Posselt U. Studies in the mobility of the human mandible. Acta Odontol Scand. 1952; 10
Eriksson A, Ockert-Eriksson G, Lockowandt P, Eriksson O. Clinical factors and clinical variation influencing the reproducibility of interocclusal recording methods. Br Dent J. 2002; 192:395-400
Fenlon MR, Sherriff M, Walter JD. Association between the accuracy of intermaxillary relations and complete denture usage. J Prosthet Dent. 1999; 81:520-525
Yurkstas AA, Kapur KK. Factors influencing centric relation records in edentulous mouths. J Prosthet Dent. 2005; 93:305-310
Grasso JE, Sharry J. The duplicability of arrow-point tracings in dentulous subjects. J Prosthet Dent. 1968; 20:106-115
Shafagh I, Yoder JL, Thayer KE. Diurnal variance of centric relation position. J Prosthet Dent. 1975; 34:574-582
Murray MC, Smith PW, Watts DC, Wilson NF. Occlusal registration: science or art?. Int Dent J. 1999; 49:41-6
Wise MD. Occlusion and restorative dentistry for the general practitioner. Br Dent J. 1982; 152:407-413
McCord JF, Grant AA. A Clinical Guide to Complete Denture Prosthetics.: British Dental Association; 2000
Daher T, Lobel WA, Massad J Predictable technique to register retruded contact position (RCP) using a disposable jaw relation recording device. Compend Contin Educ Dent. 2015; 36:323-329
Valdez Fierro MT, Lombard Romero L, Gutiérrez Camacho C Comparison between two techniques for registering mandibular position in patients with hemifacial microsomia of the Federico Gomez Children's Hospital. Rev Mex Ortod. 2014; 2:e239-246
Bonsor SJ, Pearson GJ. A Clinical Guide to Applied Dental Materials.: Elsevier/Churchill Livingstone; 2013
Gysi A. Original communications. The problem of articulation. Dent Cosmos. 1910; 52:1-19
Myers M, Dziejma R, Goldberg J Relation of Gothic arch apex to dentist-assisted centric relation. J Prosthet Dent. 1980; 44:78-81
Yeshwante B, Kale N, Baig N, Parasrampuria N. A path way to the centric – gothic arch. Int J Allied Med Sci Clin Res. 2015; 3:308-312
Cawood JI, Howell RA. A classification of the edentulous jaws. Trauma; preprosthetic surgery. Int J Oral Maxillofac Surg. 1988; 17:232-236
Saini V, Singla R. Biofunctional prosthetic system: a new era complete denture. J Pharmacy Bioallied Sci. 2011; 3:170-172
Nekora-Azak A, Evlioglu G, Özdemir-Karataş M, Keskin H. Use of biofunctional prosthetic system following partial maxillary resection: a clinical report. J Oral Rehabil. 2005; 32:693-695
Utz KH, Müller F, Lückerath W, Fuß E, Koeck B. Accuracy of check-bite registration and centric condylar position. J Oral Rehabil. 2002; 29:458-466
Ikeda K, Kawamura A, Ikeda R. Assessment of optimal condylar position in the coronal and axial planes with limited cone-beam computed tomography. J Prosthodont. 2011; 20:432-438
Ferreira A de F, Henriques JCG, Almeida GA Comparative analysis between mandibular positions in centric relation and maximum intercuspation by cone beam computed tomography (CONE-BEAM). J Appl Oral Sci. 2009; 17:27-34
Henriques JC, Fernandes Neto AJ, Almeida Gde A Cone-beam tomography assessment of condylar position discrepancy between centric relation and maximal intercuspation. Braz Oral Res. 2012; 26:29-35
Celenza FV. The centric position: replacement and character. J Prosthet Dent. 1973; 30:591-598
The Use of a Gothic Arch Tracing to Record Centric Relation in the Construction of Complete Dentures Kenneth J Strain Philippa Hoyle Zaid Ali Stephen J Bonsor Dental Update 2024 49:1, 707-709.
Authors
Kenneth JStrain
BDS, Dip H&T, PGC Med Ed, MFDS RCS(Eng)
Dental Core Trainee in Restorative Dentistry, Leeds Dental Institute, Worsley Building, Clarendon Way, Leeds
Specialty Registrar in Restorative Dentistry, Department of Restorative Dentistry, Charles Clifford Dental Hospital, 76 Wellesley Road, Sheffield S10 2SZ, UK (philippahoyle1@hotmail.co.uk)
BDS(Hons) MSc FHEA FDS RCPS(Glasg) FDFTEd FCGDent GDP
The Dental Practice, 21 Rubislaw Terrace, Aberdeen; Hon Senior Clinical Lecturer, Institute of Dentistry, University of Aberdeen; Online Tutor/Clinical Lecturer, University of Edinburgh, UK.
The establishment of a fixed and reproducible reference point (centric relation) is critical when reorganizing the occlusion in a dentate patient or constructing complete dentures in an edentulous patient. There are many techniques for guiding the patient's mandible into centric relation and recording the relationship between the maxilla and mandible in this position. Some patients are resistant to being manipulated into this position and have an unreproducible habitual path of closure. A gothic arch tracing is considered to be the most reliable and predictable method of determining centric relation. The present article describes the gothic arch tracing technique and illustrates its use in an edentulous patient during the construction of complete dentures.
CPD/Clinical Relevance: The gothic arch technique can be used to predictably locate centric relation in both dentate and edentulous patients.
Article
During the construction of complete dentures, it is essential to have a clinically reproducible position into which the patient's mandible may be placed when registering the occlusion.1 This position is known as centric relation (CR) and has been defined as a ‘maxillomandibular relationship, independent of tooth contacts, in which the condyles articulate in the anterior–superior position against the posterior slopes of the articular eminences’.2 CR, which ultimately relates to condylar position, has been argued to be the single most important measurement made during the construction of complete dentures.3 Various methods to locate CR have been suggested2,3,4 with the gothic arch tracer technique demonstrated to be the most reliable.1,5 This article discusses and illustrates the use of the gothic arch tracing in a patient who was persistently resistant to manipulation into CR using a conventional technique, and their habitual path of closure was not reproducible.
Why is finding CR important?
Despite the diversity of opinion regarding the nature of CR,6 it has been used in restorative dentistry as a stable and reproducible position when registering the occlusion in the provision of complete dentures in edentulous patients.7,8,9,10 In dentate patients, CR needs to be used only where a stable intercuspal position (ICP) is not present or where there is a clinical need to reorganize the occlusion at a new vertical dimension. Retruded contact position (RCP) relates to the position of the teeth, or in the case of edentulous patients, the tooth set up on the denture and not to condylar position.2 Mandibular movement in centric relation is purely rotational, although the mandible can make vertical, lateral and protrusive movements by moving away from CR. In other words, recording CR allows the clinician to define the antero-posterior position of the mandible relative to the maxilla.1
The edentulous patient, by definition, has no natural tooth contacts to produce a centric occlusion (CO) or retruded contact position (RCP),2 so the intermaxillary relationships will need to be recorded using wax occlusal registration rims with contact that will be located on the retruded arc of closure. The position of the mandible along this arc of closure will be determined in part by the occlusal vertical dimension (OVD) set by the dentist and patient. This information can then be transferred to the dental laboratory, permitting the casts to be mounted on an articulator. The denture teeth can then be set up for denture fabrication in this position. An error at this stage can result in occlusal discrepancies rendering the protheses uncomfortable at best and at worst unwearable.1 CR has been shown to be a reproducible position to record clinically11,12 and denture usage has been found to be positively associated with an increased accuracy of CR relationship recording.13
Recording CR
Recording an accurate CR position is multifactorial.14 Numerous variables influence the successful registration of CR, such as clinician preference, experience and training, dental material(s) recording method used, the way in which the mandible is manipulated, the patient's ability to co-operate with the procedure, their circadian rhythm and the time of day.15,16,17,18
There are many clinical techniques to guide a patient into CR and for recording CR.19 Methods for guiding a patient into CR can be classified as either patient- or clinician-guided, and some methods can be used in both dentate and edentulous patients. The patient-guided methods for edentulous patients include the Schuyler method, the physiological (swallowing) technique, gothic arch tracing and digital systems such as the Myo-motor system.4,20 The Schuyler technique4,21 involves the patient putting their tongue to the posterior roof of mouth and closing slowly into a registration material.22 Clinician-guided methods for placing the mandible in CR include chin-point manipulation, three-finger chin-point manipulation and bimanual manipulation.4 More detailed descriptions of the multiplicity of techniques available can be found in the literature.4,17,20
Techniques for creating an inter-occlusal record with the mandible in CR in edentulous patients involves the use of wax registration rims and intra-oral tracings. Various dental materials may be used to record interocclusal relationships such as (poly)vinylsiloxane (PVS), zinc oxide eugenol, modelling wax or beauty wax, or a combination thereof.22 Wax rims give good control of the OVD being recorded and can be used with a facebow registration to mount the casts on a semi-adjustable articulator. However, the stability of the registration rim on the edentulous arch may be a limiting factor and this can be optimized using an appropriately extended heat-cured acrylic base.19 Regardless of baseplate material used, the need to check for stability during the recording process should be stressed.
Gothic arch tracing
Gothic arch tracing, also known as arrow point tracing, has a long history, first being described by Hesse in 189721 and popularized by Gysi in 1910.23 The latter argued that accurate alignment of the maxilla and mandible would improve the phonetics, aesthetics and function of dental prostheses. Gothic arch tracing can be carried out quickly and can help to improve the quality and reproducibility of this process24 for both dentate and edentulous patients. The technique involves tracing the movement of the mandible in relation to the maxilla using wax occlusal registration rims combined with PMMA bases containing a metal plate and a stylus. The gothic arch tracing is based on rotational movement around the condyles, with the condyles moving back into centric relation when transitioning between left and right lateral excursions. It is also possible to carry out a gothic arch tracing using extra-oral apparatus, but this technique is not thought to be as accurate as an intra-oral recording.25 The technique may be used for remounting existing complete dentures using a system such as the Centrofix system (Amann Girrbach, Koblach, Austria), which consists of two metal plates, one with a stylus and the other with a tracing surface. The plates can be mounted to the patient's existing dentures and any issues with the vertical aspect of the dentures altered by adjusting the height of the stylus. The patient's CR position can then be recorded and the denture sent to the laboratory for an appropriately trained technician to remount the teeth.
For the edentulous patient, intra-oral tracing methods such as gothic arch give the clinician the ability to set the patient's OVD with the adjustable stylus giving confidence that the CR being recorded is correct. If desired, this method may also be used in combination with a facebow transfer. Villa26 stated that gothic arch tracings are invaluable for reproducing working and non-working side lateral movement paths. McCord and Grant1 described gothic arch tracing as being the most positive and successful method for recording CR. Michman and Langer5 found a gothic arch tracing to be more accurate than traditional wax rims. The clinical procedure of a gothic arch tracing is now illustrated.
Clinical technique in an edentulous patient
The described techniques were used to ensure optimal accuracy of the placement of the dentures as the patient had been referred to the department with suspected medication-related osteonecrosis of the jaw (MRONJ) secondary to poorly fitting complete dentures. Ill-fitting dentures have been shown to increase the risk of developing MRONJ in patients taking anti-resorptive or anti-angiogenic medications.27 It was decided, therefore, to use the gothic arch tracing technique in an attempt to gain a recording of centric relation as accurately and predictably as possible to reduce any potential trauma to the denture-bearing tissues.
After primary and secondary impressions had been made to permit the construction of the working casts, conventional occlusal registration rims on heat-cured PMMA bases were prescribed (Figure 1). Heat-cured bases have a number of advantages, such as better retention and stability, so allowing the clinician to assess these parameters clinically. As they are more rigid and dimensionally stable than other traditionally used materials, such as wax or shellac,19 it is easier to accurately and predictably record the occlusion by using them. These registration rims are used to approximate the patient's OVD and facilitate the correct vertical placement of the apparatus' stylus. A decreased OVD at this stage can lead to difficulties in setting the OVD when recording the CR using the gothic arch tracer.
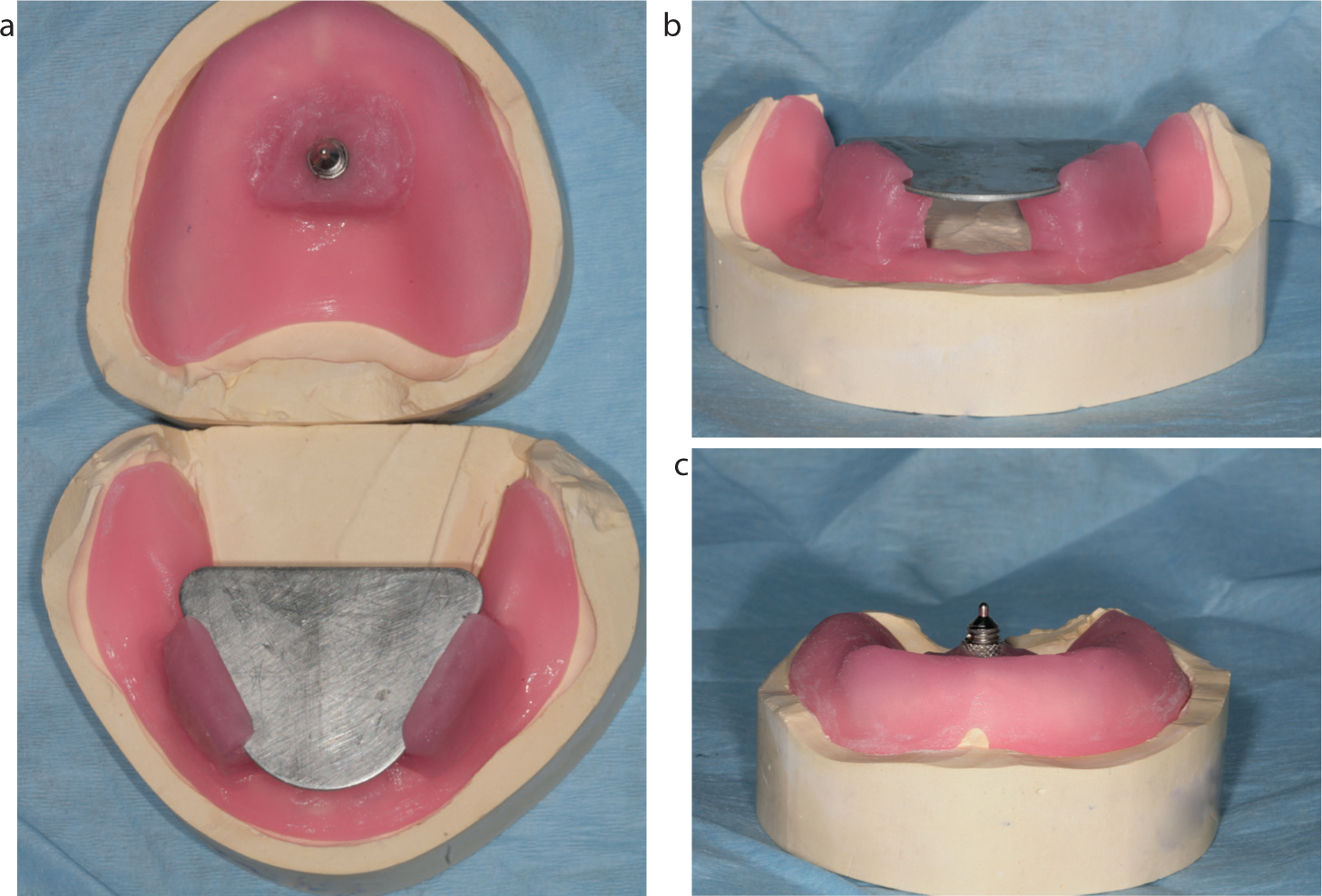
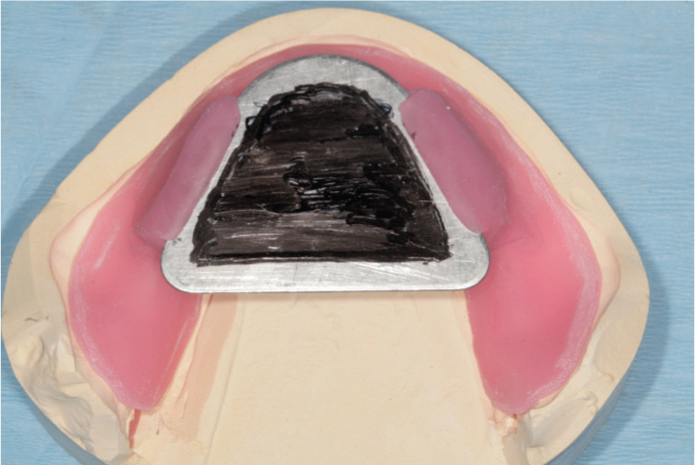
In addition, light-cured PMMA bases with the gothic arch plate mounted on the lower component and stylus mounted on the upper were constructed (Figure 2). Note that these can be mounted in the other arch, which would change the orientation of the gothic arch tracing, in other words, the direction of the arrow. The stylus, also known as the central bearing point,28 is adjusted until it contacts the recording plate at right angles. The adjustability of the stylus allows the clinician to set the desired occlusal vertical dimension for the patient and thereby influence both the OVD and subsequent freeway space of the patient, which are crucial for denture comfort, function and acceptable aesthetics.1 The point contact between the stylus and the clutch plate should be the only point of contact between the maxilla and the mandible. The lower plate should be located on well-formed and stable areas of the mandible to reduce the risk of distortion during the procedure. The clinician then rehearsed with the patient the excursive and protrusive movements to the extremes possible for the patient. To record the tracing, a marker pen, crayon, thin layer of occlusal marking spray (eg Occlude, Pascal International Inc, Bellevue, WA, USA) or articulating paper may be rubbed on the plate so that the surface of the clutch plate may be scratched off by the stylus. The indicator medium in this case was a black marker pen (Figure 3).
Figure 2.
(a–c) Light-cured PMMA bases with the gothic arch plate mounted on the lower component and stylus mounted on the upper.Figure 3. A black marker pen was used to cover the plate as an indicating medium.
The occlusion was recorded using a conventional technique and the previously mentioned occlusal rims with the OVD being verified by using two extra-oral marks (one on the maxilla and the other on the mandible) and callipers (Figure 4).
Figure 4. The occlusion was recorded using the registration rims and the OVD checked with callipers.
Reference grooves were cut in upper and lower blocks while the patient was in ‘centric relation’ achieved through bimanual manipulation. No recording material was placed between the occlusal rims (Figure 5).
Figure 5. Reference grooves cut in upper and lower blocks while the patient is in ‘centric relation’ achieved through bimanual manipulation. Note no recording material has been placed between the rims.
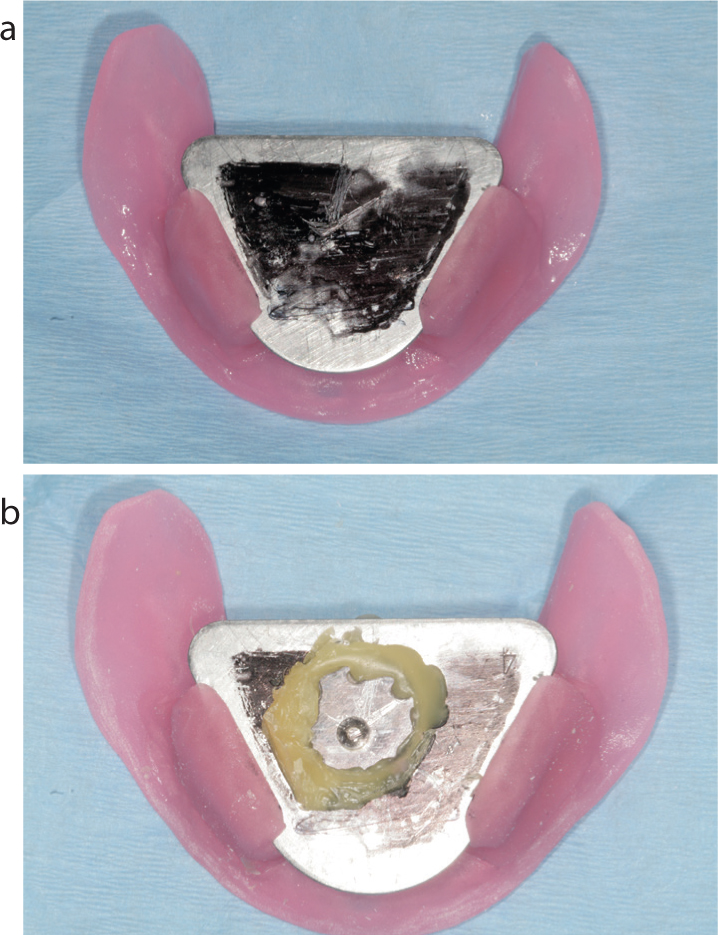
The light-cured bases with gothic arch components in situ were placed back in the mouth, ensuring that there was no overextension or interferences present, and the stability of the bases was satisfactory. The OVD recorded from the occlusal rims was used, and the screw on the stylus adjusted, until the rims came together at the same OVD measurement (Figure 6). Once the patient's OVD had been set at the correct height, the patient replicated the previously rehearsed movements and the stylus traced an arrowhead or gothic arch tracing on the tracing plate (Figure 7a,b). The intersection of the three lines on the tracing indicates centric relation. Meyers described the apex of the tracing as the starting point from which lateral and protrusive movements are made.29Figure 7a demonstrates that, even with techniques to improve the accuracy of the CR recording, we are recording a zone of CR, and gothic arch tracing assists the clinician in minimizing this zone.
Figure 6. Light-cured PMMA bases with the gothic arch plate in situ showing the stylus as a single point of contact. Baseplates were assessed for free movement and any obstructions removed prior to recording the gothic arch tracing.Figure 7.
(a, b) The recording plate with the gothic arch tracing visible and the same image with superimposed lines to highlight the shape of the tracing.
Once the tracing had been recorded, it was important that it was verified to confirm its accuracy. A clear Perspex locking plate was then attached to the gothic arch plate using Sticky Wax (Kemdent, Swindon, UK), ensuring the hole/depression is accurately positioned over the centric point where all three lines meet (Figure 7b).
The plates were returned to the patient's mouth and the patient guided back into CR allowing the stylus to engage the perforation in the Perspex, thus confirming the reproducibility of the CR recording, taking care not to change the recorded OVD. At this point, the patient's vertical and anterior-posterior maxillo-mandibular relationship had been recorded.
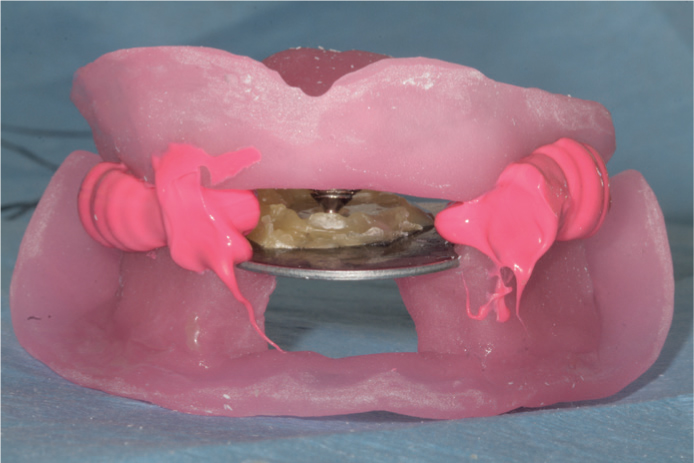
VPS Tray Adhesive (3M ESPE, Seefeld, Germany) was applied to the upper and lower light-cured bases, which were placed intra-orally, and the patient guided into the centric relation position so that the stylus engaged into the depression in the locking plate. VPS bite registration material (Imprep AC, Unodent, UK) was then placed between the two bases and allowed to set, so recording the centric relationship and enabling all components to be removed as one unit (Figure 8).
Figure 8. The clear Perspex locking plate has been attached to the gothic arch plate using Sticky Wax (Kemdent), ensuring the hole/depression is accurately positioned over the centric point where all three lines meet.
The dental technician was then able to use the appropriately adjusted light-cured bases with the attached gothic arch tracing to mount the casts on an adjustable articulator. The prosthetic teeth were then set up on the occlusal rims on the casts mounted with the gothic arch tracing to create the prototype dentures to try in at the next clinical appointment. To ensure optimal results, not only does the clinician need to practice the technique, they should also discuss the case with their lab technician prior to carrying out the recording. This is to ensure that the laboratory technician has appropriate training to make use of the results from the reading and to transfer them appropriately to the articulator.
Interpreting the gothic arch tracing
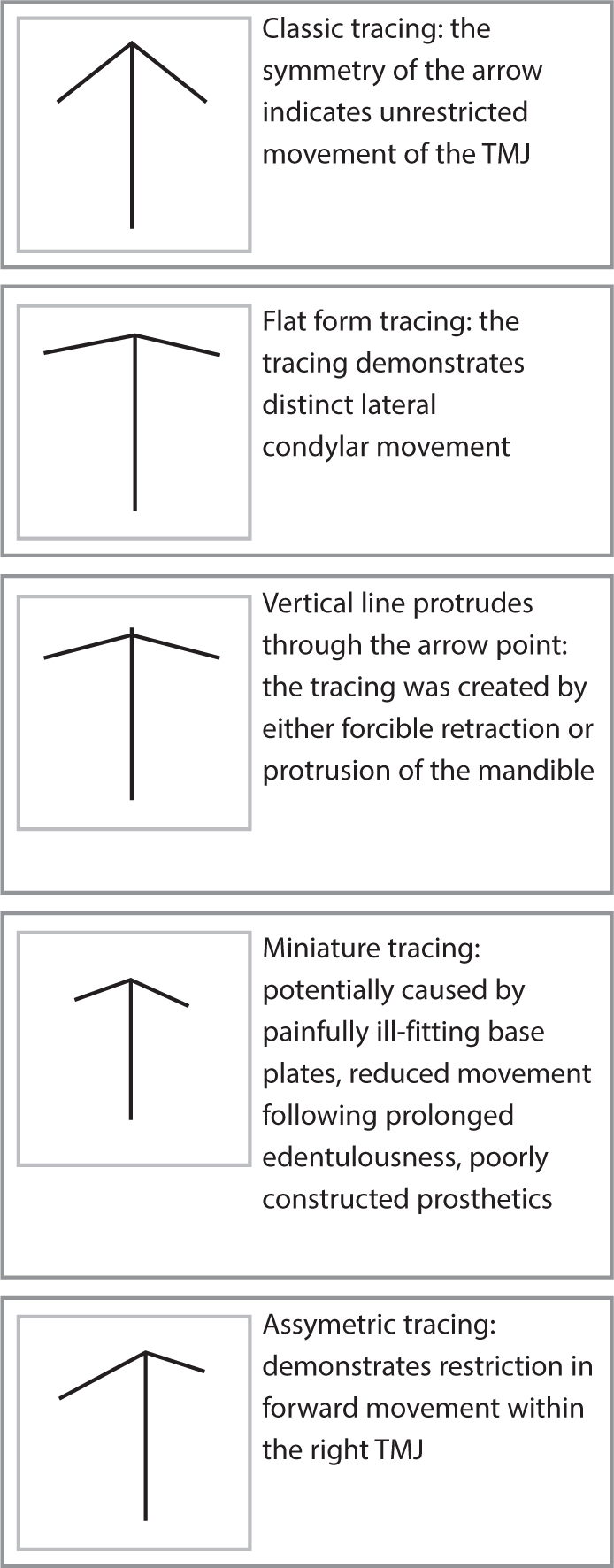
The shape of the gothic arch tracing will be determined by the posterior anatomical determinants of occlusion outlined earlier. Albert Gerber described six shapes that a gothic arch tracing may take.27 These are the classical pointed form, classical flat form, weak tracing, asymmetrical form, miniature form and a tracing with the vertical line beyond the arrow point. A sharp apex on the gothic arch tracing will be obtained when the condyles rotate from a properly situated position in the glenoid fossa.3 A flat arch indicates that the patient has a more pronounced lateral movement of the condyles in the fossae. An asymmetrical tracing is indicative of an inhibition in the translation of either the left or right condyle. A miniature tracing that is similar to a classical pointed form, indicates that the patient has restricted movement of the mandible. This could be a result of ill-fitting record plates or could indicate inhibition of condylar movements, which may follow being edentulous for a long period of time. A tracing with an overextension of the protrusive trace (the shaft of the arrow head) indicates that the patient's condyles have been placed too far posteriorly within the glenoid fossa into a ‘forced’ posterior position either by the patient or by the clinician, though this can be difficult to discern from the tracing and the comfort of this position clinically for the patient is often a reliable gauge. Figure 9 gives examples of the types of tracing that may be produced.
Figure 9. Examples of the various gothic arch tracings that may be produced.30
It is important to check the stability of the rims to ensure that they have not been displaced during the recording. A weak tracing indicates that the patient needs further instruction in the required movements. Occasionally an interrupted tracing may be recorded, this is likely to be a result of a posterior interference at the heels of the recording plates and these should be checked and adjusted as necessary, and the tracing repeated.
Drawbacks to the gothic arch technique
Although the gothic arch tracing technique has been described as being the most predictable and successful method for recording CR and more accurate than traditional wax rims,1,26 there are some drawbacks to the technique.
First, it is a more time-consuming procedure compared to other techniques such as chin point manipulation. Secondly, ridge form will influence stability of the occlusal registration rims, which can influence the centric relation position recorded. A thorough assessment of ridge form using a classification such as that of Cawood and Howell31 can prove useful. Edentulous ridges lacking height or width will reduce the stability of the rims and can affect the tracing recorded. The stylus must be placed within the centre of the record base or differential pressure will be exerted and may displace the registration rims during the tracing. Large tongues can also have an effect on the stability of the occlusal registration rims. Reproducibility can be an issue for some patients, which is why it is key to rehearse the procedure multiple times prior to recording the gothic arch. To overcome the issue of reproducibility, Ivoclar Vivadent (Schaan, Liechtenstein) has developed the Biofunctional Prosthetic System (BPS) which is designed to be used in the production of complete dentures. The system's Gnathometer is similar in design to a traditional set of registration blocks with a stylus and plate.32,33,34
Despite the best efforts of clinicians and researchers to achieve a clinically reproducible CR recording, Utz et al35 found that it was impossible to precisely locate CR position, with a number of other studies finding minimal differences between CR and ICP in patients with no history of temporomandibular disorder (TMD).36,37,38 Utz et al35 compared a number of occlusal registration techniques and found that there was a median 0.3 mm discrepancy and that differences of up to 2 mm were possible for multiple occlusal registration techniques. Eriksson et al12 found that the clinical technique rather than the recording method used had a greater impact on the accuracy of the bite registration.
It may be that achieving a ‘perfect’ recording of centric relation is not possible. However, this may not be clinically significant as long as a stable record is reproducibly achieved with the mandibular condyles in a comfortable position as close as possible to CR. Occlusion is a dynamic and adaptable state that has been shown to change over time with patients that have been restored so that ICP and RCP are coincident often reintroducing a slide from ICP to RCP.39
Conclusion
Whilst not appropriate in every case, the use of a gothic arch tracing technique may be helpful in those patients who are resistant to being manipulated into CR or who have an unfavourable habitual position when a dentate patient's occlusion requires to be reorganized or in the construction of complete dentures in an edentulous patient. The gothic arch tracing technique offers the clinician a predictable and reliable means of determining CR.