Andreasson JO. The impacted premolar. In: Andreasen JO, Petersen JK, Laskin DM (eds). Copenhagen: Munksgaard; 1997
Burch J, Ngan P, Hackman A. Diagnosis and treatment planning for unerupted premolars. Pediatr Dent. 1994; 16:89-95
Jain U, Kallury A. Conservative management of mandibular second premolar impaction. J Sci Res. 2011; 4:59-61
Frank CA. Treatment options for impacted teeth. J Am Dent Assoc. 2000; 131:623-632
Berkovitz BKB, Holland GR, Moxham BJ. Oral Anatomy, Histology and Embryology, 4th edn. : Mosby; 2009
Khalaf K, Miskelly J, Voge E, Macfarlane TV. Prevalence of hypodontia and associated factors: a systematic review and meta-analysis. J Orthod. 2014; 41:299-316
Arai Y, Tammisalo E, Iwai K Development of a compact computed tomographic apparatus for dental use. Dentomaxillofac Radiol. 1999; 28:245-248
Arikan V, Kizilci E, Ozalp N, Ozcelik B. Effects of fixed and removable space maintainers on plaque accumulation, periodontal health, candidal and Enterococcus faecalis carriage. Med Princ Pract. 2015; 24:311-317
Bjerklin K, Bennett J. The long-term survival of lower second primary molars in subjects with agenesis of the premolars. Eur J Orthod. 2000; 22:245-255
Parkin N, Benson PE, Thind B Open versus closed surgical exposure of canine teeth that are displaced in the roof of the mouth. Cochrane Database Syst Rev. 2017; 8 https://doi.org/10.1002/14651858.CD006966.pub3
Tolstunov L. Implant zones of the jaws: implant location and related success rate. J Oral Implantol. 2007; 33:211-220
Jambi S, Walsh T, Sandler J Reinforcement of anchorage during orthodontic brace treatment with implants or other surgical methods. Cochrane Database Syst Rev. 2014; 2014 https://doi.org/10.1002/14651858.CD005098.pub3
Patel S, Fanshawe T, Bister D, Cobourne M. Survival and success of maxillary canine autotransplantation: a retrospective investigation. Eur J Orthod. 2010; 33:298-304
Czochrowska EM, Stenvik A, Bjercke B, Zachrisson BU. Outcome of tooth transplantation: survival and success rates 17–41 years posttreatment. Am J Orthod. 2002; 121:110-119
Slagsvold O, Bjercke B. Autotransplantation of premolars with partly formed roots: a radiographic study of root growth. Am J Orthod. 1974; 66:355-366
Stange KM, Lindsten R, Bjerklin K. Autotransplantation of premolars to the maxillary incisor region: a long-term follow-up of 12–22 years. Eur J Orthod. 2015; 38:508-515
Second premolars are the third most likely teeth to be affected by impaction after third molar and maxillary canine teeth. Although the presence of an impacted second premolar is relatively common, and is a situation that often presents to general dentists in practice, there is relatively little published regarding this topic. Knowledge of this condition is essential for all those involved with the management of these cases. This article explores the aetiology, assessment and treatment options available to manage this condition, using examples from cases treated within our department.
CPD/Clinical Relevance: An understanding of the aetiology, assessment and various treatment options available to manage impacted second premolars will inform better treatment planning.
Article
Othman Hameed
An impacted tooth is one that is prevented from erupting in its normal functional position by bone, other teeth or fibrous tissue.1 Premolars are the third most likely teeth to be affected by impaction after third molar and maxillary canine teeth.2 The incidence of impaction among premolars is thought to be around 0.5%. Among premolars, mandibular second premolars are thought to have the highest prevalence of impaction, comprising almost a quarter of all impactions, excluding third molars.3,4 The precise aetiology of this condition is often unknown; however, a number of local and systemic factors have been associated with unerupted second premolars (Table 1).
Arch length deficiency
Premature loss of primary teeth
Retained primary teeth
Supernumerary teeth
Local pathology (cysts and neoplasms)
Hyperplastic gingival tissue
Early loss of the first permanent molar
Trauma
Ectopic position of dental follicle
Systemic factors
This paper explores the aetiology, assessment and treatment options available to manage this condition, using examples to highlight the management of unerupted second premolars.
Assessment
Maxillary second premolars typically erupt between the ages of 10 and 12, and mandibular second premolars normally erupt between the ages of 11 and 12.5 Although these tooth eruption timings are approximate, with variations of 6 months either way not being unusual, an unerupted tooth beyond the date of expected eruption should be met with suspicion of impaction, or developmental absence, as should failure of a tooth to erupt within 6 months of the same tooth on the opposite side. This is especially the case for unerupted mandibular second premolars, which are the most likely teeth to be developmentally absent, apart from the third molar teeth.6
In addition to a detailed verbal history and clinical examination, appropriate radiographic imaging is often necessary. An unerupted premolar is usually detected from a routine bite-wing radiograph, with its presence or absence generally confirmed by a panoramic radiograph. The precise location of an unerupted second premolar tooth needs to be ascertained, often requiring cone beam computed tomography (CBCT). The need for a CBCT must be balanced against increased radiation dosage; however, field limitation can help to significantly reduce the effective radiation dose (Figure 1).7 Once the presence and position of the unerupted second premolar has been confirmed, several treatment options can be explored to manage this condition:
Figure 1. (a) An OPG showing multiple supernumeraries. (b) 3D views of a CBCT scan taken of the same patient to determine the precise location of the supernumeraries.
No treatment
Symptomless, unerupted second premolars may be left in situ. This can be appropriate for grossly displaced teeth or those that are closely related to adjacent teeth or vital structures. For example, markedly displaced maxillary second premolars can lie in close proximity to the maxillary sinus, with mandibular second premolars often intimate with the inferior dental nerve (Figure 2). It is important to remember that teeth left in situ should be periodically monitored radiographically to assess for any potential adverse changes, such as deterioration in position, root resorption of adjacent teeth, or follicular enlargement and cystic formation.
Figure 2. An OPG showing a submerged LRE that has resulted in impaction of the LR5. Due to the intimate relationship of the LR5 with the inferior alveolar nerve, removal of this tooth may lead to unavoidable damage to this nerve, and consequential loss or altered sensation from the lip, chin, cheek, gums and tongue.
Interceptive treatment
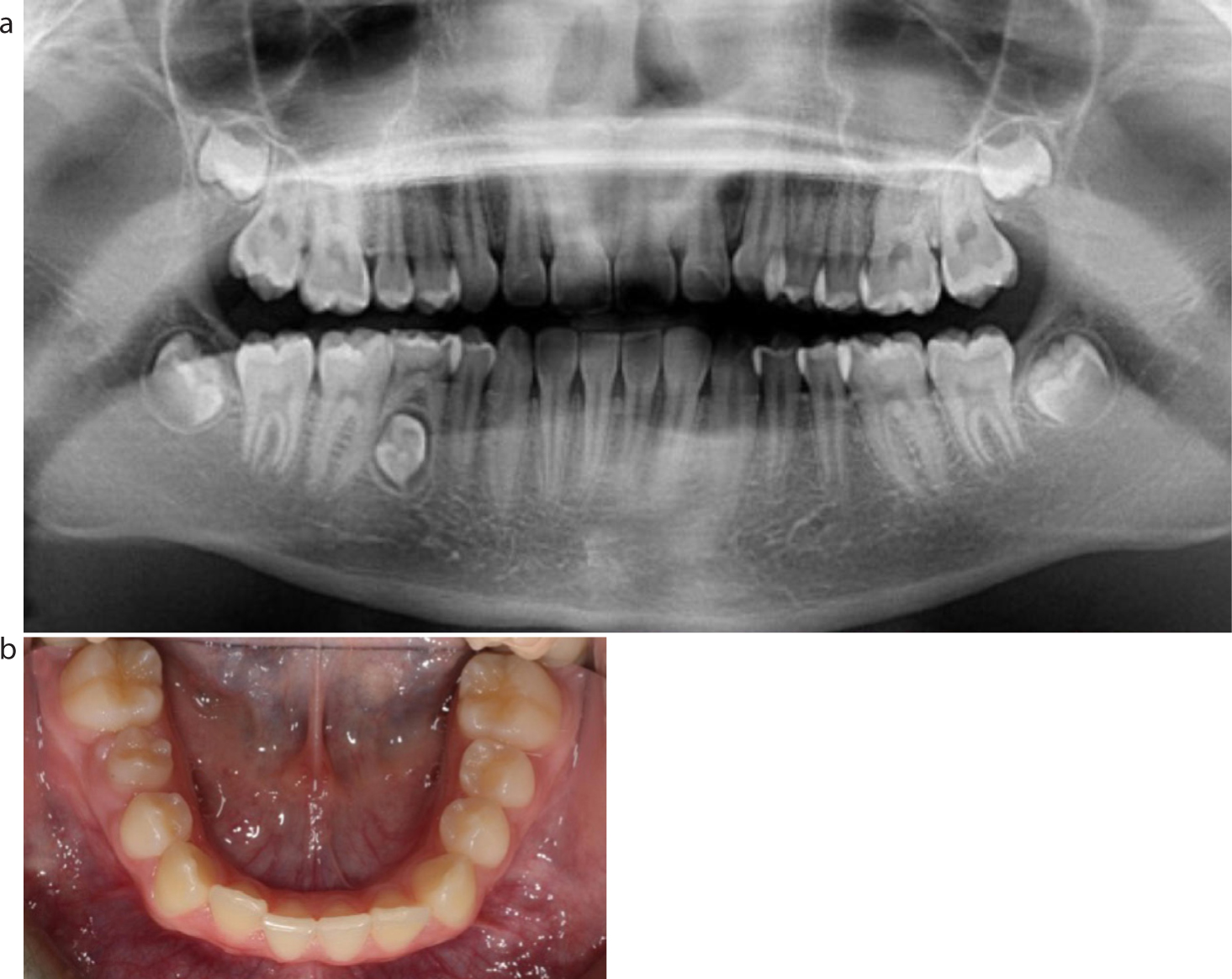
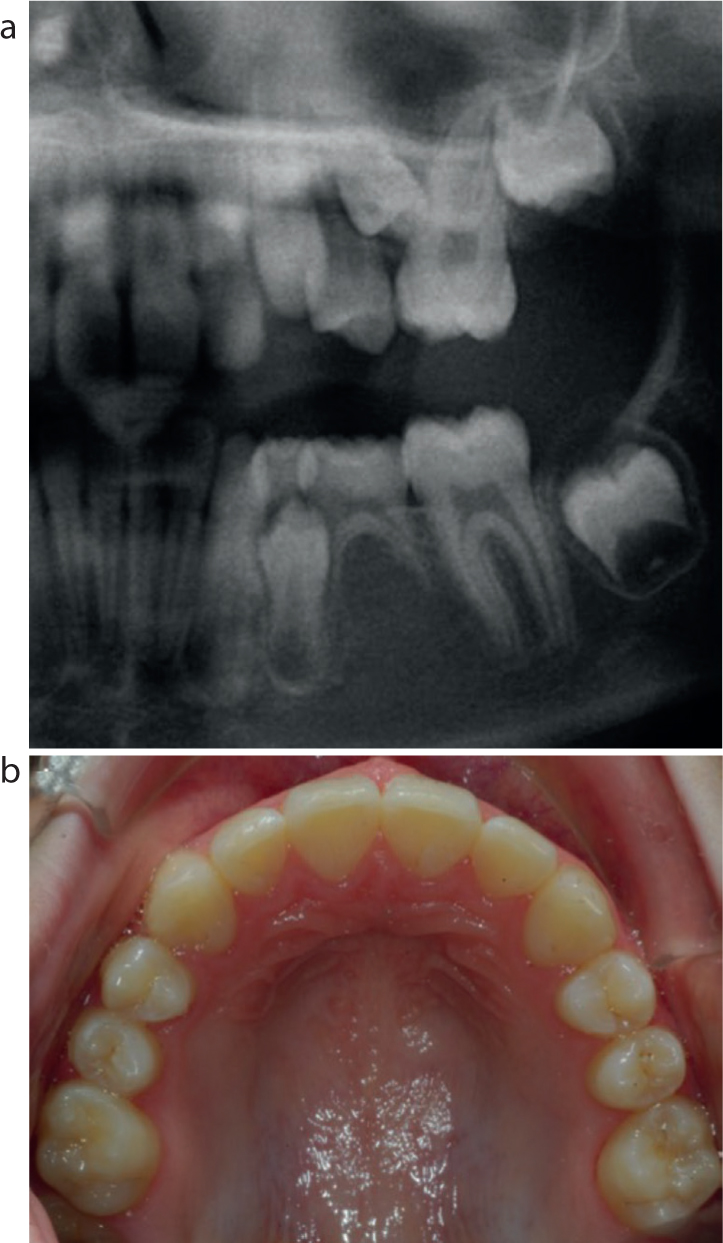
Quite often, a conservative approach with removal of the retained second primary molar tooth can lead to successful eruption of an unerupted second premolar (Figures 3–5). Equally, if a retained second primary molar is not interceptively extracted, further deterioration in the position of an unerupted second premolar may ensue (Figure 6). If space availability is an issue, or there are concerns the adjacent teeth may tip into the extraction site, space maintenance by means of a removable or fixed appliance could be considered following removal of the overlying primary tooth. However, the negative effects space maintainers can have upon periodontal health must be considered prior to their use.8
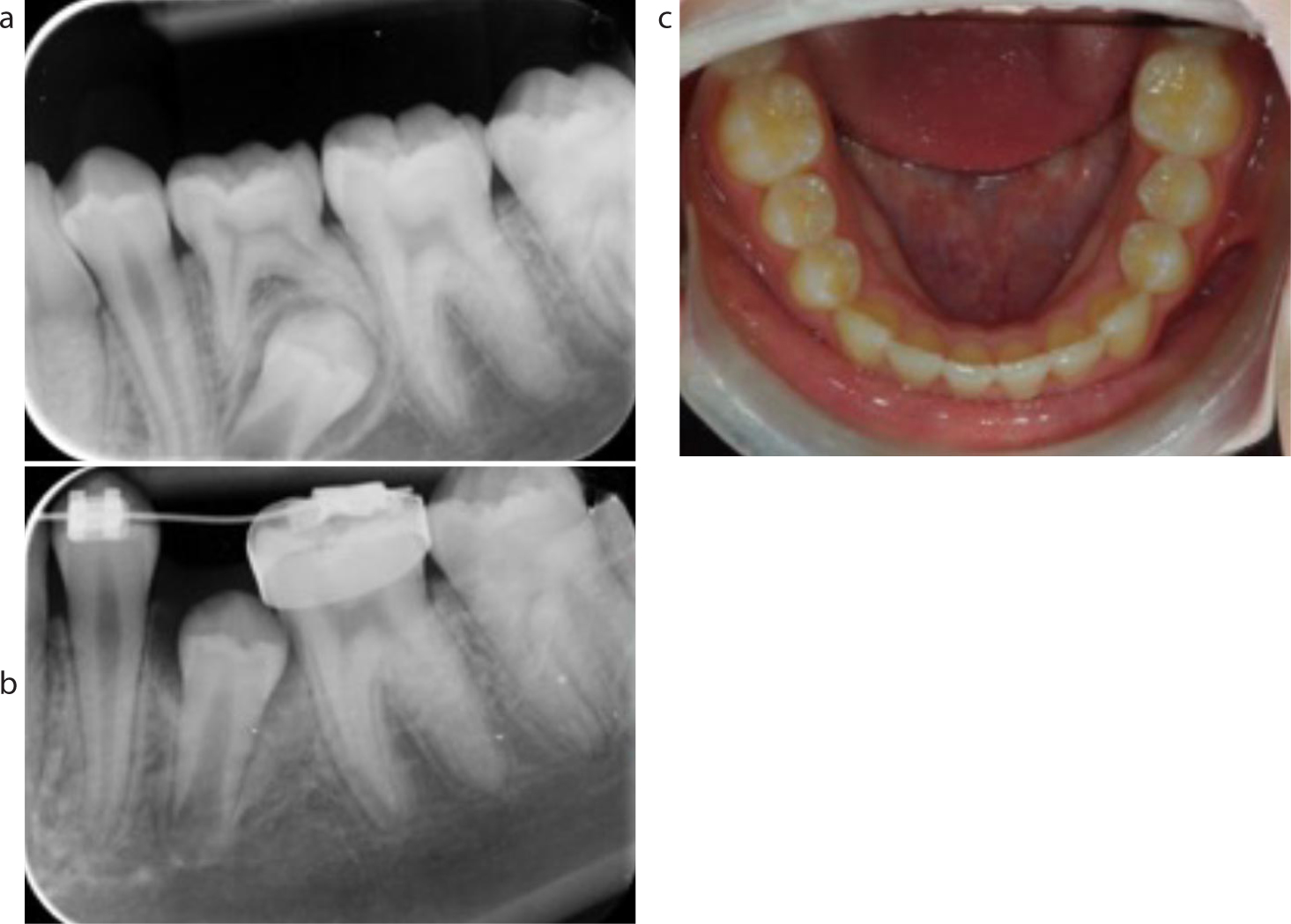
Figure 3. (a) An OPG of a 14-year-old female patient with a retained LRE and an impacted LR5. (b) A photograph taken 12 months following interceptive removal of the retained LRE. Note how the LR5 has successfully erupted without the need for any active intervention.Figure 4. (a) Peri-apical radiograph of a patient with a retained LLE and an impacted LL5. (b) Peri-apical radiograph taken 12 months following interceptive removal of the retained LLE showing improvement in the position of the LL5. (c) Debond photograph showing successful alignment of the LL5 without the need for surgical intervention.Figure 5. (a) An OPG of an 11-year-old female patient with a retained LRE and an impacted LR5. (b) An OPG taken 12 months following interceptive removal of the retained LRE showing improvement in the position of the LR5. (c) Mid-treatment photograph showing a method of orthodontic alignment being applied to the now present LR5.Figure 6. An OPG of a 17-year-old patient who had been referred by their local dentist due to an impacted LL5. If the retained LLE had been removed at an earlier stage, the degree of impaction of the LL5 may well have been less severe.
Although this approach can require patience, it is important to remember that if the retained primary tooth is removed in the mixed dentition, and the second premolar fails to improve in position after a period of review, more comprehensive fixed appliance treatment can still be provided for the patient in their early teenage years.
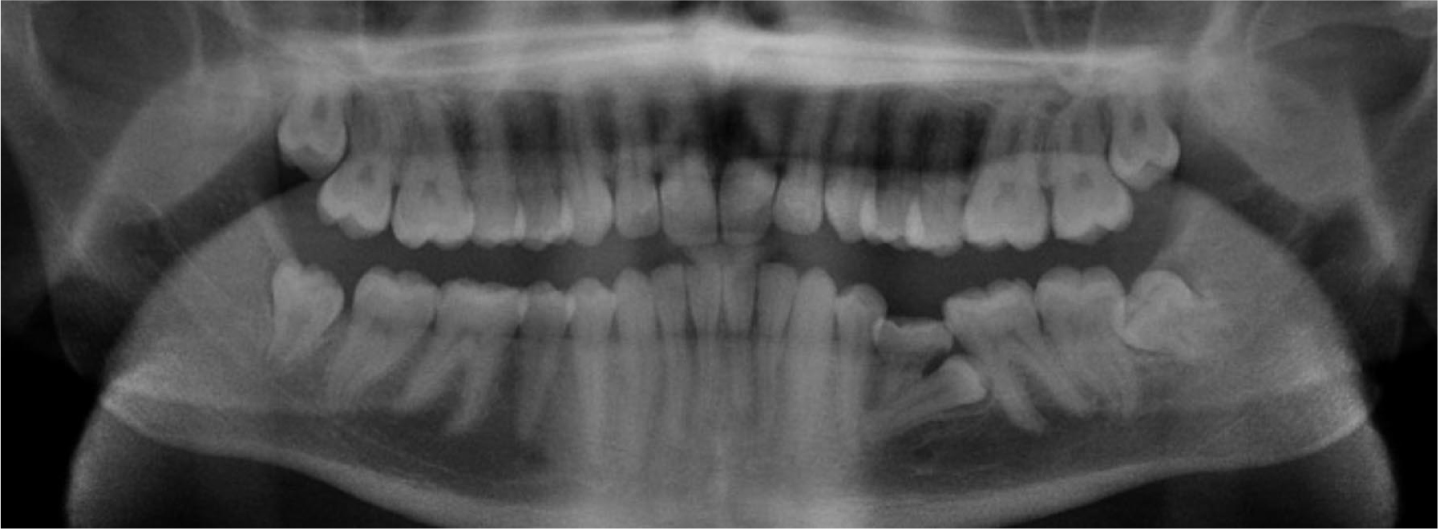
Similarly, the presence of a supernumerary tooth or odontome can also act as a physical obstruction preventing eruption of a second premolar tooth (Figure 7). Removal of the supernumerary element can often result in spontaneous eruption of the impacted second premolar tooth, provided there is sufficient space and eruptive potential.
Figure 7. An OPG showing multiple supplemental supernumeraries in the mandibular premolar regions.
Surgical removal
Patients may choose to undertake surgical removal of the unerupted second premolar tooth. Alternatively, the clinician may request its removal when orthodontic tooth movement is planned because leaving the tooth in position may limit alignment of the adjacent teeth. However, many factors influence this decision:
The degree of displacement of the tooth;
Proximity to vital structures including the maxillary sinus and inferior alveolar nerve;
Favourable long-term prognosis of the second primary molar tooth;
The existing malocclusion and amount of crowding present within the arch;
Pre-existing pathology including infection, cyst, or a tumour relating to the unerupted tooth;
Patient attitude to orthodontic treatment.
If the decision is made to remove the second premolar tooth and maintain the second primary molar tooth, the patient must be advised that, although the retained primary tooth can have a good long-term prognosis, it may be lost in the future.9 At this stage, the edentulous space would have to be accepted or restored prosthetically. Alternatively, the space could be closed orthodontically. This is often not straightforward because the space that remains following the loss of a second primary molar tooth is often large. As a result, excessive retroclination of the incisors or the need for temporary anchorage devices to aid posterior teeth protraction is often required when attempting to close these spaces orthodontically.
Exposure and orthodontic alignment
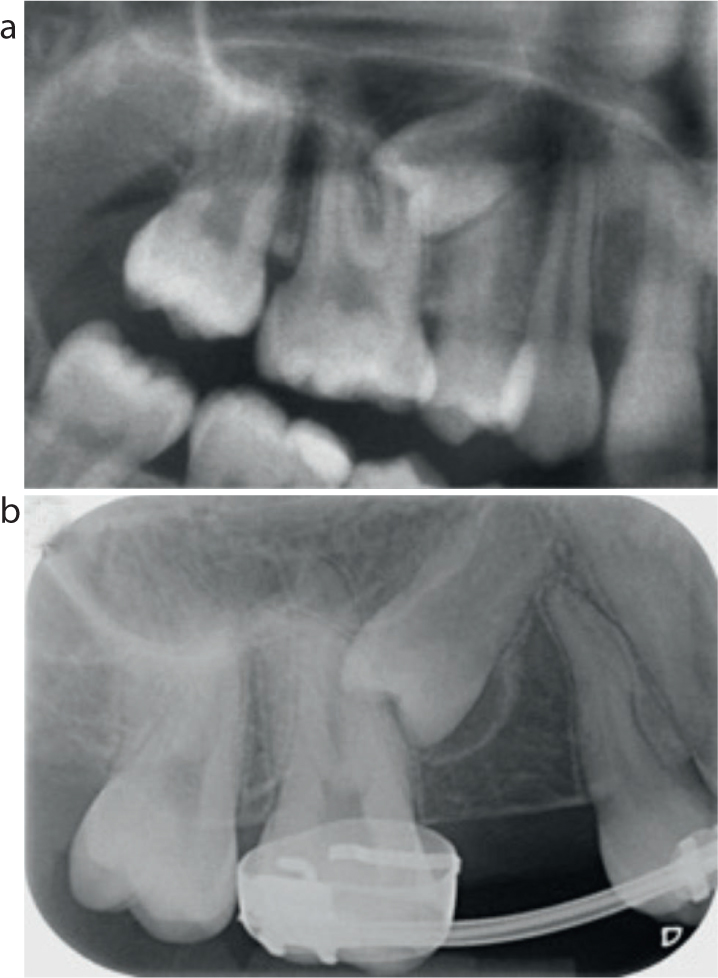
Although exposure and orthodontic alignment is the lengthiest in terms of treatment time, it can also produce the best functional and aesthetic results if undertaken successfully. This option is preferable in cases with severe hypodontia, indicating preservation of all viable teeth that are present. Prior to the surgical procedure, space creation can be undertaken with fixed appliances and the use of ‘push–pull’ mechanics. On occasions, this may lead to spontaneous eruption of the impacted second premolar tooth eliminating the need for surgical intervention (Figure 8); however, space creation alone does not always guarantee spontaneous eruption (Figure 9).
Figure 8. (a) Pre-treatment OPG showing an impacted UL5 between the UL4 and UL6. (b) Post debond photograph taken of the same patient. The UL5 erupted spontaneously, without the need for surgical intervention, following space creation with orthodontic appliances.Figure 9. (a) Pre-treatment OPG showing an impacted UR5 between the UR4 and UR6. (b) Peri-apical radiograph taken following space creation with fixed appliances. Despite there being sufficient space available to allow for spontaneous eruption of the UR5, the tooth only marginally improved in position over 12 months. The patient declined surgical exposure and bonding.
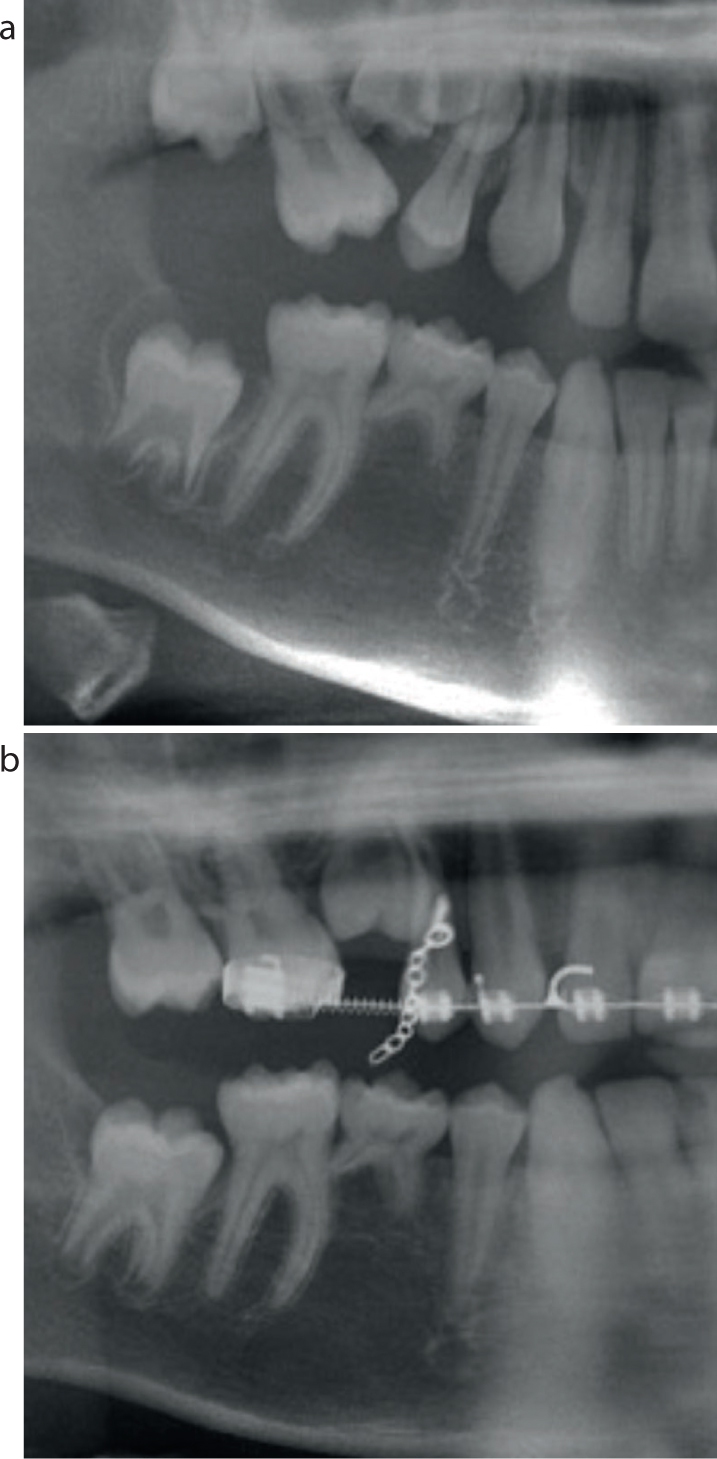
The chosen method of surgical exposure varies depending on the position of the unerupted tooth and the individual preference of the clinician, with the literature showing little difference between the available techniques in relation to treatment duration and periodontal health (Figure 10).10
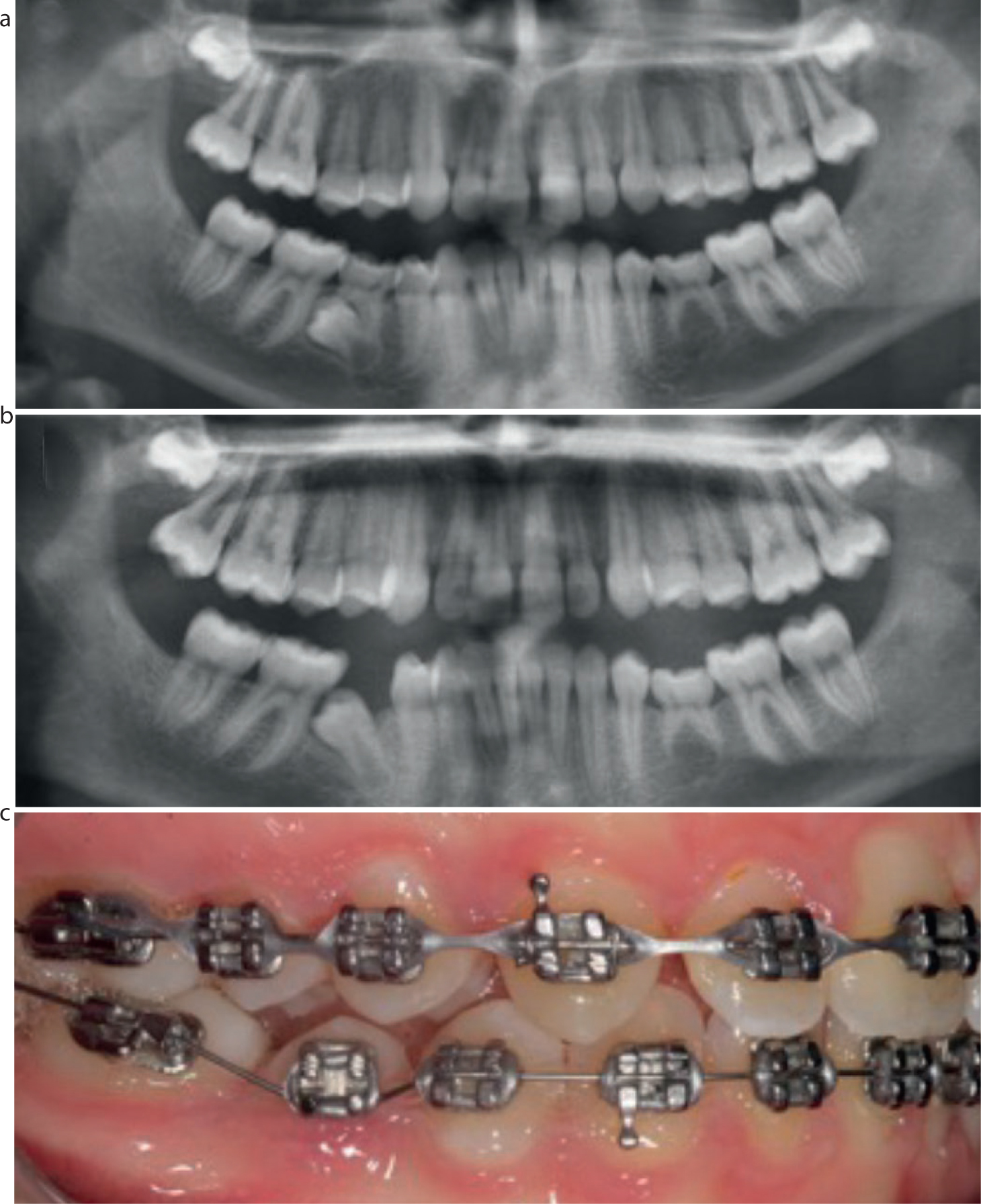
Figure 10. (a) Pre-treatment OPG showing an impacted UR5 associated with supernumeraries. Note how the UR4 and UR6 have tipped into the edentulous space. (b) Mid-treatment OPG following removal of the supernumeraries and an expose and bond procedure for the UR5. Note how fixed appliance therapy has been used to upright the UR4 and UR6 in order to recreate space for the unerupted UR5.
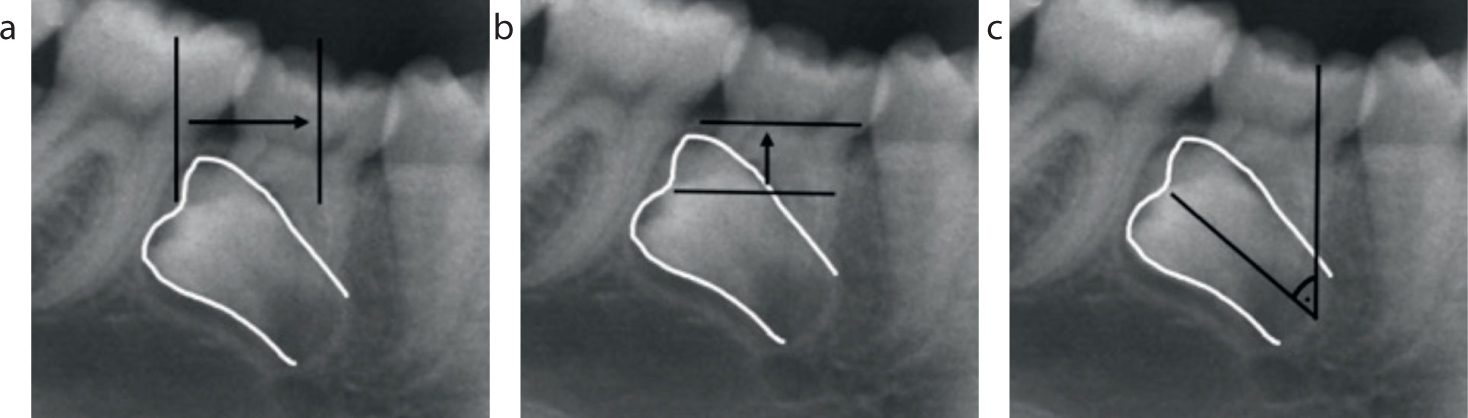
There are various orthodontic techniques available to bring the premolar into occlusion following the operation, almost all of which require comprehensive fixed-appliance therapy under the care of a suitably trained orthodontist (Figure 11). Treatment times are generally increased when premolars are more horizontally and/or vertically displaced, or have an increased crown angulation (Figure 12). In addition, the success rate of orthodontic traction to displaced teeth is reduced in older patients due to their reduced eruptive potential, therefore, identification of impaction at an early stage is extremely important. Furthermore, the alignment of mandibular premolars can often be more challenging and anchorage-demanding than that of maxillary premolars owing to the greater relative mandibular bone density.11
Figure 11. (a) Peri-apical radiograph of a patient with a retained LLE and an impacted LL5. (b) Peri-apical radiograph taken 12 months following interceptive removal of the retained LLE showing little improvement in the position of the LL5. (c) Mid-treatment photograph showing orthodontic traction being applied to the LL5 following an expose and bond procedure for the impacted tooth. (d) Mid-treatment photograph showing orthodontic traction being applied to the partially erupted LL5. (e) Mid-treatment photograph showing the newly erupted LL5.Figure 12. Assessment of the prognosis for second premolar alignment (a) Horizontal position – the further the position of the premolar crown from the intended anteroposterior position, the poorer the prognosis. (b) Vertical position – the further the position of the premolar crown from the crestal bone, the poorer the prognosis. (c) Angulation – the greater the angulation of the long axis of the premolar in relationship to a vertical line, the poorer the prognosis.
Orthodontic auxiliaries, such as a transpalatal or lingual arch, in addition to modern advances in technology, such as temporary anchorage devices, have helped reduce the effects of anchorage loss, resulting in outcomes that were previously not possible.12 However, there are still instances, in particular with grossly ectopic second premolars, where the unerupted teeth may be in highly unfavourable positions for orthodontic alignment.
Autotransplantation
Autotransplantation involves removal of a tooth and subsequent implantation into a different position within the alveolus of the same person. Space will be needed in order to accommodate this tooth, and it is often created prior to the operation with a short course of orthodontic treatment.
Although autotransplantation has benefits, including a reduced treatment time compared with aligning the tooth with orthodontic traction, this method is very technique-sensitive and is rarely undertaken. Studies have shown autotransplanted teeth to have poorer long-term prognosis owing to increased susceptibility to ankylosis and external root resorption.13 However, if successful, a transplanted tooth in a child can provide a functional unit, and preserve alveolar bone until definitive replacement with an implant-retained prosthesis is an option.
A clinical indication for autotransplantation frequently demonstrated in the literature is when a premolar is autotransplanted into the maxillary incisor region following traumatic loss or developmental absence. This method has certain benefits over prosthetic replacement because it can lead to bone induction, re-establishment of a normal alveolar process following traumatic bone loss, and does not involve neighbouring teeth.14 However, most successful cases involve undertaking the procedure prior to complete root formation, in addition to restorative camouflage of the transplanted premolar with selective grinding and composite build-up, or restoration with a crown to restore the ‘normal’ incisor morphology.15 For these reasons, although the perceived oral health status and prognosis of autotransplanted premolars to the maxillary incisor region has been shown to be favourable, the aesthetic outcome is often more uncertain.16
More rarely, in cases with severe hypodontia, autotransplantation can be undertaken to treat long edentulous spans using teeth from unaffected quadrants (Figure 13).
Figure 13. (a) An OPG of a patient with absent adult teeth in the upper right quadrant (b) An OPG of the same patient following autotransplantation of the LR5 and LL5 into the upper right quadrant. (c) Post-surgical photograph showing the recently autotransplanted LR5 and LL5 in the upper right quadrant. (d) Peri-apical radiograph of the autotransplanted LR5 and LL5 showing good bone support and no signs of peri-apical pathology. (e) Mid-treatment photograph showing the autotransplanted LR5 and LL5 in place of the absent UR4 and UR5.
Conclusion
Successful management of impacted second premolars is important for both functional and aesthetic purposes. Unerupted second premolars can present with many variations resulting in the management of this condition being heavily case-dependent. Management ranges from being relatively straightforward, requiring only interceptive treatment, to being rather more complex, requiring input from a multidisciplinary team including orthodontists, oral surgeons and occasionally, restorative dentists. Consequently, prompt identification and management at an early stage is essential in order to reduce the risks of deleterious consequences and enable more predictable treatment outcomes.