucial when planning the dental management of patients with haemophilia A, as well as close liaison with the patient's specialist haemophilia team. The severity of their haemophilia A and the risk of bleeding and must be taken into account, as well as the risk of bleeding from the dental procedure required. A dental examination without basic periodontal examination (BPE) or periodontal pocket charting should be undertaken, as well as relevant radiographs, and an appropriate treatment plan then discussed and agreed with the patient. Dental treatment should be undertaken after the patient has finished the loading dose for emicizumab, and once the patient is on the maintenance dose.10Table 2 gives a summary of dental procedures that pose an uncommon (low), and common (higher) risk of bleeding. In cases where there is a perceived risk of prolonged bleeding, the patient's haemophilia team should be contacted with details of the proposed dental treatment and an individualized haemophilia surgical management plan for the patient can then be devised. Oral tranexamic acid tablets administered 1 gram every 6–8 hours, as well as tranexamic acid mouthwash (10 ml of 5% solution) may be recommended for dental treatment (Table 3).
Uncommon (low) risk of bleeding
Common (higher) risk of bleeding
Examination (without basic periodontal examination (BPE) or periodontal pocket charting)
RCT first stage with open apex (paediatric or trauma cases)
Radiographs
Subgingival restorations in a patient with unhealthy gingivae
Prosthetics
Subgingival crown and bridge work with or without the use of retraction cord
Prophylaxis (polishing of teeth)
Supragingival scaling in a patient with unhealthy gingivae
Supragingival and subgingival restorations without LA
Subgingival scaling and root surface debridement
Restorations with buccal infiltration LA
Any procedure requiring inferior dental block LA or lingual infiltration LA
Supra-gingival crown and bridge work with buccal infiltration LA
Single tooth extraction
Supragingival scaling
Multiple teeth extractions
RCT with use of rubber dam clamp and buccal infiltration LA
Minor oral surgery such as surgical extractions, periodontal surgery, implant surgery, biopsies.
Use of matrix band
Patient
Patient A
Patient B
Patient C
Medical history
Severe haemophilia A with inhibitors
Severe haemophilia A with inhibitors
Severe haemophilia A with inhibitors
Dental treatment required
Dental restorations with local anaesthetic
Periodontal treatment and maintenance: dental scaling with local anaesthetic (infiltrations)
Deep scaling with local anaesthetic and replacement of a restoration
Example of surgical management plan
Evening before procedure: start oral tranexamic acid 1 g tablets 6 hourly for 5 days
Evening before procedure: start oral tranexamic acid 1 g 6 hourly and continue for 3–5 days post procedure
Oral tranexamic acid tablets 1 g 6 hourly for 3–5 days following the procedure
Day of procedure: no extra cover required as on emicizumab weekly prophylaxis
1 hour prior to procedure: No extra cover required as patient on emicizumab weekly prophylaxis
Continue with their usual dose of emicizumab
Post-procedure: to be reviewed at the Haemophilia centre if any bleeding problems
Tranexamic acid prescription: Tablets orally and mouthwash
No extra cover required
Additional precautions or adjustments should be undertaken by the dental team where appropriate. This includes avoiding the use of inferior alveolar blocks, and where possible, using buccal infiltrations, avoiding dental extractions and instead completing endodontic treatment where appropriate. If a dental extraction is required, then local haemostatic measures are recommended, such as the use of topical haemostatic agents and suturing sockets post-operatively. Additionally, the timing of appointments should to be taken into consideration, having them earlier in the week and at the beginning of the day to allow for management of post-operative bleeding if required.
Preventive advice should be emphasized to the patient to address any dental risk factors and reduce the need for future interventive dental treatment as advised by the Department of Health Delivering Better Oral Health toolkit.11
If a patient requires emergency dental treatment, then analgesia or antibiotics, if appropriate, may be advised. However, if invasive dental treatment with a risk of prolonged bleeding is required, then the management plan must first be discussed with the patient's haemophilia team.
In the event of post-operative bleeding, the patient should contact their specialist haematology team for management. The UKHCDO has provided some guidelines on the management of patients taking emicizumab in the event of a bleeding episode.5 These guidelines advise considering the use of tranexamic acid without the need for additional haemostatic cover for dental extractions. Literature surrounding surgery for patients on emicizumab is limited; however, one trial looked at surgical procedures in patients receiving emicizumab.12 Out of 29 surgeries, six were dental extractions, four of which resulted in prolonged post-operative bleeding. Of the four extractions resulting in post-operative bleeding events, one patient had received prophylactic peri-operative bypassing agent (rFVIIa) while three had not receive a prophylactic peri-operative bypassing agent.12 Of the four patients who had post-operative bleeding following extractions, two were treated further and were managed with recombinant factor VIIa.12 As previously mentioned, the use of aPCC is inadvisable, and the use of rFVIIa is preferred as first-line treatment for bleeds.
Conclusion
It can be appropriate for patients with haemophilia A to be examined and treated for non-invasive procedures within general practice. It is important to undertake a full risk assessment for patients with haemophilia A as well as maintain close communication with the patient's haemophilia team to ensure appropriate plans are in place to reduce and mitigate bleeding risks associated with dental treatment. The patient should have an individualized dental and haemophilia management plan devised and there should be an emphasis on shared care between the different specialities. Emicizumab is a fairly recent development in the management of severe haemophilia A and it is imperative that medical details are updated at each dental appointment to ensure any changes to medical conditions or their management are fully up to date.