The Coronavirus disease 2019 (COVID-19) pandemic, caused by the severe acute respiratory syndrome coronavirus 2 (SARSCoV-2), seems to have spared no single community. Rapid and accurate identification of COVID-19 patients are the mainstay for breaking the chain of community infection and controlling the pandemic. There are now a bewildering array of diagnostic tests available to detect COVID-19 at various stages of infection. In this, the fourth article in the COVID-19 Commentary series, we describe the basics of current clinical diagnostics, including molecular and serological testing approaches, and summarize their advantages and limitations.
The current pandemic of COVID-19 is an infectious disease caused by SARS-CoV-2 which originated in Wuhan, China in late 2019. It is now known that the median incubation period of COVID-19 is approximately 5 days (range: 2 to 14 days), and a large proportion of those infected become symptomatic within two weeks or so (range: 8 to 16 days).1 The recovery period for mild infection is 2 weeks, although in severe cases this may last up to 6 weeks. In the most severe infections, the time from symptom onset to death may range between 2 to 8 weeks, depending on various co-factors, such as the extant co-morbidities.
In the early pre-symptomatic phase, the index case unknowingly transmits the infection to others prior to symptom development and, on the contrary, a small proportion of infected individuals never develop symptoms (so called ‘asymptomatics’) and may act as ‘silent spreaders’ of the infection in the community. These two elements of the disease development have made the spread of COVID-19 virtually uncontrollable, leading to the current pandemic.
In the absence of efficacious therapeutics and a vaccine, as yet, to combat the infection, the mainstay of prevention and spread of COVID-19 is the early diagnosis of the disease, with the help of an array of diagnostic tests that are currently available. According to the World Health Organization (WHO) and US Food and Drug Administration (FDA), over 450 tests have been developed thus far for rapid identification of COVID-19 patients in clinical and research settings.2
In order to comprehend the basics of COVID-19 diagnostics, it is essential to know the structural elements of SARS-CoV-2, as the tests are based on the detection of the anatomical components of the organism. Similarly, to understand the serological tests for the virus, a clear comprehension of the host antibody response is essential. These are described first, followed by the diagnostic tests that are in common use.
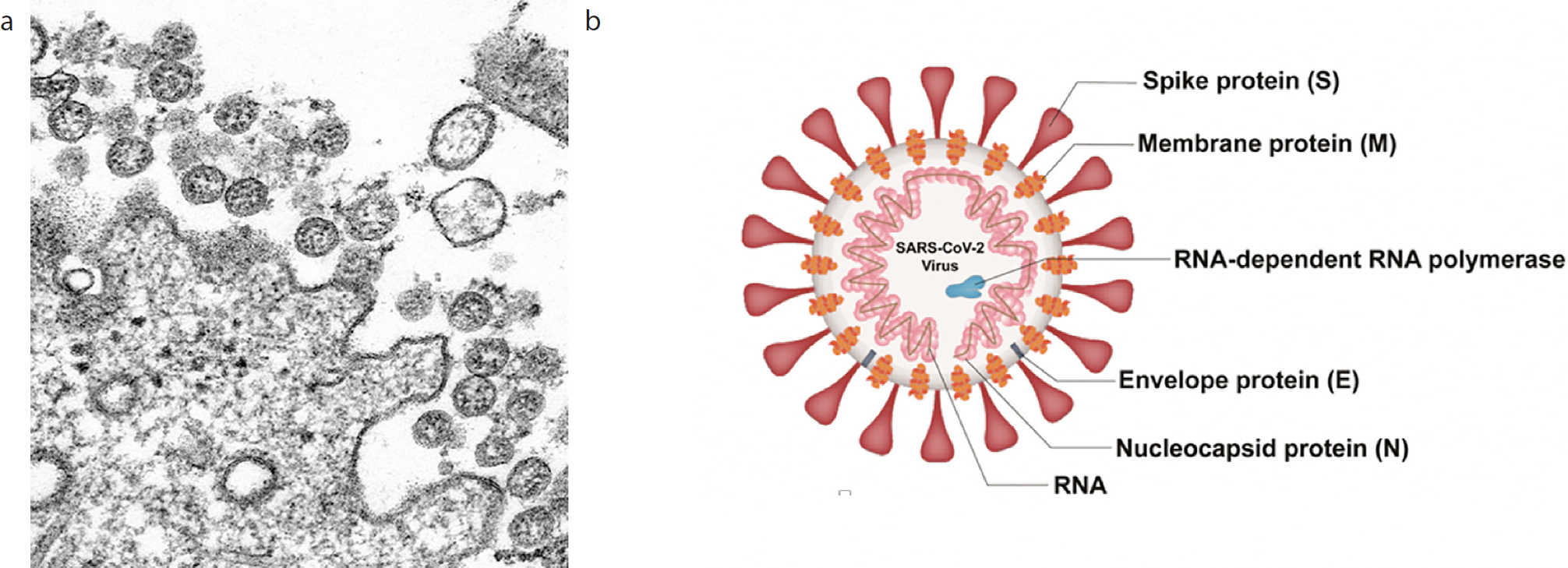
The overall structure of SARS-CoV-2 is similar to other viruses of the Coronaviridae family. It has a protein envelope with characteristic outward projecting spikes (hence the Latin name corona = crown), enclosing a single-stranded, positive sense RNA genome of approximately 30,000 nucleotides in length (Figure 1). The genome is tightly bound to a protein capsid, and both together are called a nucleocapsid. The nucleocapsid is protected by the external protein envelope, which has three major components, the spike (S) glycoprotein, envelope (E) glycoprotein, membrane (M) glycoprotein, (plus several accessory proteins). Thus:
The nucleocapsid (N) protein cover codes for 27 proteins, including an RNA-dependent RNA polymerase;
The spike or S glycoprotein is a transmembrane protein in the outer portion of the virus and forms, so called, homotrimers protruding in the viral surface, giving them the crown or corona-like appearance. They facilitate binding of the virus to the host cells by attaching to the angiotensin-converting enzyme 2 (ACE2) receptors expressed on epithelial and other cells;
The membrane, or M protein, plays a role in determining the shape of the virus envelope;
The envelope or E protein, which is the smallest protein in the SARS-CoV-2 structure, plays a role in the production and maturation of this virus.
Figure 1
(a) Morphology of SARS-CoV-2. Transmission electron microscope image of SARS-CoV-2 spherical viral particles emerging from an infected epithelial cell; (b) structural components of SARS-CoV-2. (Modified from the US Centres for Disease Control Image Library).
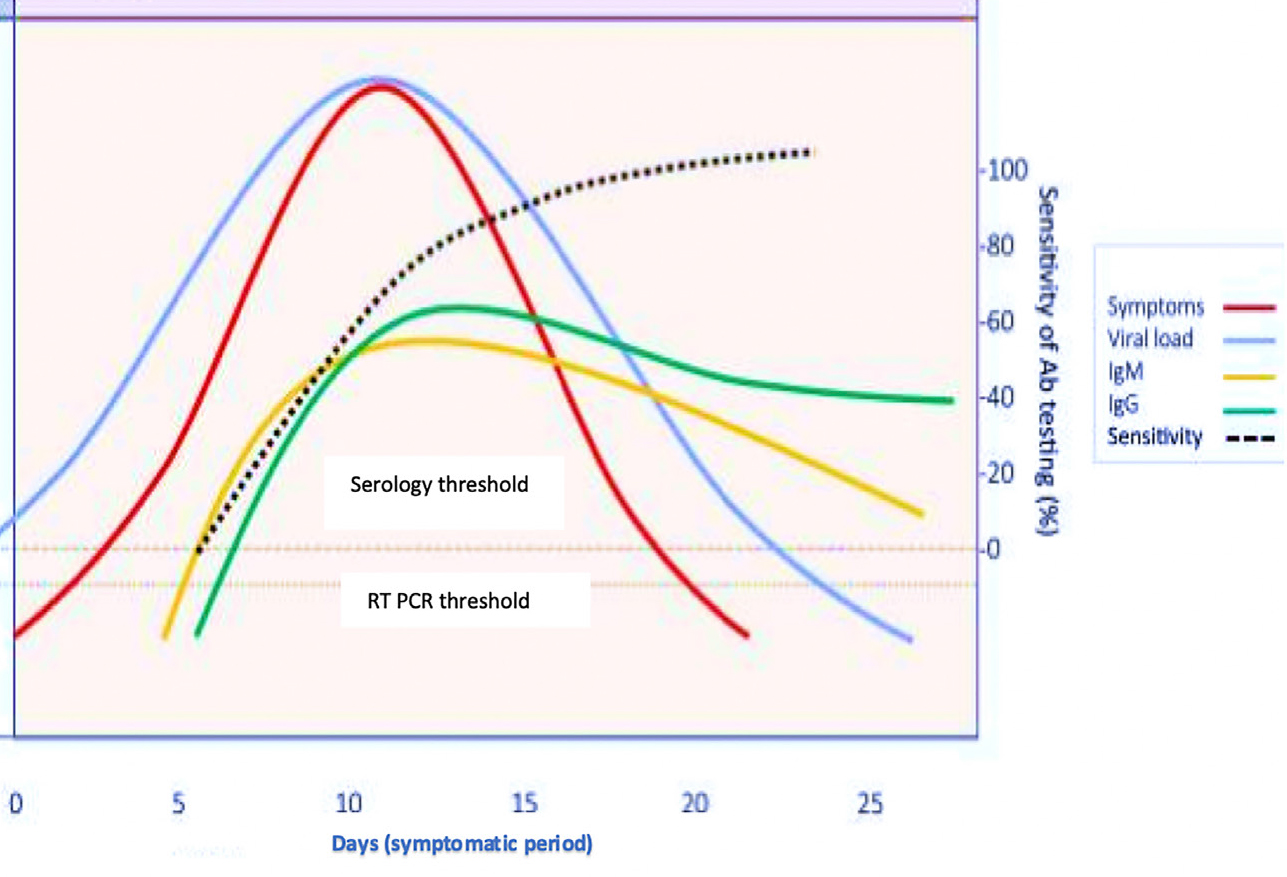
In simple terms, the host immune response of the body to SARS-CoV-2 is triggered through the stimulation of the innate immune system cells via antigen presenting cells (eg dendritic cells and macrophages as frontline guardian cells of the host). The antibodies produced are mainly IgM and IgG (together with some IgA), which have a unique profile in response to the infection. The median seroconversion time for IgM and IgG antibodies are 12 and 14 days after the onset of symptoms, respectively, whilst they are detected only in less than 40% of the patients within the first week (Figure 2). In some cases, serum IgG could appear at the same time or even earlier than IgM.
Figure 2 A diagrammatic representation of antibody development after SARS-CoV-2 infection during the symptomatic period and thereafter (x axis), and the sensitivity for antibody tests (y axis); (RT PCR, real-time reverse transcription polymerase chain reaction; IgM, Immunoglobulin M; IgG Immunoglobulin G). (Note: Antigens can also be detected by RT PCR tests during the pre-symptomatic period which is not shown in the figure).
It is noteworthy that, in addition to the antibody formation, exposure to coronaviruses in general also induce CD4 T cells and CD8 memory cell development and maturation that can last for up to 4 years. This bodes well for the development of vaccines against SARS-COV-2, as an encounter with the virus even after a few years is likely to protect the vaccinee, after the initial, successful vaccine procedure.
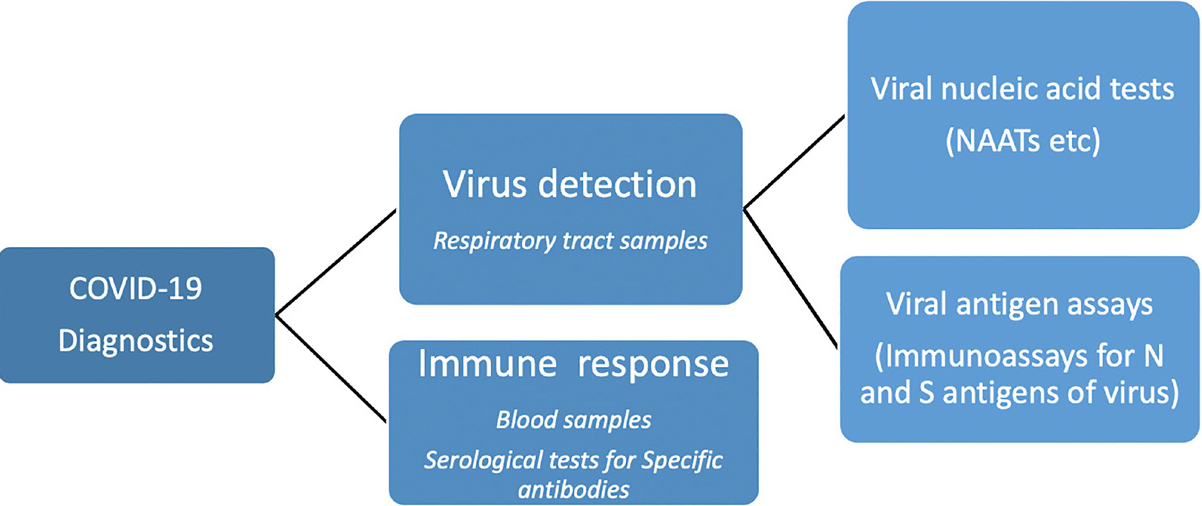
i) Detection of viral antigens which indicate current infection; or
ii) The host immune response to the virus (ie specific antibodies) that indicate past infection or vaccination (Figure 3).
Figure 3 A schematic diagram showing the principles guiding the diagnostic tests for COVID-19.
Type of Test and Synonyms
Primary Clinical Use
Specimen/s Required
Turnaround Time*
Properties
I
Viral test, molecular test, nucleic acid amplification test (NAAT), RT PCR test, LAMP test
Diagnosis of current infection
Nasal or throat swab (most tests)Saliva (a few tests): respiratory tract specimens in hospitalized patients
May vary from 15 min to 8 hr depending on the type of test, and laboratory workflow
Amplifies viral RNA; Highly sensitive and specific in ideal settings. (Results depend on the type and quality of the specimen and the duration of illness at the time of testing).Usually does not need to be repeated.
II
Antigen tests or rapid diagnostic tests
Diagnosis of current infection
Nasopharyngeal or nasal swabs
Usually less than 60 min
Most probe for nucleocapsid (N) or spike (S) proteins, ie antigens of SARS-CoV-2; generally less sensitive, and more likely to miss an active infection compared to nucleic acid tests.
III
Serology test, Serological test, serology, blood
Diagnosis of prior infection or (in future) seroconversion after vaccination
Finger prick or venepuncture blood
Usually ranges from 15 minutes to 2 hours
Checks for IgG antibodies (mainly) to the S or the spike protein or nucleocapsid, N or NC protein. Highly variable sensitivity and specificity, and hence results should be interpreted with caution; possible cross-reactivity with other coronaviruses reported.
Data from various sources including References 1 and 5; COVID-19: coronavirus disease 2019; RT PCR: real-time reverse transcription polymerase chain reaction; IgG: immunoglobulin G; loop-mediated amplification: LAMP.
*Turnaround time is influenced by the test used and laboratory workflow.
Note: the sensitivity and specificity of any diagnostic test depend upon the quality of the sample, and various other technical factors.
(Note: Antigens can also be detected by RT PCR tests during the pre-symptomatic period which is not shown in the figure)
Antigen tests colour coded in green and antibody tests in red.
The following is a primer on the currently prevalent antigen and antibody tests for COVID-19, and their utility. However, it should be noted that, due to the dynamic nature of the subject, the viral testing procedures are in a state of flux.
In general, COVID-19 diagnostic tests can be broadly classified as:
Tests for viral nucleic acid (so called nucleic acid amplification tests or NAATs);
Tests for viral antigen tests;
Antibody tests for seroconversion. (Note: A continuously updated infographic on COVID diagnostic tests can be found at https://csb.mgh.harvard.edu/covid)
Tests for viral nucleic acid (RNA)
Real-time reverse transcription polymerase chain reaction (RT PCR) test is the gold standard for diagnosis of current infection with COVID-19. It amplifies the viral RNA (Figure 1) to detectable levels; hence the term nucleic acid amplification tests (NAAT).3 This method, which is quantitative, and highly sensitive and specific, is also the commonest technique currently used to detect SARS-CoV-2 RNA from respiratory samples. The test is used increasingly on automated platforms, and may take several hours to complete (Table 1).
Tests for viral antigens
The antigen tests probe for the structural components, such as the nucleocapsid (N) or spike (S) proteins of SARS-CoV-2 (Figure 1) via lateral flow or ELISA (enzyme-linked immunosorbent assay) tests, and can be performed with only nasopharyngeal swabs. As these tests take less than an hour to complete, and yield faster results than some NAATs, they are used for point of care (POC) testing (eg airports for arrivals and departures).
However, the broad consensus is that the viral antigen tests are less sensitive than NAATs, described in Table 1, and often yield false-negative results. Hence, a negative antigen test does not necessarily rule out SARS-CoV-2 infection, and should be confirmed using a sensitive NAAT if the clinical suspicion is high. Nevertheless, antigen tests are valuable for detecting those in the early stages of infection, when virus replication is at its highest.
Serological tests
In general, serological tests are useful to determine prior viral exposure of an individual and seroconversion after a course of vaccination (eg akin to seroconversion after Hepatitis B infection or vaccination). They could also be used for retrospective assessment of the efficacy of infection control and lockdown measures, as well as for ascertaining the extent of COVID-19 in the community through en masse evaluation.
As soon as any virus infects a person, he/she will start developing antibodies, and the first such antibody type is IgM immediately followed by IgG. The former is rather transient compared to IgG, which could last for several months or years, depending on various factors. This is also the case with SARSCoV-2 infection as, in many studies, IgM and IgG seroconversion occurred in all patients between the third and fourth week. Thereafter IgM began to wane, and virtually disappeared by week 7, although IgG levels persisted beyond 7 weeks.4
As seen above, SARS-CoV-2 possesses various antigenic structural components (Figure 2), and a substantial antibody response is directed against the nucleocapsid (N or NC) protein. Hence, tests that detect antibodies to NC are the most sensitive, though they may be lacking in specificity. However, antibodies to the S or the spike protein are much more specific than that for the NC protein. Additionally, antibodies to the S protein are considered to neutralize the viral infectivity much more than the other antibodies. The long-term persistence of protection conferred by the neutralizing antibodies is unknown, as yet.
Finally, serological tests for SARS-CoV-2 should be specific and must differentiate past infections from those caused by other human coronavirus infections (eg SARS-CoV, HKU1). There are also many confounding factors that interfere with laboratory testing for COVID-19, including sample collection, transportation and so on, that are not described here, and are beyond the remit of this article.
Future perspectives and conclusions
Several simple, reliable and rapid COVID-19 diagnostic tests, which could be used at community level and obviate sample referral to a centralized laboratory and consequent prolonged turnaround time, are currently under development. They include loop-mediated amplification (LAMP), recombinase polymerase amplification (RPA) and nicking enzyme-assisted reaction (NEAR) technologies that yield results within 15 to 30 minutes. It is hoped that, in the fullness of time, such miniaturized tests, akin to ‘pregnancy tests’, could be used and interpreted by ordinary citizens at home. These rapid diagnostic tests hold much promise and would be a valuable and welcome addition to curb the pandemic, particularly in resource-poor settings in the developing world where its rabid and rampant spread has created unprecedented suffering, misery and privation.
See review of SDCEP document ’Breaking News: COVID-19 and Dentistry‘ at the end of the Letters to The Editor on page 769.