Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology.Philadelphia: WB Saunders; 1995
Bennington IC, Burnett CA, Clifford TJ. Prosthodontic rehabilitation of patients with orofcial defects. Dent Update. 2012; 39:291-296
Taylor TD. Clinical Maxillofacial Prosthetics.Illinois: Quintessence; 2000
Desjardins R. Early rehabilitative management of the maxillectomy patient. J Prosth Dent. 1977; 38
Aramany MA. Basic principles of obturator design for partially edentulous patients. Part I: classification. J Prosthet Dent. 1978; 40:554-557
Curtis TA, Marunick MT. Maxillofacial Rehabilitation. Prosthodontic and Surgical Considerations.St Louis: Mosby;
Zarb GA. The maxillary resection and its prosthetic replacement. J Prosthet Dent. 1967; 18
Ali R, Altaie A, Nattress B. Rehabilitation of oncology patients with hard palate defects. Part 2: principles of obturator design. Dent Update. 2015; 42:428-434
Siddal KZ, Rogers SN, Butterworth CJ. The prosthodontic pathway of the oral cancer patient. Dent Update. 2012; 39:98-106
Prosthodontic Pathways in the Interdisciplinary Management of a Patient with an Ameloblastoma in the Maxilla Y.K.Shashie Nathaliya Susiripala Vasantha Sivaguru Dental Update 2024 48:3, 707-709.
Authors
Y.K.Shashie NathaliyaSusiripala
BDS (Sri Lanka)
MD in Restorative Dentistry (Colombo, Sri Lanka), Senior Registrar in Restorative Dentistry, National Dental Teaching Hospital, Ward Place, Colombo, Sri Lanka
MS in Restorative Dentistry, (Colombo, Sri Lanka), Consultant in Restorative Dentistry, National Dental Teaching Hospital, Ward Place, Colombo 07, Sri Lanka
Ameloblastoma is a benign and locally aggressive neoplasm. The treatment of choice is surgical resection, which, although removing tumour, will often result in aesthetic and functional problems for the patient.
CPD/Clinical Relevance: For patients with ameloblastoma in the maxilla, careful planning with the involvement of a multidisciplinary team is essential for improving post-surgical quality of life.
Article
Ameloblastoma is a benign and locally aggressive neoplasm. It is the most common neoplasm of origin from the odontogenic epithelium and may arise from the enamel organ, epithelium of odontogenic cysts or basal cells of the oral mucosa.1 In most cases, ameloblastomata arise in the mandibular molar and ramus regions;1 however, they may also arise in the maxilla. This case report describes the prosthodontic pathways in the interdisciplinary management of a patient who was diagnosed with a solid unicystic ameloblastoma in the maxilla, and who underwent maxillectomy.
Case report
A 17-year-old male patient who was waiting for partial maxillectomy as the necessary treatment for an ameloblastoma, presented to the Restorative Unit at the Dental Institute, Colombo after being referred from the Oral and Maxillofacial Surgery Unit of the same institute. The oral and maxillofacial surgeon's main concern was the construction of a surgical obturator prior to the surgical excision of the tumour.
The patient's history revealed that he had undergone an incisional biopsy of the lesion under general anaesthesia. Histopathological features led to a diagnosis of a solid multicystic ameloblastoma.
The patient was otherwise healthy and his past dental history was limited to full mouth scaling. The patient did not smoke or drink alcohol and his oral hygiene practices were limited to once-daily tooth brushing with an adult toothbrush comprising medium textured bristles and using a fluoridated toothpaste. He was a student at a private university and had a great support from his family, teachers and friends for coping with the situation.
The extra-oral examination revealed a marked non-tender facial swelling over the upper lip extending to the left side of the cheek (Figure 1). The patient revealed that the size of the swelling had been gradually increasing over the previous year. There was no loss of sensation over the cheek or lips of the affected side.
Figure 1. Pre-surgical facial view.
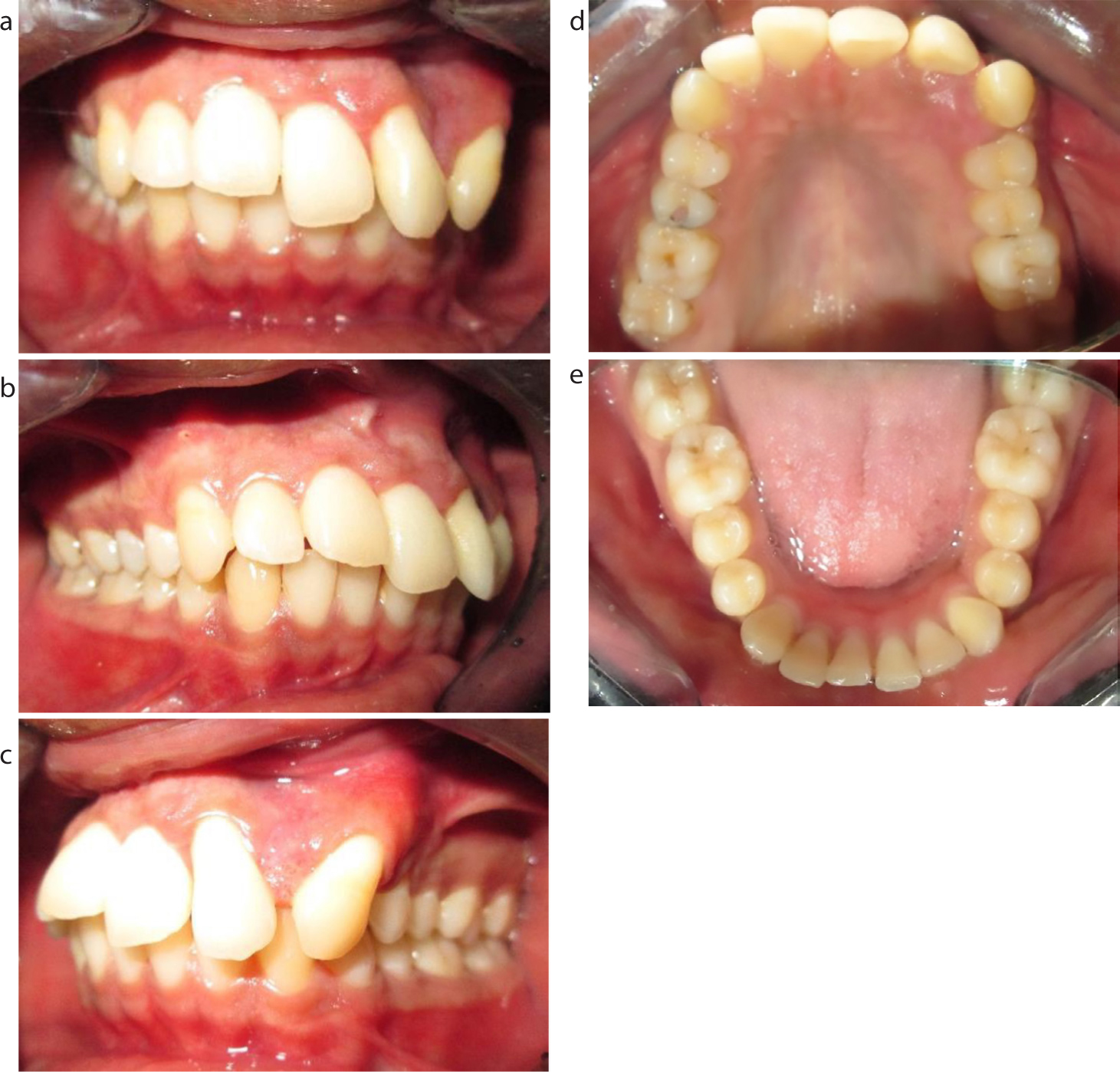
The intra-oral examination revealed that buccal, labial, lingual and palatal mucosa, and gingiva were of normal colour and texture except between UL2 and UL3 where keratinized gingiva was thin and mildly erythematous in colour. A bony hard non-tender swelling of the alveolar ridge in the UL1 to UL4 region, extending buccally and palatally with no discreet margin, was clinically observed. UL1, UL2 and UL3 were extruded with grade 1 mobility and spacing, and with no tenderness to percussion (Figure 2). A full complement of teeth was present in the mouth.
Figure 2. (a) Pre-surgical anterior view (teeth in occlusion. (b) Pre-surgical right lateral view (teeth in occlusion). (c) Pre-surgical left lateral view (teeth in occlusion). (d) Pre-surgical upper occlusal view. (e) Pre-surgical lower occlusal view.
UR5 had a carious pulp exposure, which was associated with a history of severe pain, and was clinically visible. Dentinal caries of UR6, UL6, LL6, and LR8 were also observed. The patient had marginal plaque and calculus deposits interdentally on his UR5–7, UL4–7, LR7 and LL7, but with no signs of periodontal disease. The Basic Periodontal Examination (BPE) score was <2 for every sextant.
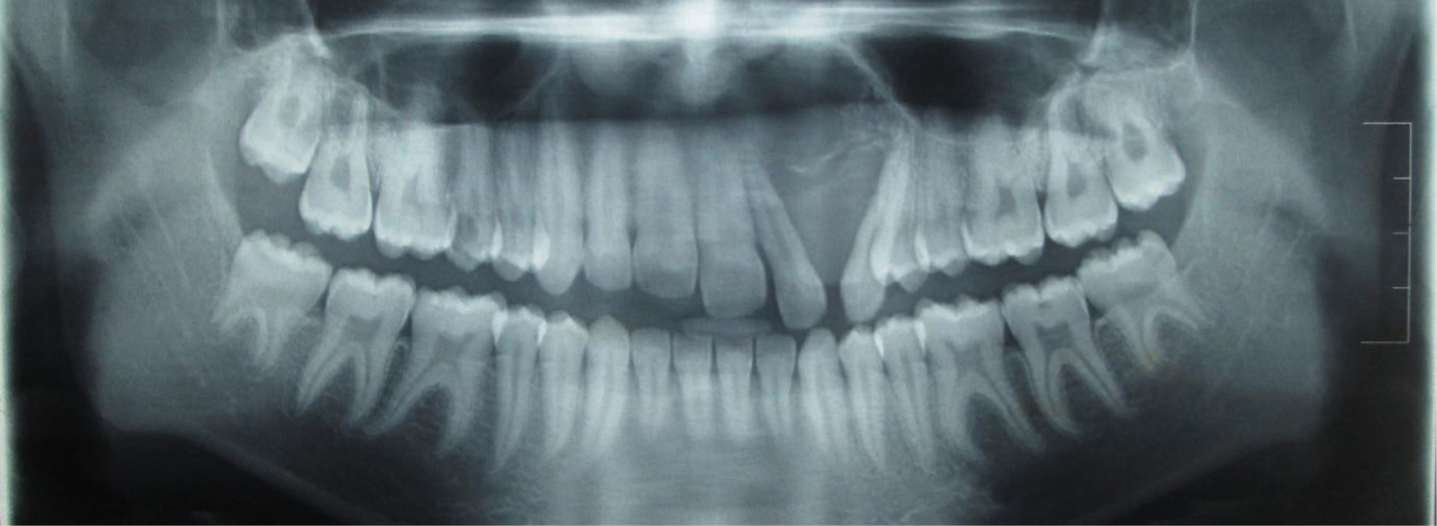
All upper teeth except UL3 and UL4 showed a positive response to sensibility testing with the electric pulp tester. Radiological investigations, including a dental panoramic tomogram (DPT), an occipitomental (OM) view of the skull and a computed tomogram (CT) scan, were taken in order to arrive at a diagnosis and plan for the surgical procedure. They revealed a radiolucent area without well-demarcated margins in the UL2 to UL3 region, with the roots of UL2 and UL3 being displaced (Figure 3). An intra-oral peri-apical (IOPA) radiograph of UR5 confirmed the absence of peri-apical radiolucency. Blood investigations, including serum electrolytes, fasting blood sugar, full blood count, were within normal reference ranges.
Figure 3. Pre-surgical dental panoramic tomogram.
A multidisciplinary treatment plan was formulated in order to ensure a good quality of life following the surgery.
The pre-surgical phase
At the initial visit, the patient was educated on the importance of good oral hygiene measures, and the maintenance of healthy gingivae and teeth in order to have uneventful post-surgical healing and, thereafter, for the survival of his remaining teeth. Brushing and flossing techniques were introduced using demonstrations. The dentinal caries in UR6, UL6, LL6 and LR8 were restored with light-cured composite (3M, Filtek, Z250XT Universal Restorative, USA). Endodontic treatment of UR5 was completed in a single visit and the coronal restoration was established with light-cured composite. Subsequently, full mouth scaling and polishing was carried out to improve the gingival condition, and the pre-surgical general dental care was completed with a prophylactic fluoride varnish (3M, Fast Release Varnish) application. Extra- and intra-oral clinical photographs and a set of articulated study models were kept as pre-surgical clinical records.
The upper arch study model was modified after discussion with the surgeon regarding the possible resection line to fabricate the surgical obturator. The technician was instructed to construct the surgical obturator from auto-polymerizing clear acrylic resin incorporating Adam's clasps on UR6, UR4 and UL6 and a C-shape wire clasp on UL5 for retention (Figure 4).
Figure 4. Surgical obturator (intaglio surface).
The surgical phase
The surgical resection was carried out through the socket rather than by sectioning between two standing teeth, in order to have a stronger bony support to the teeth adjacent to the defect. The bony excision margins were smoothed and covered with soft tissue. While considering the palatal resection margin, the hard palate was preserved as much as possible without compromising the tumour resection. Finally, at the completion of the surgery, a sterilized surgical obturator holding the surgical dressing, was inserted into the mouth. Since UR2 and UL5 were also removed during surgery, it was necessary to alter the surgical obturator prior to insertion by removing the wire clasp on UL5 and extending the surgical pack beyond the margins of the surgical obturator in order to cover the space at UR2 and UL5.
The post-surgical phase
After the surgery, the patient was prescribed 0.2% chlorhexidine mouthwash and advised to start brushing as soon as possible with a soft brush. A review appointment was arranged for 2 weeks following the surgery, at which time the defect was examined after removal of the surgical pack,
As the defect was healing, and the patient was tolerating the surgical obturator well, the fabrication of an interim obturator containing missing teeth was commenced. In the meantime, the surgical obturator was adjusted with a permanent soft reliner (UFI Gel VOCO, Germany) to prevent nasal leakage of fluid. Bite registration and a wax try-in was carried out prior to the delivery of the heat-cured acrylic interim obturator to the patient with instructions for insertion, removal and maintenance (Figure 5).
Figure 5. Interim obturator (intaglio surface).
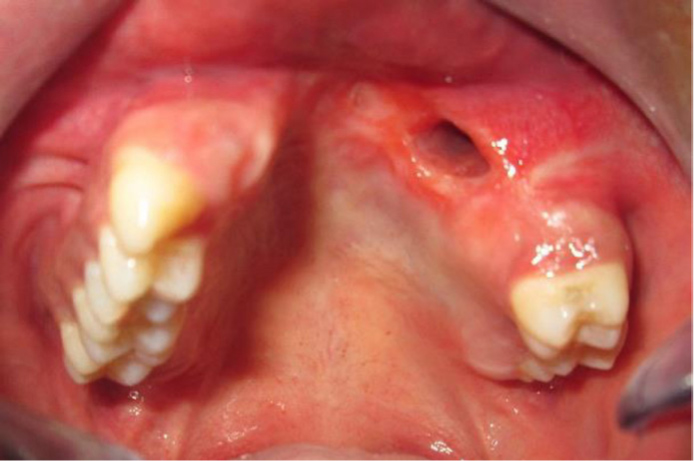
Subsequently, the interim obturator was reviewed at 2-weekly intervals during the first 6 months and then monthly for the adjustments and relining with a soft reliner for 1 year and 2 months. Thereafter the adjustment of the interim obturator was minimal and the oro-antral communication was small (Figure 6). It was then decided to deliver the definitive prosthesis.
Figure 6. Post-surgical defect.
The following options for the definitive prosthesis were discussed.
Surgical reconstruction of the oro-antral fistula and provision of the patient with a fixed-fixed conventional bridge incorporating pink porcelain to regain the soft tissue contour.
Surgical reconstruction of the soft tissue defect and the bony defect followed by provision of an implant-supported fixed partial denture.
Provision of a metal framework carrying the removable prosthesis to regain the soft tissue contour and to replace the missing teeth.
The first option was disregarded for many reasons. The patient's young age contraindicated crown and bridge work. Additionally, tooth preparation on vital teeth could endanger their vitality and, further, a fixed prosthesis would prevent the examination of the surgical site. The second option was set aside to be considered in the future, due to the chance of recurrence of the tumour.
Consequently, the upper arch study model was surveyed to design the metal framework to carry the various parts, while enhancing the retentive undercuts on UR6, UR7, UL6 and UL7 with light-cured composite (3M, Filtek, Z250XT Universal Restorative, USA).
The design of the metal framework was as follows:
A cingulum resting on UR3; embrasure rests on UR6, UR7 and UL6, UL7
A gingivally approaching I-bar clasp on UR3
Embrasure clasps on UR6, UR7 and UL6, UL7
A palatal major connector
Parallel guide planes on palatal surfaces of UR4, UR5, UR6, UL6 and mesial surfaces of UR3 and UL6
Thereafter, tooth preparation for rest seats and palatal guide planes according to the framework design, was carried out after obtaining informed written consent from the patient.
The guide planes were prepared free hand, on palatal and mesial surfaces as parallel to each other with the same angulation of a cylindrical diamond bur with the maximum possible height to achieve prepared indirect retention. The surveyed cast was kept nearby for comparison, to make sure that the bur was placed in the same relationship to the tooth as the analysing rod on the diagnostic cast. A light sweeping stroke was used to round off the buccal and the palatal proximal line angles of UR3 and UL6 as well as mesial and distal line angles of UR4, UR5, UR6 and UL6 while following the natural curvature of teeth, rather than slicing straight across the tooth.
Later, an alginate (Aroma Fine DF II, Fuji, Japan) impression was made and cast, surveying was carried out again to confirm the paralleling of the guide planes. A one-stage impression of the prepared mouth was then made with the light body and putty addition cure silicone (Express, 3M, USA) using an appropriate metal stock tray (Figure 7).
Figure 7. One-stage silicone impression following tooth preparation.
The technician was instructed to design the wax pattern for the cast framework on the master cast as planned previously, with the addition of a retentive meshwork to the side of the defect. Once the wax pattern was checked for accuracy, the technician was advised to process the metal framework. Then the cast metal framework was first tried on the master cast and then in the mouth for accuracy of complete seating and retention (Figure 8).
Figure 8. Upper occlusal view of the dentition with the metal framework.
Bite registration was carried out at the position of maximum intercuspation, and laboratory instructions were given to set the teeth in order to construct the wax trial obturator (Figure 9).
Figure 9. Wax trial obturator on the mounted casts.
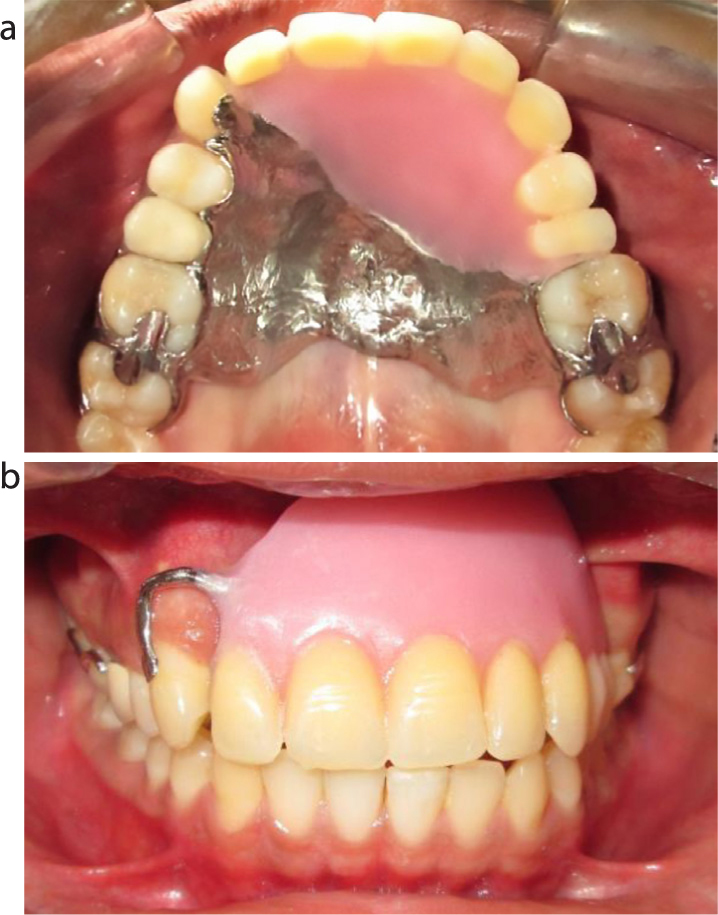
The wax try-in was checked extra-orally on mounted study casts and intra-orally for facial and dental aesthetics, retention, stability and occlusion. Since the outcome was satisfactory, it was processed as the final definitive removable prostheses with the metal framework carrying a heat-cured acrylic component in order to provide prosthetic reconstruction of the soft tissue defect and to restore the missing teeth (Figure 10).
Figure 10. (a) Upper occlusal view of the dentition with the definitive obturator. (b) Anterior view of the dentition with the definitive obturator (teeth in occlusion).
After fitting, the patient was pleased with the reconstruction of his facial appearance and routinely attended his 6-monthly review appointments to optimally maintain his oral hygiene and the condition of the prosthesis (Figures 11 and 12).
Figure 11. Front view of the face following maxillectomy.Figure 12. Patient after wearing the definitive obturator.
Discussion
A young patient affected with an ameloblastoma must pass through an exceptionally difficult journey that begins with the diagnosis of the tumour as they must follow multifarious treatment stages. Ultimately, it will have a major lifelong impact on the patient's psychological, physical and social wellbeing. The possible effects of maxillectomy surgery include:
Altered oral anatomy;
Loss of teeth and anatomical structures;
Significant scarring and bulky flaps;
Loss or alteration of sensation;
Trismus.
The presence of the defect can constantly and adversely remind the patient of theirs experience with the disease. Although survival is the primary concern of affected individuals at the stage of tumour diagnosis, later, following the surgery, the patient's concerns will shift towards the improvement and maintenance of their quality of life. The resulting defect of the maxillectomy, depending on the size, can be managed by primary surgical closure or reconstruction with a surgical flap or using a prosthetic obturation. Therefore, rehabilitation of a maxillary defect requires precise evaluation and planning by a multidisciplinary team, which must take place as soon as the tumour has been diagnosed.
The management planning for a patient awaiting a maxillectomy covers three phases:
The dental health of the patient is important. Therefore, every attempt must be taken to enhance the patient's oral condition by:
Allowing a complication-free recovery by treating active dental problems and eliminating the risk of occurrence of emergency dental problems;
Increasing the likelihood of the remaining teeth servig as adequate abutments for the obturator.3
Impressions and clinical photographs must be taken as pre-surgical records, since these will help to reconstruct the lost tissue to a normal or near normal state. The surgical obturator provides the surgeon with a scaffold to hold the surgical dressing. It also forms a barrier between the nasal and oral cavities without allowing the patient to feel the extent of the defect with their tongue and enables the patient to speak normally and to eat and drink without a nasogastric tube.3
During the surgical phase, close liaison must be made with the surgeon in order to propose a number of surgical interventions, which will aid in maximising the patient's future oral rehabilitation. Those include:
Preservation of ipsilateral and contralateral anterior teeth to the defect to be used in direct and indirect obturator retention.5
Preserving as much as possible of the hard palate without compromising tumour resection.
Placement of a split-thickness skin graft over the denuded surface of the facial flap
Placing the osteotomy cut through the extraction socket adjacent to the defect.
After surgery, the surgical obturator must be fixed in the mouth. Beumer6 suggested there should be no form of posterior occlusal contact with the surgical obturator at the side of the resection until the wound has healed.
The surgical obturator can be removed 7–10 days following surgery and impressions can be taken for the fabrication of the interim obturator.6 Once this has been delivered, the patient should be reviewed regularly every 2−4 weeks, since rapid soft tissue modifications will occur during the first 6−12 months after surgery.7 The patient should be advised to wear the obturator at all times and remove it only for cleaning, as an extended period without the obturator may result in difficulty in its re-insertion. The interim obturator may need significant modification, which may include modifying the bung with Viscose (Densply), Coe-Comfort (GC America), UFI Gel (VOCO Dental Products) or self-cure acrylic resin to improve its fit around the resection site.8 In this case, UFI Gel was used to modify the surgical obturator and to modify the bung of the interim obturator on subsequent follow-up visits.
Initially, patients who require prosthodontic post-surgical rehabilitation must be managed with conventional appliances.9 If this is not possible owing to anatomical obstructions, or if it was been tried and was unsuccessful, secondary implant-based prosthodontic management may be considered.9 In the case described, surgical correction of soft and hard tissue followed by provision of an implant-retained prosthesis, was set aside for future consideration.
It is sensible to begin the fabrication of the definitive obturator prostheses once monthly modifications of the interim obturator have become minimal, usually 6–12 months after the surgery.3 Maximum distribution of support, retention and stability are keys to the fabrication of a successful, removable prosthesis. It is advised to place multiple occlusal rests and palatal guide planes to effectively dissipate the vertical occlusal loading on the remaining teeth.3
Finally, it was possible to restore function and aesthetics for this young man to maintain his quality of life.
Conclusion
While maxillectomy will remove a tumour, post-operative aesthetics and functional problems will ultimately affect the social and psychological wellbeing of a patient. However, a maintained quality of life can be achieved with careful planning with the involvement of multidisciplinary team work.