Manley MC, Skelly AM, Hamilton AG. Dental treatment for people with challenging behaviour: general anaesthesia or sedation?. Br Dent J. 2000; 188:358-360 https://doi.org/10.1038/sj.bdj.4800480
McGeown D, Stapleton S, Nunn J. A cost analysis estimation of a single episode of comprehensive dental treatment under general anaesthesia for adults with disabilities. Br Dent J. 2018; 224:442-446 https://doi.org/10.1038/sj.bdj.2018.124
Armfield JM. How do we measure dental fear and what are we measuring anyway?. Oral Health Prev Dent. 2010; 8:107-115
Halai T, Naqvi A, Steel C, Koshal S. Complications of conscious sedation: causes and management. Dent Update. 2017; 44:1034-1040
British Society for Disability and Oral Health. The provision of oral health care under general anaesthesia in special care dentistry: a professional consensus statement. 2009. http://www.bsdh.org/documents/BSDH_GA_in_SCD_2009.pdf (accessed July 2021)
Venchard GR, Thomson PJ, Boys R. Improved sedation for oral surgery by combining nitrous oxide and intravenous midazolam: a randomized, controlled trial. Int J Oral Maxillofac Surg. 2006; 35:522-527 https://doi.org/10.1016/j.ijom.2005.11.003
Sivaramakrishnan G, Sridharan K. Nitrous oxide and midazolam sedation: a systematic review and meta-analysis. Anesth Prog. 2017; 64:59-65 https://doi.org/10.2344/anpr-63-03-06
Averley PA, Girdler NM, Bond S A randomised controlled trial of paediatric conscious sedation for dental treatment using intravenous midazolam combined with inhaled nitrous oxide or nitrous oxide/sevoflurane. Anaesthesia. 2004; 59:844-852 https://doi.org/10.1111/j.1365-2044.2004.03805.x
Lipp M, Dick W, Daublander M Effects of an intravenous sedation technique with simultaneous administration of nitrous oxide in dental surgical operations. Anesth Prog. 1989; 36:164-168
Milgrom P, Beirne OR, Fiset L The safety and efficacy of outpatient midazolam intravenous sedation for oral surgery with and without fentanyl. Anesth Prog. 1993; 40:57-62
An alternative sedation option for special care patients: combined inhalation sedation with nitrous oxide and oxygen and intravenous sedation with midazolam
An alternative sedation option for special care patients: combined inhalation sedation with nitrous oxide and oxygen and intravenous sedation with midazolam Stephanie Fenesan Sadie Hughes Neha Patel Dental Update 2024 48:7, 707-709.
Authors
StephanieFenesan
BDS, BSc(Hons), AKC, MSc, MSCD RCS Ed
Specialty Trainee in Special Care Dentistry, Department of Sedation and Special Care Dentistry, Guy's Dental Institute, Guys and St Thomas' NHS Foundation Trust
Specialist in Special Care Dentistry, Hertfordshire Special Care Dental Service, Hertfordshire NHS Community Trust, Hoddesdon Health Centre, Hoddesdon, Hertfordshire
This article highlights an alternative sedation technique by providing inhalation sedation with nitrous oxide and oxygen alongside intravenous sedation with midazolam as an additional option for patients within special care dentistry. Two case reports are described, as well as a short overview of the available literature on this technique and the indications, advantages and disadvantages. This technique should be considered alongside other sedation techniques. As with all treatment for which sedation is provided, each case needs to be considered on an individual basis and the most appropriate option selected following discussion with the patient.
CPD/Clinical Relevance: Although single sedation techniques provide a good level of sedation to facilitate dental treatment for the majority of patients, it is desirable to have an awareness of alternative sedation options that may be available for patients.
Article
Conscious sedation has become indispensable in the dental management of patients in special care dentistry. Special care dentistry includes the provision of dental treatment for those who are unable to accept routine dental care due to physical, intellectual, medical, emotional, sensory, mental or social impairment, or a combination of these factors.1 These factors can make it difficult for patients to accept dental treatment without additional anxiety management techniques, such as behaviour management techniques, conscious sedation or general anaesthesia (GA).
The Intercollegiate Advisory Committee for Sedation in Dentistry (IACSD) defines conscious sedation as: ‘A technique in which the use of a drug or drugs produces a state of depression of the central nervous system enabling treatment to be carried out, but during which verbal contact with the patient is maintained throughout the period of sedation. The drugs and techniques used to provide conscious sedation for dental treatment should carry a margin of safety wide enough to render loss of consciousness unlikely.’2 While this principle is applicable to most patients, it is with the caveat that for some special care patients, verbal contact might not be the primary form of communication.
Techniques widely used in the provision of conscious sedation in the UK include:
Inhalation sedation;
Transmucosal (for example, intranasal);
Oral;
Intravenous (IV).
The Scottish Dentistry Clinical Effectiveness Programme (SDCEP) guidelines ‘Conscious sedation in dentistry: dental clinical guidance’ and ‘Standards for conscious sedation in the provision of dental care’, published by IACSD, advise that each patient should be individually assessed and appropriately treatment planned according to their needs.1,3
The use of conscious sedation can obviate the need for GA with implications including risk assessment and cost. Manley et al reported that 20% of patients with a disability need a GA to receive dental treatment.4 McGeown et al carried out a cost analysis and estimated the average cost per patient to be £1914.96 for a day-stay GA case for an adult with additional needs, which presents a significant cost to the NHS.5 Irrespective of cost, for some patients, GA remains a necessary treatment option regardless of the associated rare, but serious risks. This article suggests that the following combined conscious sedation technique can be a useful alternative to GA for some patients.
Nitrous oxide
Nitrous oxide and oxygen is commonly used for conscious sedation in dentistry, particularly in paediatric dentistry. Administered via a specially designed inhalation sedation machine, it is a colourless and virtually odourless gas, with a low blood/gas solubility coefficient (0.47) and a minimum alveolar concentration (MAC) of 105%. MAC is defined as the minimum alveolar concentration of anaesthetic at 1 atmosphere (atm), which produces immobility in 50% of subjects exposed to a noxious stimulus, usually a skin incision.6 MAC decreases by approximately 6–7% every decade after the age of 20 years and so, caution should be exercised when administering nitrous oxide to elderly people.7 Inhaled nitrous oxide at concentrations of 50% have been compared to a 10-mg dose of parenteral morphine in a 70-kg adult.8
In that regard, nitrous oxide is a low potency, non-irritant, non-invasive agent with rapid induction and recovery. These properties, alongside the ability to rapidly alter the depth of sedation, and the machine's inability to deliver an oxygen concentration below 30%, ensures a wide safety margin and makes the state of unconsciousness unlikely. Since it is excreted virtually unchanged, this can be ideal for patients with kidney or liver disease, and for patients where other sedation methods might be deemed unsafe, such as those with obesity.9 It has analgesic, muscle relaxation and anxiolytic properties, which can be controlled by administering a titrated dose while maintaining communication. A high proportion of patients experience a euphoric, positive, relaxed demeanour, which is ideal for the concurrent use of semi-hypnotic suggestion.
Midazolam
Midazolam, introduced in 1983, is currently the intravenous drug of choice for dental conscious sedation. It is a rapid onset, short-acting, water soluble, high-potency benzodiazepine with no active metabolites.10 Slow titration to a recognized end point, through the small incremental administration, while assessing the patient's response, avoids oversedation. It is impossible to predict what dose is needed for any individual patient.11 If the effects of midazolam need to be reversed, then the reversal agent, flumazenil, can be used, for example in the event of a medical emergency, or if recovery is prolonged. The use of flumazenil is not a never event.
An advantage of using nitrous oxide alongside midazolam is that the level of nitrous oxide can be adjusted during the procedure to adjust the overall level of sedation experienced by the patient. Midazolam can cause a decrease in blood pressure and bradycardia, as well as respiratory depression, and additionally has no analgesic qualities.12 Using nitrous oxide alongside IV midazolam can help to combat these shortfalls, and can be advantageous because it has the added benefit of administered oxygen, as well as having anxiolytic and analgesic qualities. Additionally, administering nitrous oxide prior to midazolam can help to reduce anxiety and provide a degree of analgesia during cannulation.
The use of nitrous oxide with intravenous midazolam
Nitrous oxide is widely used for facilitating cannulation, being discontinued once the cannula is in situ. Many sedative drugs given concurrently have synergistic effects, which, while potentiating the sedation, can also potentiate the risk of respiratory depression, particularly in medically compromised individuals. Nitrous oxide used concurrently with IV midazolam has been explored for use in anxious patients, but there are no studies demonstrating the use of this combined technique with special care patients. Nitrous oxide administration on a designated dental inhalation sedation machine is always in conjunction with oxygen and it is impossible to administer a hypoxic mixture. The level of sedation is also easily altered. This makes its use with intravenous midazolam ideal for many dental treatments where the level of sedation a patient needs varies throughout the procedure. Patients like the euphoria provided by nitrous oxide and the anxiolysis afforded by the benzodiazepine. This is particularly useful in individuals where the combination of other sedatives is inappropriate, such as ASA III/IV (American Society of Anaesthesiologists classification system) patients, those with high anxiety and a susceptibility to nausea, or patients with a level of tolerance to certain drugs. From the authors' clinical experience, using this technique is an area that merits further exploration.
The combined technique facilitates a lower dose of midazolam while providing a good level of sedation, which can be beneficial for a range of patients including:
Chronic pain syndrome (individuals who are already taking high-dose benzodiazepines);
Reduced liver and/or kidney function;
Multitude of medications, such as chronic opioid use;
Decreased respiratory function;
Cerebral palsy where the euphoria of nitrous oxide and the muscle relaxant properties of midazolam creates a good sedation;
Failed IV midazolam as a single agent but where nitrous oxide was well tolerated for less invasive treatment;
Where advanced IV sedation techniques are contra-indicated, eg adverse reaction to opioids such as fentanyl;
Longer procedures where the effects of midazolam may be beneficial for the more invasive initial stages of dental treatment, but a longer sedation window is desirable, such as endodontic treatment or implant placement.
In these examples certain parts of the procedures such as canal instrumentation or temporary crowns may be tolerated during the midazolam recovery, thus using the effects of nitrous oxide sedation and decreasing the need for midazolam top ups, which may lengthen the recovery time.
Technique for administering combined nitrous oxide and intravenous midazolam
Nitrous oxide induction with increments titrated slowly to induce a state of anxiolysis and relaxation
The standard procedure for sedation with nitrous oxide is to start with 100% oxygen and then add 10% nitrous oxide for 1 minute while assessing patient response, before adding a further 10% for a further 1 minute, and then increasing the increments by 5% at 1-minute intervals until the patient appears relaxed.
Cannulation and intravenous midazolam administration titrated to the patient's sedation end point
The standard titration procedure for midazolam is to start with 2 mg midazolam over 30 seconds and then wait 90 seconds while assessing the patient's response, and then administer further increments of 1 mg every 30 seconds until the desired sedation end point is observed, while maintaining verbal contact with the patient, or appropriate patient interaction if the patient is non-verbal, such as in the case of some patients seen within special care dentistry. This regimen should be adjusted accordingly in response to individual patient factors – patient age, presence of comorbidities or multiple medications.
Throughout the treatment nitrous oxide can be increased or decreased as required.
At the end of the procedure
At the end of the procedure, after ceasing nitrous oxide administration, a minimum of 2 minutes of 100% oxygen should be administered. This is to prevent diffusion hypoxia, although in most healthy individuals this is a theoretical risk, and to decrease pollution in the immediate area.
Case studies
Case A
A 24-year-old male student attended the Hertfordshire Special Care Dental Service (HSCDS) for a new patient assessment. He complained of pain in the upper right and left quadrants. Medically, a diagnosis of autistic spectrum condition (ASC), dyspraxia, anxiety and depression was noted, with sertraline taken for the latter.
Access to dental treatment in his university town proved challenging due to the patient's high anxiety and the lack of understanding towards his condition by the dental practitioners he visited. This prompted the patient to return to his family home to access dental treatment, and a referral by the family GDP was made to a general sedation clinic. Owing to his medical history, this referral was redirected to the HSCDS.
At the initial assessment appointment within the HSCDS, despite his high anxiety, an examination and radiographs were completed. Dietary analysis revealed a highly cariogenic diet with the patient drinking fizzy drinks and grazing on food with a high sugar content throughout the day. He reported brushing twice daily with an electric toothbrush and fluoride toothpaste.
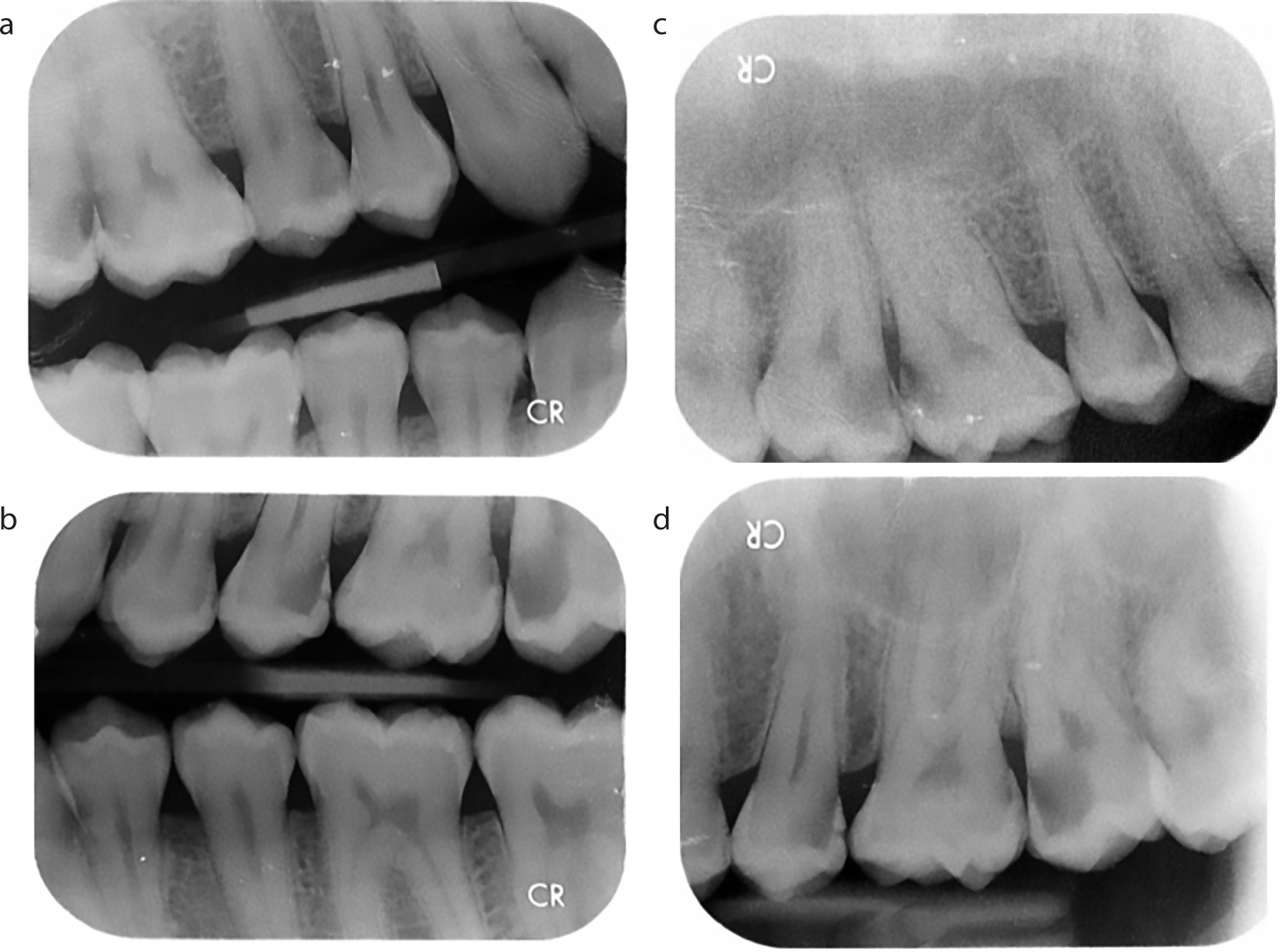
Extra-oral examination was normal. Intra-oral examination revealed poor oral hygiene with generalized plaque associated gingival inflammation, and the presence of caries, which was confirmed radiographically (Figure 1). Gross caries was present in the UR5–7, and UL4–7, which all responded positively to thermal vitality testing.
Figure 1. (a–d) Case A: pre-operative radiographs.
Following discussions about treatment and anxiety management options, treatment was planned under intravenous sedation to help reduce his anxiety and allow acceptance of dental treatment. The treatment plan consisted of preventive advice and oral health education and the restoration of UR5–7 and UL4–7 with the adjunct of intravenous sedation. Treatment was staged over five appointments. Preventative advice was provided on the use of a high-fluoride toothpaste (5000ppm), along with dietary analysis, dietary and oral hygiene advice.
Visit
Treatment
Sedation
Outcome
Visit 1
Restore UL5,7
Intravenous sedation
Poor response at end of sedation and prolonged recovery
Visit 2
Restore UR5–7
Combined intravenous sedation and inhalation sedation
Good outcome
Visit 3
Restore UL4,6 and place definitive restoration UL7
Combined intravenous sedation and inhalation sedation
Good outcome
Visit 4
Supragingival ultrasonic scale
Inhalation sedation
Good outcome
Visit 5
Definitive restoration UL5
Inhalation sedation
Good outcome
On the first treatment appointment, IV sedation was administered and 4 mg of midazolam was titrated to the patient's response, maintaining verbal contact throughout the procedure. He initially sedated well during treatment where UL5 and UL7 were treated and stabilized with Biodentine (Septodont, France). Towards the end of the treatment, and as the effects of the midazolam lessened, the patient became agitated, upset and distressed and an escalation in challenging behaviour was observed. Behaviour management techniques were used during the recovery period to de-escalate the negative emotional response and attempt to keep the patient as calm as possible. However, a gross hypersensitivity to the environment, light and sounds was observed, particularly the high-pitched noise made by the washer-disinfector in an adjacent room, which exacerbated his distress. This led to an increased time in recovery as the patient was tearful, distressed and unable to leave the building for a prolonged period following the discontinuation of the invasive treatment phase.
Following this appointment, it was discussed whether it would be appropriate to continue treatment with intravenous sedation due to the patient's response. An alternative technique combining IV sedation with midazolam alongside inhalation sedation with oxygen and nitrous oxide was discussed as an appropriate option.
On the second treatment appointment, a combined sedation approach was used. Inhalation sedation with nitrous oxide and oxygen was initiated and titrated to response, with 30% nitrous oxide administered via a Porter MXR 3000 (Parker Hannifin Corporation, USA) flow meter alongside the use of active scavenging equipment. The patient was observed to be calm and relaxed at this point. Successful cannulation was followed by the administration of IV midazolam, titrated to 2 mg, in line with the patient's response, and while maintaining verbal contact throughout the procedure. The patient responded very well to the combined technique, with successful treatment of UR5,6, with recovery being smoother, more gradual and, therefore, pleasant for the patient. This was a successful appointment and it was agreed with the patient to continue to use this method to complete the remainder of their dental treatment. Two further appointments were needed to successfully complete restorations on UR7 and UL4,6 using the combined technique.
The patient became acclimatized to having dental treatment and felt less anxious. At the penultimate appointment, he felt confident enough to trial having a supragingival scale using inhalation sedation with oxygen and nitrous oxide alone. Following the success of this appointment and after discussion, the patient felt confident to have the final treatment, which included occlusal reduction of Biodentine and placement of definitive composite restoration on UL5. This was successfully carried out by titrating the level of nitrous oxide to 30%, in line with the patient response.
Case B
A 38-year-old female patient attended for a routine check-up complaining of a fractured tooth in the lower right quadrant. Medically, she had cerebral palsy with left-sided hemiplegia and associated dystonia affecting her left arm, a mild learning disability and was medicated with baclofen, cetirizine and trihephenidyl. Also reported were an allergy to codeine and an adverse reaction to tramadol. The patient lived independently with limited support, and was supported by her mother for her dental appointments.
She presented with a heavily restored dentition and a high caries rate. Preventive advice was given, which included oral hygiene advice, use of a high-fluoride toothpaste and dietary analysis and advice. Her oral hygiene and diet have improved, but are not yet at an optimal level.
After discussion of treatment options, it was decided to attempt IV sedation with midazolam and although initially, the patient appeared well sedated, she had a very short treatment window and her involuntary movements increased when active treatment was attempted. Further midazolam was titrated; however, this was not helpful in reducing her involuntary movements, which continued. As such, it was very difficult to safely and effectively continue treatment.
Further treatment options were discussed, which included the option of GA; however, owing to her high caries rate, treatment would have needed to be more radical to avoid repeat GA sessions. The patient was informed that posterior teeth, which may have been suitable for endodontic treatment under sedation would be extracted, in addition to those with a poor/guarded prognosis in accordance to local policy and as per BSDH guidelines.13 The patient was keen to try and keep as many teeth as possible and on this basis, avoid a GA. Sedation with midazolam and fentanyl was not appropriate because of the patient's previous adverse reaction to opiates. It was decided to try combined inhalation sedation with nitrous oxide and IV sedation with midazolam, alongside behaviour management techniques.
In the subsequent appointment using the combined technique; nitrous oxide was administered first and titrated to 45/55% nitrous oxide/oxygen followed by IV midazolam titrated to 3 mg, in conjunction with behaviour management techniques. This combined technique was helpful in reducing involuntary movements and lengthening the treatment window allowing treatment. Using this combined method, the patient was able to avoid GA and undergo more conservative treatment, including endodontic treatment, which would not have been viable under GA because of day-case anaesthesia time constraints.
Discussion
The combined technique is useful as an additional sedation tool for patients for whom basic single sedation techniques have not been successful. However, there is limited discussion of this method available in the literature.
Venchard et al carried out a prospective randomized controlled trial in an oral surgery setting comparing sedation with inhaled nitrous oxide, IV midazolam and the combined technique with nitrous oxide and midazolam.14 They found a significant reduction in the amount of midazolam administered and a reduction in recovery time with the combined technique when compared to using the single agents. It was also found that the operating conditions were improved with the combined technique, and the mean lowest oxygen saturation recorded was higher with the combined technique.
A meta-analysis that examined studies that compared the combined use of nitrous oxide and midazolam sedation with their individual use found only four studies that met their inclusion criteria, while only three met their inclusion criteria for quantitative meta-analysis.15 Of the four studies systematically reviewed, two looked at adults and two at children. All four assessed patient cooperation between single agent and combination sedation techniques. They found no statistically significant reduction in cooperation scores overall. Additionally, there was no significant difference between adult and child cooperation. However, Averley et al and Venchard et al found the total dose of midazolam administered was significantly less in the combined group.14,16 Consequently, the recovery time was found to be less because of the lower doses of midazolam.
Lipp et al investigated the use of IV midazolam and pentazocine with the additional administration of nitrous oxide and found that the combined technique was regarded as the best technique by patients, resulting in a reduction in anxiety and lower pain scores. However, nitrous oxide was administered after the administration of IV midazolam.17 The benefits of nitrous oxide were still delivered for the duration of treatment, but there would have been no anxiolytic effects at the beginning during cannulation. Furthermore, the nitrous oxide benefits can only be seen after the midazolam sedation end point had been reached, potentially resulting in oversedation.
Following the systematic review, Sivaramakrishnana and Sridharan recommended: ‘the use of the nitrous oxide–midazolam combination technique rather than the individual use of either drug due to the advantage of reducing the total dose of midazolam used’.15 It can be argued that if a lower dose of midazolam is used, safety can be increased, and this complies with the principle of giving the minimum amount of drug necessary to achieve the desired effect.2
Critically, all patients included in these studies were ASA I and ASA II. Clinicians must be vigilant, especially when combined sedation techniques are used, to ensure that underlying medical issues and comorbidities are not exacerbated because of the sedation. Monitoring the patient's respiratory status is paramount, particularly as there is a risk that the additional oxygen administered could mask initial respiratory depression. The IACSD standards state that: ‘no one technique is suitable for all patients. However, adopting the principle of minimum intervention, the simplest and safest technique that is likely to be effective, based on robust patient assessment and clinical need, should be used’.2 It might be argued that the technique described can fulfil this aim more effectively than other more commonly used multidrug techniques.
In addition to the advantages discussed, a further benefit of this particular technique is that, for most sedation clinics, no extra equipment is needed.
A more commonly used combined technique is IV midazolam with fentanyl. In the authors' experience, patients have responded more favourably with combined nitrous oxide and IV midazolam rather than fentanyl and midazolam. Fentanyl often causes nausea and longer-lasting unwanted effects compared to the pleasant euphoric feeling of nitrous oxide; however, it has been shown that there are benefits of opioid use in sedation.18 Future studies to compare the use of fentanyl or nitrous oxide as an adjunct to IV midazolam would be useful.
Environmental impact of nitrous oxide
Increasingly, the medical profession is required to justify the sustainability of the equipment and resources used. Nitrous oxide is extremely stable with an atmospheric lifetime of 100–150 years. It is degraded by ultraviolet radiation, producing nitrogen oxide as a by-product which, by means of various chain reactions, destroys ozone. Nitrous oxide is used commercially as a propellant in food aerosols, it is produced during the combustion of fossil fuels, found in nitrogen-containing fertilizers, and used as an anaesthetic and sedative agent.
Owing to its ability to reflect heat energy back to the surface of the earth, nitrous oxide is labelled a greenhouse gas. Maskell et al stated that nitrous oxide contributes to the greenhouse effect by approximately 6%; however, it has been estimated that only 1% of this is due to anaesthetic use.19,20
Training needs
Although there is no evidence to show that this combined technique causes a higher risk of respiratory depression, multidrug techniques are for experienced sedationists. Multidrug sedation is categorized as an advanced technique in the UK.2,3 There is no specific mention in existing documentation or guidance in the UK of nitrous oxide with oxygen and IV midazolam being administered as a combined technique, or whether this is specifically an ‘advanced’ or ‘basic’ sedation technique. However, sedationists wishing to use it should be experienced and skilled in using both techniques as single agents before attempting to use them concurrently. As this technique is not well recognized in the UK or routinely taught on sedation courses, there is no minimum recommended number of supervised cases stipulated in contemporaneous sedation guidance documentation. However, in an environment where treating individuals with comorbidities or additional needs, it would be prudent to undertake supervised cases initially. This is an area that needs further clarification and local policies may need to be revised and updated to reflect this if clinicians intend to use this combined technique.
Conclusion
In theory, nitrous oxide with IV midazolam for dental conscious sedation could be one of the most accessible and safe combined techniques for experienced sedationists to learn, when compared to other advanced techniques.
Any current single sedation technique will have limitations and, undoubtedly, as with all sedation cases, patient selection is key. Although single-agent techniques provide a good level of sedation to facilitate dental treatment for the majority of patients, they do not provide adequate sedation for all. When single-agent sedation has failed, GA is often considered the only other available treatment option. For a minority of patients, combined techniques offer a safe, effective alternative and should be included in the experienced sedationist's armamentarium. As medicine evolves, our anxiety management techniques and options should also. These case studies illustrate patients for whom GA or IV midazolam alone would not have been in their best interests, and it is important that alternative techniques are studied to prove their efficacy.