Patel S, Arias A, Whitworth J, Mannocci F. Outcome of endodontic treatment – the elephant in the room. Int Endod J. 2020; 53:291-297
Patel S, Foschi F, Mannocci F, Patel K. External cervical resorption: a three-dimensional classification. Int Endod J. 2018; 51:206-214
Patel S, Brown J, Semper M European Society of Endodontology position statement: use of cone beam computed tomography in endodontics. Int Endod J. 2019; 52:1675-1678
Patel S, Lambrechts P, Shemesh H, Mavridou A. European Society of Endodontology position statement: external cervical resorption. Int Endod J. 2018; 51:1323-1326
Andreasen JO. Luxation of permanent teeth due to trauma. A clinical and radiographic follow-up study of 189 injured teeth. Scand J Dent Res. 1970; 78:273-286
Andreason FM, Zhijie Y, Thomsen BL, Anderson PK. Occurrence of pulp canal obliteration after luxation injuries in the permanent dentition. Endod Dent Traumatol. 1987; 3:103-115
Robertson A, Andreason F, Bergenholtz G Incidence of pulp necrosis subsequent to pulp canal obliteration from trauma of permanent incisors. J Endod. 1996; 22:557-560
Jacobsen I, Kerekes K. Long term prognosis of traumatized permanent anterior teeth showing calcifying processes in the pulp cavity. Scand J Dent Res. 1977; 85:588-598
O Carroll MK, Duncan WK, Perkins TM. Dentin dysplasia: Review of the literature and a proposed sub classification based on radiographic findings. Oral Surg Oral Med Oral Pathol. 1991; 72:119-125
Shakiba B, Hamedy R, Pak JG Influence of increased patient age on longitudinal outcomes of root canal treatment: a systematic review. Gerodontology. 2017; 34:101-109
Connert T, Zehnder MS, Weiger R Microguided endodontics: accuracy of a miniaturized technique for apically extended access cavity preparation in anterior teeth. J Endod. 2017; 43:787-790
Kim JE, Shim JS, Shin Y. A new minimally invasive guided endodontic microsurgery by cone beam computed tomography and 3-dimensional printing technology. Restor Dent Endod. 2019; 44
Moreno-Rabié C, Torres A, Lambrechts P, Jacobs R. Clinical applications, accuracy and limitations of guided endodontics: a systematic review. Int Endod J. 2020; 53:214-231
Connert T, Krug R, Eggmann F Guided endodontics versus conventional access cavity preparation: a comparative study on substance loss using 3-dimensional-printed teeth. J Endod. 2019; 45:327-331
Maia LM, de Carvalho Machado V, da Silva NRFA Case reports in maxillary posterior teeth by guided endodontic access. J Endod. 2019; 45:214-218
Sônia TDO, Camila de Freitas MB, Santa-Rosa CC, Machado VC. Guided endodontic access in maxillary molars using cone-beam computed tomography and computer-aided design/computer-aided manufacturing system: a case report. J Endod. 2018; 44:875-879
Tavares WLF, Viana ACD, de Carvalho Machado V Guided endodontic access of calcified anterior teeth. J Endod. 2018; 44:1195-1199
Low KM, Dula K, Bürgin W, Arx T. Comparison of peri-apical radiography and limited cone-beam tomography in posterior maxillary teeth referred for apical surgery. J Endod. 2008; 34:557-562
Abubara A, Baratto-Filho F, Aguiar Anele J Efficacy of clinical and radiological methods to identify second mesiobuccal canals in maxillary first molars. Acta Odontol Scand. 2013; 71:205-209
Bystrom A, Sundqvist G. Bacteriologic evaluation of the efficacy of mechanical root canal instrumentation in endodontic therapy. Scand J Dent Res. 1981; 89:321-328
Byström A, Sundqvist G. The antibacterial action of sodium hypochlorite and EDTA in 60 cases of endodontic therapy. Int Endod J. 1985; 18:35-40
Sharma S, Sharma V, Grover S, Mittal M. CBCT diagnosis and endodontic management of a maxillary first molar with unusual anatomy of two palatal canals: a case report. J Conserv Dent. 2014; 17
Durack C, Patel S Cone beam computed tomography in endodontics. Braz Dent J. 2012; 23:179-191
Abella F, Morales K, Garrido I Endodontic applications of cone beam computed tomography: case series and literature review. G Ital Endod. 2015; 29:38-50
Shemesh H, Cristescu RC, Wesselink PR, Wu MK. The use of cone-beam computed tomography and digital peri-apical radiographs to diagnose root perforations. J Endod. 2011; 37:513-516
Mena-Álvarez J, Rico-Romano C, Lobo-Galindo AB, Zubizarreta-Macho Á. Endodontic treatment of dens evaginatus by performing a splint guided access cavity. J Esthet Restor Dent. 2017; 29:396-402
Ali A, Arslan H. Guided endodontics: a case report of maxillary lateral incisors with multiple dens invaginatus. Restor Dent Endod. 2019; 44
Byun C, Kim C, Cho S Endodontic treatment of an anomalous anterior tooth with the aid of a 3-dimensional printed physical tooth model. J Endod. 2015; 41:961-965
Lai PT, Yang SF, Lin YM, Ho YC. Computer-aided design-guided endodontic microsurgery for a mandibular molar with hypercementosis. J Formos Med Assoc. 2019; 118:1471-1472
Perez C, Finelle G, Couvrechel C. Optimisation of a guided endodontics protocol for removal of fibre-reinforced posts. Aust Endod J. 2020; 46:107-114
Estrela C, Bueno MR, De Alencar AH Method to evaluate inflammatory root resorption by using cone beam computed tomography. J Endod. 2009; 35:1491-1497
Patel S, Dawood A, Wilson R The detection and management of root resorption lesions using intraoral radiography and cone beam computed tomography – an in vivo investigation. Int Endod J. 2009; 42:831-838
Heithersay GS. Invasive cervical resorption. Endod Topics. 2004; 7:73-92
Heithersay GS. Clinical, radiologic, and histopathologic features of invasive cervical resorption. Quintessence Int. 1999; 30:27-37
Patel S, Brown J, Pimentel T Cone beam computed tomography in endodontics – a review of the literature. Int Endod J. 2019; 52:1138-1152
Kraus RD, von Arx T, Gfeller D Assessment of the nonoperated root after apical surgery of the other root in mandibular molars: a 5-year follow-up study. J Endod. 2015; 41:442-446
DiAngeli AJ, Andreasen JO, Ebelesede KA International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations of permanent teeth. Dent Traumatol. 2012; 28:2-12
Cohenca N, Simon JH, Roges R Clinical indications for digital imaging in dento-alveolar trauma. Part 1: traumatic injuries. Dent Traumatol. 2007; 23:95-104
Li F, Li J, Zhang D, Wu F. Role of computed tomography scan in dental trauma: a cross-sectional study. Dose Response. 2018; 16
Cohenca N, Silberman A. Contemporary imaging for the diagnosis and treatment of traumatic dental injuries: a review. Dent Traumatol. 2017; 33:321-328
Bernardes RA, de Moraes IG, Duarte MAH Use of cone-beam volumetric tomography in the diagnosis of root fractures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 108:270-277
Amir FA, Gutmann JL, Witherspoon DE. Calcific metamorphosis: a challenge in endodontic diagnosis and treatment. Quintessence Int. 2001; 32:447-455
Andreasen FM, Andreasen JO, Bayer T. Prognosis of root fractured permanent incisors; prediction of healing modalities. Endod Dent Traumatol. 1989; 5:11-22
Kruse C, Spin-Neto R, Evar Kraft DC Diagnostic accuracy of cone beam computed tomography used for assessment of apical periodontitis: an ex vivo histopathological study on human cadavers. Int Endod J. 2019; 52:439-450
Kanagasingam S, Lim CX, Yong CP Diagnostic accuracy of peri-apical radiography and cone beam computed tomography in detecting apical periodontitis using histopathological findings as a reference standard. Int Endod J. 2017; 50:417-426
de Paula-Silva FW, Wu MK, Leonardo MR Accuracy of peri-apical radiography and cone-beam computed tomography scans in diagnosing apical periodontitis using histopathological findings as a gold standard. J Endod. 2009; 35:1009-1012
Uraba S, Ebihara A, Komatsu K Ability of cone-beam computed tomography to detect peri-apical lesions that were not detected by peri-apical radiography: a retrospective assessment according to tooth group. J Endod. 2016; 42:1186-1190
Davies A, Mannocci F, Mitchell P The detection of peri-apical pathoses in root filled teeth using single and parallax peri-apical radiographs versus cone beam computed tomography–a clinical study. Int Endod J. 2015; 48:582-592
Liang Y, Li G, Wesselink P, Wu M. Endodontic outcome predictors identified with peri-apical radiographs and cone-beam computed tomography scans. J Endod. 2011; 37:326-331
Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: peri-apical health. Int Endod J. 2011; 44:583-609
Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J. 2006; 39:921-930
Venskutonis T, Daugela P, Strazdas M, Juodzbalys G. Accuracy of digital radiography and cone beam computed tomography on periapical radiolucency detection in endodontically treated teeth. J Oral Maxillofac Res. 2014; 5
Cheung GSP, Wei WLL, McGrath C. Agreement between peri-apical radiographs and cone-beam computed tomography for assessment of peri-apical status of root filled molar teeth. Int Endod J. 2013; 46:889-895
Yeung AW, Jacobs R, Bornstein MM. Novel low-dose protocols using cone beam computed tomography in dental medicine: a review focusing on indications, limitations, and future possibilities. Clin Oral Investig. 2019; 23:2573-2581
Krastl G, Zehnder MS, Connert T Guided endodontics: a novel treatment approach for teeth with pulp canal calcification and apical pathology. Dent Traumatol. 2016; 32:240-246
Neves FS, Vasconcelos TV, Vaz SL Evaluation of reconstructed images with different voxel sizes of acquisition in the diagnosis of simulated external root resorption using cone beam computed tomography. Int Endod J. 2012; 45:234-239
Bechara B, McMahan CA, Nasseh I Number of basis images effect on detection of root fractures in endodontically treated teeth using a cone beam computed tomography machine: an in vitro study. Oral surg Oral Med Oral Pathol Oral Radiol. 2013; 115:676-681
Durack C, Patel S, Davies J Diagnostic accuracy of small volume cone beam computed tomography and intraoral peri-apical radiography for the detection of simulated external inflammatory root resorption. Int Endod J. 2011; 44:136-147
Hashem D, Brown JE, Patel S An in vitro comparison of the accuracy of measurements obtained from high-and low-resolution cone-beam computed tomography scans. J Endod. 2013; 39:394-397
Lennon S, Patel S, Foschi F Diagnostic accuracy of limited-volume cone-beam computed tomography in the detection of peri-apical bone loss: 360° scans versus 180° scans. Int Endod J. 2011; 44:1118-1127
Jones D, Mannocci F, Andiappan M The effect of alteration of the exposure parameters of a cone-beam computed tomographic scan on the diagnosis of simulated horizontal root fractures. J Endod. 2015; 41:520-525
Hendee W, Edwards FM. ALARA and an integrated approach to radiation protection. Semin Nucl Med. 1986; 16:142-150
NCRP. Achievements of the past 50 years and addressing the needs of the future. Fiftieth annual meeting of the National Council on Radiation Protection and Measurements (NCRP). 2014. https://ncrponline.org/wp-content/uploads/2018/08/Annual/pp50.pdf (accessed November 2021)
When to consider the use of CBCT in endodontic treatment planning in adults Nisha Dowling Andrew Gemmell David Edwards Dental Update 2024 48:11, 707-709.
With the recent publication of European Society of Endodontology (ESE) position statements, newly proposed three-dimensional (3D) classification for external cervical resorption and new techniques such as guided access using 3D printed splints, cone beam computed tomography (CBCT) has never been more important in endodontics. Furthermore, CBCT machines are becoming more affordable, resulting in imaging being more accessible in primary and secondary care. This, aligned with higher resolution images at lower effective doses, means CBCT must now be considered when planning and delivering a range of endodontic procedures.
CPD/Clinical Relevance: To review the use of CBCT in endodontics and raise awareness of its indications in primary and secondary care.
Article
Imaging is essential before commencing any surgical or non-surgical endodontic treatment to understand root morphology and adequately carry out the mechanical aspects of treatment, giving valuable information for treatment planning and execution.1 Currently, two-dimensional (2D) imaging is most commonly employed for assessment, but has several limitations including superimposition, distortion, magnification and background noise, making interpretation subjective.2 The introduction of CBCT has transformed dental imaging, improving diagnosis, offering more informed treatment planning, and even opportunities for novel treatment approaches. CBCT may be essential for comprehensive treatment planning and the safe execution of treatment in some cases, whereas it may be a useful adjunct in others. This is recognized both in the newly proposed three-dimensional (3D) classifications for external cervical resorption,3 and in the recently published European Society of Endodontology (ESE) position statements.4,5 The advantages and limitations of CBCT in endodontics are presented, with some clinical examples discussed.
Negotiation of calcified canals
Canal obliteration can be idiopathic, due to hereditary disorders (eg dentinogenesis imperfecta) or occur following trauma, orthodontic treatment, pulpal injury, caries or restorative treatment.6,7,8,9,10 Furthermore, the normal ageing processes, whereby secondary dentine is deposited, can complicate canal location and negotiation.11 Although not always essential, in anatomically challenging cases, where difficulty is greater and the risk of perforation, deviation and failure may be higher, planning cases using CBCT has been shown to improve outcomes and reduce complications.12
Guided endodontic treatment
Guided access in endodontics has resulted in improved success rates, efficiency and patient experience in both orthograde and surgical endodontics, as summarized in Table 1. The wealth of information about tooth morphology and surrounding structures provided by CBCT can be combined with scan data of the teeth using specialist software typically used for implant planning. The data may be from an intra-oral scan or scan of a cast from an alginate or silicone impression. Following this, a 3D drilling pathway is planned, and a guide to accommodate this either 3D printed or milled. Additionally, digital burs and files can be designed and superimposed via the software to allow personalized access to a tooth, and these can be miniaturized if conventional burs are too wide and unsuitable.13Figure 1 illustrates the stages involved in the fabrication of a surgical guide for access.
Improved canal location
More conservative access cavities
Less operator-sensitive access
Lower risk to vital structures/reduced iatrogenic damage
Reduced surgery time
Fewer intra-operative radiographs necessary
Figure 1.
(a) UL1 was tender to percussion and clearly discoloured after a previous traumatic injury and (b) the incisal part of the root canal is seemingly obliterated. (c) The provisional filling finishing the first attempt. (d) Following CBCT and intra-oral data, virtual planning was completed and the data were ready to be sent for production of the guide. Note, the location of the new position of the access cavity is marked with a blue dot in (c). (e) With the guide in place, the guided drilling could then begin with the drill in a slow-speed handpiece. (f) The successful negotiation and further instrumentation was performed with the rubber dam in place. Note, the enamel of the access cavity was removed prior to guided drilling and, because of the selected angle, the access cavity was slightly off the first access cavity. (g) The completed root filling prior final restoration. With permission from J Buchgreitz and L Bjørndal.
Guided access offers numerous benefits over conventional access cavities. Of utmost importance is the improved accuracy and predictability of canal location, which appears to be independent of operator experience.14,15,16,17,18 This may allow for considerably more complex cases, which may otherwise have been referred to specialist centres, to be carried out in primary care. Guided access techniques may also be more conservative than conventional approaches, thereby preserving tooth structure and integrity.18,19 The use of guided access has also been reported to be more efficient, reducing surgery time by up to 30%.14
Complex anatomy
Complex canal anatomy increases risk of iatrogenic damage. Identifying this in advance using 3D imaging enables appropriate planning to minimize risk and maximize successful outcomes. Clinicians and patients can be fully informed, consent is more valid and, where necessary, clinicians can appropriately refer or consult guidance before treating.
Supplemental or missed canals
CBCT demonstrates a superior ability to identify additional or supplemental canals,20,21 thereby facilitating the preparation, disinfection and obturation of all canals, essential to eliminate bacteria and facilitate healing.22,23 If canal anatomy is complex or peri-apical radiographs unclear, CBCT should be considered,24 with prior assessment of anatomy reducing the likelihood of iatrogenic errors including ledges, transportations and perforations.25 In the event of a perforation, or where a perforation is suspected, detection by 2D imaging may be challenging because of superimposition, particularly labial and lingual root surface defects26 while 3D imaging has a greater ability to detect and assess,27 again facilitating appropriate management.
Atypical root morphology
CBCT has also proved beneficial in the management of atypical root morphology, for example, dens invaginatus and dens evaginatus.28,29 As well as facilitating a guided approach to treatment, the diagnostic value of CBCT is greater than 2D imaging in such cases. This allows clearer visualization of the precise location and depth of the pulpal tissue within the tubercle and intricacies of canal morphology, clarifying if and where there may be communications between the invagination and the primary canal. Other examples of challenging root morphology successfully treated with the aid of CBCT and guided access include dilaceration, hypercementosis and fibre post removal.30,31,32
Resorption
Resorption is defined as a physiological or pathological process resulting in the loss of dentine, cementum and/or bone.33 Diagnosis of resorption via CBCT has greater accuracy than peri-apical radiographs,34,35 and is indispensable to properly diagnose and treatment plan more advanced resorption cases.4 Where operative intervention is planned, it is desirable to gain as much information as possible prior to undertaking irreversible procedures in order to make informed decisions. The importance of CBCT in treatment planning is illustrated in Figure 2. This is especially true in cervical resorption, which can be particularly aggressive.36 This is recognized with the latest ESE position statement3,5 in which a new 3D classification is recommended and it is acknowledged that a 2D classification37 (Table 2) cannot fully identify the extent of the lesion, possibly resulting in inappropriate surgery when an extraction followed by replacement may be the most appropriate option. It is important to note that CBCT is only indicated where there are uncertainties regarding restorability or treatment options, as illustrated in Figure 3.
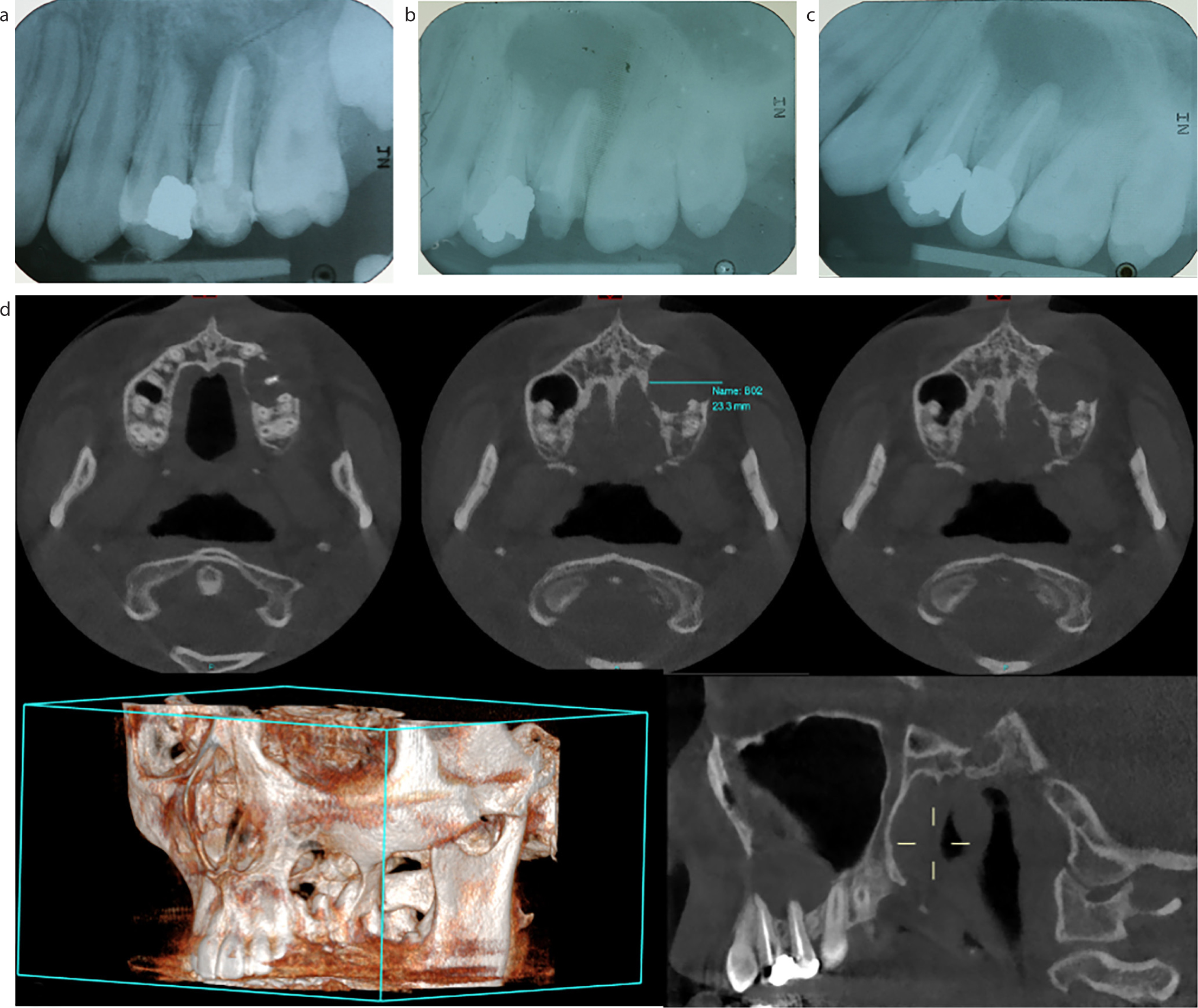
Figure 2.
(a) Peri-apical radiograph shows cervical resorption of UR4 invading into root dentine that appears to be amenable to surgical repair. (b–d) Following referral by the patient's GDP, a CBCT was taken that shows the resorptive lesion extending to the apex of the palatal root (3D classification: 4;D;p), which was not visible from the 2D image (2D classification: class 2, borderline 3). According to the 2D classification, the prognosis may have been good (77.8–100%) and treatment may have been attempted. However, 3D assessment by CBCT rendered the tooth unrestorable, altered the treatment plan and the root was subsequently extracted before surgical repair was attempted.
2D classification based on peri-apical radiographs
3D classification based on CBCT
Classification
Description
Prognosis
Height
Circumferential spread
Proximity to the root canal
Class I
A small invasive resorptive lesion near the cervical area with shallow penetration into dentine
100%
1. At cementoenamel junction level or coronal to the bone crest (supracrestal)
a. ≤90°
d. Lesion confined to dentine
Class 2
A well-defined invasive resorptive lesion that has penetrated close to the coronal pulp chamber, but shows little or no extension into radicular dentine
100%
2. Extends into coronal third or the root and apical to the bone crest (subcrestal)
b. >90° to ≤180°
p. Probably pulpal involvement
Class 3
A deeper invasion of dentine by resorbing tissue, not only involving the coronal dentine, but also extending into the coronal third of the root
77.8%
3. Extends into mid-third of the root
c. >180° to ≤270°
Class 4
A large, invasive resorptive process that has extended beyond the coronal third
12.5%
4. Extends into apical third of the root
d. >270°
Figure 3.
(a) A peri-apical radiograph of internal inflammatory resorption. In this case, the lesion was explored using a microscope, disinfected and obturated using a thermoplastic technique. (b) In this situation, CBCT was not necessary as the peri-apical radiograph provided sufficient information.
Pre-surgical assessment
Prior to surgical endodontic treatment, 3D assessment of the surgical field has a multitude of advantages – root length and curvature can be precisely measured which is not possible with peri-apical radiographs38 and CBCT allows the option of using a guided approach, discussed previously. Apical periodontitis is identified clearly without distortion from superimposition of the cortical plate so that treatment of multi-rooted teeth can be root specific,39 which, in addition to a guided approach will largely reduce bone loss, procedure time and extent of treatment. This allows for more rapid healing, lower risk of infection and improved patient comfort, prosthetic and aesthetic outcomes.14,31,38 Relationships to anatomical structures can be fully assessed and risk of damage minimized, with guided techniques offering a reduced risk to the inferior alveolar nerve, mental nerve, maxillary antrum and adjacent teeth.14Figure 4 describes a complex endodontic case where surgery was considered but CBCT showed this to be contraindicated.
Figure 4. A 28–year-old female presented with symptoms of apical periodontitis and a radiolucent area associated with the apex of the LR3. (a) The patient's GDP was unable to locate the canal. (b) Further progress was made using a goose-neck bur and pin bur, but a canal could not be located with the operating microscope, and it was clear the root was grooved, suggesting the possibility of two canals. A CBCT was taken to assess the peri-apical region ahead of endodontic surgery because an orthograde approach had been unsuccessful. (c) Shows the presence of a figure 8–shaped root, which may have previously contained two canals, but imaging confirmed that the canals were almost completely obliterated. (d) Shows that the apex of the tooth was very close to the lingual cortex. From this information, the risks of endodontic surgery (lingual plate perforation, excessive bone loss, damage to vascular bundles) were considered too high, and the treatment plan was changed to extraction and implantation before any surgery was attempted.
Dento-alveolar trauma
For patients presenting with dento-alveolar trauma, clinical and 2D radiographic examinations may be insufficient to assess pulpal and periodontal injury or healing and CBCT may aid diagnosis and treatment planning. The International Association of Dental Traumatology guidelines recognize that CBCT can provide enhanced visualization of traumatic dental injuries, including monitoring of healing and complications, while both the ESE and American Association of Endodontists state that CBCT should be considered in the diagnosis and management of dento-alveolar trauma and detection of secondary changes, where clinical examination and conventional imaging are inconclusive.4,40,41 CBCT is particularly relevant in trauma to show a third dimension not present in peri-apical radiographs; eliminating errors that may occur with conventional intra-oral radiography including poor sensitivity detecting minimal displacements, missed diagnoses of root and alveolar fractures, superimposition and processing errors and therefore can improve the ability to accurately diagnose traumatic injuries.42
When identifying root fractures, intra-oral radiographs have limited diagnostic yield, particularly where there is no fragment displacement or formation of granulation tissue, therefore, multiple radiographs at varying angles are recommended.40,43 Accurate determination of the apical extent of a crown-root fracture is not always possible with 2D radiography and exploration of the location and extension of the fracture with a CBCT is strongly recommended to assess crown to root ratio which influences treatment options and long-term prognosis.40,44 An increased detection rate of root fractures from 30–40% with 2D imaging to 90% with a CBCT has been reported.45 The enhanced visualization of dento-alveolar injury through CBCT can show oblique components to fractures, alveolar bone fractures, displaced root fragments, subluxations and areas of trauma-induced root resorption that may otherwise not be detected and remain undiagnosed.
A further complication is that canal obliteration is a frequent finding following root fractures,46,47 therefore these cases would certainly benefit from CBCT and potentially guided access techniques for endodontic management.
If there is any suspicion that dento-alveolar trauma is not diagnosed adequately on a 2D image, CBCT should be considered to aid both diagnosis and treatment planning. Figure 5 describes a case where a patient presented with trauma to several teeth and following CBCT, the treatment plan was altered significantly from that made when assessing peri-apical radiographs only. This additional information facilitated the most appropriate treatment option and avoided an approach which could have a negative biological and financial impact.
Figure 5. A 25-year-old male presented to Newcastle Dental Hospital following dento-alveolar trauma. (a, b) Initial assessment with peri-apical radiographs show uncomplicated fractures UR1 and UL2 and complicated fracture UL1. The treatment plan for UL1 involved extraction of the coronal portion of the tooth, crown lengthening and orthodontic extrusion of the fragment prior to restoration. (c, d) However, following a CBCT, the tooth was deemed unrestorable because of the depth of the fracture margin on the buccal aspect. The tooth was therefore extracted and replaced with an implant.
Diagnosis and assessment of pathology
Apical periodontitis
Despite being the standard technique for diagnosis of apical periodontitis, 2D imaging may underdiagnose peri-apical radiolucencies because of superimposition and distortion. In cases with undiagnosed pain suggestive of apical periodontitis, where there is no clear pathology on a 2D image, CBCT may again be justified. Studies show a greater accuracy of CBCT in the diagnosis of apical pathology compared to peri-apical radiographs and suggest that a clinician would be able to differentiate most diseased and healthy teeth correctly with a high sensitivity and specificity.48,49,50,51,52 This may positively impact treatment planning when deciding whether to restore a large carious lesion or begin endodontic treatment, particularly if asymptomatic. Additionally, this may improve outcomes of endodontic therapy if CBCT leads to earlier diagnosis of apical periodontitis as the presence and size of a pre-operative radiolucency significantly reduces success (Table 3).
Factor
Influence on prognosis
Canal under instrumented short of the terminus
-12%/mm
Increasing size of peri-apical lesion
-14%/mm
Interappointment complications (pain or swelling)
-47%
Pre-operative sinus
-48%
Pre-operative peri-apical lesion
-49%
Combining 0.2% chlorhexidine and sodium hypochlorite for irrigation
-53%
Root perforation
-56%
Overextension of root filling
-62%
Use of EDTA in secondary endodontic treatment
Two-fold increase
Achieving patency at the apex
Two-fold increase
Good-quality coronal restoration
11–fold increase
Review of endodontic treatment
As well as diagnosis of endodontic disease, CBCT may also be beneficial post-operatively in assessing the quality of root filling and post-treatment healing. CBCT may reveal more suboptimal root fillings than peri-apical radiographs, identifying more voids and the extent of over/under obturation, particularly in the bucco-lingual plane,53 all of which can influence success (Table 3). Figure 6 is an example where endodontic treatment may appear to have been completed to a high standard two dimensionally, but 3D imaging suggests otherwise, offering an explanation for failure. The radiographic root apex does not always correspond with the clinical apex,54 therefore CBCT can be considered a much more precise assessment of the root filling terminus where this is unclear from 2D imaging. ESE quality guidelines state that if a lesion is unchanged or only diminished, the outcome is ’uncertain’ and should be assessed for up to 4 years.55 CBCT has a significantly superior ability to identify peri-apical lesions following root canal treatment,51,52,56,57 leading us to question whether the existing estimated success rate of 83% for primary treatment54 is overestimated while peri-apical radiographs are employed as the method for reviewing and whether CBCT should become the gold standard method.
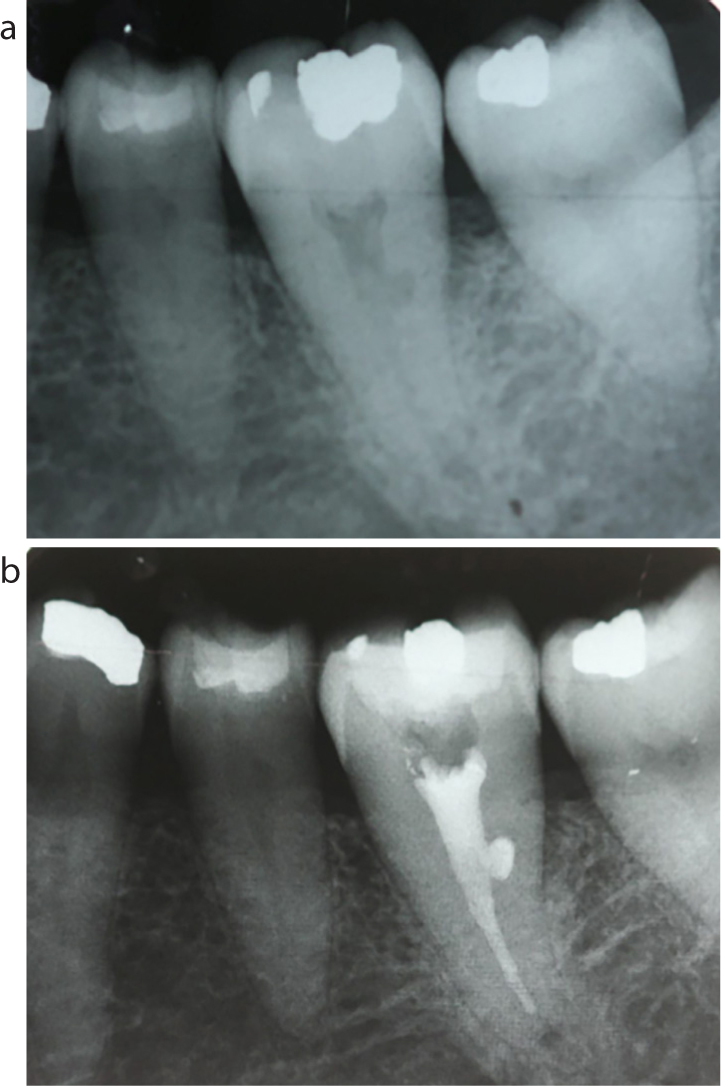
Figure 6.
(a, b) A 55-year-old female was referred because of pain from the upper anterior region. The referring GDP suspected pain from UR1. Peri-apical radiography confirmed the UR1 was obturated short of the ideal radiographic working length, and had a coronal restoration with poor margins. Despite this, no obvious peri-apical pathology was evident, prompting the use of CBCT for further investigation. This showed the UL1, which appeared to be obturated to ideal radiographic working length, was overextended and had an associated area of peri-apical pathology. This was therefore re-treated as the primary cause of the pain, which subsequently resolved. Without the information from the CBCT, it may have been appropriate to complete peri-radicular surgery
Other pathology
Benefits are also seen in diagnosing other pathologies, especially where surgical intervention is considered. Figure 7 is another example of where the employment of CBCT altered diagnosis entirely and alternative treatment was provided to resolve symptoms and pathology.
Figure 7.
(a) An 18–year-old female presented with a swelling and peri-apical radiolucency surrounding UL4 and a root-filled UL5. (b) Root canal treatment to UL4 was completed, with no resolution of swelling and an increase in size of the radiolucency at 1–year review. (c) Therefore, re-root canal treatment of UL5 was completed, with no further improvements at 6–months. (d) Subsequent CBCT imaging showed the presence of a large radicular cyst that was managed by enucleation and endodontic surgery.
Dose and exposure
CBCT exposes patients to an increased radiation dose compared to 2D imaging and, therefore, justification and dose optimization are imperative. A major influence of dose is the volume of tissue irradiated by the CBCT, known as the field of view (FOV). For endodontic therapy, a small FOV CBCT would typically be used to show a localized area of several adjacent teeth and their peri-apical regions.58 There is a balance between dose and image resolution/voxel size. Modern CBCT machines are capable of generating a small FOV image with as little as 4 μSv; however, for endodontics, a typical minimum exposure of 11 μSv would be expected, compared to 2D radiographs, which may range from 0.3 μSv for a single peri-apical to 21.6 μSv for multiple or 2.7–38 μSv for a panoramic radiograph.1,58 It is important to bear in mind that a single CBCT can replace multiple intra-oral radiographs in endodontic treatment; the latter could result in a greater dose overall.59 A CBCT provides a much smaller dose than a medical head CT (2000 μSv) and a similar dose to a knee radiograph.58 A low-dose protocol alters factors to reduce dose without impacting diagnostic value and may involve reducing current (mA), scan time, projection number, rotation, increasing voxel size or altering image parameters and, with developing technology, this is becoming increasingly possible. Several studies have found that employing a low-dose protocol has no impact on accuracy and outcome of detection of root fractures, external root resorption, peri-apical bone loss or measuring endodontic parameters.60,61,62,63,64,65 While radiation doses should always be kept ALARA (’as low as reasonably achievable’), there has been a shift proposed to ALADA (’as low as diagnostically acceptable’);66,67 hence, it is still important to recognize where 2D imaging does not provide sufficient diagnostic information and where CBCT may alter diagnosis and treatment planning and, in these cases, this increased exposure is justified.
Potential limitations
It is important to be aware of the limitations of CBCT and where it may not be indicated. As previously discussed in Figure 2, if the diagnostic value of 2D imaging is sufficient, and 3D imaging would not alter diagnosis or treatment planning, it is not necessary. CBCT also suffers from scatter, especially with densely radiopaque materials, such as endodontic sealer and gutta-percha. This must be taken into consideration when planning a CBCT. For example, in Figure 3, the CBCT was taken with the tooth ‘open’ following the removal of the temporary restoration in order to maximize diagnostic yield. In the UK, the Health Protection Agency requires dentists prescribing CBCT scans to have undertaken additional ‘Core training in CBCT’. Cost implications may be a concern, but CBCT is becoming increasingly economically viable and costs significantly less than a medical CT scanner.4 A guided approach involves specialist software, additional equipment and the use of highly accurate impression materials, or ideally intra-oral scanning, all of which increase financial cost; however, we must not overlook the reduced biological cost of conserved dentine, bone and vital structures. Moreover, it is important to consider that catastrophic failure with freehand techniques, condemning a tooth to extraction, would result in greater costs for implants or other replacement options. While planning time may increase, treatment and surgery time is reduced to compensate for this.
Summary
As CBCT becomes increasingly affordable, available, accessible and appropriate in terms of dose, its benefit in endodontic diagnosis and management should be increasingly considered by the dental team because it has been shown to provide correct and accurate diagnoses to permit informed and optimal treatment planning and delivery.