Loomans B, Opdam N, Attin T Severe tooth wear: European Consensus statement on management guidelines. J Adhes Dent. 2017; 19:111-119 https://doi.org/10.3290/j.jad.a38102
Hemmings K, Truman A, Shah S, Chauhan R. Tooth wear guidelines for the BSRD part 1: aetiology, diagnosis and prevention. Dental Update. 2018; 45:483-495 https://doi.org/10.12968/denu.2018.45.6.483
Varma S, Preiskel A, Bartlett D. The management of tooth wear with crowns and indirect restorations. Br Dent J. 2018; 224:343-347 https://doi.org/10.1038/sj.bdj.2018.170
Mehta SB, Banerji S, Millar BJ, Suarez-Feito JM. Current concepts on the management of tooth wear: part 4. An overview of the restorative techniques and dental materials commonly applied for the management of tooth wear. Br Dent J. 2012; 212 https://doi.org/10.1038/sj.bdj.2012.137
Davies S, Gray R, Whitehead S. Occlusion: good occlusal practice in advanced restorative dentistry. Br Dent J. 2001; 191
Van't Spijker A, Rodriguez JM, Kreulen CM Prevalence of tooth wear in adults. Int J Prosthodont. 2009; 22:35-42
White DA, Tsakos G, Pitts NB Adult Dental Health Survey 2009: common oral health conditions and their impact on the population. Br Dent J. 2012; 213:567-572 https://doi.org/10.1038/sj.bdj.2012.1088
Bartlett D, Varma S. A retrospective audit of the outcome of composites used to restore worn teeth. Br Dent J. 2017; 223 https://doi.org/10.1038/sj.bdj.2017.583
Aristidis GA, Dimitra B. Five-year clinical performance of porcelain laminate veneers. Quintessence Int. 2002; 33:185-189
Valderhaug J, Jokstad A, Ambjørnsen E, Norheim PW. Assessment of the periapical and clinical status of crowned teeth over 25 years. J Dent. 1997; 25:97-105 https://doi.org/10.1016/S0300-5712(96)00008-5
Saunders WP, Saunders EM. Prevalence of periradicular periodontitis associated with crowned teeth in an adult Scottish subpopulation. Br Dent J. 1998; 185:137-140 https://doi.org/10.1038/sj.bdj.4809750
Bergenholtz G. Iatrogenic injury to the pulp in dental procedures: aspects of pathogenesis, management and preventive measures. Int Dent J. 1991; 41:99-110
Smales RJ, Berekally TL. Long-term survival of direct and indirect restorations placed for the treatment of advanced tooth wear. Eur J Prosthodont Restor Dent. 2007; 15:2-6
Lucarotti PSK, Burke FJT. The ultimate guide to restoration longevity in England and Wales. Part 9: incisor teeth: restoration time to next intervention and to extraction of the restored tooth. Br Dent J. 2018; 225 https://doi.org/10.1038/sj.bdj.2018.1025
Milosevic A. The survival of zirconia based crowns (Lava) in the management of severe anterior tooth wear up to 7-years follow-up. Oral Biol Dentistry. 2014; 2
Mesko ME, Sarkis-Onofre R, Cenci MS Rehabilitation of severely worn teeth: a systematic review. J Dent. 2016; 48:9-15
Restoration of severe localized tooth wear with zirconia-reinforced lithium silicate: A case report Anurag Srinivas Gareth Brock Dental Update 2024 47:11, 707-709.
Authors
AnuragSrinivas
DCT 2 in Restorative Dentistry, Birmingham Dental Hospital
Tooth wear is becoming an increasingly common cause for referral to restorative dentistry departments in the UK. Often, these cases are treated with resin-bonded composite direct restorations in the first instance. This article presents a case of 23-year-old patient who was treated using zirconia-reinforced lithium disilicate restorations.
CPD/Clinical Relevance: In certain cases, indirect restorations can be considered a first-line treatment, based on the presentation and patient factors. Each case should be evaluated on its own merits and careful consideration should be given to the evidence base and its relevance.
Article
Non-carious tooth wear (TW) is a common reason for referral to restorative dentistry departments in UK dental hospitals. Following implementation of appropriate preventive strategies, localized anterior TW cases are commonly treated with direct composite resin restorations in the first instance.1 We present a case of a 23-year-old woman who presented with severe localized TW of the maxillary anterior sextant, treated with an alternative management strategy.
Case report
Patient SP is a 23-year-old female who was referred by her GDP regarding severe TW. SP's main concerns were increasing hypersensitivity of her maxillary anterior teeth, and poor aesthetics.
The patient had suffered from an illness in her late teens leading to daily vomiting for almost 2 years. Gastroenterological investigation indicated that certain foods were causing the vomiting. Appropriate preventive strategies were implemented and the patient's vomiting is now rare.
On presentation, teeth in the maxillary anterior sextant were severely worn, through to dentine, labially and palatally. The wear lesions appeared to be erosive in nature with a pseudo-chamfer ring of enamel present, cervically, around the teeth. Mild TW consistent with erosive ‘cupping’ lesions were noted in the premolar regions in both arches. The TW could be considered pathological as the amount of wear caused concern for the patient and the wear progressed quickly in comparison to SP's age.2 Periodontally, there were only localized areas of bleeding on probing in two of the sextants. There was no pathological pocketing and no evidence of active periodontal disease. Her basic periodontal examination (BPE) scores were:
The patient had a class 1 static occlusion. Dynamic occlusal analysis showed canine guidance on the left-hand side and group function on the right-hand side. There was minimal posterior disclusion on protrusive excursions.
In light of the presentation of the lesions in this case, and after discussing all the options available with the patient, indirect restorations were chosen as the first-line treatment. The wear lesions appeared similar to the tooth preparations required for dentine-bonded crowns, therefore, a minimal amount of further tooth preparation would be required to permit for indirect restorations. The patient did not wish to consider metal–ceramic restorations owing to aesthetic concerns and so, ceramic restorations were used.
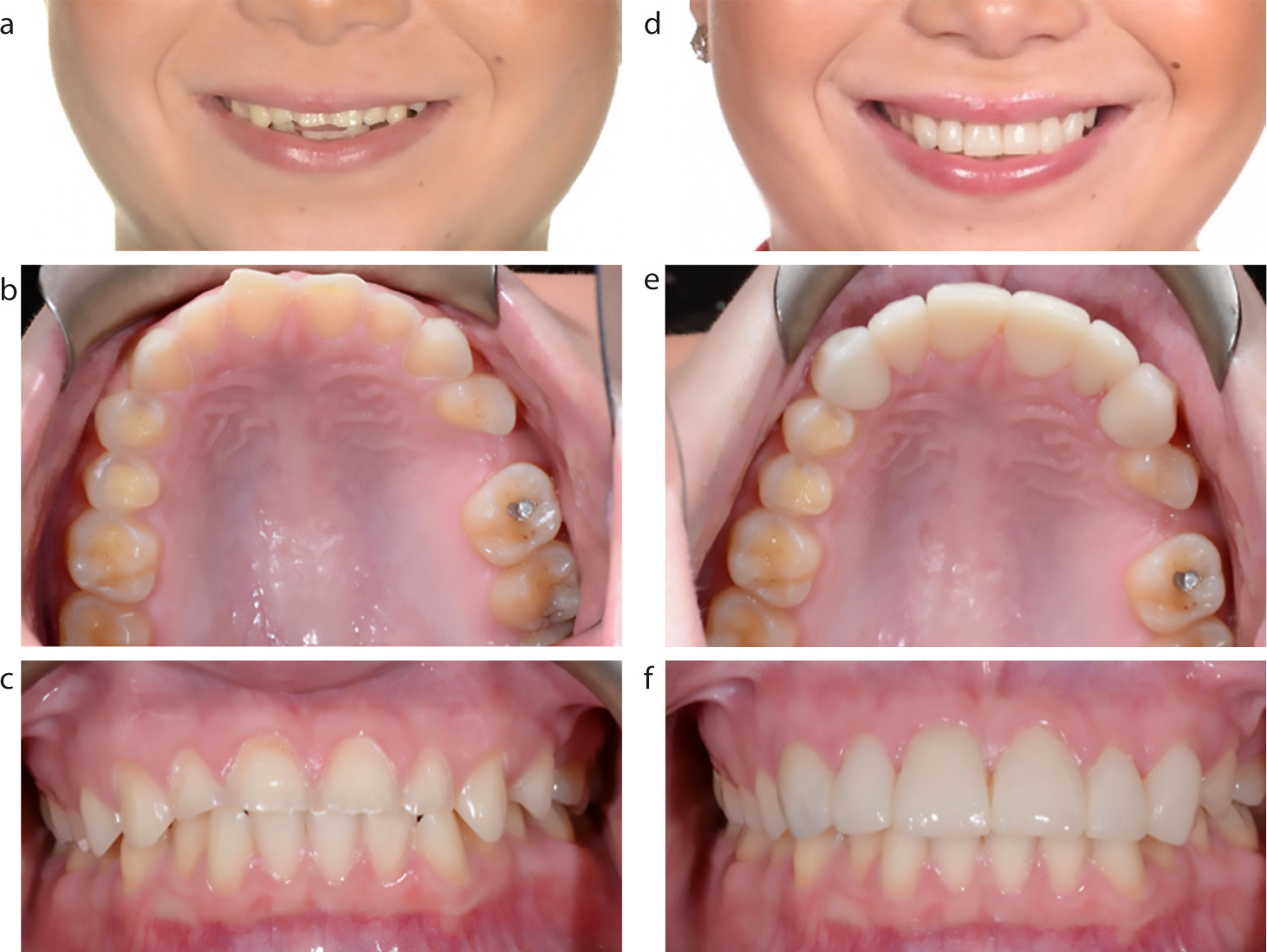
Figure 1. Intra-oral photograph following minimal tooth preparations.Figure 2. Provisional restorations.Figure 3. (a–f) Pre- and post-operative images.
Articulated study models demonstrated that there was insufficient space to accommodate the ceramic restorations, palatally. In this case, the occlusal vertical dimension (OVD) was increased marginally opposed to greater palatal tooth reduction, which may have led to an increased risk of iatrogenic damage to the teeth. The teeth were going to be allowed to ‘Dahl’ into the new occlusion.3,4 Lab-made diagnostic wax-ups, mimicking the definitive restorations, were used to create fixed bis-acryl composite resin provisional restorations. These were trialled for 6 weeks to assess the patient's ability to adapt to the altered occlusion, increased OVD and aesthetics.4,5 Adjustments were made to the provisional restorations and replicated in the definitive ceramic restorations.
Zirconia-reinforced lithium silicate (ZLS) restorations (Celtra Press, Dentsply Sirona) were used to restore the teeth, definitively. The restorations were successful in meeting the patients' aesthetic expectations, while also providing predictable and functional restoration of the erosive lesions.
Diagnoses
Pathological tooth wear with a primarily erosive aetiology
Mild localized gingivitis
Treatment options
Direct/indirect composite restorations
Indirect ceramic restorations
Indirect metal–ceramic restorations
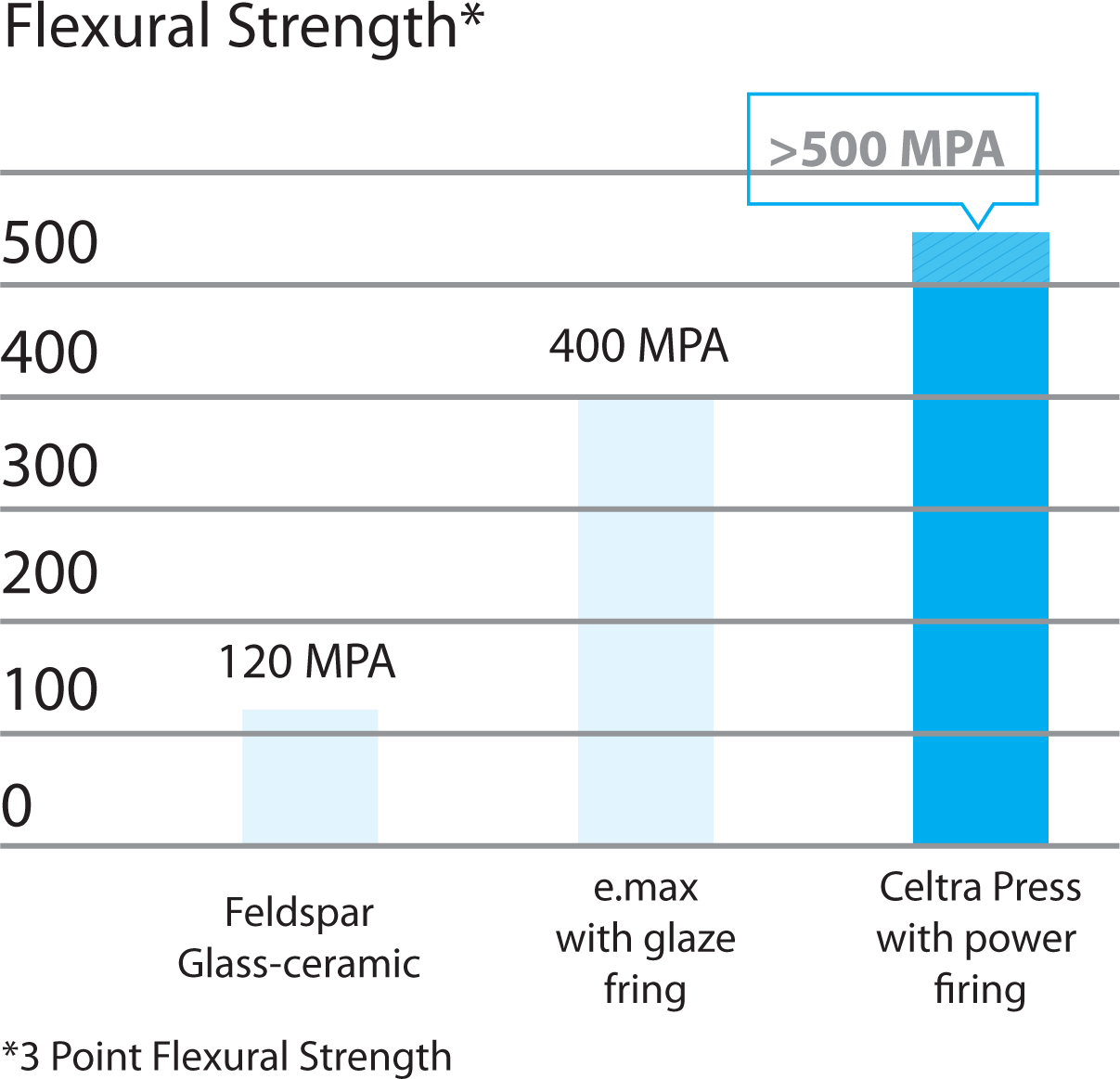
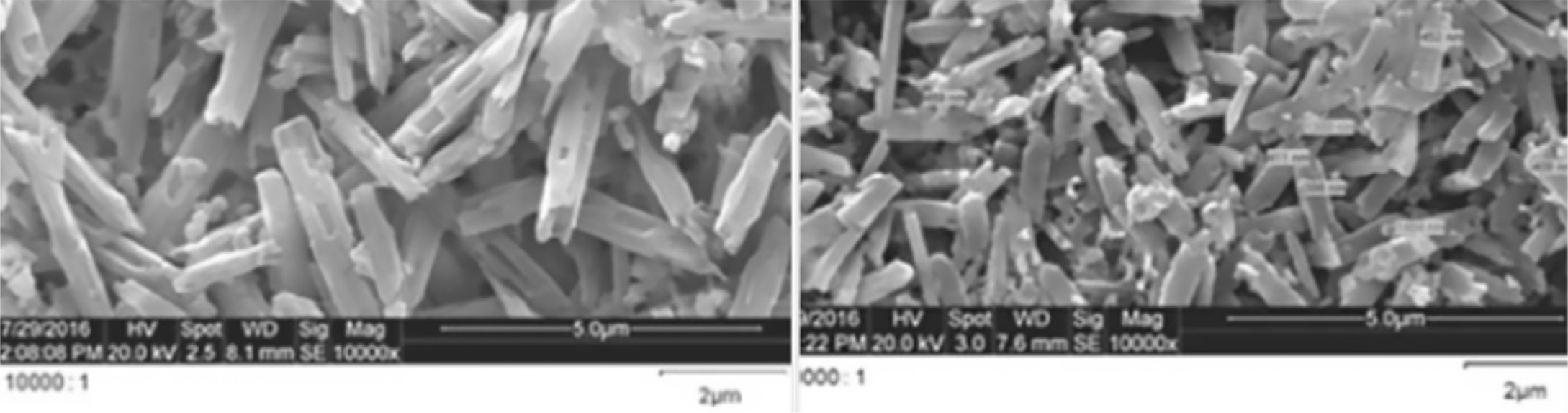
ZLS is a ceramic material that is becoming increasingly available. It is superior in terms of flexural strength compared to lithium disilicate (LS2) restorations (Figure 4).6 ZLS has a finer microstructure once pressed in comparison to LS2 (Figure 5), which allows for a superior finish when polished.6
Figure 4. Flexural strength of Celtra Press compared to emax and feldspathic porcelain. (Supplied by Dentsply, Sirona.)Figure 5. Microstructure of lithium disilicate (left) and celtra press (right). (Reproduced with permission from Dentsply, Sirona.)
Tooth wear is a common reason for referral to secondary care. The prevalence of severe TW is reported to be 3% in 20 year olds, increasing to 17% in 70 year olds.1,7 The Adult Dental Health Survey 2009 indicated that the prevalence of signs of anterior TW was 77% compared to 66% in 1989.8 Localized anterior TW cases are commonly treated with preventive strategies and direct resin-bonded composite restorations (RBCs).1Table 24,9 displays some of the considerations that were taken into account before deciding to use indirect restorations in this case. Metal–ceramic restorations were not discussed in this case, due to SP's wishes.
Composite
Ceramic
Advantages
Disadvantages
Advantages
Disadvantages
Non-invasive
Aesthetically inferior to ceramic restoration
Superior aesthetics
Require tooth reduction
Useful as provisional restorations
Polymerization shrinkage that could cause marginal leakage
Improved wear resistance
Brittle and prone to fracture
Well tolerated by pulp
Staining
Well tolerated by gingival tissues
Higher failure rates among patients with parafunctional habits
Simple to repair/modify
Accelerated wear rate/risk of bulk fracture
Improved marginal adaptation reducing the risk of leakage (anecdotal)
Potentially abrasive to the opposing dentition
Restorations may be applied within a single visit
Operator and technique sensitive
ZLS tooth reduction requirement is only 0.4–0.6 mm
Difficult to repair/adjust
At least 2-mm thickness required in occlusally loaded areas; bulky and unaesthetic
Potentially more catastrophic failure
Require comprehensive planning and trial, prior to definitive restoration
A success rate of 90% over a period of 5 years has been reported for ceramic restorations in the anterior segment.4,10 Valderhaug and Jokstad11 found that 92% of vital teeth that were crowned remained free from pulpal damage at 10 years. The authors advise that careful assessment of the status of pulp vitality prior to treatment is crucial to long-term success.
Saunders and Saunders12 found 19% of vital teeth that were prepared for crowns showed signs of periradicular disease. They concluded that pulpal damage might occur during crown preparation and recommended regular radiographic review. Their paper did, however, suggest many of these preparations were for porcelain bonded to metal crowns and proposed that the increasing popularity of resin-bonded crowns may allow for a more conservative preparation, mitigating this risk. Aside from the amount of dentine removal that takes place, they also point to inadequate cooling and faulty or worn equipment during preparation, as possible threats to pulp vitality. Bergenholtz13 suggested the term ‘dentinogenic injury,’ to describe iatrogenic damage to the pulp during tooth preparation.
Over 10 years, Smales and Berekally14 noted survival estimates of 58.9% for anterior RBCs and 70.3% for anterior ceramic restorations. Their study examined a small sample and the indirect restorations were metal–ceramic. It is noted that failure of indirect restorations could be more catastrophic and require more extensive treatment than cases of failed RBCs. This was attributed to the preparation needed for the indirect restorations. Lucarotti and Burke15 had similar findings when they assessed the time to re-intervention and time to extraction of approximately 2.5 million restorations of incisor teeth. They found that in incisor teeth, crown restorations lasted longest before requiring re-intervention. However, the lifespan of these teeth was shorter than those that were restored with RBCs or veneers.
Milosevic16 reported a mean survival time of 74 months for zirconia crowns used to restore severely worn anterior teeth. The data suggested risk of failure was correlated with an edge-to-edge occlusion; the presence of a bruxism habit or evidence of attrition. The risk of failure did not appear to be correlated with an increase in occlusal vertical dimension (OVD) using the Dahl approach. In the case of SP, erosion appeared to be the primary factor in tooth surface loss and there was no history of bruxism. The Dahl approach was used to increase the OVD to make space for the restorations.
In the case of SP, much of the tooth preparation had already been completed, pathologically, through erosion. The mechanical properties of ZLS allow for it be used to great effect in thin sections. As illustrated, a very minimal amount of further preparation was required to accommodate the ZLS restorations. Owing to the degree of erosion, the authors do not believe the risk to pulpal health was greatly increased by the minimal preparation. Comprehensive assessment of pulpal health was undertaken. Adequate cooling was used throughout and we believe the treatment was carried out to a high standard. The resources were available in the dental hospital to provide a high strength and relatively minimally invasive indirect full coverage restoration to meet the patient's demands.
Treatment plan
Oral hygiene instruction, tooth brushing instruction, diet assessment and advice
Ceramic restorations of UR3 to UL3
Re-assess and consider restoration of UR4, UL4 +/- options to replace UL5 space in primary care
Maintenance
The evidence shows that crowns in the anterior region can perform comparably to RBCs. They require less maintenance over time; however, they may reduce the longevity of a tooth. It should be considered that many of the studies assessed metal–ceramic restorations and few were limited to patients suffering from erosive TW. It is thought that iatrogenic pulpal damage during tooth preparation is the primary cause for higher rates of catastrophic failures. In cases such as SP, where the erosive wear presents at a later stage, the risk of pulpal damage is not greatly increased post-operatively, when a minimal preparation design is followed.
Conclusions
The European Consensus1 recommends that patient's wishes should be a factor in decision-making and it is crucial to gain valid consent for any treatment plan. For this reason, Mesko et al17 endorse the inclusion of crowns as a legitimate treatment option. Patients must be given detailed explanations of each option and counselled about the long-term implications of each option.
In the case of SP, the aesthetic expectations were high and there was a desire for as minimal long-term maintenance as possible. Aesthetically, the ZLS restorations were successful in meeting the patients' expectations while providing predictable and functional restoration of the erosive lesions. SP was happy with the outcome.
The authors suggest that in similar cases, with patients who have significant erosive lesions in the anterior sextant, indirect restoration with ZLS may provide an alternative first-line aesthetic management strategy.