Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference. Official Records of the World Health Organization. 1948; 19456:(2)
Knutson JW, Klein H, Palmer CE. Dental needs of grade-school children in Hagerstown, MD. J Am Dent Assoc. 1940; 41:579-588
Locker D. Measuring oral health: a conceptual framework. Community Dent Health. 1988; 5:3-18
Locker D, Miller Y. Evaluation of subjective oral health status indicators. J Public Health Dent. 1994; 54:167-176
Regulations 1990.P3 London: HMSO;
Yewe-Dyer MR. The definition of oral health. Br Dent J. 1993; 174:224-225
Oral Health Strategy Group. An oral health strategy for England. 1994. https://tinyurl.com/yxm3dqqe (accessed October 2020)
Glick M, Williams DM, Kleinman DV A new definition for oral health developed by the FDI World Dental Federation opens the door to a universal definition of oral health. J Am Dent Assoc. 2016; 147:915-917
Glick M, Williams DM, Kleinman DV A new definition for oral health developed by the FDI World Dental Federation opens the door to a universal definition of oral health. Br Dent J. 2016; 221:792-793
Lamster IB. Defining oral health: a new comprehensive definition. Int Dent J. 2016; 66:321-323
Burke FJT, Wilson NHF. Measuring oral health: an historical view and details of a contemporary oral health index (OHX). Int Dent J. 1995; 45:358-370
Cvar JF, Ryge G. Reprint of criteria for the clinical evaluation of dental restorative materials. 1971. Clin Oral Investig. 2005; 9:215-232
Hickel R, Roulet JF, Bayne S Recommendations for conducting controlled clinical studies of dental restorative materials. Science Committee Project 2/98 – FDI World Dental Federation study design (Part I) and criteria for evaluation (Part II) of direct and indirect restorations including onlays and partial crowns. J Adhes Dent. 2007; 9:121-147
Marquillier T, Doméjean S, Le Clerc J The use of FDI criteria in clinical trials on direct dental restorations: a scoping review. J Dent. 2018; 68:1-9
Ainamo J, Barnes D, Beagrie G Development of the World Health Organization (WHO) Community Periodontal Index of Treatment Needs (CPITN). Int Dent J. 1982; 32:281-291
Caton JG, Armitage G, Berglundh T A new classification scheme for periodontal and peri-implant diseases and conditions. Introduction and key changes from the 1999 classification. J Clin Periodontol. 2018; 45:S1-S8
Dietrich T, Ower P, Tank M Periodontal diagnosis in the context of the 2017 classification system of periodontal diseases and conditions: implementation in clinical practice. Br Dent J. 2019; 226:16-22
Milward MR, Roberts A. Assessing periodontal health and the British Society of Periodontology implementation of the new classification of periodontal diseases 2017. Dent Update. 2019; 46:918-929
Pitts NB, Stamm J. International Consensus Workshop on Caries Clinical Trials (ICW-CCT) final consensus statements: agreeing where the evidence leads. J Dent. 2004; 83:125-128
Pitts NB. ICDAS: an international system for caries detection and assessment being developed to facilitate caries epidemiology, research and appropriate clinical management. Community Dent Health. 2004; 21:193-198
Shivakumar KM, Prasad S, Chandu GN. International caries detection and assessment system: a new paradigm in detection of dental caries. J Conserv Dent. 2009; 12:10-16
Smith BGN, Knight JK. An index for measuring the wear of teeth. Br Dent J. 1984; 156:435-439
Bartlett D. A proposed system for screening tooth wear. Br Dent J. 2010; 208:204-209
Holt VP. Patient satisfaction questionnaires – how to do them successfully. Dent Update. 2006; 33:338-346
McDowell I, Newell C. Measuring health. A guide to rating scales and questionnaires.Oxford: Oxford University Press; 1996
The evaluation of Canadian dental health. A system for recording and statistical analysis at the community, provincial and national level.Toronton: Canadian Dental Association; 1959
Lambert C, Freeman E. The Clinic Habit.Newhaven, CT, USA: College and University Press; 1967
Bulman JS, Richards ND, Slack GL, Willcocks AJ. Demand and need for dental care: a sociodental study.London: Oxford University Press; 1968
Carr W, Wolfe S. Unmet need for dental services. Working paper.: Centre for Health Care Research Meharry Medical College; 1975
Nikias MK, Sollecito WA, Fink R. An oral health index based on ranking of oral status profiles by panels of dental professionals. J Public Health Dent. 1979; 39;:16-26
Marcus M, Koch AL, Gershen J.A. An empirically derived measure of oral health status for adult populations. J Public Health Dent. 1980; 40:334-343
Marcus M, Koch AL, Gershen JA. A proposed index of oral health status: a practical application. J Am Dent Assoc. 1983; 107:729-733
Ireland RS, Jenner AM, Williams MJ, Tickle M. A clinical minimum data set for primary dental care. Br Dent J. 2001; 190:663-667
Mann J, Sgan-Cohen HD, Asher RS Treatment need index: a pilot study. Int Dent J. 1993; 43:129-134
Hede B. Oral health in Danish hospitalized psychiatric patients. Comm Dent Oral Epidemiol. 1995; 23:44-8
Witter DJ, Cramwinckel AB, van Rossum GMJM, Kayser AF. Shortened dental arches and masticatory efficiency. J Dent. 1990; 18:185-189
Burke FJT, Greene PR, Roberts C. Reproducibility studies on a newly designed Index of oral health. J Dent Res. 1994; 73
Burke FJT, Busby M, McHugh S Evaluation of an oral health scoring system by dentists in general dental practice. Br Dent J. 2003; 194:213-218
Burke FJT, Busby M, McHugh S A pilot study of patients' views of an oral health scoring system. Primary Dent Care. 2004; 11:37-39
Busby M, Burke FJT, Matthews R Measuring oral health as part of a concise patient survey. Br Dent J. 2012; 213:1-5
Denplan Excel Training Manual.Winchester: Denplan;
Rooney E. Risk driven care pathways in publicly funded care. In: Chapple ILC, Papapanou PN (eds). : Springer; 2020
Scottish Dental Clinical Effectiveness Programme (SDCEP). Oral health assessment and review: guidance in brief. 2011. https://tinyurl.com/y2wr273v (accessed Ocober 2020)
Chapple L, Yonel Z. Oral health risk assessment. Dent Update. 2018; 45:841-847
An independent review of NHS Dental Services in England. 2009. https://tinyurl.com/yxhdtuzt (accessed October 2020)
Newton JT, Asimakopoulou K. The perceived acceptability of the DEPPA patient assessment tool: a questionnaire survey of Denplan Excel patients. Br Dent J. 2017; 222:767-770
Asimakopoulou K, Newton JT, Daly B The effects of providing periodontal disease risk information on psychological outcomes: a randomized controlled trial. J Clin Periodontol. 2015; 42:350-355
Asimakopoulou KG, Nolan M, McCarthy CCL, Newton JT. The effect of risk communication on periodontal treatment outcomes; a randomized controlled trial. J Periodontol. 2019; 90:948-956
Lucarotti PSK, Burke FJT. Patient history as a predictor of future treatment need? Considerations from a dataset containing over nine million courses of treatment. Br Dent J. 2020; 228:345-350
Peres MA, Macpherson LMD, Weyant RJ, Daly B Oral disease: a global health challenge. Lancet. 2019; 394:249-260
The ability to measure oral health is central to successful, patient-oriented clinical practice. In this regard, there have been a variety of definitions of oral health over the years, with the most recent being one by the FDI. Specific quality measures have been designed to assess, for example, the technical excellence of restorations, periodontal health, tooth wear, and, depth of caries (e.g. ICDAS). However, a single index that would produce a composite score of oral health could be considered desirable and the ideal criteria for this are discussed, namely, that it should be reproducible and valid, readily understood and capable of being used by dentists with minimal instruction and training. The profession has now entered the era of personalised medicine where risk factors need to be identified and patients educated about these, thus empowering them to work with their care provider and at home to take responsibility for their own dental health. As a result, a variety of oral health assessments, which include assessments of risk factors, have now become available: examples of these are described, with suggestions regarding the implementation of such into a clinician's practice being given.
CPD/Clinical Relevance: The ability to measure oral health is central to successful clinical practice.
Article
What is oral health?
The World Health Organization1 describes health in holistic terms as ‘a state of complete physical, mental and social wellbeing and not merely the absence of disease or infirmity’. This definition is broader than our traditional definitions of health, including patient-centred outcomes, which, in dentistry, we capture using quality-of-life measures and patient-reported outcomes. However, historically, dental health, and more recently, oral health has been measured in a number of ways. A common method of describing dental health was the DMFT or DMFS index (decayed missing and filled teeth or surfaces).2 However, this measure has been considered to have limitations (Table 1).
Components are not qualitatively similar and do not reflect the relative success of treating disease
Does not reflect the functional state and perceived health status
M component may be an unreliable indicator of caries
In adults, DMFT becomes saturated
Sealant restorations in children may not show up on the index
Questions regarding the accuracy of measuring caries
Disease may be unreported without radiographs
Many such measures of oral conditions do not assess their impact on a patient's quality of life, and, increasingly the drive is to record socio-dental indicators, defined by Locker as ‘measures of the extent to which dental and oral disorders disrupt normal role functioning’ should be applied.3 A study by Locker and Miller examined eight subjective oral health status indicators: the ability to chew and speak; oral pain and symptoms; ease of eating and communication; impact on daily life and worry/concern about appearance or health of teeth or mouth.4 The results indicated that it may be possible to identify populations in need of treatment and prevention using subjective indicators alone. However, it is the view of the principal author that examination of a patient (and speaking with them) is essential to measure their oral health. This is particularly pertinent in the COVID-19 era, where the role of remote consultations has a place, but may not facilitate the formulation of a diagnosis.
There have been a variety of definitions of oral health over the years. Traditionally, oral health was defined as an absence of disease. However, this fails to recognize the relevance of a patient's values and expectations. A 1990 definition5 was the first to link oral health with general health, with oral health being defined as: ‘such a standard of health of the teeth, their supporting structures and any other tissues of the mouth, and of dental efficiency, having regard to the need to safeguard general health’.
This definition could be criticized, given that many conditions relating to teeth may be detrimental to oral health, but not general health, for example, chipped or worn teeth. An alternative definition was put forward by Yewe-Dyer,6 and was the first to suggest that dental appearance was involved in oral health and that prevention was relevant:
‘Oral health is the state of the mouth and associated structures where disease is contained, future disease is inhibited, the occlusion is sufficient to masticate food and the teeth are of a socially acceptable appearance’.
In ‘An Oral Health Strategy for England’ the Oral Health Strategy Group publication, oral health was defined as:7
‘A standard of health of the oral and related tissues which enables an individual to eat, speak and socialize without active disease, discomfort or embarrassment and which contributes to general wellbeing’.
Most recently, the FDI World Dental Federation has proposed a universal definition of oral health,8 considering that a definition was needed that included the full scope of oral health and wellbeing, and, ultimately, a definition that could be agreed by all. They consider that the new definition acknowledges the multifaceted nature of oral health, as follows:
‘Oral health is multifaceted and includes the ability to speak, smile, smell, taste, touch, chew, swallow and convey a range of emotions through facial expressions with confidence and without pain, discomfort and disease of the craniofacial complex’.
They add that further attributes of oral health include:
It is a fundamental component of health and physical and mental wellbeing. It exists along a continuum influenced by the values and attributes of people and communities;
It reflects the physiological, social and psychological attributes that are essential to the quality of life;
It is influenced by the person's changing experiences, perception, expectations and ability to adapt to circumstances.
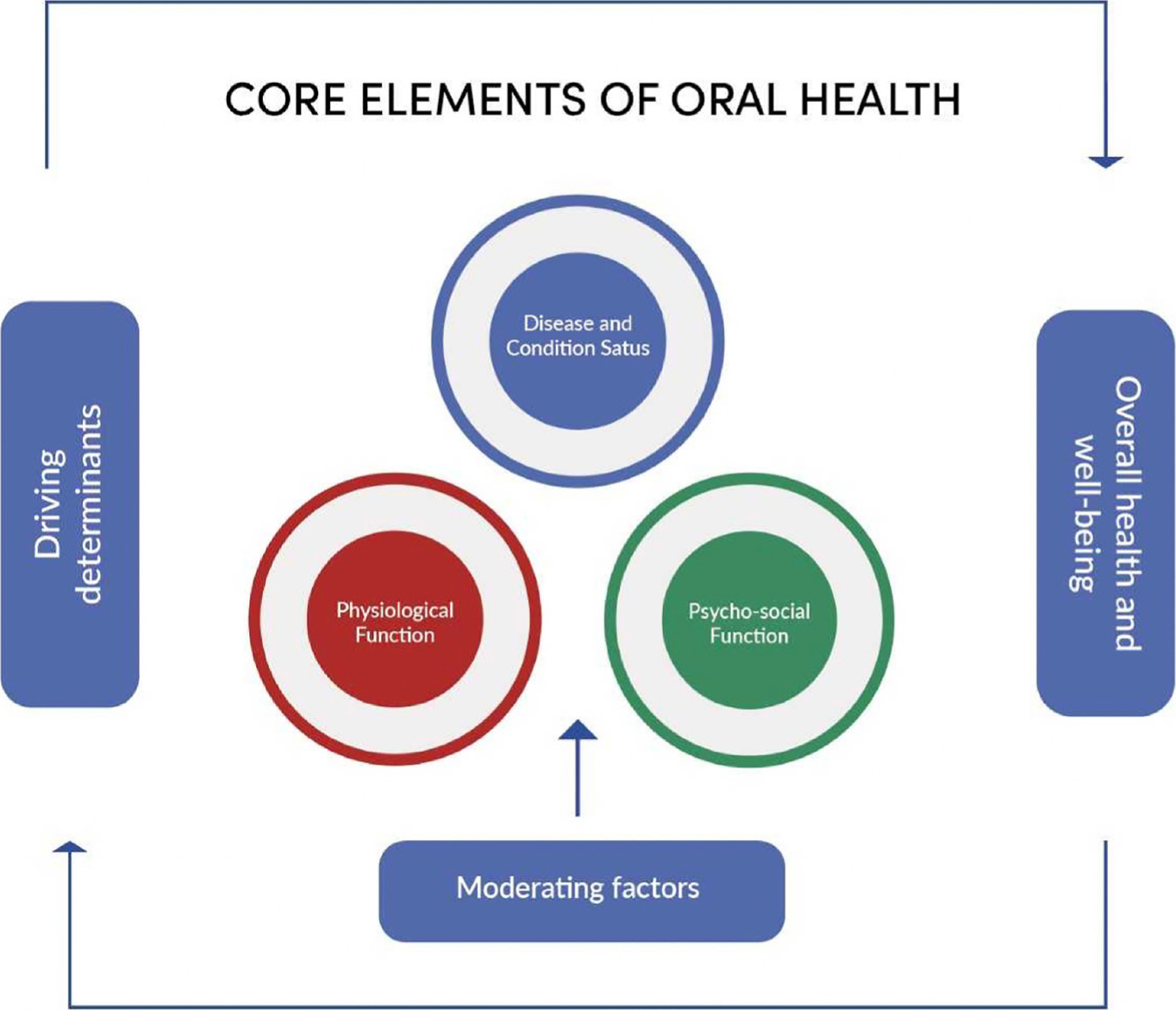
The FDI, which represents more than one million dentists in more than 100 countries, represents dentistry at the World Health Organization. The new definition, which resulted from consultations with many stakeholders (such as patients, practising dentists, researchers and politicians) is intended to be used by all stakeholders and has been considered a definition that will enable common understanding when addressing the needs of communities, and when making a case for the importance of optimal oral health.9 The FDI has published moderating factors for their definition (Figure 1), with the following being taken verbatim from the caption for this illustration which has been adapted from that in Glick et al.8
Figure 1. Framework for oral health. Adapted from Glick et al.8
The core elements of oral health are as follows: disease and condition status refers to a threshold of severity or a level of progression of disease, which also includes pain and discomfort; physiological function refers to the capacity to perform a set of actions that include, but are not limited to, the ability to speak, smile, chew, and swallow; and psychosocial function refers to the relationship between oral health and mental state that includes, but is not limited to, the capacity to speak, smile, and interact in social and work situations without feeling uncomfortable or embarrassed. Driving determinants are factors that affect oral health and cover five main domains: genetic and biological factors, social environment, physical environment, health behaviors, and access to care. In turn, driving determinants nest within systems that can support or serve as a barrier to maintaining and promoting oral health and managing oral diseases and conditions. Moderating factors are elements that determine or affect how a person scores his or her oral health and include, but are not limited to, age, culture, income, experience, expectations, and adaptability.
This new definition is not without critics. For example, it has been considered by Lamster and co-workers10 to set a challenge, given its breadth, potentially including quantitative measures such as periodontal status, qualitative measures (quality of life) and summative activities (chewing and smiling). These workers also considered that different definitions will need to be developed for different age groups, as the definition will change over the course of life.
Measuring oral health: why bother?
The ability to measure oral health is central to successful, patient-orientated clinical practice and the importance of measuring oral health may be considered from three viewpoints, namely: national, patient and professional. In more detail:11
From a national point of view, it is important for government and the public sector to determine the direct costs of healthcare provision and manpower needs, and also to direct resources to promote a healthy population by increasing access to care and reducing health inequalities;
From a patient (or consumer) viewpoint, measuring oral health is important because it enables them to understand the nature and extent of their oral health and empowers them to make decisions on the actions they will take to prevent future disease. A measure of oral health could be considered to motivate a patient to improve their score (for example, ‘your score is presently 60% but you should be aiming for 80% by improving your oral hygiene’) and enable them to monitor the progress made.
From the dental professional's point of view, it may be considered that they should be interested in quality control (for example, how long do their restorations survive, for example, or what proportion of their patients lose teeth), audit and clinical governance (which is an essential aspect of a professional's life), professional satisfaction (knowing how well their treatments perform), the effect of advice and/or treatment (does this improve an oral health score), and research.
It may therefore be concluded that measuring oral health is important and that one measure that can be adapted to these various roles would be useful.
Specific quality measures
Businesses often measure quality aspects, such as failure or reject rates, the level of product returns and customer satisfaction (usually measured by a survey). There are many measures for dental quality assessment relating to individual characteristics of overall oral health. These include the following.
Technical excellence of restorations
A commonly used method for assessing the adequacy of individual restorations has been the United States Public Health Service (USPHS) classification, initially described by Ryge.12 This produced a measure for each of five (although some variants of this measure more) aspects of restoration adequacy (Table 2). The authors consider that this is a relatively simple method that may have value in dental practice for the purpose of, for example, clinical audit of various aspects of restorations. This systematic methodology, also described in the present issue (pp 823–828), has served dental researchers well, despite suggestions that it should be replaced by the more comprehensive scheme devised by Hickel and colleagues,13 because changes over time are not easily detected by the limited sensitivity of the Ryge criteria, and that more scientific rigour was needed. Ten years after the introduction of the new criteria, results from a scoping review indicated that its uptake was not universal, with only 50% of clinical research studies using these criteria, while 16.3% of the studies used FDI criteria in the time period for 10 years from 2010.14
Criteria
Anatomical form
A: Restoration is continuous with existing anatomical form, not under contoured
B: Restoration is under contoured but no dentine or base exposed
C*: Sufficient restorative material is missing so that dentine or base is exposed
Margin integrity
A: No visible evidence of a crevice along the margin into which a probe will catch
B: Probe catches in a crevice along the margin, no exposure of dentine or base
C*: Visible evidence of a crevice with exposure of dentine or base along the margin
Indices were developed for the assessment of periodontal disease at a population survey level, such as the Community Periodontal Index of Treatment Need (CPITN),15 in which status codes are equated with treatment need. In 1986, the British Society of Periodontology developed the Basic Periodontal Examination (BPE) from the CPITN, and several iterations followed in 1994, 2000 and 2011. It was updated in 2019 following the 2017 World Workshop Classification of Periodontal Diseases (www.bsperio.org.uk/assets/downloads/BSP_BPE_Guidelines_2019.pdf), to create a journey from BPE screening, through clinical investigations, to diagnosis and ultimately classification as the final step. This classification step involves the staging of disease into stages I, II, III and IV (mild, moderate, severe and very severe) and ‘grading’ of disease to capture its rate of progression and, therefore, risk of tooth loss if untreated (grades A, B and C). The full classification system is summarized by the workshop introductory publication,16 adapted for the UK healthcare system in 201917 and summarized for Dental Update readers by Milward and Roberts.18
The International Caries Detection and Assessment (ICDAS) system19,20
ICDAS presents a technique for the classification of dental caries developed from systematic reviews on the clinical caries detection system and other sources.18 In this, the ICDAS codes for coronal caries range from 0 to 6, depending on the severity of the lesion. A detailed description of each of the codes is given under the following headings, to assist in the training of examiners in the use of ICDAS: pits and fissures; smooth surface (mesial or distal); free smooth surfaces and caries associated with restorations and sealants (CARS). However, the basis of the codes is essentially the same throughout (Table 3).
Code
Description
0
Sound
1
First visual change in enamel (seen only after prolonged air drying or restricted to the confines of a pit or fissure)
2
Distinct visual change in enamel
3
Localized enamel breakdown (without clinical visual signs of dentinal involvement)
4
Underlying dark shadow from dentine
5
Distinct cavity with visible dentine exposed (may require debris removal)
6
Extensive distinct cavity with visible dentine (involving ≥50% of tooth)
Tooth wear assessments
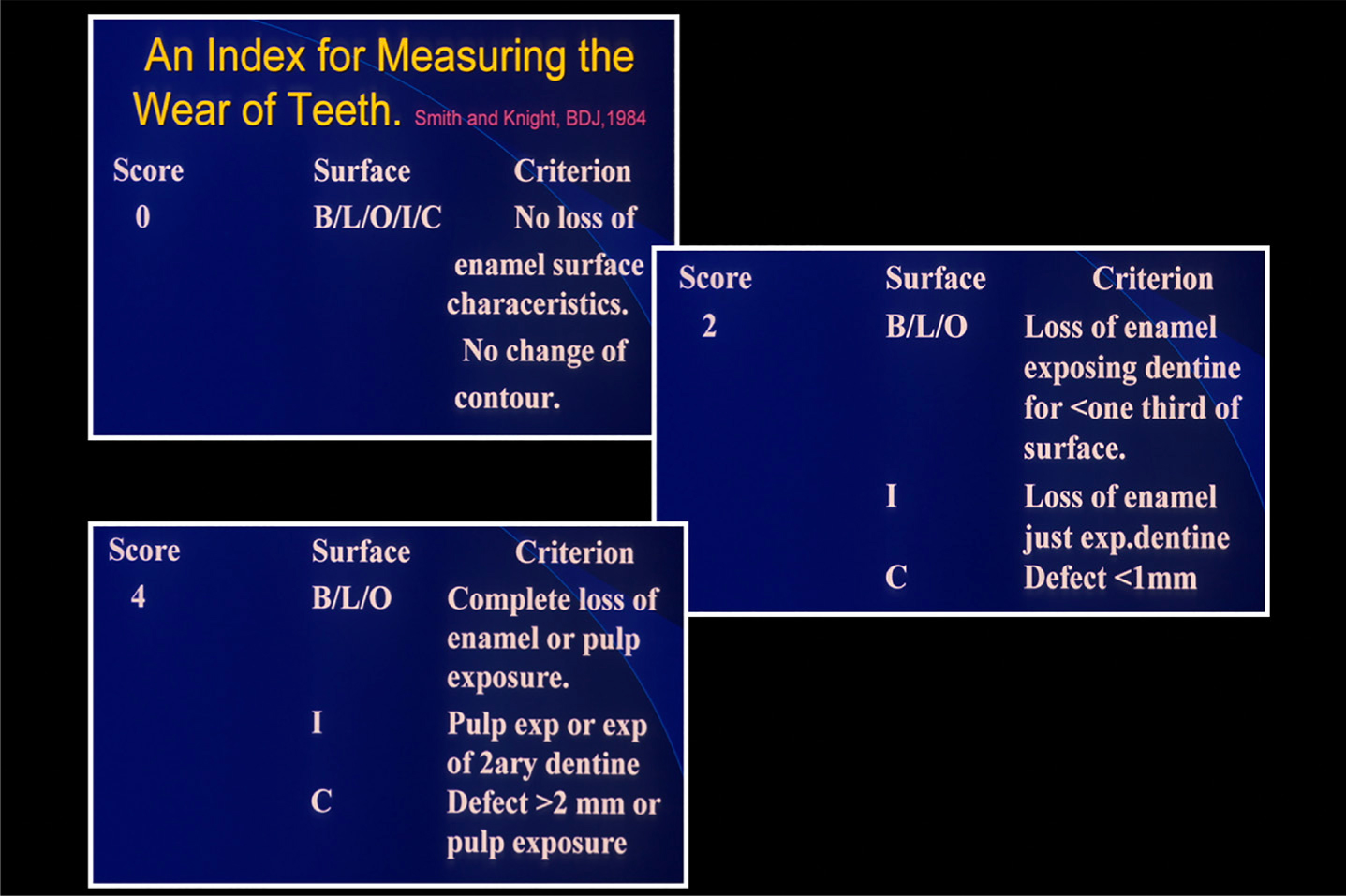
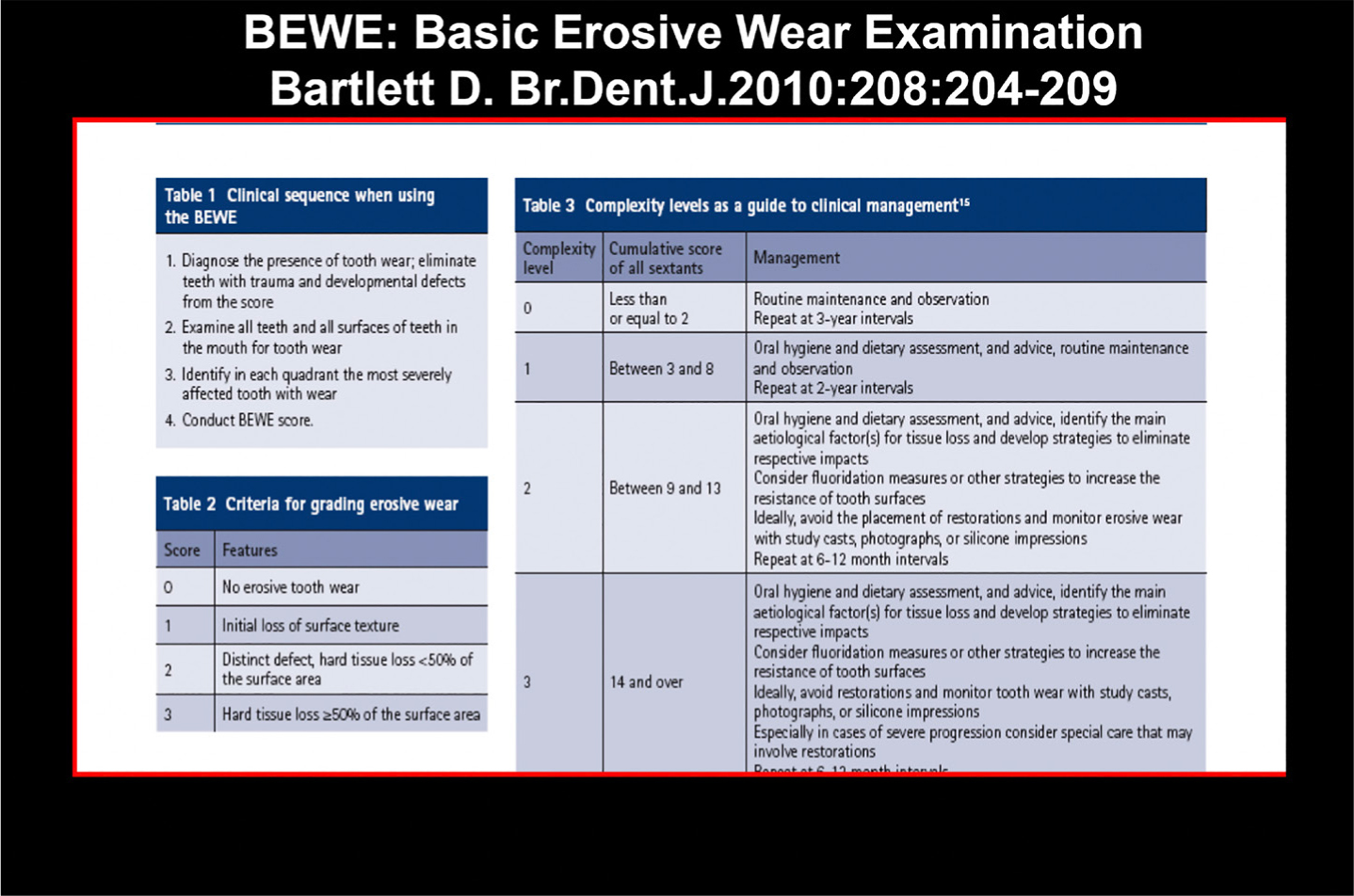
The Smith and Knight tooth wear index was published in 1984,22 and, for many years, was the index most used by researchers for measurement of tooth wear. However, it was not widely used in general dentistry, being complicated and difficult to commit to memory (in the first author's opinion) (Figure 2). It is therefore heartening to report that a measure, based upon visual comparisons of a patient and published illustrations of cases, is now becoming widely used. It uses a similar concept to BPE, namely, the degree of tooth wear per sextant and is known as the Basic Erosive Wear Examination (BEWE) (Figure 3).23
Figure 2. Examples of the criteria used in the Smith and Knight22 tooth wear index.Figure 3. Aspects of the BEWE index.
O'Toole and colleagues24 have published advice on the use of the BEWE index, and its use in risk assessment and monitoring of tooth wear in a previous issue of Dental Update. Readers are directed towards this paper for further information on the implementation of this useful tool into their practices.
Patient satisfaction
Customer surveys are widely used in business to assess levels of satisfaction with services and/or products. The dental practice is no exception, as it is important for practice owners and their teams to assess the needs and levels of satisfaction of the patients for whom they care. Readers are therefore directed to the article by Holt,25 which discusses the planning and execution of a patient satisfaction questionnaire survey. A well-run survey will not only reveal levels of patient satisfaction with the practice care and service, but also allow the practitioner to assess patients' awareness of the levels of care and service being delivered.
Are there any ‘off the shelf’ measures of oral health?
It has been considered11 that none of the measures of general health, as described by McDowell and Newell,26 are appropriate to oral health. Therefore, many composite measures of oral health have previously been described, but none has found acceptance, either in terms of widespread use by general dental practitioners or have proven validity or reproducibility. Among the first of such indices was the National Dental Health Index (NDHI) developed by the Canadian Dental Association for the purpose of measuring national variations in dental disease.27 This index measured four components: caries; periodontal disease; malocclusion; and existing treatment level; however, the index was never published. Other indices include the following:
Lambert and Freeman developed a comprehensive multidimensional Index of Treatment Need (IDN) for use in an epidemiological survey of teenagers in Massachusetts.28
Bulman and co-workers29 produced the Oral Health Grading that was used in an epidemiological comparison of oral health in two urban areas of England. It combined three categories of dental health: dental (A), periodontal (B) and prosthetic (C), which were then subdivided into three grades, with the oral health grading expressed as a six digit code consisting of three letters and three numbers, eg A2B2C3, which is, in the opinion of the authors, overly complex.
Carr and Wolfe30 have also published details of a composite index of oral health, as have Nikias and co-workers.31
Marcus et al32,33 developed an empirically derived measure of oral health status. In the study,32 12 GDPs were required to select the patient who had better oral health from 315 successive pairings formulated from 232 simulated patient cases, which included 18 independent variables representing a diverse range of conditions that may compromise oral health. The results indicated that four (core variables) of the original 18 were important factors in a substantial majority of the preference decisions, these being periodontal disease, missing teeth, decay and fillings.
More recently Ireland et al34 developed a clinical minimum data set (CMDS) to measure oral health status. In this study a random sample of dentists was asked to rank a list of 38 clinical indicators in order of their perceived importance as a means of measuring oral health. Consensus was reached between these dentists and key dental organizations, on a core group of 10 indicators, which can provide information on patients' perception of pain, function and appearance, and professional measurements of caries, teeth present, periodontal disease, oral sepsis, presence of mucosal pathology and tooth wear. This CMDS has, so far, not been universally accepted in the UK.
Mann et al35 proposed a treatment needs index (TNI) for use by health service providers in determining the treatment needs of a community, while finally, Hede36 conducted a study to describe oral health status in a group of hospitalized mental patients.
However, none of these indices has come into widespread use, hence the need to design an index of oral health that would be capable of being used in the area where most dental treatment is performed (ie in general dental practice), and without associated cost implications. This implies that the index should be easy to use and quick to complete. No previously developed index appears to fulfil these criteria.11
Characteristics of a composite index of oral health
Capable of implementation by all dentists (and dental personnel, where permitted) with minimal instruction and training.
It should also be simple, quick to determine, and involve only a minimum of widely available dental equipment, suitable for pre- and post-operative assessment of patients, and appropriate for epidemiological purposes with minimal modification. Ideally, the index should be meaningful to the patient and, therefore, heighten motivation towards optimizing oral health. Above all, the index must enable third parties and the general dental practitioner to operate to an agreed standard and to be consistent.
In 1995, Burke and Wilson11 published details of an Oral Health Index (OHX). The index was designed to provide a numerical measure of the overall state of a patient's oral health by means of a series of simple clinical examinations. Its principal application was intended to be in the assessment of clinical outcome as a proportion of optimum oral health. However, other uses for the index may be envisaged, among these being:
A means of patient motivation, by which a patient is provided with a score of their oral health, and, possibly, comparing that with a score which could be considered optimal;
For measuring changes with time in a patient's oral health status;
For assessing the consistency and thoroughness of an individual dentist's diagnostic procedures;
For service planning and evaluation;
As a marketing tool for an individual practice (for example, 90% of our patients achieve a score of >90% following a course of treatment);
To monitor variation in OHX values achieved by different practices;
For clinical audit of interventions because a caring profession should undertake periodic review of outcomes;
As an epidemiological tool, if sufficient measures of the index are undertaken.
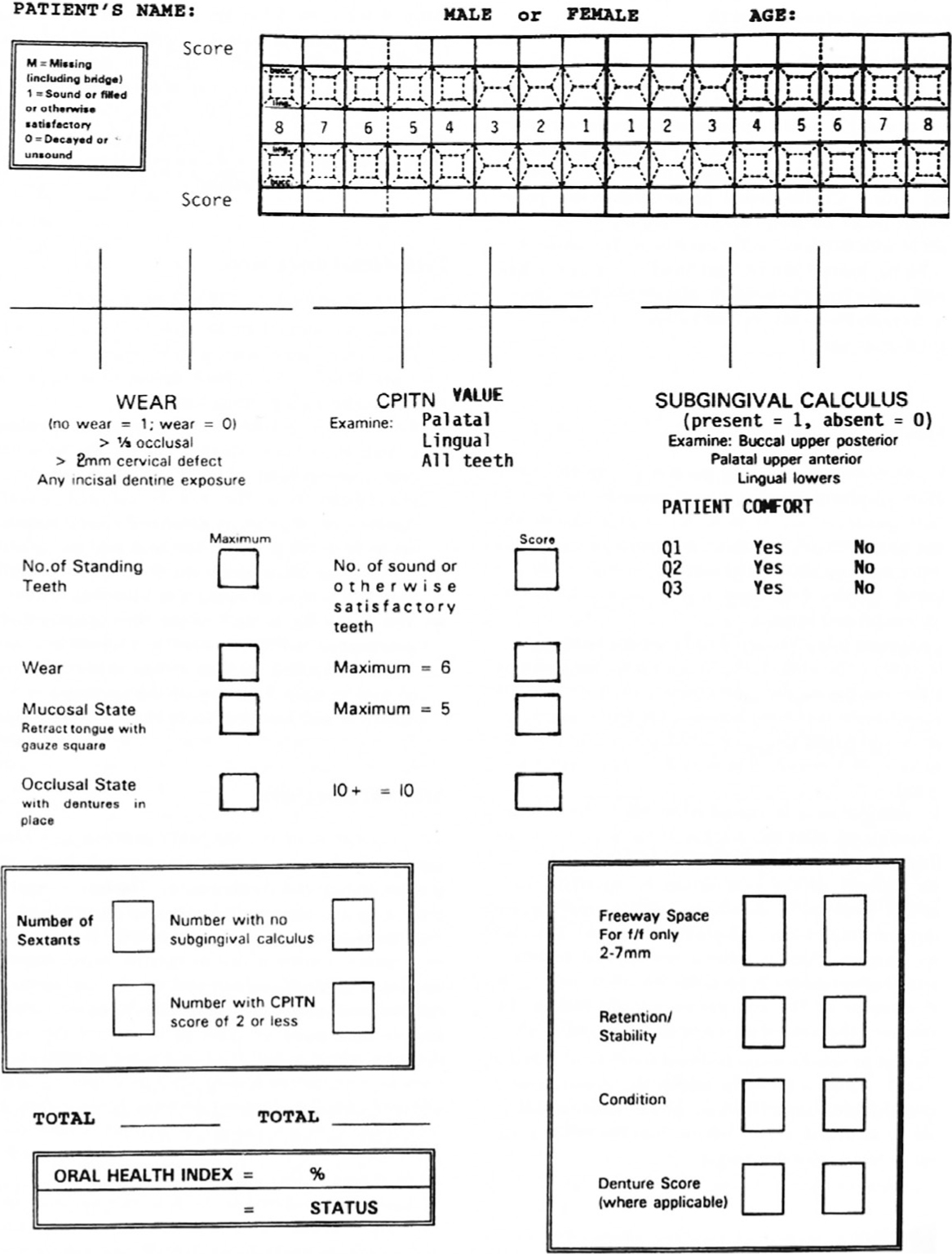
Use of the OHX involves assessing patient comfort and satisfaction in addition to the assessment of caries, periodontal disease, tooth wear, mucosa, occlusion and dentures, where appropriate. Previously accepted standards and/or indices were used to comprise the various elements of the index. The original paper-based scoring form is presented in Figure 4. The OHX score included a section on ‘status’, because a patient with complete dentures, which were of satisfactory appearance and function, could score similarly to a patient with a healthy mouth of 32 teeth. Status was defined as a function of the number of pairs of opposing teeth, because masticatory function is compromised when fewer than ten occluding pairs of teeth are present.37 Two studies have reported on the reliability of the OHX. The results of a comparison of two general dental practitioners indicated an overall value of 0.88, which was considered acceptable.11 The second study compared four dentists (two GDPs and two hospital-based dentists) and indicated correlation coefficients between the four examiners of 0.94–0.99, indicating good correlation between the examiners.38
Figure 4. The original paper-based version of the OHX proforma used in the initial research on the index.
Although the OHX was adopted and developed by Denplan (Winchester, UK), a company providing a privately funded dental capitation scheme for patients and dentists, there is no reason why the OHX, or a derivative thereof, could not be used by any dental practitioner, anywhere. In Denplan's development of the OHX, changes were made to the scoring system, but not to the overall concept, with the OHX being renamed the Denplan Oral Health Score (OHS). A questionnaire-based study examined the views of clinicians using the OHS, with the results indicating its general acceptance, plus an additional benefit as a means of patient motivation.39 Results of further work on attitudes of patients who had had an OHS examination in everyday clinical practice40 indicated that the OHS was considered by most to be a good method for communicating about the patient's oral health between dentist and patient. It was also found to provide a valid and relatively quick method of assessing oral health, given that, within its scoring system, three relevant questions on patient comfort were included. The results of a further study,41 which amount to a ratification of the OHS by most users, indicated that clinical examination of patients is still considered necessary to provide an estimate of oral health. Details of the OHS are presented in Table 4. Patients can achieve a maximum score of 100, with a reduced score being awarded for when there are inadequacies identified in different sections. Readers are directed to the Denplan Excel training manual42 for further details. To date, the OHS has been used in the oral examination of several million patients (M Busby, personal communication).
Stage
Description
Max Score
Patient perception
The patient is asked three direct questions about their own perception of their dental comfort, function and appearance. Each satisfactory response scores 8
24
Tooth health assessment
Examine the teeth and update your dental chart and score as follows. No caries and no restorations: 24. Sound restorations, no caries: 18. Up to 10% of teeth requiring restoration: 12. 10–30% of teeth requiring restoration: 6. More than 30% of teeth requiring restoration: 0
24
Non-carious tooth surface loss
Non-carious tooth surface loss is scored as follows. Normal wear for age: 12. More than expected for age: 6. Much more expected for age: 0
12
Periodontal health
Examine the periodontal tissues, update your records and grade the patient's periodontal health. Each patient scored as follows. Healthy: 24. Gingivitis only:18. Mild disease: 12. Moderate disease: 6. Severe disease: 0
24
Occlusal assessment
With any dentures in place, the occlusion is examined for the presence of 10 or more teeth (natural or prosthetic) opposite each other. This scores 8
8
Mucosal assessment
An oral cancer/mucosal health examination is performed visually. Healthy mucosa scores 8
8
Denture assessment
Each denture present is assessed for freeway space, retention and stability, and acceptable condition. Unsatisfactory scores in any sextant reduces its ‘wear and tear’ score (as described above) to zero
Total:
100
Latest oral health measures, including risk assessments
Oral health assessments, by definition, focus on the current health of a patient. We have, however, now entered the era of personalized medicine where it is recognized that prevention must form the foundation of oral care. Risk factors need to be identified and patients educated about their personal risk behaviours or exposures, thus empowering them to work with their care provider, and at home, to take responsibility for their own health. As a result, a variety of oral health assessments, which include assessments of risk factors, have now become available. These include the NHS England Oral Health Assessment,43 the SDCEP Oral Health Assessment and Review44 developed in Scotland, Assessment of Clinical Oral Risks and Needs (ACORN), developed in Wales,45 and PreViser and DEPPA (the Denplan PreViser Patient Assessment).46
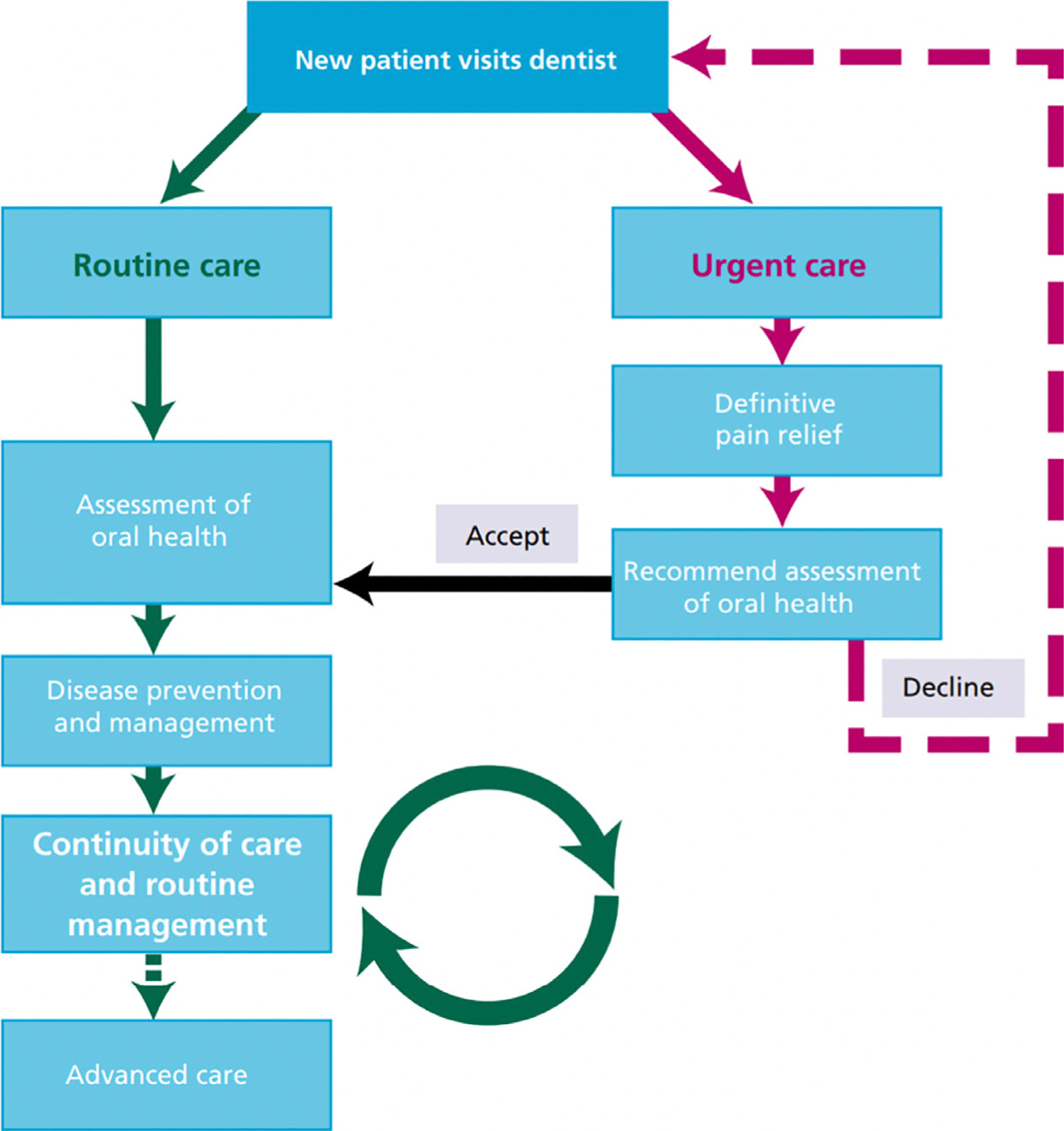
In 2009, the Department of Health in England commissioned a review of NHS dentistry that set out the priorities for public investment in oral health and suggested that the focus should be public health, prevention and the delivery of care through a pathway approach.47 As a result, a pathway was developed by a multidisciplinary group, which included members of the public (Figure 5). It includes an assessment of risk factors and focuses on four oral diseases: caries, periodontal disease, tooth surface loss and soft tissue pathology. A report is produced that suggests a health status category of red, amber or green, which clinicians use to guide their conversations, preventive advice and treatment for patients.
Figure 5. The pathway suggested in the so-called ‘Steele Report’.47
The essential features of the pathway are as follows:
The opportunity for urgent care for everyone when required;
For those without a regular dentist, the opportunity to enter continuing care;
For new patients, there should be a formal oral health assessment to evaluate the risks of all major dental disease (caries, periodontal disease and oral cancer) and the need for treatment. Personalised prevention should be started;
For existing patients who are in a continuing care arrangement (who are returning within an appropriate period, depending on recall interval), there is an assumption that the dentist is aware of, and managing, their preventive needs;
Advanced aspects of restorative care are provided only when there is a stable oral environment, where disease risks are managed and when the patient is established in a continuing care relationship.
ACORN45 is a toolkit designed by dental professionals during the GDS Reform Programme that supports dental teams to carry out a comprehensive risk and needs assessment in a systematic manner. It summarizes findings from the patient history and clinical examination. It supports practices to give personalized advice and agree a preventive annual dental care plan. Training is available via Health Education and Improvement Wales (HEIW): https://ytydysgu.heiw.wales/go/qwlmhn. The GDS Reform Practices are expected to use this toolkit once a year as a part of the overall patient assessment (or at a longer interval if dental recall for a patient has been set longer than 12 months).
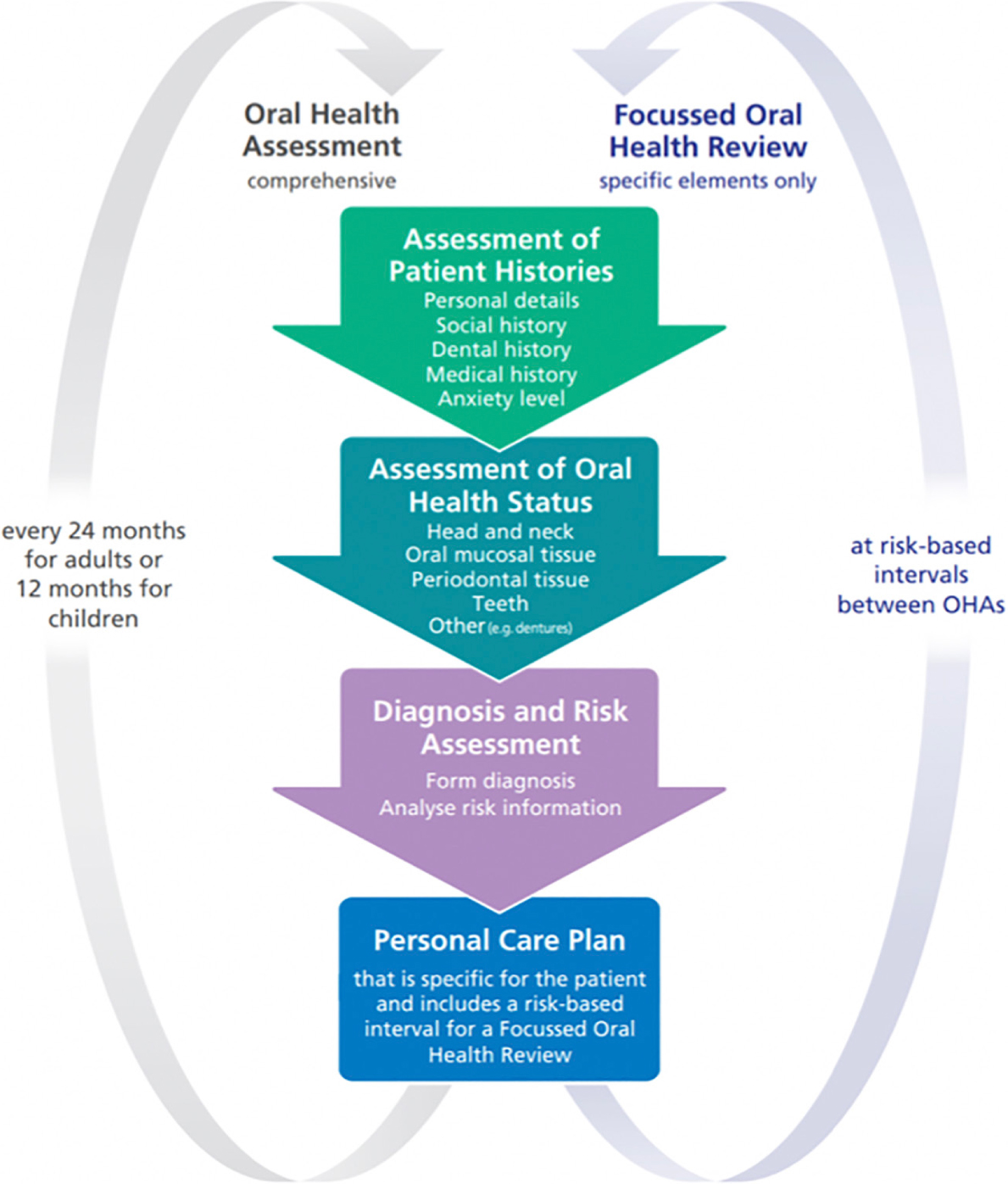
SDCEP published an Oral Health Assessment in 201144 (Figure 6), stating that their ‘key aim was to facilitate the move from a restorative approach to patient care to a preventive and long-term approach that is risk-based and meets the specific needs of individual patients. It also aims to encourage the involvement of patients in managing their own oral health’. A key element of this is that quality measures should be included in the pathway. It could be considered that adoption to such a pathway might provide practitioners with a useable, meaningful tool.
Figure 6. Overview of the SDCEP Oral Health Assessment and Review.
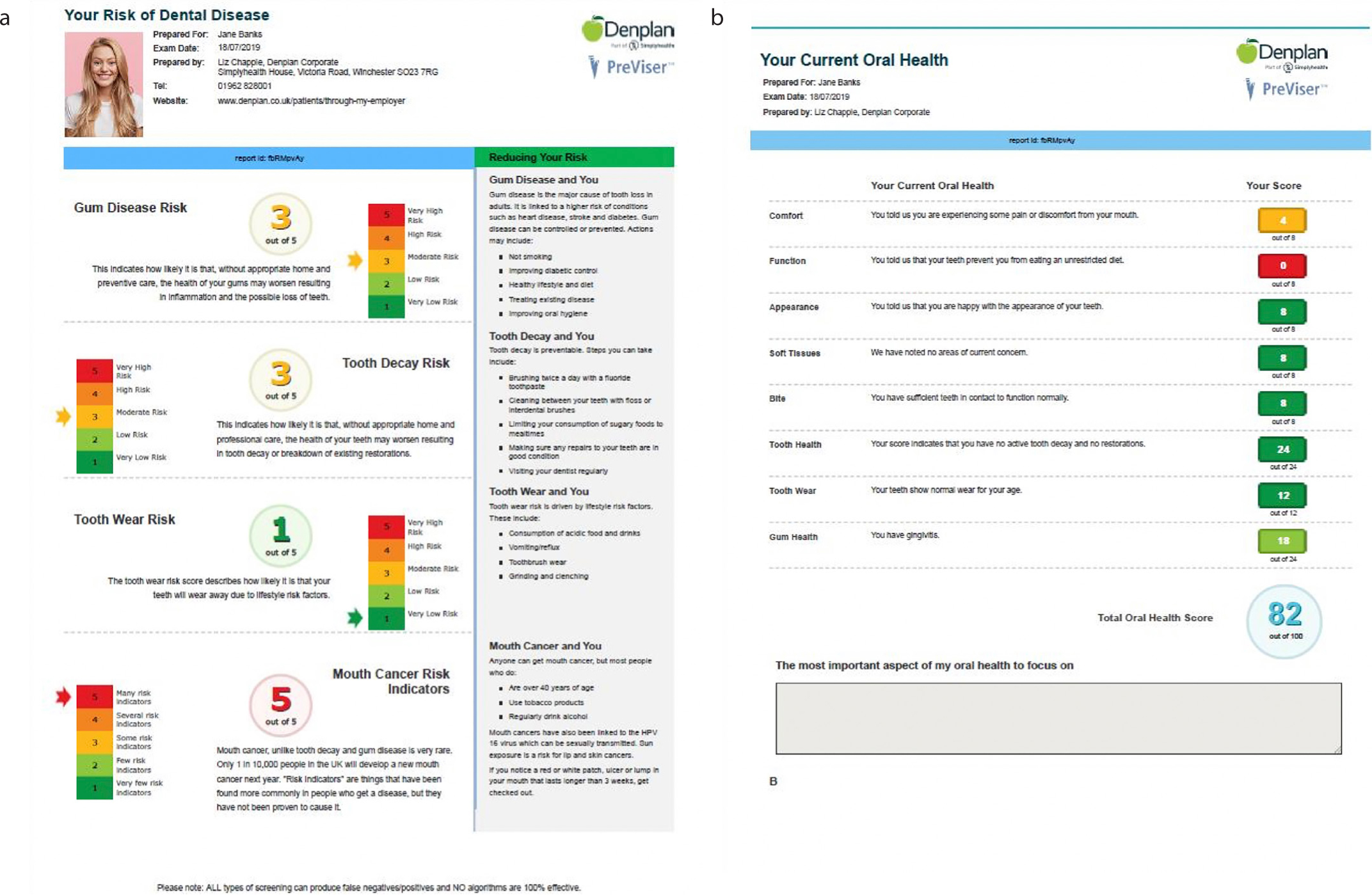
PreViser and DEPPA are clinically validated online disease risk and health assessment systems.46 Both PreViser and DEPPA (a tailored version of PreViser for Denplan practices, which incorporates an updated version of the Denplan Oral Health Score), allow the patient to answer questions on their lifestyle risk factors at home or in the practice, and then use inputs from a routine patient examination to generate risk and disease/health scores. These are run through PreViser algorithms to present the patient with a simple, personalized report in numerical form and on a traffic light scale, which enables the patient to understand their future risk and current health status, alongside the actions they can take to protect their health (Figure 7).48 It has been demonstrated in independent randomized controlled trials that PreViser's periodontal risk assessment improves patient–practitioner trust,49 and improves a patient's understanding of their disease and their motivation to comply with instructions from their dentist. Use of PreViser also improves clinical oral health outcomes.50 PreViser is one of two clinical risk and health assessment tools recommended for periodontal risk assessment by the European Federation of Periodontology's (EFP) consensus workshop on prevention. DEPPA has been used to date by over 830 dentists to generate over 150,000 patient assessments.
Figure 7. (a, b) Illustrations of DEPPA taken from the Denplan Previser Patient Assessment booklet (publisher Denplan from Simply Simply Health Professionals).
Which measure should the practitioner choose?
Readers may, understandably, be confused by the array of measures of oral health, and the risk assessment systems, which are now available. Like most things, it is probably better to start the oral health measurement journey simply. Risk assessment is key to the future of NHS dentistry47 and digital systems exist for the NHS in England and Scotland, and for the private sector, some being embedded into practice management software systems. The authors suggest using the Oral Health Score,40 or a digital derivative thereof, which will provide a good starting point, and is also in line with the comprehensive oral health assessment concept promoted by Steele.47 It is important to use validated systems that have been tried and tested in general dental practice.
Finally, despite the progress that has been made in risk assessment in dentistry in recent years, results of a survey51 of a total of 455,844 patients who met the study inclusion criteria from a large dataset and who received a total of 9,341,583 courses of treatment indicated that treatment history provided an important correlate of future treatment needs. The authors of the study classified treatment into ‘active’ (eg restorations, extraction of prosthesis) and ‘not active’ (eg prevention, diagnosis), with the results indicating that ‘active’ treatment was the more important component in terms of predicting treatment need. However, the authors added that historic treatment costs are not a good basis for predicting treatment at an individual patient level, but the data showed that the historic average spend per patient may readily be translated into the amount of predicted spend in the future. In short, therefore, despite the above, some form of risk assessment or measure of oral health will still be needed.
Conclusion
Perves and colleagues,52 writing in the Lancet, stated: oral health matters. The teeth and mouth are an integral part of the body, supporting and enabling essential human functions and the mouth is a fundamental feature of personal identity. The ability to measure oral health may, therefore, be considered central to successful patient management and treatment. In that regard, the measurement of oral health has come a long way since its early beginnings in Canada, to the development of the Oral Health Index in 1995, and its subsequent development to form the Oral Health Score, which remains in use in its latest form in many dental practices. A variety of oral health measurement tools, which also incorporate risk assessment measurements are also presently available. In order to incorporate these into practice, practitioners should evaluate each in more depth than has been possible in this article and commence training in the measure considered most user-friendly and relevant to their practices. In this regard, the use of a measure of oral health on a personal and/or national scale, is to be encouraged.