Burke F, Lucarotti P. Ten-year outcome of crowns placed within the general dental services in England and Wales. J Dent. 2008; 37:12-24
Meyers I. Herodontics – is there a place for maintaining the apparently hopeless tooth?. Aust Dent J. 2019; 64:S71-S79
Elangovan S, Guzman-Armstrong S, Marshall T, Johnsen D. Clinical decision making in the era of evidence-based dentistry. J Am Dent Assoc. 2018; 149:745-747
Bauer J, Spackman S, Chiappelli F, Prolo P. Evidence-based decision making in dental practice. J Evid Based Dent Pract. 2005; 5:125-130
Nalliah R. Clinical decision making – choosing between intuition, experience and scientific evidence. Br Dent J. 2016; 221:752-754
A definition of a restorative disaster is proposed. Reasons are discussed that contribute to restorative disasters that primarily focus on dentist factors within the dentist–patient relationship. For prevention of a restorative disaster in the failing dentition, the importance of effective communication, the use of an evidence-based approach and having clear consent processes are stressed. The negative consequences of an inability to say ‘no’, a reliance on experience and intuition in decision making, a simple misplaced desire to help and the creation of false hope are seen as factors in managing the failing dentition that may lead to restorative disaster. Using a clinical example, a broad strategy for effective management of a restorative disaster is discussed, which readers may find helpful to apply to similar situations that may occur on occasion in clinical practice.
CPD/Clinical Relevance: This article is relevant to both generalists and specialists involved in the clinical management of heavily restored and failing dentitions, together with students who will be likely to face similar issues in the future.
Article
Failure of restorations is an everyday occurrence for a dentist. Despite advances in materials and technology, the dental restoration remains imperfect, particularly when placed in the hostile environment of the oral cavity. A typical example is to consider that the survival rate of porcelain crowns placed in the General Dental Services in England and Wales is merely 48% at 10 years.1 So, for the dentist, clinical decision making (CDM) and treatment planning (TP) around restoration management, later failure and cycles of replacement are an unavoidable daily reality.
Dentists will, therefore, often find themselves attempting to manage failing dentitions where deteriorating teeth, restorations, medical issues or poor oral health, or a combination of these, means a loss of adequate basic oral functions, such as mastication and acceptable aesthetics, is inevitable if unaddressed. Managing some of these situations by herodontics (Table 1) to maintain function and dignity, particularly in the ageing, failing dentition, using largely minimal intervention dentistry, can be a practical and pragmatic solution when a robust consent process is adopted.2 Yet for some, patient preference for a fixed result rather than the dreaded denture can result in clinicians adopting a much more complex and invasive superherodontic (Table 1) approach in largely futile attempts to maintain the status quo, rather than facing the inevitable reality. In most of these cases, it is only a matter of time before restorative disaster results. When it does, not only can the situation be harder to manage, but the false hope and unwittingly increased expectations created can lead to negative physical, emotional and economic consequences for an increasingly disappointed patient. This in turn can have medico-legal or regulatory repercussions for dentists who may well feel genuinely aggrieved, believing that they have gone above and beyond the call of duty for an ‘ungrateful’ patient.
Herodontics
The use of minimally invasive adhesive dentistry to restore or maintain the function or aesthetics, sometimes provisionally, of a questionable and compromised tooth/dentition (adapted from Meyers2)
Superherodontics
The concept of attempting overambitious high failure risk, often invasive and complex, restorative treatment to restore a questionable and compromised tooth/dentition
There is no accepted definition of a restorative disaster. Perhaps it is best framed as an event or events resulting in the uncontrolled or sudden loss or failure of a significant part of the dentition or complex restorations. The impact of the disaster on the patient and dentist may be much more pronounced were it to occur at an inconvenient time and/or in an inconvenient place.
A typical example of a restorative disaster is seen in Figures 1 and 2, where a full arch bridge on four root-treated teeth with virtually no coronal dentine, has been twice replaced by the same dentist in a short timescale, despite progression of caries. Following many failed attempts at repeated cementation, and eventually, dentist advice to the patient to instead use denture fixative daily, disaster finally strikes, when, despite these superherodontic efforts, bridge retention is suddenly zero.
Figure 1. Carious bridge abutments.Figure 2. Failed bridgework: remnants of denture fixative can be seen on the fitting surface.
This article first aims to explore the reasons for restorative disasters and, in doing so, would hope to allow the reader to reflect on how they can try to avoid them insofar as is possible in clinical practice. Secondly, it proposes a management strategy that may be helpful for both disaster avoidance and management.
Reasons for disasters
CDM and TP is a complex process, even for cases that, at first sight, are relatively straightforward. That complexity increases when managing failing dentitions. While there is, in many circumstances, an overload of information available upon which a dentist can base CDM and TP, scientific evidence is often acquired from research that frequently excludes patient types seen in practice settings,3 meaning that extrapolation of results to some clinical situations, such as the failing dentition, is problematic.
In modern dentistry, CDM and TP are characterized not only by tooth, medical, oral health and disease factors, but by the complex inter-relationship between patient and dentist. While, very occasionally, restorative disaster may be attributed to an unethical approach to dentistry, most disasters appear to occur when the dentist is trying to solve a difficult problem and to do their best for the patient. It is this inter-relationship between patient and dentist, and particularly those parts of the relationship presented by the dentist, that can, in certain circumstances, be the foundation for restorative disaster. This article explores aspects of these in turn; however, the reasons for disaster are multi-factorial and in some disasters, certain reasons will be more important than others and many undoubtedly occur together with differing relative importance within any individual disaster.
Hoping to help
Healthcare professions, such as dentistry, are characterized by professional principles of service and healing, with the main aim being to help patients. Restorative dentistry, with its one-to-one dentist–patient contact, empowers a dentist to directly ‘help’ a patient. The dentist, being uniquely placed to help, usually wants to do so, particularly if they have been managing the patient for a considerable time. They may believe that they are the person best-placed to help, and are almost hard-wired to do so by their professional identity and dentist–patient relationship. The patient, in turn, is likely to be very receptive to offers of help from a trusted professional. It is with these laudable good intentions that many dentists approach the failing dentition.
In failing dentitions, appropriate help may often mean removal of a fixed solution and prosthetic replacement with, initially at least, a removable solution. For the patient, the help they hope for usually means maintenance of some type of fixed solution. In some instances, the patient becomes desperate for help and the dentist eventually accedes to provide some form of superherodontics, often due to being empathetic to the emotional response of the patient, which may only increase the dentist's desire to help. In hoping to help appropriately, the dentist has now misplaced that help, and so embarks on treatment that, on later reflection, or with the benefit of hindsight, is ill-advised, would be unsupported by peers and puts the patient on the path to restorative disaster.
Previous experiences and intuition
Dentists rely on many factors on which to base their CDM and TP. While evidence-based practice should result in a dentist informing an individual patient of the best available evidence and all the reasonable treatment options, there are often situations in clinical practice when the clinical presentation and patient values are uncertain.4 The dentist is then left in the awkward situation of advising treatment interventions whose benefits and risks may be equally uncertain, or indeed unknown. Some advocate the use of decision trees in these circumstances,4 whereas others rely on previous experiences and intuition to guide CDM and TP.
Nalliah, while indicating that many dentists rely on experience and intuition when they should be relying on evidence-based practice, concedes that in a few circumstances, intuition is as, or more effective in CDM.5 Indeed, ideal circumstances where intuition may be useful include situations where a rapid decision is needed, where the evidence base is weak and cannot be related to the particular situation, and where a complex or ambiguous problem does not fit into the usual rules.5 At first sight, a failing dentition could be thought to fit into these situations, and intuition and/or past experience of making complex and fixed restorations is used to make an overambitious fixed restoration with the genuine belief that it is the right decision. However, it is likely to be doomed to disaster.
However, if the lens of reflective practice were to be placed over the use of intuition in such circumstances, there would be realization that most failures are not complex. They often occur due to combinations of caries, periodontal disease, fracture, poor oral health and overloading, which is perhaps due to lack of posterior support, or the effect of previous cycles of replacement of restorations on a diminishing tooth tissue. All can be moderated by medical, social and economic influences. Structured evidential CDM and TP usually offers better solutions for these cases.
Moreover, if experience and intuition is to be used in CDM and TP, it requires high-volume experience and expertise in the particular field.5 While dentists have much experience in dealing with failure of restorations, few, if measured again with the lens of reflection, have sufficient experience or expertise in managing the failed dentition with complex fixed restorations to be able to base their CDM on experience and intuition. An evidence-based approach would be more likely to lead to better decisions. In the failing dentition, the complexity is often not in the clinical situation, but in the effective communication of that to the patient.
Failure to effectively communicate the problem
The General Dental Council mandates that a dental professional ‘must communicate effectively with patients'. This sound advice suggests that this should be done by listening, taking into account individual views and giving time to consider information. Unfortunately, effective communication is not an easy skill to master. It needs to be well learned and for that learning to be regularly updated, together with much practise and reflection.7 Undoubtedly, in the failing dentition, effective communication often means the breaking of bad news, which is considered to be one of the most difficult tasks that a dentist has to do.8 There are barriers to its effective communication, such as personal fears, time factors, and inadequate support.9 Moreover, avoidance of the emotional reactions to the news, by both the patient and the dentist, may compound the problem.10 When bad news is not effectively communicated, the dentist may unwittingly create false hope for the patient. As Groopman11 writes:
‘False hope does not recognize the risks and dangers that true hope does, false hope can lead to intemperate choices and flawed decision making’.
As a consequence, ineffective communication may ultimately lead the dentist on the path to provision of an overambitious and poorly planned fixed restoration that ignores basic design principles, risking failure and restorative disaster in time.
Once the dentist is on the path to making that intemperate choice or flawed decision, there will be attempts to effectively communicate the risks and benefits of the proposed treatment to the patient, as is their professional obligation. However, there is significant evidence that patients not only overestimate the benefits of interventions,12 but significantly more underestimate the risks of interventions.13 When this is added to the dentist perhaps conveying an overestimate of the chances of success and/or an underestimate of the risks of failure, there is a ‘perfect storm’ of ineffective communication, misunderstanding and false hope from which restorative disaster may emanate.
Inability to say ‘no’
Dentists in clinical practice more often than not restore teeth, repair teeth, transform the unaesthetic smile to the aesthetic smile or make the painful tooth painless. In short, when asked by a patient to address a problem, the dentist regularly says ‘yes’.
Saying ‘no’ to a patient's wishes can be something that the dentist is both unaccustomed to and finds counterintuitive to the need to ‘help’ a patient. Psychologists note that this inability to say ‘no’ may in part be due to a fear of conflict and the need to neither disappoint nor hurt someone.14 The reasons for not saying ‘no’ may well resonate with many dentists who have managed failing dentitions. A patient is likely to have an array of feelings when faced with the advice that a large part of their dentition has failed and a fixed solution is inadvisable. They may be emotionally upset, angry, indicate disbelief, become withdrawn or anxious and fearful. Not all dentists are equally well-equipped to manage these reactions, nor are some able to respond as empathetically as a patient may want. In consequence, saying ‘yes’ may be easier to avoid dealing with such reactions and, at that point, a dentist may feel obligated to think of a plan that in reality has no chance of success.
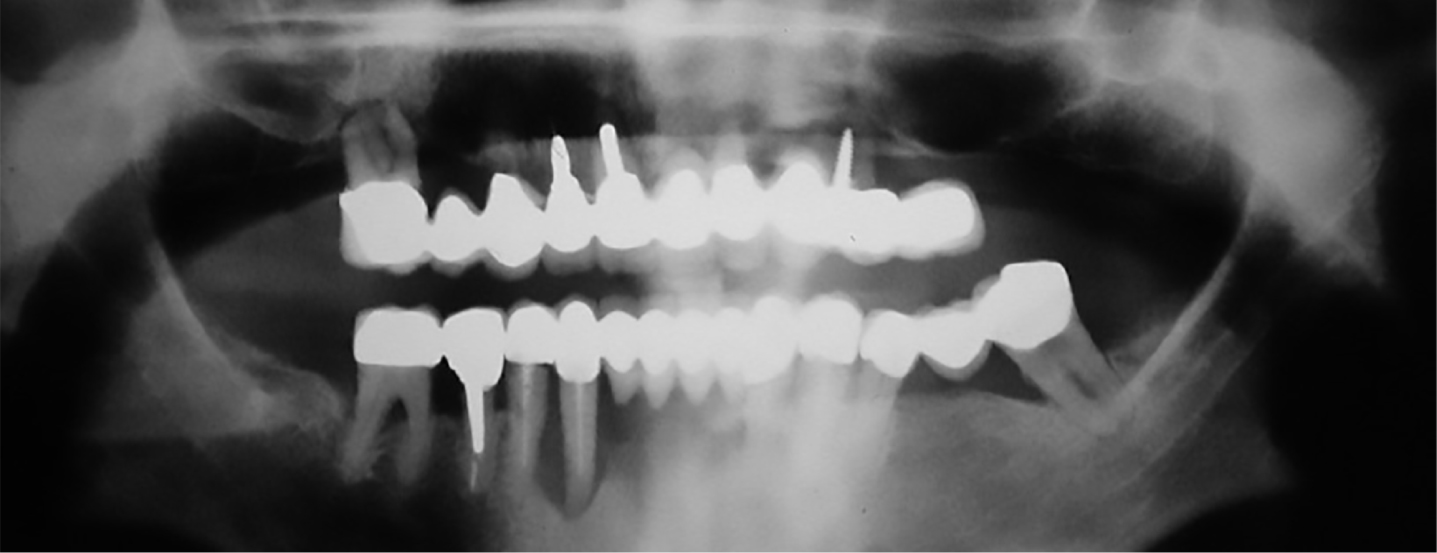
Worse still, not saying ‘no’ risks the dentist embarking on a plan that they may not be clinically competent to deliver and requires high-level technical support that may also be beyond the technical competence of their dental laboratory. To deliver such a superherodontic plan may again involve the need to ignore basic design principles, leading to increased chances of error and the provision of uncleanable restorations with an outcome that is likely to spiral towards restorative disaster relatively quickly. Such a situation is seen in Figures 3–5 where the upper arch bridge made in this case lasted less than a year before detaching from all teeth except UR6, which was mobile and severely periodontally compromised.
Figure 3. OPT radiograph showing a failed full upper arch bridge on heavily restored periodontally compromised teeth. Major lower arch problems are seen.Figure 4. The upper bridge is uncleanable with abutment teeth carious around margins.Figure 5. Failed bridgework: only UR6 was retaining the bridge.
In cases similar to that seen in Figures 3–5, not only is the dentist left with an even more disappointed and distraught patient, along with a likely breakdown of the professional relationship, they are potentially left with the financial consequences of both an early failure of an expensive fixed restoration and the remedial management of the restorative disaster. At worst, the patient may choose to escalate that disappointment in the form of a claim for compensation, or a complaint to the regulator. These can be tough lessons that may arise from an inability to say ‘no’.
Misunderstandings of obligations and consent
Shared decision making is a standard to which dental professionals should adhere6 in CDM and TP, and is of paramount importance in the failing dentition. One of the mistakes that a dentist can make in patient management is the erroneous belief that, if a patient ‘wants’ a particular treatment, the dentist is obligated to provide that treatment. This is of particular importance in the failing dentition when a patient often ‘wants’ a fixed solution to a problem where sense and reason dictate such an option to be completely unreasonable.
The General Dental Council (GDC) asks dentists to listen to patients, to discuss options with patients, to give full and honest answers to patients, to give risks and benefits of all options (including risks of delay or no treatment) and to encourage patients to ask questions about options.6 The GDC, however, does not ask dentists to present or provide unreasonable treatment options to patients. When faced with a patient who ‘wants’ the unreasonable fixed solution, a robust explanation of its unreasonableness, empathetic answering of questions, discussion on reasonable treatment options and giving the patient time to come to terms with the situation, may involve short-term difficult conversations, but may well avoid a future restorative disaster. The superherodontic approach, which does what the patient ‘wants’ in these circumstances is likely to be an expressway to restorative disaster.
Patients value the professional opinion of dentists, yet, too often in CDM and TP, options are presented neutrally to a patient, perhaps to avoid paternalism. This can sometimes lead to patient confusion around multiple options. However, the GDC advises that things that a ‘patient might want to know’ include the recommended treatment option of the dentist.6 In effect, the option recommended by the dentist is valued highly by many patients as an inherent component of the professional relationship between patient and dentist. It is imperative that this trust that patients have in dentists is not abused, and it is the responsibility of the dentist to give appropriate reasonable recommendations. Using such recommendations is likely to facilitate CDM and TP in the failing dentition and may avoid some restorative disasters.
Following the Montgomery ruling,15 it is even more important to present treatment options to patients in a manner that they can understand, and to find out about their specific circumstances and what concerns they may have on an individual basis. This is particularly important in the failing dentition where concerns regarding loss of a fixed option may weigh heavily on a patient's mind. When considering acceding to patient demands for an unreasonable or overambitious plan, the dentist would be mindful to reflect on their obligations to fully explain risks, which, as has already been discussed, are often underestimated by a patient. If the dentist fails to warn of risks appropriately, which should include inevitable failure in such cases, they risk a later accusation of providing treatment without valid consent and may be left open to complaints, claims and regulatory consequences that would be hard to defend.
Strategy for restorative disaster management
There is no single solution for managing the restorative disaster as each will have its own unique problems, yet despite that, broad general principles can be applied to facilitate management.
Using the case already presented in Figures 3–5 as an example to aid understanding, a strategy for restorative disaster management is presented.
History taking and examination
It cannot be overstressed how important a thorough history is in the failing dentition. It should include an in-depth medical and social history to gain holistic understanding of patient circumstances and expectations. A history is not simply a timeline of facts, it allows the dentist to hear firsthand the patient's ‘story’. It is the dentist's first opportunity to listen carefully to the patient and, as the GDC emphasizes, that is something that patients expect.6
In this case, the patient's story was of seeking help from a dentist a year previously following failure of some upper bridgework and with a purported promise that another bridge would solve the problem, the present bridge was made. It apparently worked well for a few months and the patient was pleased despite it being expensive. Then, suddenly it became loose, then looser and then there was a crisis point when the patient felt that it was hanging by a thread. The patient reported disappointment, regret and anger that things had failed so quickly and wanted another bridge, not wishing to contemplate a denture. The previous patient–dentist relationship had not survived intact. The lower arch was symptom free except for some mild toothache from LL7.
This history (or patient story) is a very familiar one regarding the presentation of a restorative disaster, but it is important to remember that it is only one side of a story. The dentist's story is unknown, so avoiding undue criticism is advisable. For the dentist managing such a disaster, effective listening is paramount, not just for appropriate clinical management, but for self-protection, because failure to treat a patient with respect, or failure to show the patient that they are being listened to, has been implicated in many complaints and claims for compensation.16
While at first sight in most restorative disasters, failure is obvious, an in-depth examination and appropriate special tests and imaging are even more important in the restorative disaster. First, it is easy to miss other issues by focusing solely on the chief complaint. For example, in this case the lower arch is not the patient's focus yet Figure 3 and clinical examination show significant generalized periodontal disease, unrestorable lingual caries in tooth LL7 (a bridge abutment) (Figure 6), a perio-endo lesion on LR3 (a bridge abutment), sub-optimal root fillings in teeth LR4, LR3 and LL4 and marginal caries around teeth LR5 and LR4 (both bridge abutments). In reality, following examination, the lower arch is headed for a restorative disaster too, albeit at a slower rate than the upper arch. Secondly, detailed examination is paramount to ensure detailed, accurate and contemporaneous clinical records in restorative disasters. The dentist should be aware that the records may be viewed externally were the patient to take matters further regarding their anger and disappointment at previous treatment. In addition, the dentist is likely to recommend a removable solution, which is not what the patient initially wanted, and it is important for the treating dentist to appreciate that no matter how bad the previous result, it was ‘fixed’ and the treating dentist from the patient's view was the person who could not provide them with a fixed result. In consequence, were the patient to fail to adapt to a removable prosthesis, the treating dentist may find a disappointed patient and their own actions later being subject to external scrutiny with the records used as evidence.
Figure 6. Unrestorable buccal caries on LL7.
One of the difficulties in history taking and examination in a restorative disaster is that the dentist is presented with a high volume of often complex information, and making instant impulsive decisions is likely to be problematic. A better approach is to take time (albeit the nature of a restorative disaster may mean that the timescales are relatively short) to appropriately assimilate the information and reflect upon it, so that options can be presented to the patient in a considered manner. Additionally, the dentist should be aware of patient interpretations of their communication during examination. Communicating to a patient within the moment of discovery that something is horribly wrong – the so called ‘Oh No! Second’17 – is likely to cause undue stress for the patient before the dentist is yet able to fully interpret the information from that discovery. The dentist should be cautious in what the patient is told at this stage, while still being open and honest, as an inadvertent comment made in haste, without reflection, may mean the patient is inadvertently given unintentional misleading information.
Diagnosis, CDM and breaking bad news
In a restorative disaster, diagnosis is generally relatively simple in that widespread terminal failure of abutments is often evident. In this case, in the upper arch, the abutment teeth UR6, UR3, UR2, UR1, UL2 and UL4 were all affected by insurmountable multiple pathologies with various combinations of periodontal disease, sub-alveolar caries, root fracture and perio-endo pathologies (Figures 3 and 4). In the lower arch, the situation of the whole arch was less imminently terminal, but teeth LL7 and LR3 (Figures 3 and 6) were highly likely not to be amenable to realistic restoration.
At first sight in a case such as this, CDM would appear relatively straightforward in the upper arch. Realistically, the only reasonable initial treatment option was a clearance and a complete upper immediate denture. This, however, oversimplifies the effect that such a decision is likely to have on the patient. Few dentists, even when presented with the overwhelming issues and evidence from examination as in this case, are likely to feel 100% confident in that irreversible decision, the author included. Dentists work within a dental team, and without the need of an unnecessary secondary care referral that is likely to bring unwanted delay, all that is required is usually a sense check or second opinion from a trusted colleague, either within the same dental team, or another practice in the locality, to give some peer review of the proposed decisions.
In the lower arch, there are more options. In some circumstances in restorative disaster situations, secondary care advice may be appropriate regarding longer-term management. However, that is usually best left until simple initial remedial advice and treatment has been taken forward.
Once satisfied with the CDM, the dentist's next role in a restorative disaster is to break bad news. Bad news for a patient with a restorative disaster is the type of situation that could be considered life-changing and devastating, because it often involves unexpected extractions and loss of fixed anterior teeth,10 just as in this case. This is a situation that the dentist may dread because there are many common barriers to effective communication of bad news. These include patient under-preparedness, time factors, fear and anxiety around patient reactions and, in particular, emotional responses, feelings of failure or blame, and removal of hope from the patient.18 The problem in a restorative disaster is that the impact of the bad news appears to be proportional to the difference between the patient's assumptions of the situation and the actual reality.18 Using this case as an example, patient expectations were of a replacement bridge, but the harsh reality was the necessity for an upper clearance and an immediate denture. Undoubtedly the patient will most likely be distraught when presented with the bad news. How well or otherwise this news is communicated will affect how well the patient understands the issues involved and how well they are satisfied with the dentist breaking the bad news.19 Indeed, as Buckman and Kason19 wrote about breaking bad news:
‘If we do it badly, the patients and family members may never forgive us; if we do it well they may never forget us.’
It is imperative, therefore, that bad news is presented to the patient effectively, and with clarity, transparency and honesty, and above all, in both a sensitive and empathetic manner. The SPIKES protocol20 is ideally suited as a communication method for the restorative disaster. While originally designed for breaking bad news for cancer patients, it has been taught effectively in the dental curriculum10 and is a communication method that is a tool of great value to any dentist.
Of particular importance in the restorative disaster is the need for time for patient acceptance of their situation. Such patients may be in denial or be angry and upset and unable to move on to a stage of acceptance as quickly as the constraints of a traditional dental appointment allow. This means the dentist putting the patient's interests first, and having to manage time appropriately, often on more than one occasion, to break bad news effectively. Unless the patient can move on, then treatment cannot commence. A key component of SPIKES is having a strategy to move forward towards remedial treatment.20 This involves seeking the patient's views, which allows the patient to regain control and to be inherently involved in the proposed treatment.10 With the restorative disaster, which is an uncontrolled failure, the importance of the patient regaining control is pivotal to management. In most cases, effective communication permits treatment to commence, but if it fails to do so, the dentist should consider referrals to other colleagues for additional opinion and review. Sometimes communication barriers between individuals require a fresh approach, and a change in personnel may aid patient acceptance.
Obtaining consent for remedial TP
The Montgomery case15 informs dentists that they have to respect a patient's right to autonomy and, in so doing, their right to make informed choices about their care. One of the major problems in a restorative disaster scenario is that gap between patient expectation and reality. The treating dentist may only have options that are guaranteed to disappoint, so with that in mind, the first step to consent is effective communication, as previously described. Consent is a process, and a major part of that process is how risks are communicated to the patient.21
Consent requires not only the general risks to be effectively communicated, but also those that the dentist would consider of particular importance to the individual patient.21 In this case, where consent involves advising an upper clearance and a complete upper immediate denture, where patient expectation was a hoped-for replacement bridge, there is a big disappointment gap to fill. To achieve consent, it would be imperative to inform such a patient of the limitations of an immediate denture, the need for much aftercare, the difficulties in adapting to a denture, the need for perseverance and, most importantly, that despite best efforts, the patient may never cope with a denture that meets all their expectations to their complete satisfaction.
Just as important in the restorative disaster would be to heed GDC advice22 and ‘document your discussion with the patient in their notes’ in case the consent is later subject to scrutiny. Additional validation and evidence of a sound consent process in a restorative disaster may be found by the dentist writing directly to patients. This has the advantages of further involving the patient in their care (a key tenet of the NHS Constitution23), offering a patient-centred communication style24 and doing this both strengthens the professional relationship, and helps the patient cope with the clinical problem.25 For dentists unfamiliar with writing to patients, some excellent guidelines are available from the Academy of Medical Royal Colleges25 to assist effective communication by this method. Often, the difficulty in the restorative disaster is the pressing time in which to make decisions because the final event of a restorative disaster may occur within a short time. Thus, consent processes can be more problematic, but it is essential that, despite this, every effort is made to achieve valid consent.
While the adoption of effective communication and a sound and sensitive explanation of risks, benefits and reasonable treatment options achieves consent for remedial treatment in most restorative disasters, this is not always the case. Exceptionally, some patients will refuse treatment and, in such cases, it is important that the dentist either lets the patient walk away knowing the risks of no treatment, or refers them to others. A mistake in this situation is for the dentist to somehow feel obligated to provide overambitious, hopeless and futile treatment simply because they feel coerced to do so by a potentially demanding patient who is as yet unable to cope with the disappointment gap. Ultimately, such an approach is in the interests of neither patient nor dentist.
Keeping treatment simple
TP in restorative disasters is usually less complex than the failure that has resulted in disaster. Inherently, treatment usually simplifies the mouth. Key to TP in these cases is the already-taken steps of history and examination, diagnosis, CDM and effective communication of bad news, followed by consideration of options and consent for remedial treatment. In effect, a logical sequence is followed to treatment plan appropriately.
Logical TP puts neat phases in place. For example, an emergency and stabilization phase followed by prevention and control, and then an initial restorative phase.26 While this works for the majority of TP in dentistry, it is sometimes not as rigidly applicable to the restorative disaster. For example, in this case, the emergency and stabilization phase (ie upper clearance and removal of tooth LL7; Figures 5 and 6) needs to be contemporaneous with the initial restorative phase in the provision of the complete immediate upper denture at the initial detriment of prevention and control. Thereafter, attempts at oral health improvement in the lower arch, stabilization of the periodontal condition via basic treatment, root amputation of tooth LR3 keeping the bridge intact, and minimally invasive herodontics to restore carious lesions on bridge retainer margins of teeth LR5 and LR4 (Figure 7), can be delayed and undertaken a short time later.
Figure 7. Herodontic restoration of LR5 and LR4 with root amputation of LR3 to maintain the lower arch.
While the plan itself, like most restorative disasters, is straightforward and simple in that it deals with the restorative disaster in the upper arch and starts to manage the lower arch to prevent a restorative disaster, it does present the dentist with some difficult problems that sometimes require some thinking ‘out of the box’ using different treatment protocols and techniques than the norm. For example, in this case the upper bridge was ‘hanging like a thread’ from UR6 only (Figure 5) and was highly unlikely to remain in situ for long, potentially leaving the patient in an undignified state with no denture made. There was a real risk that taking an impression would inadvertently remove UR6 and the bridge. To mitigate these risks, wax was placed around undercuts, petroleum jelly smeared over the bridge with the impression taken in one stage with an adapted stock tray using alginate. Jaw registration was straightforward with an inter-occlusal record, and the patient provided a photograph for tooth selection. The denture was thus made in one stage from the impression/jaw registration stage to finish, because a try-in stage had minimal value and time was of the essence to prevent total disaster.
With the possible exception of the root amputation of tooth LR3 (Figure 7), there was nothing extraordinary or complex about this approach to restorative disaster TP and delivery, and that is true of most of these case types. Problem-solving was needed, as it is in most disasters, but that skill is fortunately commonplace among dentists. The complexity in the restorative disaster is generally not in the TP or the treatment, it is encouraging the patient to accept the approach to treatment positively.
Reassessment and reflection
Traditionally, reassessment occurs at defined stages in TP. In the aftermath of a restorative disaster, reassessment needs to be dynamic and continual, particularly in the early stages following remedial treatment. For example, in this case, there were multiple extractions and the patient moved from fully dentate to edentate in the upper arch with no previous denture-wearing experience in the course of one visit and was provided with a prosthesis, which by its very nature was temporary, had limitations, and was likely to have sub-optimal tissue adaptation.
Reassessment is necessary to determine reline strategies and when to proceed to a more definitive denture. In this case, the patient coped well with the transition from bridge to denture, and following provision of a definitive complete upper denture, no further treatment was necessary in the upper arch. This is not always the case, and at appropriate times reassessment may involve implant consultations, or the delivery of further bad news.
In this case, reassessment in the lower arch was focused on ensuring a restorative disaster did not occur whatever way the lower arch went, and that instead there was proactive management of problems. For completeness, the lower arch was maintained for 2 years without further treatment, but deterioration in abutments required a planned move to a partial lower acrylic denture from the bridge keeping LR6, LR4, LL3 and LL5. This situation was maintained for a further 5 years until, eventually, the mandibular dentition was lost, but in a planned manner, and a complete lower denture made. This time, and not unsurprisingly, the patient adapted less well to the complete lower denture. Further reassessment took place regarding an implant overdenture (for economic reasons the patient was unable to afford other options). After much discussion, the patient chose to accept the existing conventional denture, albeit with limitations.
This story is fairly typical of how a restorative disaster plays out over a prolonged time. Reassessment is a great part of that process and it should occur whenever it is needed, by either the patient or the dentist, and not necessarily at fixed time points.
Fortunately, restorative disasters are not that common, but they are situations that can provide a dentist with deep insight into how effective or otherwise their management is of challenging situations that do not necessarily follow the normal rules. Reflective practice is an essential component of all health professions27 and it is through the lens of reflective practice that the dentist should examine the restorative disaster.
Using tools such as the Gibbs reflective cycle,28 or similar, and reflecting frequently and deeply can promote lifelong learning and guide the development of personal development plans. Using the reflective learning from a restorative disaster positively, whether created by the dentist or managed by the dentist, or both, is likely to aid the reflective practitioner to enhance communication skills, CDM and TP, which in turn may well improve management, not only of these type of cases, but additionally, of more routine cases.
Conclusion
Restorative disaster can sometimes be hard for the dentist to avoid and, on reflection, some readers may recognize some of the pitfalls, often borne out of misguided attempts to find a solution that the patient ‘wants’, that may have impacted on their CDM and TP in such cases where fixed restoration failure has occurred. The reasons for restorative disaster presented herein rarely occur alone, and often co-exist together, with some being more prominent than others, on an individual basis. The restorative disaster is best managed by good clinical history and examination skills and effective communication of the nature of the problem, reasonable treatment options, and risks and benefits. Additionally, sound management requires an approach that puts patient's interests first, which commonly involves the provision of high-quality, simple (usually removable prosthesis-based) treatment and later reassessment, potentially using other practitioners for second opinions and advice, where necessary, at any stage in the process where the treating dentist or patient feels that this may be beneficial to optimal patient care. Self-reflection on restorative disaster causes and management is integral to a practitioner's lifelong learning process in this difficult area of clinical dentistry.