National Institute for Clinical Excellence. Improving outcomes in head and neck cancers. 2004. http://www.nice.org.uk/guidance/csg6 (accessed April 2022)
Nutting C. Radiotherapy in head and neck cancer management: United Kingdom National Multidisciplinary Guidelines. J Laryngol Otol. 2016; 130:(S2)S66-S67 https://doi.org/10.1017/S0022215116000463
Rogers SN, Semple C, Babb M, Humphris G. Quality of life considerations in head and neck cancer: United Kingdom National Multidisciplinary Guidelines. J Laryngol Otol. 2016; 130:(S2)S49-S52 https://doi.org/10.1017/S0022215116000438
Tolentino Ede S, Centurion BS, Ferreira LH Oral adverse effects of head and neck radiotherapy: literature review and suggestion of a clinical oral care guideline for irradiated patients. J Appl Oral Sci. 2011; 19:448-454 https://doi.org/10.1590/s1678-77572011000500003
Kumar N, Brooke A, Burke M The oral management of on-cology patients requiring radiotherapy, chemotherapy and/or bone marrow transplantation. Fac Dent J. 2013; 4:200-203
Butterworth C, McCaul L, Barclay C. Restorative dentistry and oral rehabilitation: United Kingdom National Multidisciplinary Guidelines. J Laryngol Otol. 2016; 130:(S2)S41-S44 https://doi.org/10.1017/S0022215116000414
Critchlow SB, Morgan C, Leung T. The oral health status of pre-treatment head and neck cancer patients. Br Dent J. 2014; 216 https://doi.org/10.1038/sj.bdj.2013.1246
Breslin M, Taylor C. Incidence of new carious lesions and tooth loss in head and neck cancer patients: a retrospective case series from a single unit. Br Dent J. 2020; 229:539-543 https://doi.org/10.1038/s41415-020-2222-2
Lieshout HF, Bots CP. The effect of radiotherapy on dental hard tissue – a systematic review. Clin Oral Investig. 2014; 18:17-24 https://doi.org/10.1007/s00784-013-1034-z
Dobroś K, Hajto-Bryk J, Wróblewska M, Zarzecka J. Radiation-induced caries as the late effect of radiation therapy in the head and neck region. Contemp Oncol (Pozn). 2016; 20:287-290 https://doi.org/10.5114/wo.2015.54081
Nutting CM, Morden JP, Harrington KJ PARSPORT trial management group. Parotid-sparing intensity modulated versus conventional radiotherapy in head and neck cancer (PARSPORT): a phase 3 multicentre randomised controlled trial. Lancet Oncol. 2011; 12:127-136 https://doi.org/10.1016/S1470-2045(10)70290-4
Kasibhatla M, Kirkpatrick JP, Brizel DM. How much radiation is the chemotherapy worth in advanced head and neck cancer?. Int J Radiat Oncol Biol Phys. 2007; 68:1491-1495 https://doi.org/10.1016/j.ijrobp.2007.03.025
Epstein JB, Güneri P, Barasch A. Appropriate and necessary oral care for people with cancer: guidance to obtain the right oral and dental care at the right time. Support Care Cancer. 2014; 22:1981-1988 https://doi.org/10.1007/s00520-014-2228-x
Thariat J, Ramus L, Darcourt V Compliance with fluoride custom trays in irradiated head and neck cancer patients. Support Care Cancer. 2012; 20:1811-1814 https://doi.org/10.1007/s00520-011-1279-5
Marinho VC, Chong LY, Worthington HV, Walsh T. Fluoride mouthrinses for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2016; 7 https://doi.org/10.1002/14651858.CD002284.pub2
Raphael S, Blinkhorn A. Is there a place for Tooth Mousse in the prevention and treatment of early dental caries? A systematic review. BMC Oral Health. 2015; 15 https://doi.org/10.1186/s12903-015-0095-6
Marinho VC, Worthington HV, Walsh T, Clarkson JE. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2013; (7) https://doi.org/10.1002/14651858.CD002279.pub2
Talwar B, Donnelly R, Skelly R, Donaldson M. Nutritional management in head and neck cancer: United Kingdom National Multidisciplinary Guidelines. J Laryngol Otol. 2016; 130:(S2)S32-S40 https://doi.org/10.1017/S0022215116000402
Jawad H, Hodson NA, Nixon PJ. A review of dental treatment of head and neck cancer patients, before, during and after radiotherapy: part 2. Br Dent J. 2015; 218:69-74 https://doi.org/10.1038/sj.bdj.2015.29
National Institute for Clinical Excellence. Dental checks: intervals between oral health reviews. 2004. https://www.nice.org.uk/guidance/cg19 (accessed April 2022)
Aguiar GP, Jham BC, Magalhães CS, Sensi LG, Freire AR A review of the biological and clinical aspects of radiation caries. J Contemp Dent Pract. 2009; 10:83-89
Dhanda J, Pasquier D, Newman L, Shaw R. Current concepts in osteoradionecrosis after head and neck radiotherapy. Clin Oncol (R Coll Radiol). 2016; 28:459-466 https://doi.org/10.1016/j.clon.2016.03.002
McCaul LK. Oral and dental management for head and neck cancer patients treated by chemotherapy and radiotherapy. Dent Update. 2012; 39:135-140 https://doi.org/10.12968/denu.2012.39.2.135
Hong CHL, Hu S, Haverman T A systematic review of dental disease management in cancer patients. Support Care Cancer. 2018; 26:155-174 https://doi.org/10.1007/s00520-017-3829-y
Radiation caries describes the rapid onset and progression of dental caries in patients who have received radiotherapy to the head and neck. The combination of salivary gland damage resulting in hyposalivation and a cariogenic diet can have catastrophic consequences with a considerable impact on the quality of life of individuals. Caries risk must be managed at all stages of the patient's head and neck cancer journey from the pre-assessment to their lifelong maintenance. This paper provides an overview of the aetiology, presentation and management of radiation caries demonstrated with clinical cases.
CPD/Clinical Relevance: With the increasing incidence of head and neck cancer, clinicians should be aware of the significance of radiation caries, understand its specialist management and be able to contribute to the patient's long-term management.
Article
Around 12,400 new head and neck cancer (HANC) cases are diagnosed annually in the UK, and the incidence is on the rise.1 HANC patients are managed in secondary care by a multidisciplinary team of specialists.2 The three main management strategies are surgery, radiotherapy and chemotherapy, which may be used as a single modality or in combination.3 It is reported that 43–85% of HANC cases receive radiotherapy.1 Radiotherapy to the head and neck region can have a number of adverse short- and long-term complications on the oral cavity, with a significant impact upon the quality of life of patients during and post cancer therapy.4 Complications include mucositis, candidiasis, altered taste, osteoradionecrosis, trismus, xerostomia and radiation caries.5
The designated oral healthcare team, led by a restorative consultant, plays a role throughout the journey including the patients pre-assessment, oral care during treatment, rehabilitation and maintenance post treatment.6 With patients retaining their teeth for longer, the role of the team is becoming increasingly complex and, considering HANC patients often present with poor oral health, the subsequent undesirable effects of radiotherapy on the oral cavity result in a high risk of dental caries.7,8 Primary care dentists are increasingly likely to encounter patients following cancer therapy presenting with radiation caries and will play a key role in long-term monitoring and maintenance.
What is radiation caries?
Radiation caries describes the rapid onset and progression of dental caries in individuals who have been exposed to head and neck ionizing radiation. Overt caries may be seen within 3 months of completing treatment.9 Radiation caries is very common with a recent retrospective analysis of 95 patients who had received radiotherapy for HANC demonstrating an average of 6.63 carious teeth over a mean follow-up of 3.75 years.10
Radiation-induced damage to the enamel, dentine and the amelo-dentinal junction may predispose individuals to caries.11 However, radiation caries is thought to develop primarily as an indirect effect of radiotherapy on the salivary glands resulting in reduced quantity and quality of saliva in combination with a cariogenic diet.12,13 A reduced flow of viscous saliva with reduced buffering capacity, reduced clearance and a reduced pH creates a shift in the oral microflora, favouring cariogenic bacteria, such as Streptococcus mutans and Lactobacillus and the development of dental caries.12,13,14Table 1 summarizes the factors that may contribute to radiation caries.
Reduction in quantity and quality of saliva
Increased nutritional requirements resulting in frequent consumption of refined carbohydrates
Poor oral hygiene due to mucositis, trismus and lower prioritization of dental health
Altered taste resulting in a preference for cariogenic foods
Direct effects of radiation on the dental hard tissues
An individual's risk of salivary dysfunction depends on their initial salivary function, radiation dose and radiation field with particular emphasis on volume of salivary gland irradiation.15 Consequently, when compared to conventional radiotherapy, sparing of the parotid glands with use of intensity-modulated radiation therapy (IMRT) has been associated with a reduced incidence of xerostomia, better recovery of saliva production and improved quality of life.16 Adjuvant chemotherapy increases the biological equivalent dose of radiotherapy and so these patients may be at greater risk of radiation caries.17
Pre-treatment dental assessment
Patients whose treatment will affect the mouth or jaw should have a dental assessment prior to their cancer therapy.2 Restorative consultants working within a multidisciplinary team are in the best position to conduct these assessments owing to their expertise in prevention and management of complications, and the need for complex oral rehabilitation.2,7,18 Patients requiring a dental assessment are identified at the multidisciplinary team meeting, and assessed as soon as possible to allow sufficient time for the required dental treatment to be completed.6,7,13 The aims of the dental assessment are as follows:6,7,13
Planning for the extraction of teeth that are unrestorable, have a doubtful prognosis or are at risk of future dental disease in an area that would be at risk of osteoradionecrosis. Extractions should be completed at least 10 days prior to commencing cancer therapy.
Planning for the restoration of the remaining teeth that may be carious or have the potential to traumatize the soft tissues.
Avoid unscheduled interruptions to cancer therapy attributable to dental problems.
Prepare the patient for the anticipated short- and long-term oral complications of cancer therapy.
Develop a plan for prevention, oral rehabilitation and follow-up.
Once dental treatment is complete, the patient should be dentally fit and have a dentition that can be maintained and rehabilitated post therapy.7 The key to maintaining oral health and reducing the risk of radiation caries is daily self-care with an individualized preventive regimen. There is limited evidence regarding effectiveness of caries prevention strategies in HANC patients. Therefore, a range of prevention methods are recommended based on the wider evidence-base for caries prevention. Fluoride remains the cornerstone of prevention, and routine caries prevention advice is detailed in Table 2.
Caries prevention advice
Comments
Maintain good oral hygiene through effective tooth brushing and interdental cleaning
Tooth brushing should be undertaken at least twice daily, last thing at night and on one other occasion19
Daily use of 5000ppm fluoride toothpaste
Toothpastes containing higher fluoride concentrations are more effective at caries prevention19
In addition, application of fluoride in custom trays worn for 5–10 minutes daily has been recommended, although the evidence shows compliance is low in HANC patients20
Daily 0.05% sodium fluoride mouth rinse
A daily fluoride rinse used at a different time to brushing may significantly reduce the risk of caries19,21
Daily use of remineralizing toothpaste (eg Tooth Mousse, GC, Japan)
Although the evidence suggests no significant benefit from using remineralizing toothpastes containing casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) (eg Tooth Mousse) over the use of fluoride, the free calcium and phosphate, often lacking in patients with hyposalivation, has been shown to be beneficial for the prevention and remineralization of root caries in HANC patients who have undergone radiotherapy22,23
Twice yearly application of fluoride varnish (2.2% NaF)
The topical application of fluoride varnish has a caries-inhibiting effect and is recommended in patients with high risk of caries19,24
Provide dietary advice under close liaison with the dietitian
An energy-dense diet may be recommended by the dietitian and should be balanced against the patient's risk of caries. Close liaison with the dietitian with the aim of reducing the frequency of sugars between meals may be beneficial
A healthy balanced diet should be encouraged during the post therapy period and the frequency and amount of sugary food and drink reduced19,25
Sugar-free medicines should be used where possible
The use of sugar free medicines should be coordinated with the oncologist.6 Where there are no suitable alternatives, the patient should be advised to rinse their mouth following consumption
Dental care during cancer therapy
Involving the restorative consultant during cancer therapy may help to improve the patient's oral comfort and reduce the risk of complications.18 The importance of prevention cannot be underestimated and the patient's pre-planned preventive regimen should be reinforced (Table 2). It is recognized that the short-term side effects of radiotherapy or chemotherapy, such as mucositis, may indirectly increase caries risk by reducing tolerance to oral hygiene measures.13 Consequently, management of these effects may indirectly contribute to caries prevention. Where effective tooth brushing is hindered due to mucositis, a soft toothbrush may be used in the short term. Some patients find mint-flavoured high-fluoride toothpaste too strong to tolerate, and alternative products should be recommended.26 Sodium lauryl sulphate-(SLS) free and unflavoured toothpastes (eg OraNurse, UK) are preferred by some patients. Taste changes during radiotherapy often result in patients choosing cariogenic foods.6 This is compounded by the need for an energy-dense diet, including nutritional supplements (eg Ensure, Abbott Laboratories, UK), resulting in a frequent intake of refined carbohydrates.13,25 While it is recognized that this significantly increases the risk of dental caries, this should be balanced against the patient's weight and nutritional status. Close liaison with the dietitian is recommended to reduce the frequency of sugars between meals, in addition to sticky foodstuffs with a low oral clearance.27 Modifications, such as consuming sugar-containing drinks through straws, may also be beneficial.6
Dental care post cancer therapy
Maintenance care
All HANC patients require close follow-up with a focus on prevention owing to the life-long increased risk of dental disease.6,18 The initial recall interval based on NICE guidance is 3 months, although this may later be altered based on the patient's risk assessment.28 Patients experiencing late complications may require longer-term follow-up within a specialist environment. However, where the patient has been rehabilitated and demonstrates stable oral health, they may be discharged to primary care for maintenance.6,7 The initial interval for radiographic monitoring for the purpose of caries detection is 6 months, which may be increased to 12 months if long-term stability is evident.29
Presentation of radiation caries
The presentation of caries tends to differ in those who have received radiotherapy. It presents as atypical lesions affecting surfaces normally resistant to caries including incisal edges, cusp tips, lingual and smooth surfaces, likely due to the lack of mechanical cleansing from salivary flow as a result of hyposalivation. The most common type of radiation caries affects the cervical surface and progresses circumferentially at the cementoenamel junction (CEJ) eventually resulting in decoronation.30 Breslin and Taylor10 identified that mandibular incisors and canines were most commonly affected by radiation caries, followed by the maxillary incisors and canines. However, this was likely to be a result of fewer posterior teeth as these are more commonly extracted pre-radiotherapy.
Management of radiation caries
Management of radiation caries should aim to reduce the risk of osteoradionecrosis (ORN) by avoiding extractions in irradiated sites. ORN is commonly defined as an area of exposed devitalized bone, in a previously irradiated field, in the absence of neoplastic disease (Figure 1).31 Teeth should be retained wherever possible, which may include the need for root canal treatment, retention of roots or decoronation. Primary care dentists may provide routine restorative treatment, but where there is no suitable alternative, it has been recommended for extractions to be referred to secondary care.6,32
Figure 1. ORN presenting in the posterior mandible following tooth extractions in a patient previously irradiated for the management of HANC.
The restoration of teeth in those with radiation caries is not without its challenges, particularly as patients may present with extensive atypical lesions and trismus. Composite resin, resin-modified glass ionomer and amalgam restorations perform more favourably than glass ionomer cements. However, in those with poor adherence to fluoride regimens, glass ionomer cements may be preferred owing to a reduced rate of recurrent caries at the expense of regular maintenance and replacement.33 Caries should be managed conservatively initially with direct restorations. Indirect restorations may be considered in patients who are stable with a good level of oral hygiene.6
Case reports
Case 1
A 67-year-old male diagnosed with a T4N3M0 basaloid squamous cell carcinoma (BSCC) that affected the skin posterior to the right ear was referred, following surgery, to the restorative team for a dental assessment prior to chemoradiotherapy.
The patient presented with a minimally restored, periodontally stable lower arch and an upper complete denture. A pre-operative orthopantomogram (OPG) was taken (Figure 2a). Extraction of the heavily restored LL7 was promptly arranged. Oral hygiene advice was given and 5000ppm fluoride toothpaste prescribed.
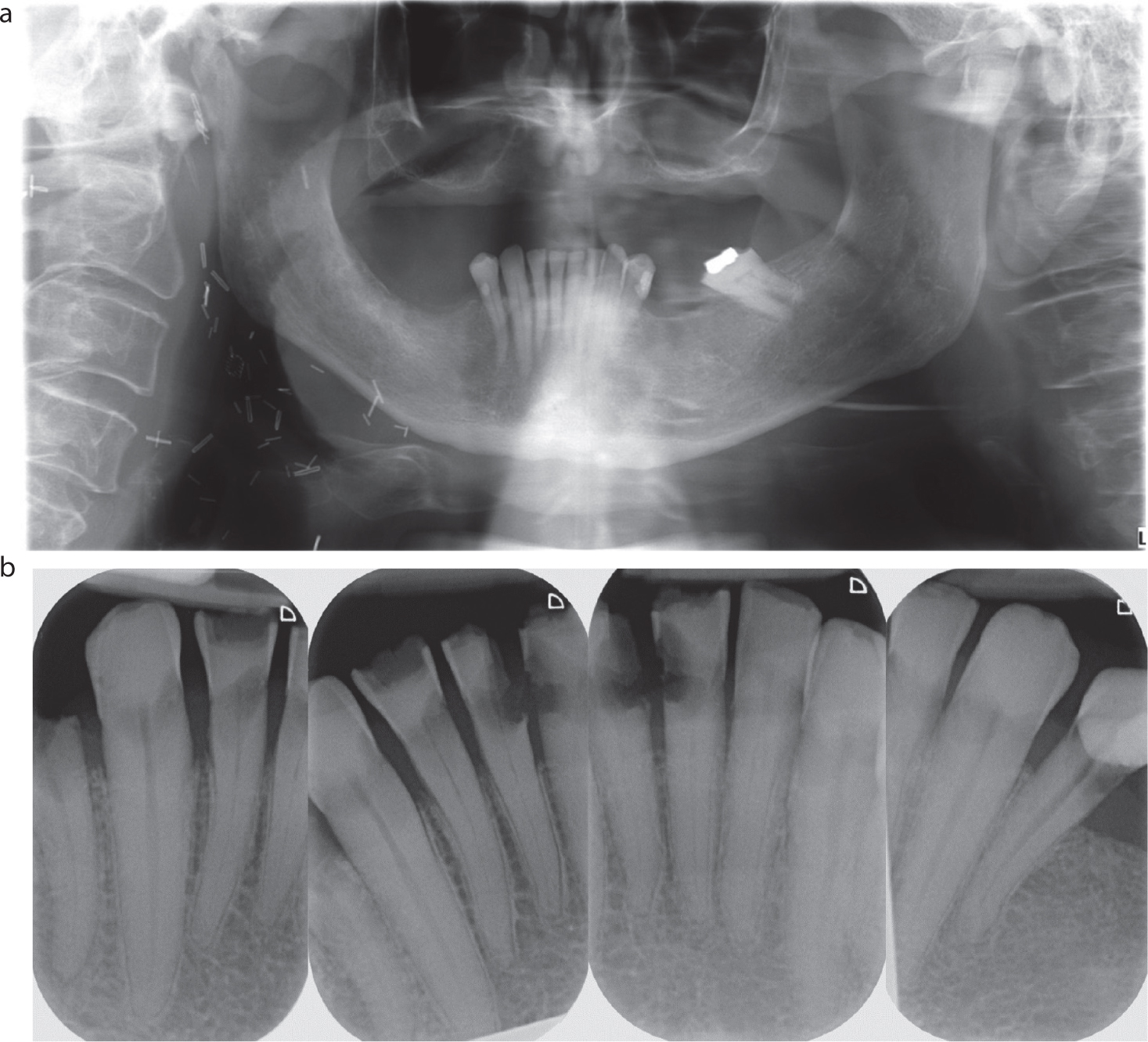
Figure 2. Radiographic progression of radiation caries in Case 1. (a) OPG pre-radiotherapy. (b) Periapical images taken 18 months after the initial OPG demonstrating the classical presentation of radiation caries at the CEJ.
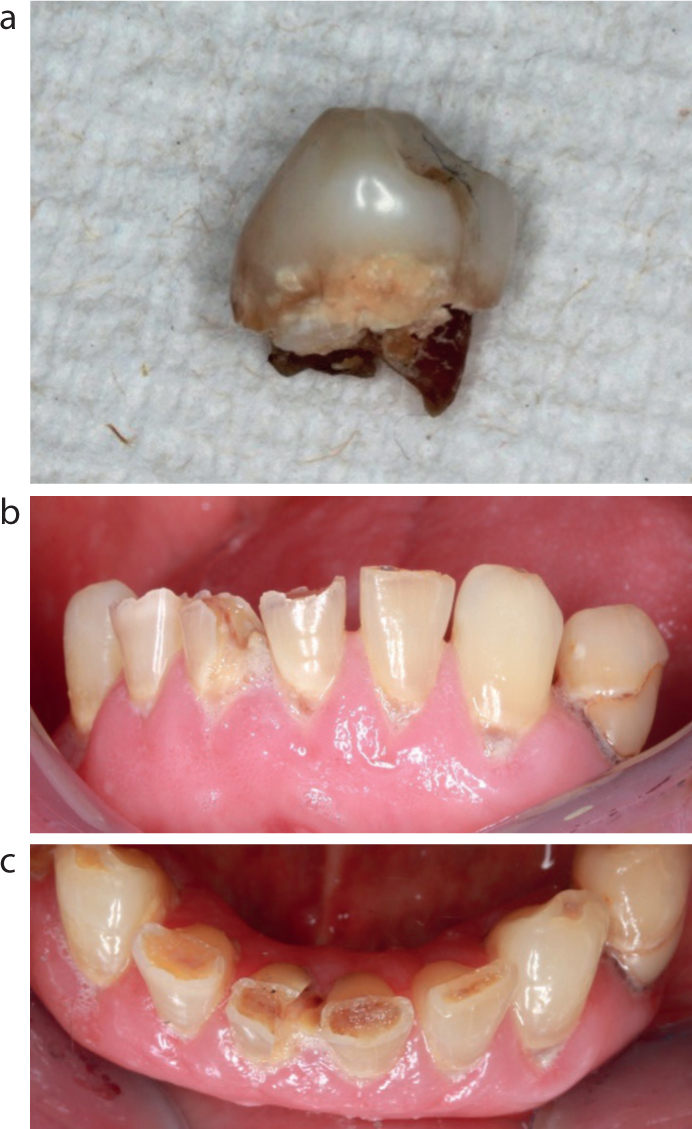
The patient was reviewed 2 months post-radiotherapy, presenting with a dry mouth, and a salivary replacement spray was prescribed. Despite regular reviews, reinforcement of oral hygiene advice and high-fluoride toothpaste, the patient attended with a decoronated LR4 14 months later (Figure 3a). Clinical examination revealed poor oral hygiene, viscous frothy saliva and caries affecting the remaining dentition (Figure 3b, c). Peri-apical radiographs confirmed extensive caries (Figure 2b). A dental clearance was performed, followed by provision of a new complete upper denture and immediate lower denture.
Figure 3. Clinical presentation of radiation caries in Case 1. (a) Decoronated LR4 demonstrating circumferential caries at the CEJ. (b) Anterior view demonstrating radiation caries affecting cervical and incisal aspect of the mandibular teeth. (c) Occlusal view demonstrating radiation caries affecting incisal surfaces of the mandibular teeth.
Case 2
A 63-year-old male patient diagnosed with a right tongue base T4N2M0 squamous cell carcinoma (SCC) was seen for a dental assessment prior to chemoradiotherapy.
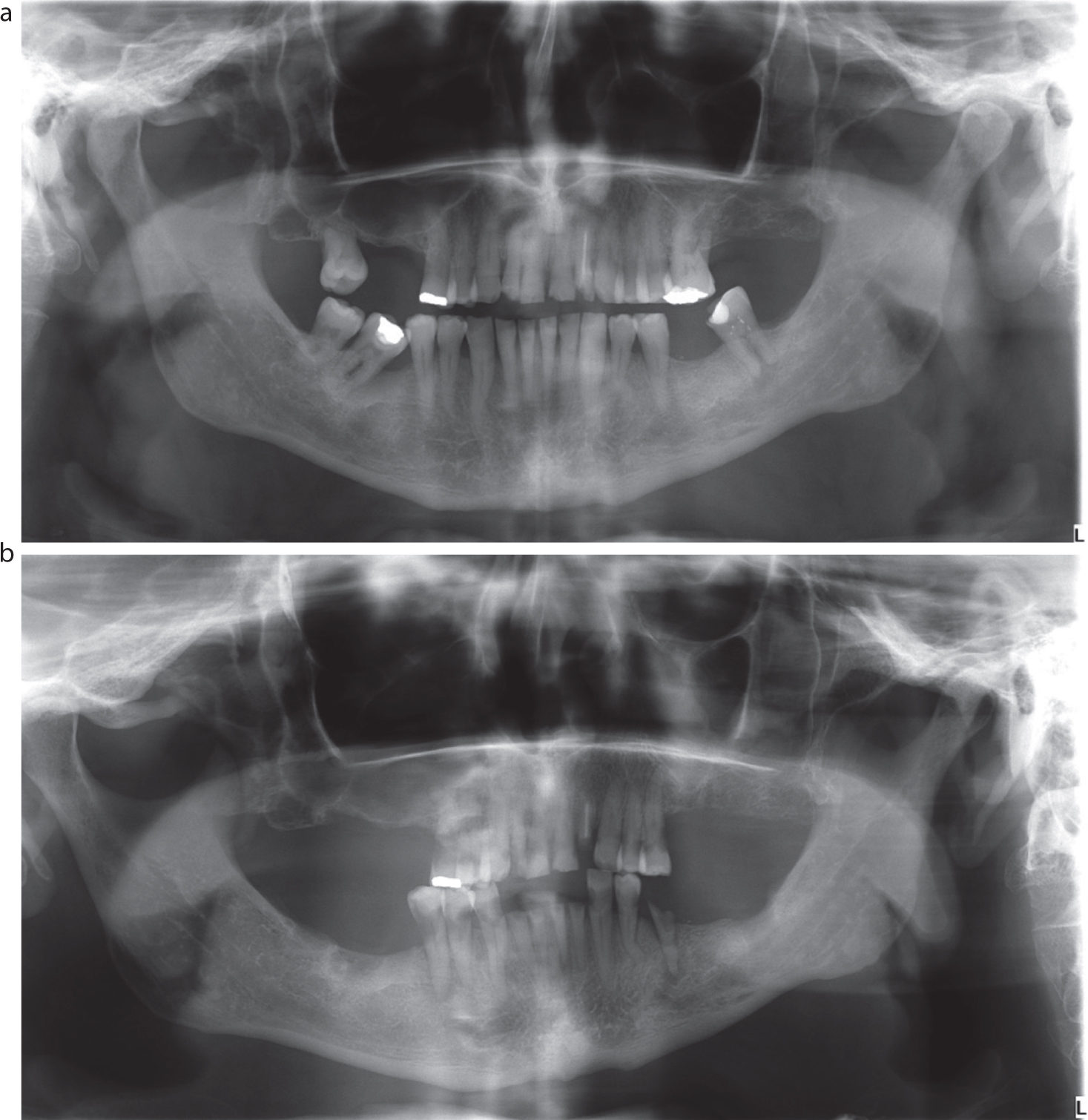
The patient was an infrequent dental attender. An OPG was taken to assess the dentition (Figure 4a). The UR8, UL6, LL8, LR7 and LR8 were extracted. High-fluoride toothpaste and 0.05% fluoride mouthwash were prescribed.
Figure 4. Radiographic progression of radiation caries in Case 2. (a) OPG pre-radiotherapy. (b) OPG following delayed presentation post-therapy demonstrating retained roots and widespread radiation caries.
The patient failed to attend his scheduled review. He attended 12-months post radiotherapy reporting multiple broken teeth. Clinical and radiographic evaluation revealed grossly carious teeth (Figure 4b). A full clearance was arranged and complete dentures constructed.
Case 3
A 66-year-old male diagnosed with a T1N1M0 BSCC of the left tonsil was seen for a dental assessment prior to chemoradiotherapy.
The patient had fair oral hygiene and a heavily restored dentition. Multiple extractions, including the LR7, were performed. The patient lived a considerable distance from the secondary care service and the general dental practitioner (GDP) was asked to complete full-mouth ultrasonic debridement, prescribe high-fluoride toothpaste and replace the LR6 crown due to marginal deficiencies (Figure 5a).
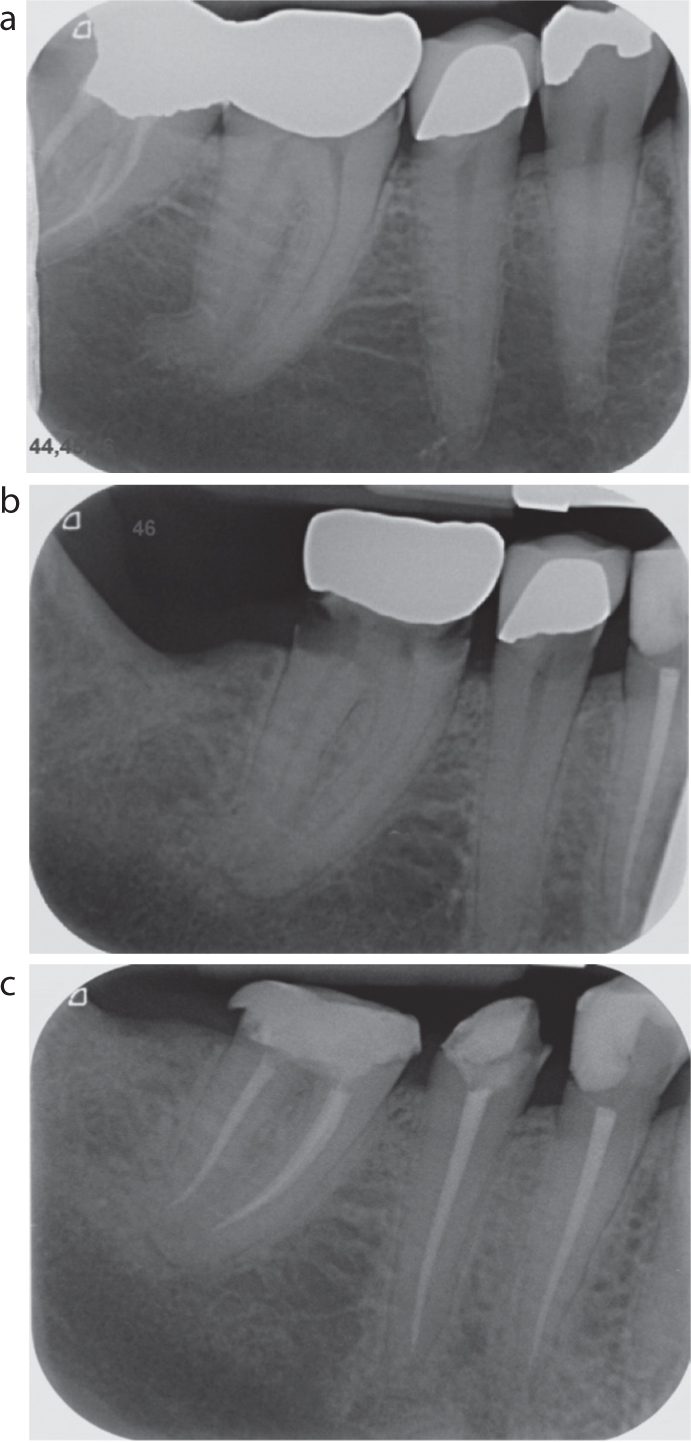
Figure 5. Periapical radiographs demonstrating the progression and management of radiation caries in the LR5 and LR6 of Case 3. (a) Pre-chemoradiotherapy; (b) 17 months following the initial image; (c) post root canal treatment and prior to final coronal restoration.
The patient failed to attend his post-therapy review and presented 17 months later with pain in lower right quadrant. Peri-apical radiographs demonstrated caries affecting multiple teeth (Figure 5b). A gingivectomy followed by root canal treatment of the LR5 and LR6 was performed to avoid extraction and the risk of osteoradionecrosis (Figure 5c).
Case 4
A 58-year-old male patient with a T3N1M0 right tongue base SCC was managed with surgery and adjuvant chemoradiotherapy. He was referred 17 months later to the restorative dentistry department by the ear, nose and throat (ENT) team due to extensive dental caries.
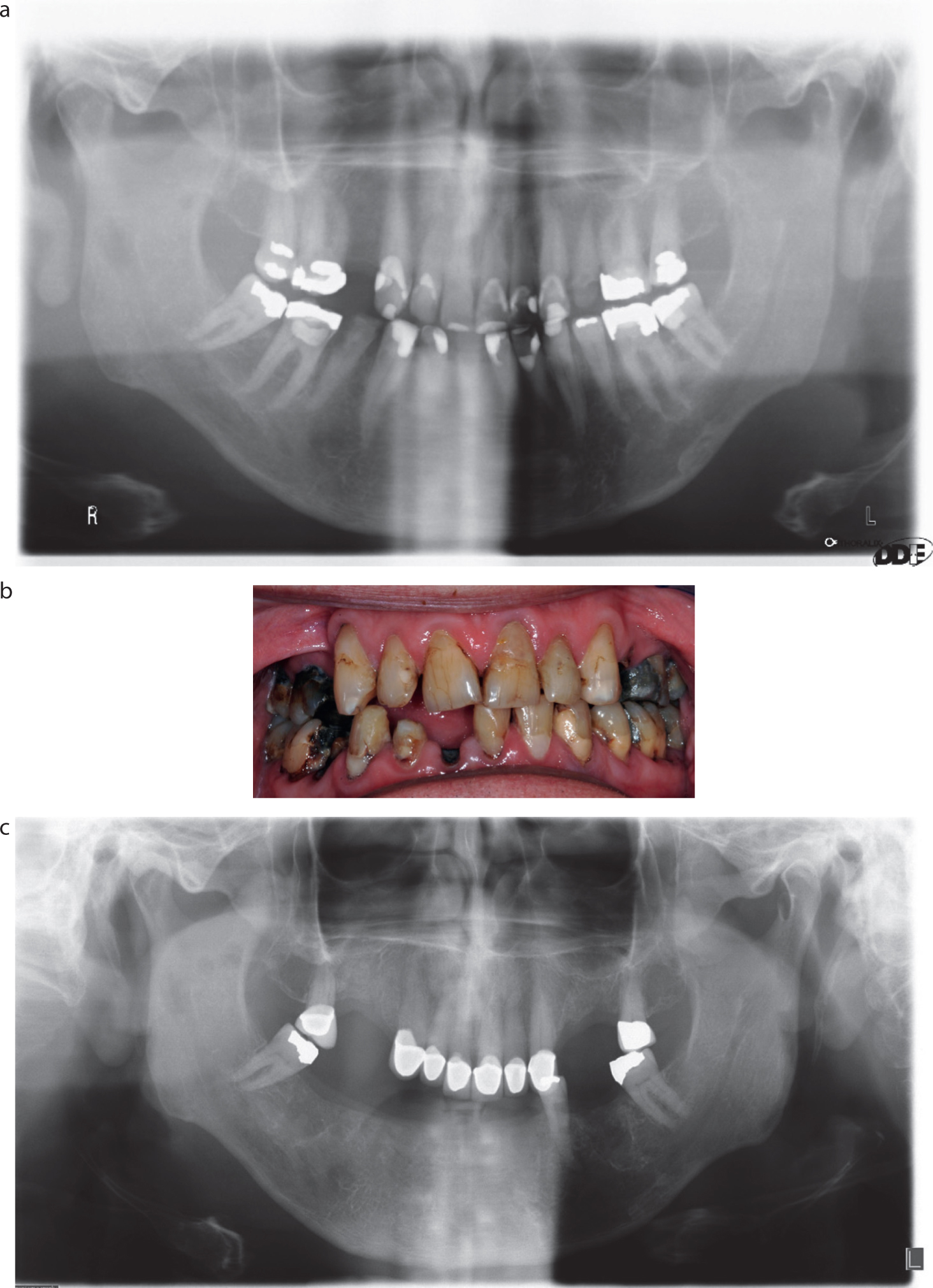
The patient had a dry mouth with poor oral hygiene and caries affecting multiple teeth. Oral hygiene advice, high-fluoride toothpaste and fluoride mouthwash were given, followed by direct restoration of carious teeth. Over the course of several years, secondary caries compromised the restorability of the teeth and those of hopeless prognosis were extracted (Figure 6a, b). A lower partial acrylic denture with stainless steel clasps was constructed. Porcelain metal crowns were provided for the UR7, UR3, UR2, UR1, UL1, UL2, UL3 and UL7 with guide planes and rest seats allowing the provision of a cobalt–chrome denture (Figure 6c). This functioned well for several years until the remaining lower teeth developed caries and required extraction. A complete denture was constructed, and the patient was functioning satisfactorily with the dentures.
Figure 6. Radiographic presentation and management of radiation caries in Case 4. (a) OPG demonstrating failing restorations. (b) Clinical photograph demonstrating failed restorations prior to further treatment. (c) OPG 17 months after image (a) showing healed extraction sockets and restoration of teeth in upper arch.
Conclusion
Head and neck radiotherapy can have adverse effects on the oral cavity that can affect an individual's quality of life. Radiation caries is a frequent complication that is due to a combination of factors, namely oral discomfort, hyposalivation and a cariogenic diet. It has a rapid onset and progression, with an atypical presentation on surfaces usually resistant to caries. An individualized preventive regimen, which is reinforced pre, during and post radiotherapy is essential in reducing the risk of caries. When radiation caries presents, the aim should be to restore and retain teeth to avoid the risk of ORN following extractions. Primary care dentists have an important role in the long-term maintenance and monitoring of the HANC population and are increasingly likely to encounter such complications in practice. Further research is required to assess the effectiveness of preventive measures in the HANC population to reduce morbidity and improve quality of life.