Hansen CH, Michlmayr D, Gubbels SM Assessment of protection against reinfection with SARS-CoV-2 among 4 million PCR-tested individuals in Denmark in 2020: a population-level observational study. Lancet. 2021; https://doi.org/10.1016/S0140-6736(21)00575-4
All healthcare workers, including dental professionals are foot soldiers in the battle against the COVID-19 pandemic. Indeed, in the USA, dental practitioners and dental students are now recruited to deliver COVID-19 vaccines to the general population to expedite vaccine uptake, and rapidly suppress the pandemic. There are many unknowns in the evolving COVID-19 vaccine story, although we now see the true situation in a better light, with the rapid emergence of data from numerous countries, including UK, where the vaccine has currently been administered to millions. The situation is further compounded by the reported vagaries of the increasing number of brand-name vaccines, manufactured on both the new and old vaccine platforms, the purported or real, vaccine adverse effects, the emergence of possible vaccine-resistant viral variants, and the resultant low vaccine uptake due to vacillating public opinion. In this COVID-19 Commentary, we provide an update on the efficacy of the vaccines and the prevalence of adverse effects, as well as a summary of useful information for dental care workers on vaccine protocols appertaining to special situations, as promulgated both by the UK Committee on Vaccination and Immunisation, and the US Advisory Committee on Immunization Practices (ACIP).
Article
March 11 2020 will go down in the annals of human history as a day of reckoning. On that day, confronted with an uncontrollably raging novel viral infection sweeping across the world, the World Health Organization (WHO) declared coronavirus disease 2019 (COVID-19) as a pandemic.1 Since then, the infection has spared virtually no country, claiming over 121 million lives globally and killing over 2.6 million in total.2 A small piece of RNA has indelibly changed human history.
The global research community, at the time, predicted that it may take at least a year or more before an effective vaccine would be found for the disease, because no vaccine for an infectious disease has ever been invented within a year of the infection's arrival, and only a sceptic would have dared to suggest that an efficacious COVID-19 vaccine would be discovered, evaluated and administered within 9 months. Nevertheless, due to the remarkable ingenuity of humankind and the recent, explosive technological advances, both in molecular biology and industrial automation, there are currently at least 13 COVID-19 vaccines approved for early or limited use, and a further 27 are in large scale, Phase III, final trials (as of 18 March 2021).2,3
Vaccine efficacy compared
At the time of their introduction, the effectiveness of these vaccines in large population groups on a community-wide basis, was unknown. Clearly due to the Phase III trials in limited cohorts, which provide only efficacy data under experimental conditions, (note the differentiation between efficacy versus effectiveness), the larger, looming question was how effective would they be on a global scale once administered on a community-wide basis? Initial comparisons of effectiveness in different vaccine trials, in various countries, has been fraught with difficulties. There are many reasons for this, such as their assessment in populations with or without mild symptoms, testing the vaccine in countries with viral variants, and evaluation of the symptomatology after a single dose. Nevertheless, mass vaccination data tracking repositories that collate and analyse ‘big data’ on a global scale, now indicate the profound effectiveness of almost all of the current COVD-19 vaccines. The most satisfying and comforting result of all is that almost all of the currently approved vaccines are highly effective in halting hospital admissions of the vaccinees, meaning that the vaccines stops SARS-CoV-2 in its tracks, totally suppressing its potency to cause severe disease requiring hospitalization, and the associated morbidity and mortality (Table 1).
Name
Platform
Required doses
Interval between dose 1 and dose 2
Cost (US$)
Efficacy against original strain (%)
Efficacy against variants
Preventing hospitalization (%)
Protection from severe disease (%)
Protection from milder disease (%)
Pfizer
mRNA in lipid nanoparticles
2
21 days
19.50
95
UK, South African, Latin American
100
100
94.1
Moderna
mRNA in lipid nanoparticles
2
28 days
25–37
95
UK, South African, Latin American
100
100
95.0
AstraZeneca/Oxford
Adenovirus based
2
Between 4 and 12 weeks
25–37
70
UK, South African, Latin American (low)
100
100
90.0
Johnson & Johnson
Non-replicating human adenovirus-based/DNA
1
NA
10
66–77
UK; South African, Latin American (low)
100
85
USA: 72.0 Latin America: 66 South Africa: 57
Sputnik V
Non-replicating chimp adenovirus-based/DNA
2
21 days (may be increased up to 3 months, if necessary
–
90
No data
100
100
USSR: 91.4
Sinovac
Inactivated SARS-CoV-2
2
28 days apart
US: 30 China: 58
50–90 (various trials)
50% against Latin American strain
100
–
–
Novavax
Protein-based/subunit (RBD Matrix M adjuvant)
2
16 days
–
89
UK, South African
100
–
UK: 89.3 South Africa: 60
One dose or two doses?
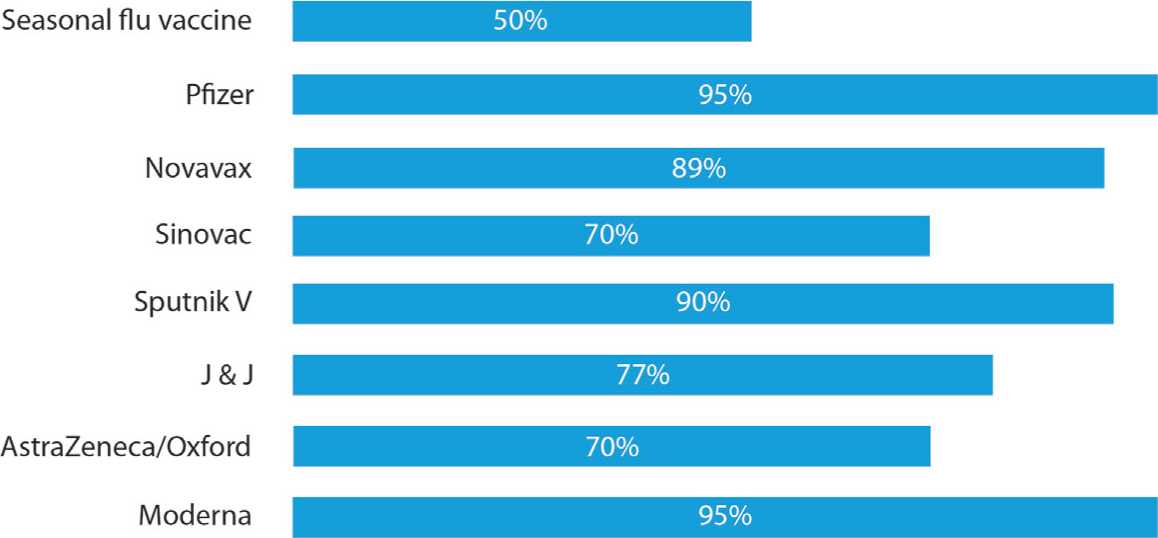
Over two centuries of vaccine history, since their introduction in early 1800s by Edward Jenner in UK, indicates that they do not need to be extremely effective to save lives, and prevent disease. The popular ‘flu shot’ for seasonal influenza, administered annually for example, has an effectiveness of 40–60% according to the Centres for Disease Control and Prevention (CDC) (Figure 1).4 For instance, during 2018–2019, it prevented around 4.4 million influenza illnesses, and some 3,500 influenza-associated deaths.5
Figure 1. The efficacy of COVID-19 vaccines in comparison to the seasonal influenza vaccine (top bar) recommended for dental professionals.
It is also noteworthy that the number of doses can also improve the effectiveness of some vaccines. In the case of vaccines against polio and measles, a higher number of doses will confer peak effectiveness. Similarly, a third dose of hepatitis B vaccine (that should be taken by all dental professionals) leads to seroconversion and will provide cover for the very small minority of individuals (5–7%) who may not seroconvert after the first two doses.6 Of the currently recommended COVID-19 vaccines, all apart from the Johnson and Johnson vaccine need to be administered as a double dose, and even the latter vaccine appears to confer higher protection after a double dose. A double-dose Johnson and Johnson vaccine trial is currently being conducted in UK (Table 1).
Vaccine hesitancy
Despite such emerging and striking data on COVID-19 vaccine efficacy, the rate of vaccine uptake appears to be low in most parts of the world. One reason for this may be the so-called ‘vaccine hesitancy’ due to their real or perceived adverse side-effects. Another could be the ‘vaccine politics’ that has subsumed vaccine uptake, particularly in USA.
Indeed, side-effects of any vaccine are a major concern in general. This is particularly the case when, in the case of COVID-19, a vast majority (approximately 70%) of the whole human populace has to be vaccinated to elicit global herd immunity. Hence, hard data on vaccine side-effects are needed. With the numbers of vaccinees in different jurisdictions increasing on a daily basis, these effects can be seen in a much better light. The WHO, the European Medicines Agency (EMA) and the vaccine regulators in the UK keep a tab on such vaccine adverse effects. For instance, in the UK where 10 million doses of each of the AstraZeneca and Pfizer vaccines have been administered to date, it appears that both vaccines cause between three and six adverse effects, all of which are mild, for every 1000 doses of vaccines administered.7
Although, overall, vaccine-associated severe morbidity seems to be relatively low, a few sporadic reports of major illnesses, such as anaphylaxis that may be likely to be associated with vaccination, appear to be a major concern in some quarters.8 Another case in point is the AstraZeneca vaccine, which was recently suspended in over 13 European countries due to reports of ‘thromboembolic events,’ and later re-introduced (as we were going to press),9 and the sporadic reports of facial palsy with the Sinovac vaccine.10 Yet, it is too early to draw conclusions from these sporadic reports of severe adverse effects, particularly in older people with various comorbidities, until the causality of such adversity is confirmed by detailed analyses, and differentiated from mere association and coincidence.
Vaccines and viral variants
Yet another headache for the vaccine manufacturers is the efficacy of their vaccines in the face of the intermittent arrival of new viral variants through genetic mutations.11 There are up to three major viral variants, and their derivatives, in global circulation: B117 (UK), B1351 (South Africa) and P1 (South America/Brazil1). Fortunately, a number of the currently available vaccines appear to be highly effective against these variants (Table 1). Indeed, according to the manufacturers of mRNA vaccines (i.e. Moderna and Pfizer-BionTech) these are amenable to rapid chemical reconfiguration to combat the variants in the event of the emergence of host-susceptible, viral penetrants, which may become the predominant circulating strain/s. RNA viruses mutate frequently, although the frequency of mutation in coronaviruses is generally lower than other RNA respiratory viruses, such as influenza viruses. This appears to be a saving grace in the battle against COVID-19; however, the unpredictability of viral mutations in general means that there is a great need to keep a close vigil and be ready for rapid action in such an event.
Returning to the story of COVID-19 vaccine administration, there are still a number of debated issues, such as its administration for those who have contracted the disease, mixed vaccine administrations, timing of the first and second dose, and the necessity for a second dose. Various authorities have now stated their positions on these, and given below are salient excerpts of interest to the dental profession, obtained from the recommendations on various vaccine protocols appertaining to special situations, as promulgated by the UK JCVI,12 as well as the US ACIP.13 However, it should be noted that the statements below are based on the currently available data (20 March 2021), and owing to the dynamic nature of the topic, they are subject to constant revision and modification.
COVID-19 vaccination in special situations
Administration of mixed dose vaccines (of two different bands)
There may be rare, exceptional situations where mixed administration of vaccines may be permissible, such as in the case of the unavailability of the same brand of vaccine for the second dose, if there is no record of which vaccine the person received first, if the individual is likely to be at immediate high risk, or is considered unlikely to attend again. The JCVI has stated that such individuals could be given different brands, but has stressed the lack of data on the efficacy of mixed-mode vaccination and the potential side-effects.12 Trans-Atlantic practices appear to differ on this issue, as unlike in UK, the US would not permit people to receive two different vaccine brands, owing to the sparsity of data.13
People with prior SARS-CoV-2 infection
Data from clinical trials indicate that the currently authorized COVID-19 vaccines can be given safely to people with evidence of a prior SARS-CoV-2 infection. People should be offered vaccination regardless of history of prior symptomatic or asymptomatic SARS-CoV-2 infection. Viral testing to assess for acute SARS-CoV-2 infection, or serological testing to assess for prior infection, is not recommended for the purposes of such vaccine decision-making.
A very recent study has shown that natural protection, especially among older people, cannot be relied on, although having had a SARS-CoV-2 infection provides about 80% protection against re-infection.14 There was also no evidence that this immunity waned over the study's 6-month follow-up period. However, when researchers broke down the data by age, they learned that this protection was not uniform – previous infection conferred only 47% protection for people over 65 years old.
People with current SARS-CoV-2 infection
Vaccination of people with known current SARS-CoV-2 infection should be deferred until the person has recovered from the acute illness (if the person had symptoms). While there is no recommended minimum interval between infection and vaccination, current evidence12,13 suggests that the risk of SARS-CoV-2 re-infection is low in the months after initial infection, but may increase with time due to waning immunity. People with recent documented acute SARS-CoV-2 infection may choose to temporarily delay vaccination, if desired.
People who previously received passive antibody therapy
Currently, there are no data on the safety and efficacy of COVID-19 vaccines in people who received monoclonal antibodies or convalescent plasma as part of COVID-19 treatment.
Based on the estimated half-life of such therapies and evidence14 suggesting that re-infection is uncommon in the 90 days after initial infection, vaccination should be deferred for at least 90 days.
Vaccinating people with a known COVID-19 exposure or during COVID-19 outbreaks
COVID-19 vaccines are not currently recommended for outbreak management or for post-exposure prophylaxis to prevent SARS-CoV-2 infection in a person with a known exposure. Because the median incubation period of COVID-19 is 4–5 days,3 it is unlikely that a dose of COVID-19 vaccine would provide an adequate immune response, within the incubation period, for effective post-exposure prophylaxis.
People in the community, or in outpatient settings, who have had a known COVID-19 exposure should not seek vaccination until their quarantine period has ended to avoid potentially exposing healthcare personnel and others during the vaccination visit. This recommendation also applies to people with a known COVID-19 exposure before receipt of the second mRNA vaccine dose.
Considerations for vaccination of people with certain underlying medical conditions
Any currently authorized COVID-19 vaccine can be administered to people with underlying medical conditions who have no contraindications to vaccination.16 Clinical trials demonstrated similar safety and efficacy profiles in people with some underlying medical conditions, including those that place them at increased risk for severe COVID-19, compared to people without comorbidities. Two of these situations appertaining to dentistry are described below and further details on all other underlying conditions are well described in reference 16.
People with a history of Bell's palsy
Cases of Bell's palsy were reported following vaccination of participants in the COVID-19 vaccine clinical trials. However, the authorities did not consider these to be above the frequency expected in the general population, and has not concluded that these cases were causally related to vaccination. Post-vaccination safety surveillance will be important to further assess any possible causal association. In the absence of such evidence, people with a history of Bell's palsy can receive a COVID-19 vaccine.10
People with a history of dermal filler use
Infrequently, people who have received dermal fillers might experience swelling at, or near the site of, filler injection, usually the face or lips, following administration of a dose of an mRNA COVID-19 vaccine. The swelling appears to be temporary, and resolves with medical treatment, including corticosteroid therapy. COVID-19 vaccines can be administered to people who have received injectable dermal fillers who have no contraindications or precautions for vaccination.16 However, these people should be advised to contact their healthcare provider for evaluation if they experience swelling at, or near, a dermal-filler site following vaccination.
Conclusions
Vaccines for COVID-19 are the last great hope for eradicating a ‘once in a century,’ debilitating disease from the face of the earth. Nevertheless, there are many nay-sayers, vaccine doubters, and falsehoods that have led to their rejection by a significant proportion of the community in all regions of the world. Hence, dental professionals have a duty and an obligation to inform their patients, and the local community, of the truth and facts behind the vaccines, and dispel the concerns and fears surrounding this issue. It should not be forgotten that ‘no one is safe until all are safe’ and there is a critical need for global eradication of the virus to return to a post-COVID-19 ‘normalcy.’ For, mutants/variants that may be resistant to the current crop of vaccines, originating from any far corner of the world may lead to further frightening waves of the pandemic.