Malmgren B, Cvek M, Lundberg M, Frykholm A Surgical treatment of ankylosed and infrapositioned reimplanted incisors in adolescents. Scand J Dent Res. 1984; 92:391-399
Day PF, Kindelan SA, Spencer JR Dental trauma: part 2. Managing poor prognosis anterior teeth – treatment options for the subsequent space in a growing patient. J Orthod. 2008; 35:143-155
Atwood DA Reduction of residual ridges: a major oral disease entity. J Prosthet Dent. 1971; 26:266-279
Rodd HD, Davidson LE, Livesey S, Cooke ME Survival of intentionally retained permanent incisor roots following crown root fractures in children. Dent Traumatol. 2002; 18:92-97
Malmgren B, Malmgren O, Andreasen JO Alveolar bone development after decoronation of ankylosed teeth. Endod Topics. 2006; 14:35-40
Malmgren O, Malmgren B Orthodontic management of the traumatized dentition, 4th edn. (eds). Oxford: Blackwell; 2007
Kinirons MJ, Gregg TA, Welbury RR, Cole BOI Variations in the presenting and treatment features in reimplanted permanent incisors in children and their effect on the prevalence of root resorption. Br Dent J. 2000; 189:263-266
Andreason JO, Borum MK, Jacobsen HL, Andreason FM Replantation of 400 avulsed permanent incisors. Part 4. Factors related to periodontal ligament healing. Endod Dent Traumatol. 1995; 11:76-89
Andreason JO, Hjorting-Hansen E Replantation of teeth. Part 1. Radiographic and clinical study of 110 human teeth replanted after accidental loss. Acta Odontol Scand. 1966; 24:263-286
Donaldson M, Kinirons MJ Factors affecting the time of onset of resorption in avulsed and replanted incisor teeth in children. Dent Traumatol. 2001; 17:205-209
Lindskog S, Blomlöf L Influence of osmolality and composition of some storage media on human periodontal ligament cells. Acta Odontol Scand. 1982; 40:435-441
Barrett EJ, Kenny DJ Survival of avulsed permanent maxillary incisors in children following delayed replantation. Endod Dent Traumatol. 1997; 13:269-275
Andersson L, Bodin I, Sorensen S Progression of root resorption following replantation of human teeth after extended extra oral storage. Endod Dent Traumatol. 1989; 5:38-47
Trope M Clinical management of the avulsed tooth: present strategies and future directions. Dental Traumatol. 2002; 18:1-11
Andreasen JO, Bakland LK, Matras RC, Andreasen FM Traumatic intrusion of permanent teeth. Part 1. An epidemiological study of 216 intruded permanent teeth. Dent Traumatol. 2006; 22:83-89
Andreasen JO, Bakland LK, Andreasen FM Traumatic intrusion of permanent teeth. Part 2. A clinical study of the effect of preinjury and injury factors, such as sex, age, stage of root development, tooth location, and extent of injury including number of intruded teeth on 140 intruded permanent teeth. Dent Traumatol. 2006; 22:90-98
Al-Badri S, Kinirons M, Cole B, Welbury R Factors affecting resorption in traumatically intruded permanent incisors in children. Dent Traumatol. 2002; 18:73-76
Humphrey JM, Kenny DJ, Barrett EJ Clinical outcomes for permanent incisor luxations in a pediatric population. I. Intrusions. Dent Traumatol. 2003; 19:266-273
Campbell KM, Casas MJ, Kenny DJ Ankylosis of traumatized permanent incisors: pathogenesis and current approaches to diagnosis and management. J Can Dent Assoc. 2005; 71:763-768
Hadi A, Marius C, Avi S Ankylosed permanent teeth: incidence, etiology and guidelines for clinical management. Med Dent Res. 2018; 1:1-11
Malmgren B Decoronation: how, why, and when?. J Calif Dent Assoc. 2000; 28:846-854
Kofod T, Würtz V, Melsen B Treatment of an ankylosed central incisor by single tooth dento-osseous osteotomy and a simple distraction device. Am J Orthod Dentofacial Orthop. 2005; 127:72-80
Malmgren B, Malmgren O Rate of infraposition of reimplanted ankylosed incisors related to age and growth in children and adolescents. Dent Traumatol. 2002; 18:28-36
Isaacson RJ, Strauss RA, Bridges-Poquis A Moving an ankylosed central incisor using orthodontics, surgery and distraction osteogenesis. Angle Orthod. 2001; 71:411-418
Jimenez-Castellanos E, Orozco-Varo A Prevalence of alterations in the characteristics of smile symmetry in an adult population from southern Europe. J Prosth Dent. 2016; 115:736-740
Einy S, Kridin K, Kaufman AY, Cohenca N Immediate post-operative rehabilitation after decoronation. A systematic review. Dent Traumatol. 2020; 36:141-150
Sigurdsson A, Endo C, Odont C Decoronation as an approach to treat ankylosis in growing children. Pediatr Dent. 2009; 31:123-128
Malmgren B Ridge preservation/decoronation. J Endod. 2013; 39:67-72
Severe traumatic dental injuries to permanent incisor teeth often result in replacement resorption following significant damage to the periodontal ligament. This leads to ankylosis and subsequent infra-occlusion of the traumatized tooth in a growing paediatric patient. Extraction of these teeth can lead to vertical bony defects that complicate restorative management of the edentulous space. Decoronation is a technique employed to preserve bone in the alveolar crest in an attempt to reduce these defects.
CPD/Clinical Relevance: This paper aims to remind readers of the processes of replacement resorption and ankylosis and introduces the use of decoronation for such teeth.
Article
Decoronation is a relatively simple technique that is used as an alternative to extraction in cases of infra-occluding permanent incisor teeth. It involves the removal of the coronal portion of a tooth and, if present, its entire root canal filling. It usually involves gingival mucoperiosteal flap elevation and subcrestal removal of the tooth crown, leaving the root in situ to undergo replacement resorption. This technique should not be confused with root submergence or ‘root burial’ which is the elective burial of a root when the crown has undergone substantial traumatic fracture, such as that in a crown-root fracture with or without pulpal exposure.
Decoronation was first described by Malmgren and colleagues in 1984, and was suggested as an alternative treatment to the extraction of ankylosed teeth.1,2 Routine extractions can result in 0.5-mm alveolar ridge height reduction annually, as well as horizontal bone width, particularly in the premaxilla region, which can compromise future prosthetic rehabilitation.3,4 Extraction of ankylosed anterior teeth can be more destructive, resulting in bony ridge deformities that can complicate future prosthetic treatment. Preserving the root acts as a matrix for new alveolar bone development during replacement resorption. Additionally, vertical alveolar bone is rebuilt during the eruption of the adjacent teeth.
In a study of 77 re-implanted and subsequently decoronated teeth, vertical growth of the socket occurred in patients with residual vertical alveolar growth.5 Patients who underwent decoronation prior to or during peri-pubertal growth periods, experienced no further infrapositioning of the alveolar bone and maintained labial/palatal ridge dimensions into adulthood.6
Replacement resorption
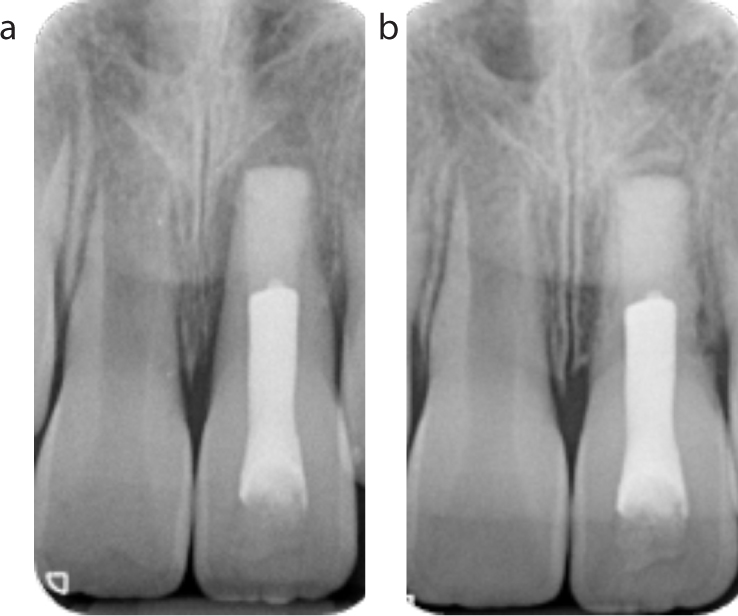
Immediately after a tooth is re-implanted, an inflammatory process occurs within the periodontal ligament (PDL), and reorganization of the new apparatus process is initiated. If there are no vital PDL cells, mesenchymal cells surround the root to repopulate its surface.2 Osteoclasts and osteoblasts directly contact the root surface, initiating resorption of the dentine and simultaneous deposition of new bone, resulting in the replacement of dental tissues by bone.5 This process is known as replacement resorption (Figure 1).
Figure 1. These images demonstrate the process of replacement resorption on a patient's UL1, most noticeable on its distal surface. It shows the fast progression that can occur in a matter of months, between (a) October 2018, and (b) January 2019, following delayed re-implantation and extra-oral root canal treatment of an avulsed tooth.
Replacement root resorption following re-implantation of an avulsed incisor has a reported prevalence of 57–80%.7,8,9,10 Factors that are significantly correlated with an increased risk of replacement resorption include the storage medium of the avulsed tooth, length of extra-oral dry time and the age at which the injury occurs.8,9,10,11,12,13,14
Intrusion injuries occur when the tooth is moved in an apical direction into alveolar bone: they comprise 0.2–1.9% of dental injuries to the permanent dentition.15,16 Severe intrusion can damage the PDL and alveolar socket, leading to replacement resorption and subsequent ankylosis.16,17,18
Ankylosis
Ankylosis is the pathological fusion of cementum or dentine to alveolar bone that occurs following damage to the periodontal ligament. This occurs particularly with severe injuries, such as avulsion and intrusion.1,19 An ankylosed tooth may have a characteristic high percussion tone dependent on the percentage of the root surface involved. Another pathognomonic sign of ankylosis is reduced or absent mobility; however, an ankylosed tooth may still be mobile if less than 20% of the root is ankylosed. Radiographic evidence of replacement resorption includes loss of PDL space and impaired discrimination between the lamina dura and root dentine (Figure 1).20 Nevertheless, conventional radiographs may not necessarily show whether teeth are affected by ankylosis if the affected area is not perpendicular to the X-ray beam. For this reason, cone beam computerized tomography (CBCT) has been described as a promising tool for diagnosis and treatment planning in these cases.20 Failure of a tooth to move under orthodontic forces is also diagnostic of ankylosis.
An ankylosed tooth may exhibit possible infra-occlusion and tilting of adjacent teeth, particularly in those patients still undergoing significant growth.18 The relative infra-occlusion results from continued growth of the adjacent teeth and alveolus, compared to retarded growth of the tooth and related alveolus of the ankylosed tooth (Figure 2).19,22,23 In 2002, Malmgren and Malmgren concluded that, if ankylosis occurs before the age of 10, or before the growth spurt, a high risk of developing severe infrapositioning exists.23 In the case shown in Figure 2, the patient's UL1 was avulsed 30 months previously. It was replanted at a local Accident and Emergency, following 4-hours of storage in milk. This image also demonstrates space loss that can occur during infra-occlusion, when adjacent teeth tilt into the affected tooth's space.
Figure 2. Demonstrates the clinical presentation of an ankylosed and infraoccluded UL1. The UR1 has tilted into the UL1 space, with resultant loss of restorative space.
Ankylosis limits treatment options for traumatized permanent teeth. If an ankylosed tooth is left in situ in children and young adolescents, it will arrest the vertical growth height of the alveolar ridge in the region leaving unsightly gingival margin discrepancies. Attempts to orthodontically extrude an ankylosed tooth, without surgical luxation or distraction osteogenesis, will be unsuccessful, and is likely to result in intrusion of the neighbouring teeth.24 Extraction is often the treatment of choice; however, this can be destructive and result in a vertical bony defect (Figure 3). Therefore, decoronation is advised as an alternative, more conservative option, to preserve the alveolar bone for future restoration of the space with a prosthesis.
Figure 3. Illustrates a small vertical bony defect in another patient following the recent extraction of an UL1, and is likely to progress further with time.
Decoronation
Indication
Decoronation should be performed within the early mixed dentition (7–10 years), ideally within 2 years of the diagnosis of ankylosis or before the patient's growth spurt.1,21,25 If they are in the late mixed dentition stage (10–12 years), then the optimal timing is assessed on a case-by-case basis according to the patient's dental and orthodontic development. Decoronation requires significant vertical bone growth and turnover, and therefore, it is not indicated for those patients who have stopped growing.20
Technique
Decoronation is a relatively simple technique and well tolerated by children and adolescents.26 The procedure involves gingival mucoperiosteal flap elevation and removal of the crown to a subcrestal level. The steps of decoronation are outlined below with clinical images (Figures 4 and 5). The viability of this treatment is dependent on patient cooperation. Cases have been undertaken with the adjunct of inhalation sedation and intravenous sedation. However, inhalation sedation can significantly compromise access to the anterior maxilla and it is preferable that it is used only for administration of the local anaesthetic.
Figure 4. Shows the ankylosed root reduced to 2 mm short of the marginal bone height, this is the same patient as illustrated in Figure 2.Figure 5. Primary closure following decoronation of UL1.
Step 1
A full thickness mucoperiosteal flap is raised around the ankylosed tooth, and the coronal portion is reduced to 2-mm short of the marginal bone height using a diamond bur with continuous saline irrigation (Figure 4). Raising a mucoperiosteal flap increases access to ensure the tooth is removed to a subcrestal level and to enable primary closure. However, the authors are aware that some clinicians undertake this procedure without raising a mucoperiosteal flap and allow healing by secondary intention.
Step 2
An endodontic file can be used to remove the root canal filling, with the aim of preventing a localized foreign body reaction. The file can be inserted through the apex to encourage bleeding and the formation of a blood clot within the canal.
Step 3
Thorough irrigation of the root canal with saline encourages blood flow into the tissue space, allowing an organized blood clot to form from the surrounding tissues. This is vital for new bone formation. Blood within the root canal space not only decreases the risk of infection, but also encourages additional replacement resorption from the internal aspect, while the external resorption process continues. A new periosteum forms on the alveolar crest. As the patient continues to grow, and the adjacent teeth continue to erupt, bone apposition is induced through traction in the periosteum from reorganized fibres.19
Step 4
The mucoperiosteal flap is sutured with the aim of achieving primary closure (Figure 5). The remaining root is left to be gradually, fully resorbed.1,21,23
Step 5
The patient's removable partial denture is fitted. Care must be taken not to place pressure on the surgical site (Figure 6). The coronal portion of the tooth can also be attached to the adjacent tooth (if it is a suitable abutment) as a temporary restoration.
Figure 6. Anterior view of the partial denture in situ, avoiding pressure on the surgical site.
Step 6
Clinical and radiographic review should be undertaken to ensure soft-tissue healing and alveolar bone deposition (Figure 7). Figure 8 shows the same patient 4 months after surgery, demonstrating preservation of the alveolar ridge both horizontally and vertically.
Figure 7. Anterior view of patient two months post-surgery demonstrating good healing of the surgical site and a lost composite restoration UR1. The UR1 had already been root canal treated.Figure 8.
(a) is an anterior view of the patient demonstrating continued healing of the surgical site. The bleeding around the gingival margin is due to replacement of the composite restoration. (b) is an occlusal image which shows horizontal alveolar ridge preservation.
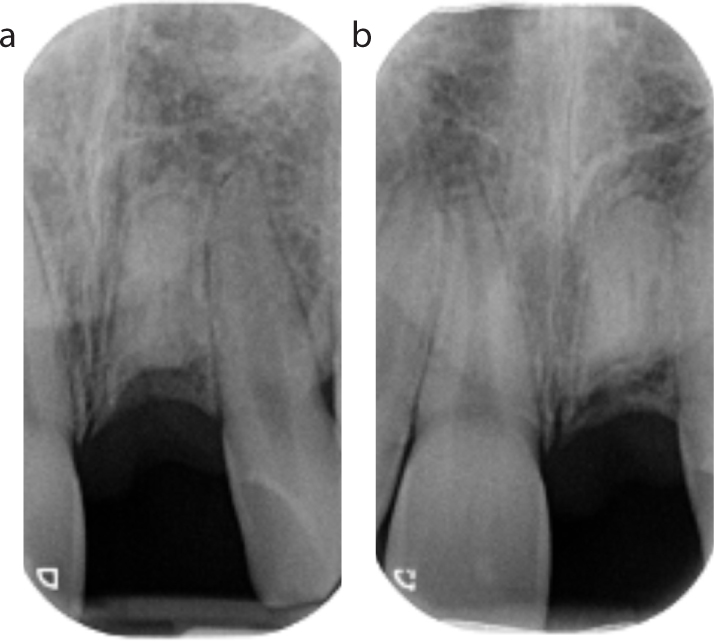
Figures 9–11 illustrate another clinical case of decoronation. A 6-year-old boy avulsed his UL1 while climbing a tree. The tooth had an extra-oral time of 80 minutes (stored in milk) prior to replantation. The tooth was kept under regular review and 2 years later, ankylosis was detected and replacement resorption was noted radiographically (Figure 9). Owing to his age and perceived inability to tolerate decoronation, the tooth was kept under further clinical review. Infra-occlusion progressed (Figure 10) and, at age 11, decoronation was undertaken. His radiographs (Figure 11) demonstrate alveolar bone deposition following this procedure.
Figure 9. This radiograph demonstrates early signs of replacement resorption two years following an avulsion injury to UL1.Figure 10. Anterior view demonstrating infraocclusion of UL1 in an 11-year-old boy, 5 years after an avulsion injury. The gingival discrepancy is evident, and could have been avoided with earlier intervention, but the patient was unable to tolerate decoronation prior to this stage.Figure 11. Demonstrating alveolar bone deposition (a) 3 months and (b) 15 months following decoronation in the same boy as Figures 9 and 10.
Risks and complications of decoronation
Decoronation carries with it all the usual surgical risks: pain, bruising, bleeding, swelling and post-operative infection, and it is important that informed consent is obtained for this procedure. Operators must be careful to avoid damaging the adjacent roots, a risk that is minimized by improving the surgical field of vision by raising a mucoperiosteal flap. It is important to achieve primary closure to minimize the risk of post-operative infection. However, wound breakdown may occur even when primary closure has been achieved. It is important that the patient maintains good oral and, if applicable, denture hygiene post-operatively. Furthermore, the remaining root may become infected.
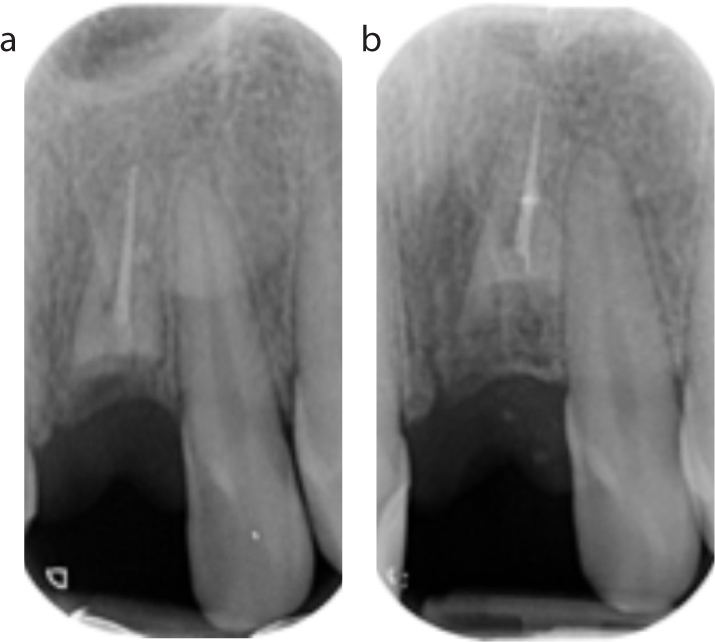
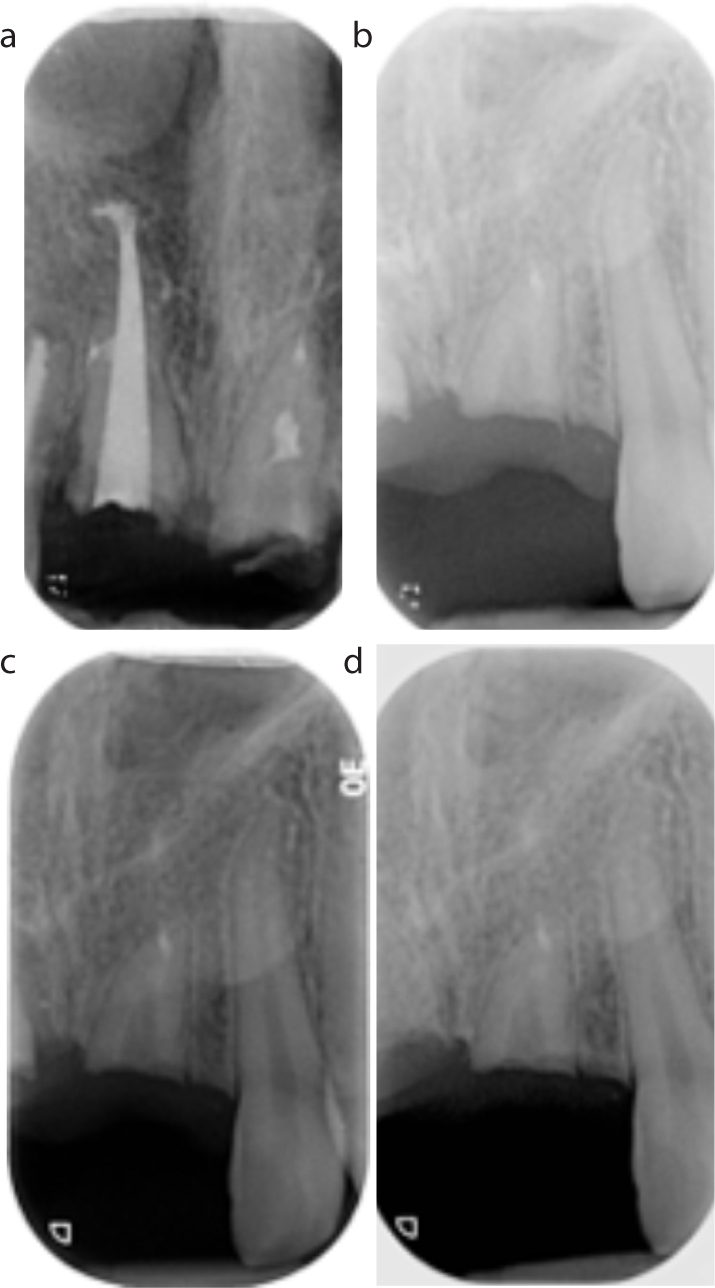
Ideally, all root canal filling should be removed during the procedure to prevent a localized reaction, and to allow alveolar deposition in this area. However, as illustrated in Figure 12, even when remnants of root filling material are left, alveolar bone deposition can still occur. Failure to decoronate below the subcrestal level will result in no vertical bony deposition as illustrated in Figure 13.
Figure 12. Periapical radiographs of UL1 showing remnants of the root canal filling UL1: (a) 3-months post-surgery; and (b) 12-months post-surgery. Continued replacement resorption and alveolar bone deposition above the UL1 root is seen.Figure 13. Demonstrating no vertical alveolar bony deposition: (a) 17 months; (b) 39 months; (c) 47 months; and (d) 59 months after decoronation as subcrestal decoronation was not undertaken at the time of surgery.
The social and psychological effect of losing a tooth in the aesthetic area should be considered as part of the consent process, before the surgical procedure is performed.26,27
Restoration of space
It is beyond the scope of this article to go through the restorative options in depth. Readers are directed to a systematic review for further detail.26 However, it is important that a multidisciplinary team should be involved prior to decoronation to ensure the most suitable provisional restoration is employed and monitored continuously post-surgery.26
Initial restoration of the edentulous space can be completed by immediate denture placement, lingual bar with prosthetic crown, resin-retained bridgework, or attaching the coronal tooth fragment to an adjacent tooth. The latter technique is described by Malmgren as an immediate acid etch bridge, with the intention of a semi-permanent replacement once the wound has healed.28 It is imperative that a prosthetic option is employed to prevent space loss by drifting or tilting of the adjacent teeth. However, bridgework should be undertaken with caution in the early stages, considering the high likelihood of trauma to the neighbouring teeth at the initial injury. Figure 14 demonstrates a partial denture in situ to replace UR1, with evidence of an ankylosed infra-occluding UL1, which would clearly be an unsuitable abutment tooth for a resin-retained bridge. Multidisciplinary input is required in such cases. Figure 6 shows a partial denture in situ following the decoronation of UL1, which, in addition to ensuring aesthetics for the patient, allows for space maintenance and alveolar ridge healing.
Figure 14. This image represents another case and highlights the importance of not undertaking bridgework in the early stages post-surgery. The UR1 has a partial denture replacement following decoronation and the UL1 subsequently became ankylosed and infraoccluded. The UL1 would clearly not have made a good abutment tooth.
Care should be taken to ensure 1-mm space between the mucous membrane and the pontic to avoid interference with alveolar bone remodelling at a later stage. By retaining the resorbing root, the labial contours of the socket can be preserved, allowing improved conditions for potential implant placement at a later date.
Conclusion
Decoronation is a simple, well-tolerated technique to maintain alveolar bone, and facilitate future restorative treatment, when a severe dental injury results in replacement resorption and ankylosis in children and adolescents. General dental practitioners should be aware of this technique so that they can refer paediatric patients to paediatric dental specialists once signs of ankylosis are detected in a growing patient.