Maloney PL, Doku HC. Maxillary sinusitis of odontogenic origin. J Can Dent Assoc. 1968; 34:591-603
Matsumoto Y, Ikeda T, Yokoi H, Kohno N. Association between odontogenic infections and unilateral sinus opacification. Auris Nasus Larynx. 2015; 42:288-293
Troeltzsch M, Pache C, Troeltzsch M Etiology and clinical characteristics of symptomatic unilateral maxillary sinusitis: a review of 174 cases. J Craniomaxillofac Surg. 2015; 43:1522-1529
Lechien JR, Filleul O, Costa de Araujo P Chronic maxillary rhinosinusitis of dental origin: a systematic review of 674 patient cases. Int J Otolaryngol. 2014; 2014 https://doi.org/10.1155/2014/465173
Lim CG, Spanger M. Incidental maxillary sinus findings in patients referred for head and neck CT angiography. Singapore Dent J. 2012; 33:1-4
Cooke LD, Hadley DM. MRI of the paranasal sinuses: incidental abnormalities and their relationship to symptoms. J Laryngol Otol. 1991; 105:278-281
Iwabuchi Y, Hanamure Y, Ueno K, Fukada K, Furuta S. Clinical significance of asymptomatic sinus abnormalities on magnetic resonance imaging. Arch Otolaryngol Head Neck Surg. 1997; 123:602-604
Rak KM, Newell JD, Yakes WF, Damiano MA, Luethke JM. Paranasal sinuses on MR images of the brain: significance of mucosal thickening. Am J Roentgenol. 1991; 156:381-384
Carmeli G, Artzi Z, Kozlovsky A, Segev Y, Landsberg R. Antral computerized tomography pre-operative evaluation: relationship between mucosal thickening and maxillary sinus function. Clin Oral Implants Res. 2011; 22:78-82
Zinreich SJ, Kennedy DW, Kumar AJ, Rosenbaum AE, Arrington JA, Johns ME. MR imaging of normal nasal cycle with sinus pathology. J Comput Assit Tomogr. 1988; 12:1014-1019
Wilson PS, Grocutt M. Mucosal thickening on sinus X-rays and its significance. J Laryngol Otol. 1990; 104:694-695
Phothikhun S, Suphanantachat S, Chuenchompoonut V, Nisapakultorn K. Cone beam computed tomographic evidence of the association between periodontal bone loss and mucosal thickening of the maxillary sinus. J Periodontol. 2012; 83:557-564
Nunes CA, Guedes OA, Alencar AH, Peters OA, Estrela CR, Estrela C. Evaluation of periapical lesions and their association with maxillary sinus abnormalities on cone beam computed tomographic images. J Endod. 2016; 42:42-46
Block MS, Dastoury K. Prevalence of sinus membrane thickening and association with unhealthy teeth: a retrospective review of 831 consecutive patients with 1662 cone-beam scans. J Oral Maxillofac Surg. 2014; 72:2454-2460
Roque-Torres GD, Ramirez-Sotelo LR, Vaz SL, Bóscolo SM, Bóscolo FN. Association between maxillary sinus pathologies and healthy teeth. Braz J Otorhinolaryngol. 2016; 82:33-38
London: National Radiological Protection Board, Department of Health; 2001
White S, Pharoah M.St Louis: Mosby; 2009
Herrmann BW, Forsen JW Simultaneous intracranial and orbital complications of acute rhinosinusitis in children. Int J Paediatr Otorhinolaryngol. 2004; 68:619-625
Selden HS, August DS. Maxillary sinus involvement – an endodontic complication. Report of a case. Oral Surg Oral Med Oral Pathol. 1970; 30:117-122
Hauman CH, Chandler NP, Tong DC. Endodontic implications of the maxillary sinus: a review. Int Endod J. 2002; 35:127-141
Schilder H. Filling root canals in three dimensions. Dent Clin North Am. 1967; 11:723-744
Schilder H. Cleaning and shaping the root canal. Dent Clin North Am. 1974; 18:269-296
Sjögren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long term results of endodontic treatment. J Endod. 1990; 16:498-504
Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: Part 1: periapical health. Int Endod J. 2011; 44:583-609
Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment. Part 2: Tooth survival. Int Endod J. 2011; 44:610-625
Seltzer S, Soltanoff W, Sinai I, Goldenberg A, Bender IB. Biologic aspects of endodontics part III. Periapical tissue reactions to root canal instrumentation. Oral Surg Oral Med Oral Pathol. 1968; 26:534-546
Bergenholtz G, Lekholm U, Milthon R, Engstrom B. Influence of apical over instrumentation and over filling on re-treated root canals. J Endod. 1979; 5:310-314
Fairbourn DR, McWalter GM, Montgomery S. The effect of four preparation techniques on the amount of apically extruded debris. J Endod. 1987; 13:102-108
Fukushima H, Yamamoto K, Hirohata K, Sagawa H, Leung KP, Walker CB. Localization and identification of root canal bacteria in clinically asymptomatic peri-apical pathosis. J Endod. 1990; 16:534-538
Harrington GW, Natkin E. Midtreatment flare-ups. Dent Clin North Am. 1992; 36:409-423
Marais JT, van der Vyver PJ. Invasion of the maxillary sinus with calcium hydroxide. Sizing gutta percha points with a gauge to ensure optimal lateral condensation. J Dent Assoc S Afr. 1996; 51:606-608
Haanaes HR, Hepse HU, Stenvik A, Stermer Beyer-Olsen EM, Bjornland T. Effect of calcium hydroxide implantation in maxillary sinus in macaques. Endod Dent Traumatol. 1987; 3:229-232
Fava LR. Calcium hydroxide paste in the maxillary sinus: a case report. Int Endod J. 1993; 26:306-310
Pashley EL, Birdsong NL, Bowman K, Pashley DH. Cytotoxic effects of NaOCL on vital tissue. J Endod. 1985; 11:525-528
Ehrich DG, Brian JD, Walker WA. Sodium hypochlorite accident: inadvertent injection into the maxillary sinus. J Endod. 1993; 19:180-182
Kavanagh CP, Taylor J. Inadvertent injection of sodium hypochlorite into the maxillary sinus. Br Dent J. 1998; 185:336-337
Laverty DP. A case report of accidental extrusion of sodium hypochlorite into the maxillary sinus during endodontic retreatment and review of current prevention and management. J Res Dent. 2014; 2:96-100
Sjögren U, Sundqvist G, Nair PN. Tissue reaction to gutta-percha particles of various sizes when implanted subcutaneously in guinea pigs. Eur J Oral Sci. 1995; 103:313-321
Kapolowitz GJ. Penetration of the maxillary sinus by overextended gutta percha cones. Report of two cases. Clin Prev Dent. 1985; 7:28-30
Bjørnland T, Haanaes HR, Marhrethe E, Beyer-Olsen S. Sinusitis caused by endodontic materials displaced into the maxillary sinus. Endod Dent Traumatol. 1987; 3:37-40
Ericson S, Finne K, Persson G. Results of apicoectomy of maxillary canines, premolars and molars with special reference to oroantral communication as a prognostic factor. Int J Oral Surg. 1974; 3:386-393
Ioannides C, Borstlap WA. Apicoectomy on molars: a clinical and radiographical study. Int J Oral Surg. 1983; 12:73-79
Rud J, Rud V. Surgical endodontics of upper molars: relation to the maxillary sinus and operation in acute state of infection. J Endod. 1998; 24:260-261
Freedman A, Horowitz I. Complications after apicoectomy in maxillary premolar and molar teeth. Int J Oral Maxillofac Surg. 1999; 28:192-194
Selden HS. The interrelationship between the maxillary sinus and endodontics. Oral Surg Oral Med Oral Pathol. 1974; 38:623-629
Benninger MS, Sebek BA, Levine HL. Mucosal regeneration of the maxillary sinus after surgery. Otolaryngol Head Neck Surg. 1989; 101:33-37
Kim S, Kratchman S. Modern endodontic surgery concepts and practice: a review. J Endod. 2006; 32:601-623
Watzek G, Bernhart T, Ulm C. Complications of sinus perforations and their management in endodontics. Dent Clinic North Am. 1997; 41:563-583
Legent F, Billet J, Beauvillain C, Bonnet J, Miegeville M. The role of dental canal fillings in the development of Apergillus Sinusitis. A report of 85 cases. Arch Otorhinolaryngol. 1989; 246:318-320
Giardino L, Pontieri F, Savoldi E, Tallarigo F. Aspergillus mycetoma of the maxillary sinus secondary to overfilling of a root canal. J Endod. 2006; 32:692-694
Nolard N, Detandt M, Beguin H. Ecology of Aspergillus species in the human environment. In: Vanden Bossche H, MacKenzie DWR, Cauwenbergh G (eds). Boston, MA: Springer; 1998
Mousavi B, Hedayati MT, Hedayati N, Ilkit M, Syedmousavi S. Aspergillus species in indoor environments and their possible occupational and public health hazards. Curr Med Mycol. 2016; 2:36-42
Saral R. Candida and Aspergillus infections in immunocompromised patients: an overview. Rev Infect Dis. 1991; 13:487-492
Tamgadge AP, Mengi R, Tamgadge S, Bhalerao SS. Chronic invasive aspergillosis of paranasal sinuses: a case report with review of the literature. J Oral Maxillofac Pathol. 2012; 16:460-464
van de Peppel RJ, Visser LG, Dekkers OM, de Boer MGJ. The burden of invasive Aspergillosis in patients with haematological malignancy: a meta-analysis and systematic review. J Infect. 2018; 76:550-562
Kanj A, Abdallah N, Soubani AO. The spectrum of pulmonary aspergillosis. Respir Med. 2018; 141:121-131
Odell E, Pertl C. Zinc as a growth factor for Aspergillus sp. and the antifungal effects of root canal sealants. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995; 79:82-87
Sato FR, Sawazaki R, Berretta D, Moreira RW, Vargas PA, de Almeida OP. Aspergillosis of the maxillary sinus associated with zygomatic implant. J Am Dent Assoc. 2010; 141:1231-1235
The Maxillary Sinus: what the general dental team need to know part 3: maxillary sinus disease of endodontic origin James C Darcey Garmon W Bell Iain Macleod Colin Campbell Dental Update 2024 47:6, 707-709.
Authors
James CDarcey
BDS, MSc, MDPH MFGDP, MEndo FDS(Rest Dent)
Consultant and Honorary Lecturer in Restorative Dentistry and Specialist in Endodontics, University Dental Hospital of Manchester
This paper, part 3 of the series, discusses the variation in maxillary sinus mucosal thickening when seen on radiographic images and the relation to disease. The role of apical periodontitis in disease of the maxillary sinus and its lining, the stages of endodontic treatment at which problems can arise and how these can be prevented, are considered. Complications involving extruded endodontic materials will also be discussed.
CPD/Clinical Relevance: Apical periodontitis may very occasionally contribute to maxillary sinus infection, when the roots of teeth lie in close relation to the sinus. Apical displacement of infection, irrigants or materials during endodontic treatment may contribute to inflammation and infection and should be avoided.
Article
James C Darcey Garmon W Bell Ian MacLeod Colin Campbell
In this third paper on the maxillary sinus and the importance to the Dental Team, the role that chronic apical periodontitis contributes to maxillary sinus disease of endodontic origin is examined, and the modifications to endodontic technique needed to avoid maxillary sinus involvement are discussed.
It is frequently reported that approximately 12% of cases of unilateral maxillary sinusitis are of dental origin.1 Some authors report as high as 75% prevalence.2,3 Considering the prevalence of apical periodontitis in the population, the relatively high proportion of unilateral cases of maxillary sinusitis attributed to odontogenic causes is not reflected in the work load of most Ear Nose and Throat surgeons, or the Oral/Oral and Maxillofacial surgeons who work alongside them. It is therefore quite probable that, while there is an ample supply of case reports and case series of endodontic and periodontal disease contributing to inflammation of the maxillary sinus lining, or suppurative chronic maxillary sinusitis, there may have been bias in patient selection such that the cases presented may not accurately reflect the prevalence within the greater population.
Oro-antral fistulae, and displaced roots of teeth are the greatest contributory factors to maxillary sinus disease of odontogenic origin.4 Apical periodontitis, periodontal disease, ectopic teeth or odontomes, with or without cystic involvement, may also cause maxillary sinus disease.4 Dental implants with bone regenerative techniques are regarded as making an increasing contribution, and will be discussed in part 4 of this series.
Inflammation of the paranasal sinus lining
Inflammatory changes of the paranasal sinus lining are generally of an allergenic nature, although these may also occur due to localized or atmospheric irritants. Changes are often identified via co-incidential findings on computed tomography or magnetic reasonance imaging scans performed for purposes other than imaging of the paranasal sinuses.5,6 These inflammatory changes can range from areas of localized thickening, to retention cysts caused by duct obstruction in a sero-mucinous gland, or polyps and expansile mucoceles. Mucosal thickening is a common finding in ethmoid and maxillary sinuses, as are retention cysts. As a result of ostial obstruction, mucoceles can exert pressure, causing bone expansion and resorption. However, these are rarely found in the maxillary sinus, presenting more often in the frontal sinus. One presentation of inflammatory paranasal mucosal swelling does not necessarily progress to another.
There is little correlation between signs of paranasal sinus lining thickening and patient reported symptoms of disease.7 There is little agreement on what level of maxillary sinus thickening is within variation of normal or related to disease, although generalized thickening of 5 mm or more can be associated with increased incidence of ostial obstruction.8,9 There is a recognized cyclical variation over a period of hours of the thickness of nasal and ethmoid sinus mucosa as a result of congestion related to blood flow, such that the mucosa when viewed on cross-sectional imaging will vary depending upon the time of imaging.10 The maxillary sinus lining does not show this same pattern.
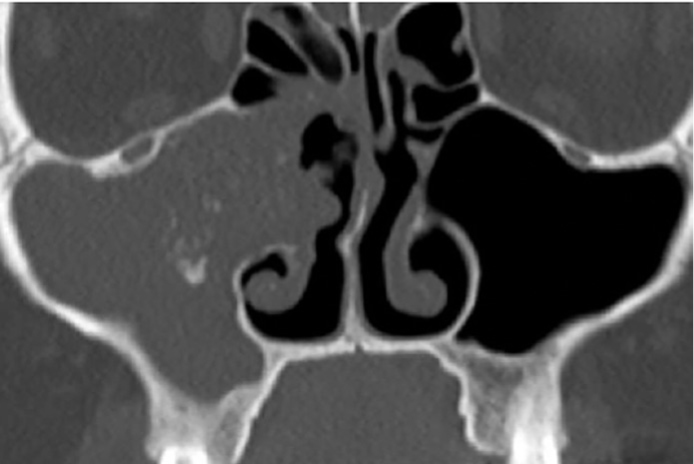
Thickening of the paranasal sinus lining has previously been identified on plain radiographs of the paranasal sinuses in 50% of the population, who have no symptoms of disease and were subsequently identified as not having rhinosinal disease.11 Thickening of the maxillary sinus lining has always been visible on plain radiographic intra-oral films and continues to be visible on modern digital systems. With the exponential use of Cone Beam Computed Tomographic (CBCT) scanning in Dentistry, maxillary sinus lining thickening is now observed more often by dentists, as is the incidence of apical periodontitis. However, there are conflicting reports as to the role of apical periodontitis and periodontal disease in contributing to maxillary sinus thickening. Some authors report increased thickness of the maxillary sinus lining in association with periodontal disease, and others reduction in maxillary sinus thickening following treatment of chronic dental infection.12,13 However, others have been unable to demonstrate any significant difference in sinus lining thickening between healthy and unhealthy dentitions.14 Maxillary sinus lining thickening has also been reported in disease-free dentitions.15 There is a risk that, as a result of the additional imaging that is now more freely available, the Dental Profession may be observing something that was always there and not necessarily related to odontogenic disease, particularly when the patient selection is not randomized from the general population (Figures 1 and 2). In the process of making observations from radiographic images and comparing such to the presence or absence of odontogenic disease, the matter of aeration of the sinus and normal muco-ciliary clearance, which contribute to sinus function, may not be considered, nor the presence or absence of patient symptoms.
Figure 1. Coronal reconstruction of a CBCT image. The thickening of the mucosa within the floor of the right maxillary sinus, and to a lesser extent the floor and medial wall of the left maxillary sinus, demonstrates inflammatory changes. Although the ostia are not shown in this image, they are obviously patent, and the antra are well aerated and drained.Figure 2. Sagittal reconstruction of CBCT showing apical periodontitis with widening of periodontal ligament space, and apical bone loss involving the third and probably also second molar. The thickening of the maxillary sinus floor is generalized and not localized to the site of disease, and therefore caution should be taken when reporting the image, and making a correlation between the apical infection and the thickening of the maxillary sinus lining.
Dome-shaped swellings of the floor of the maxillary sinus
Retention cysts of the floor of the maxillary sinus are a well-recognized feature of dental radiography. Caused by obstruction of the duct within sero-mucinous glands of the maxillary sinus, they are of no clinical significance on the basis that there are no signs of loss of adjacent bone.
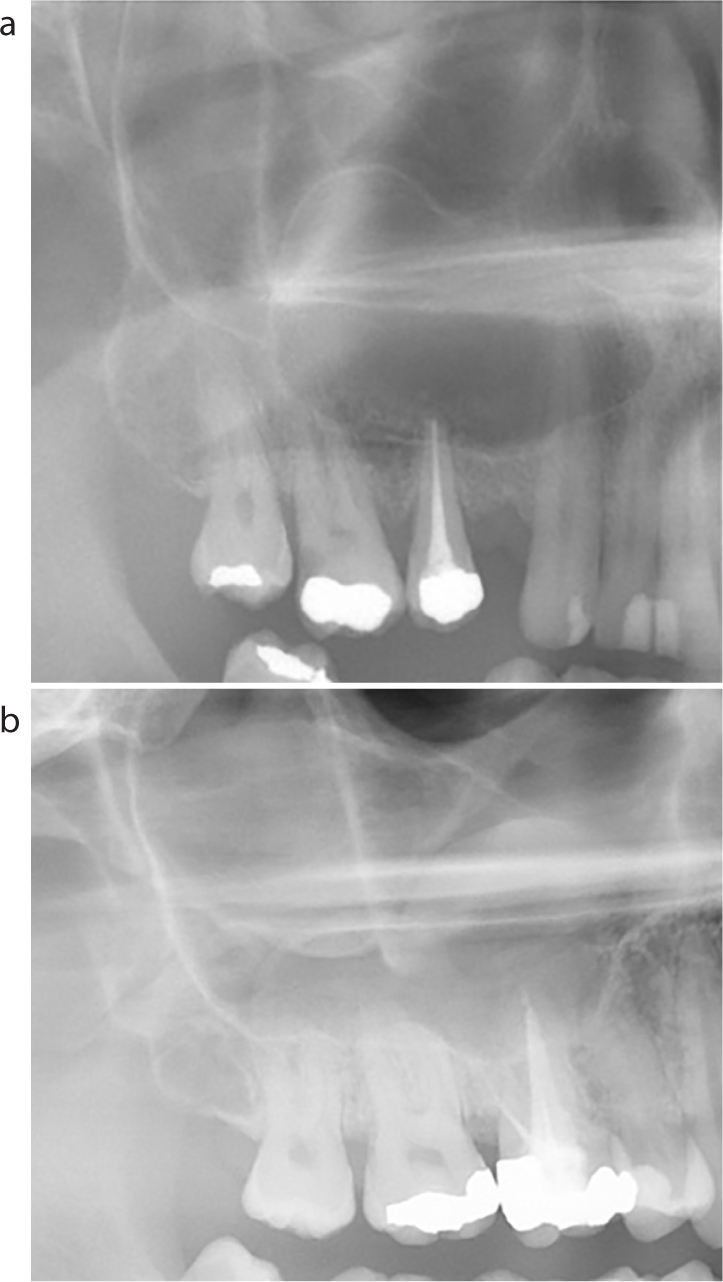
Being able to separate a retention cyst from an odontogenic lesion is a basic skill for the dental surgeon. An odontogenic cyst will have a corticated upper border as the area of bone apical to the source of infection will have expanded upwards. If the tooth that is the source of infection remains, it is usually centrally positioned within the cystic lesion. A retention cyst which has arisen within the mucosa of the sinus lining will not have any bone involvement and, as such, will not have a corticated upper border and will appear opaque as compared to the surrounding air of the sinus (Figures 3 and 4).
Figure 3.
(a, b) Composite image showing important differentiating radiographic features between retention cyst of maxillary sinus lining, and odontogenic cyst. (a) A radiolucency with a corticated margin arising from the second premolar. This is a radicular cyst. (b) A radiodensity, with no corticated upper margin extending from the floor up into the maxillary sinus. This is a retention cyst. The endodontically treated first molar is not associated with the retention cyst.Figure 4. Intra-oral radiograph of an edentulous alveolus showing a non-corticated radio-opacity extending from the maxillary sinus floor. Importantly, the adjacent bony wall is intact with no evidence of erosion. These antral cysts are a common finding and nearly always of no clinical significance.
Anatomical relation of maxillary teeth to maxillary sinus – spread of infection
The apices of maxillary teeth distal to the canine lie in close proximity to the maxillary sinus, and this can only be evaluated by radiography. There are many publications reporting the relation of roots of various teeth to the floor of the maxillary sinus, involving a broad range of imaging modalities. Despite the increased amount of information available from CBCT, for most diagnostic and therapeutic purposes peri-apical radiography of maxillary teeth should be sufficient.16,17 Periapical radiographs should be grade 1 (National Radiological Protection Board), with 3 mm of tissue visible beyond the apex.18 CBCT should not be regarded as a first line radiographic investigation for endodontic diagnosis or treatment.16
The radiographic artefact, known as the lamina dura, should be traced around each root where possible, acknowledging that, on occasions, there will be no bone between the roots of posterior maxillary teeth and the lining of the maxillary sinus.19 Changes can be described from thickening of the lamina dura, widening of the periodontal ligament space or frank loss of lamina dura. Condensing osteitis may be seen frequently in the mandible but rarely in the posterior maxilla. When a radiolucency exists, diffuse margins may reflect recent bone loss and well corticated margins reflect a chronic disease process (Figures 5–7).
Figure 5.
(a, b) Composite image with periapical radiograph showing radiolucency involving the mesio-buccal root of the UR6 tooth. On the periapical radiograph the corticated margin of the maxillary sinus floor is intact. The sagittal reconstruction of the CBCT image (note reversed image as per reconstruction) confirms the presence of an apical lesion with an intact maxillary sinus floor. The adjacent mild thickening of the maxillary sinus lining is not related to the apical infection. Septa within sinus noted.Figure 6. Periapical radiograph demonstrating apical periodontitis arising from UR5, sometimes referred to as an antral halo, with the floor of the maxillary sinus extending down and between roots of teeth. The corticated margin of the apical lesion maintains the separation of the lesion from the maxillary sinus lining. The partly imaged, dome-shaped, non-corticated radio-opacity on the floor of the maxillary sinus is most likely a retention cyst, but localized inflammatory changes, related to the apical periodontitis, cannot be excluded from this image alone.Figure 7.
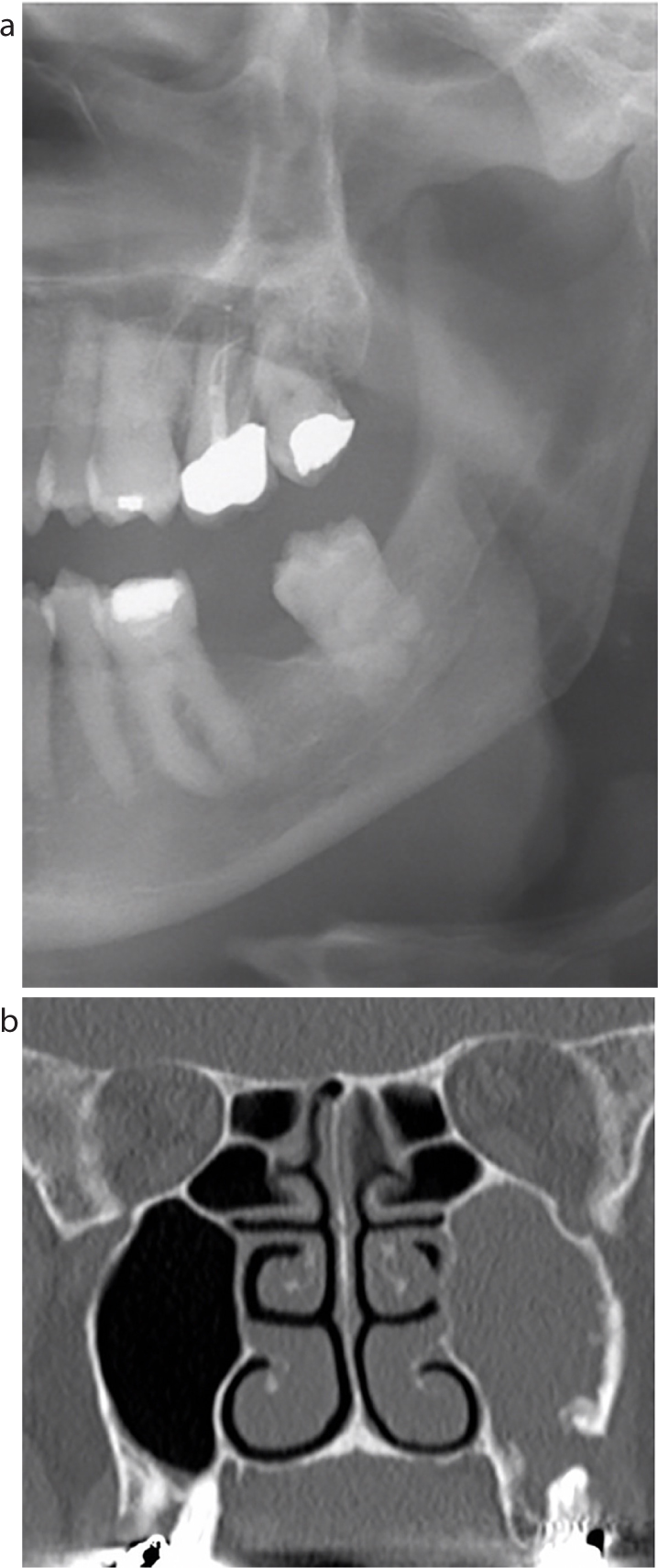
(a, b) Composite image of dental panoramic tomogram and coronal reconstruction of computed tomographic scan showing erosion of floor of maxillary sinus arising from chronic infection of UL7, with unilateral suppurative maxillary sinusitis. The corticated floor of the maxillary sinus adjacent to the UL7 is missing on the panoramic image.
On rare occasions, odontogenic infection within the maxillary sinus may behave in a fashion similar to severe acute bacterial rhinosinal disease by extension into the orbit and from there intracranially.20
Involvement of the maxillary sinus floor or mucosa in apical periodontitis should not be regarded as a contra-indication to conventional endodontic treatment. On the basis that there are no suppurative changes in the sinus, conventional root canal treatment should be undertaken and the lesion will resolve21,22 (Figure 8).
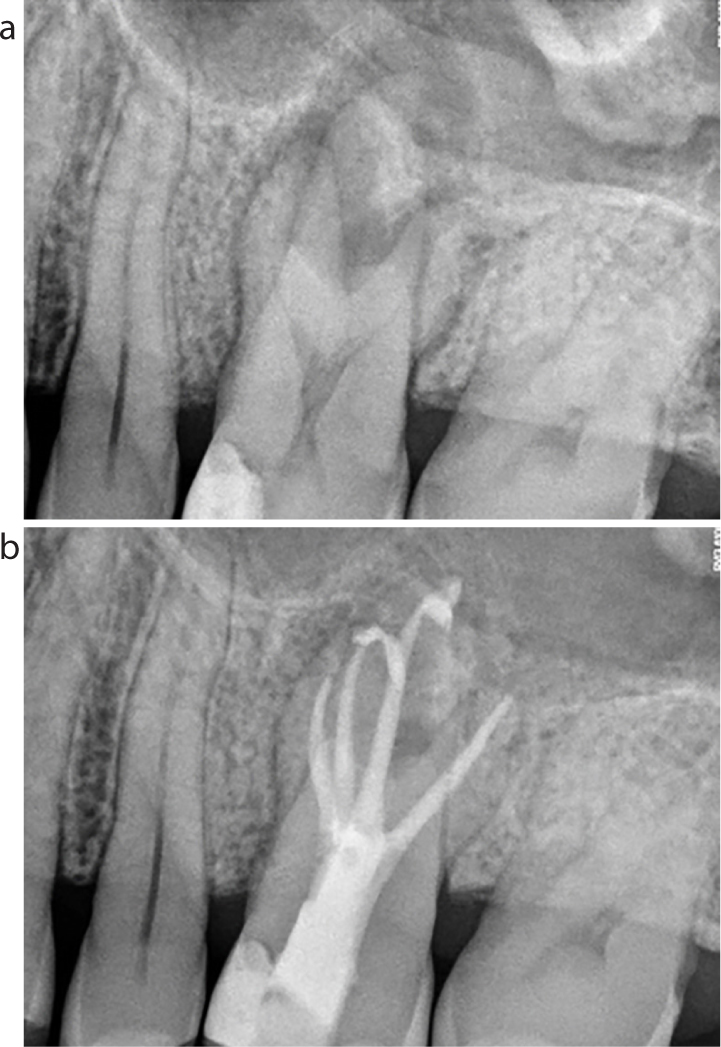
Figure 8. Composite image showing (a) taurodont upper molar with apical periodontitis extending towards maxillary sinus floor with halo of corticated bone. (b) Response to control of source of infection and bone healing 6 months later with re-establishment of normal contours of maxillary sinus floor. No maxillary sinus soft tissue changes identified.
Length control and precision endodontics
The primary mechanical and biological goals of root canal treatment are to create a shape within the canal that can be predictably cleaned and filled.23,24 Although it is accepted that the radiographic and anatomical apex are rarely coincident, shaping, cleaning and obturation within 1–2 mm of the radiographic apex is associated with improved outcomes.25,26,27 From a purely endodontic perspective, over preparation and any subsequent over fill or over extension of endodontic material is associated with a significant reduction in success of treatment.26 With respect to preventing sinus inflammation and disease, length control is equally important. Not only is the maxillary sinus in close proximity to the apices, it offers little or no resistance to endodontic extrusions. This potentially increases the risk of:
Iatrogenic damage from over-zealous instrumentation;
Iatrogenic inoculation of periapical tissues with bacteria transferred from within the pulp space system;
Separation of instruments beyond the apex;
Extrusion of debris into the periapical tissues;
Extrusion of irrigant into the periapical tissues;
Extrusion of medicaments into the periapical tissues;
Extrusion of obturation materials into the periapical tissues.
The consequences of these preventable complications to the sinus are discussed below.
Transient inflammation and post-operative pain
Routine root canal treatment is associated with apical tissue damage, but iatrogenic mechanical trauma from instrumentation and introduction of both debris and bacteria into the tissues will result in more inflammation.28,29,30,31,32 The extrusion of inter-appointment dressings, such as calcium hydroxide, will result in inflammation because of alkalinity that may cause transient pain.33,34,35 Small debris and bacteria are readily phagocytosed, may be removed by muco-ciliary function, and are of little consequence. Larger portions that cannot be cleared will cause inflammation, tissue damage and stasis with infection.
Severe tissue damage, inflammation and pain with possible tissue necrosis
The principle irrigant of choice remains sodium hypochlorite and the extrusion of this apically can result in tissue damage.36,37,38 This can result in immediate severe pain, haemorrhage and swelling. As the inflammatory reaction increases, there may be increased swelling, bruising and ultimately tissue necrosis, with or without paresthesia of oral mucosa or skin of the face, depending on the extent of extrusion.39
Inadvertent extrusion of hypochlorite into the maxillary sinus airspace will rarely cause pain, as the mucosa will protect the underlying bone. The mucosa will experience a chemical injury and muco-ciliary clearance will be reduced. Most patients will only experience an unpleasant hypochlorite taste for the following few hours until the small volume of hypochlorite is removed by residual muco-ciliary function. One case report described the need for antral access, lavage and ultimately extraction of the tooth.38 However, as the paranasal sinuses and nasal cavity combined produce 1.5–2.0 litres of sero-mucinous secretions per day, the maxillary sinus should be regarded as self-cleansing and have sufficient volume of secretions to overcome any ingress of irrigant, on the basis that the concentration is not so high as to cause a severe chemical injury to the mucosa.
Persistent chronic sinus inflammation and discomfort
Over extension of obturation materials may result in a more prolonged inflammatory response. Larger areas of GP may become encapsulated, whereas finer debris may result in a more intense inflammatory response. Either way, there may be a degree of chronic inflammation.40 Over-extended gutta percha can contribute to chronic sinusitis as a result of a foreign body producing inflammation and stasis, by reduced muco-ciliary clearance.41,42
The risk of these sinus complications and endodontic failure can be reduced with the following simple steps:
Assess the proximity of apices to the sinus before treatment to estimate the length of the roots, and shape of roots, to quantify the risk, and thoroughly consent the patient to sinus-related complications.
Always follow a crown down procedure to remove coronal bacteria and minimize interferences accessing the apical anatomy.
Use apex locators to identify the terminus of the canal more precisely, and ensure instrumentation is confined to the canal space.
Regularly cross reference the length during instrumentation with the apex locator to ensure that there is no loss of length in curved canals.
Perform careful patency filing with a size 10 file only 0.5 mm beyond the terminus of the preparation.
Employ judicious use of working length radiographs if the apex-locator reading appears inaccurate.
Follow instrumentation protocols safely to minimize the risk of instrument separation.
Irrigate carefully with sodium hypochlorite using non-end-ejecting syringes with luer-lok attachments, measured no closer than within 2 mm of the apex. Use gentle finger pressure and never allow the needle to bind. Take extra caution on wider palatal canals or where apical anatomy may have been compromised through iatrogenic damage or resorption.
When filing either with hand files or rotary instruments, clean the flutes between uses, irrigate and recapitulate regularly to prevent debris accumulating or being extruded.
Minimize extrusion of intracanal medicaments.
Use a cone-fit radiograph to ensure that the GP matches the preparation.
Consider the use of a bioactive sealer to promote more favourable healing.
Use cold condensation of gutta percha apically, reserving thermomechanical compaction for the rest of pulp space.
Avoid use of injection molded thermoplasticized gutta percha in apices of teeth intimately related to maxillary sinus.
Safe endodontic micro-surgery
When orthograde treatment has failed and retreatment is not possible via an orthograde approach, endodontic surgery may be the only option remaining to control persistent disease. Treatment of maxillary premolars and molars will often necessitate surgery in close proximity to the sinus. Key ambitions for successful surgery without sinus complications will be:
Prevention of damage to the maxillary sinus lining;
Prevention of displacement of root apices into the sinus;
Prevention of displacement of retrograde filling materials into the sinus;
Prevention of the creation of an oral-antral fistula.
Reports suggest that damage to the sinus lining may be common during traditional surgery.43,44,45,46 In itself this may have no long-term significance as it has been demonstrated that full regeneration of the sinus membrane will occur around 5 months following surgery.47,48 It may be that displacement of materials or the failure to control the contamination may be the main contributory factor in the initiation or persistence of inflammation of the sinus tissues.
Advances in the approach to endodontic surgery may have a significant impact upon the risk of adverse complications from the sinus. The use of magnification, microsurgical instruments, piezo and bioceramics provide the following advantages:49
Smaller, more precise surgical incisions;
Smaller, more precise osteotomies;
Controlled apical amputation;
Improved apical preparation using ultrasonics;
Controlled apical obtruation with biocompatible materials;
More precise primary closure.
Nonetheless, should the operator be aware of damage to the sinus lining, the placement of iodine-soaked (if the patient is not allergic to iodine) gauze will help reduce the risk of displacement of the root tip or retrograde materials into the sinus. Patient and clinicians should be reassured that it is unlikely that this will have an impact upon success of the treatment.49,50 It is important to have discussed this possible risk with the patient pre-operatively as part of the consenting process.
Aspergillosis of the maxillary sinus – what is the role of endodontic materials?
There are many case reports and case series of Aspergillosis occurring in the presence of extruded endodontic filling materials, predominantly zinc oxide based materials, and primarily gutta percha. It has been suggested that 85% of cases of Aspergillosis involving the maxillary sinus are related to over extended endodontic filling materials.51 It has also been suggested that zinc plays a crucial role in the development of Aspergillosis of the maxillary sinus as the fungus requires zinc as an essential co-enzyme to function, and with the high zinc content in endodontic filling materials the ideal environment is provided.52
Aspergillus species are a group of fungi normally present in the environment, although some warm, damp environments will contain a higher proportion of fungi. Therefore, it is inevitable that everyone will breathe aspergillus species into the naso-pharyngeal airways on a regular basis.53,54 What determines the outcome is the local environment within a person's nasal and paranasal airspaces, and also whether the host is immunocompetent or immunocompromised.55
Extruded endodontic filling materials within the maxillary sinus will act as foreign bodies, causing local inflammation and, if normal muco-ciliary clearance cannot remove the irritant, stasis will occur such that infection will arise. Aspergillosis is one such species that will take advantage of that stasis in the immunocompetent individual and produce infection. This may result in the formation of collections of material within the sinus airspace called mycetoma (fungus balls) which, if time and local conditions allow, may become calcified and can be observed as antroliths on radiographs (Figures 9 and 10). Should Aspergillosis arise within the maxillary sinus, diagnosis and treatment would be undertaken by an Ear Nose and Throat surgeon.
Figure 9. Intra-oral radiograph demonstrating antroliths in the maxillary sinus. Further clinical and radiological investigation is required to confirm cause of antroliths.Figure 10. Cropped coronal CT of the maxillary antra. Note the opacification of the right maxillary sinus extending into the ethmoid sinuses and lateral nasal wall with the presence of variable denser opacities within the right antrum. Further investigation revealed the lesion to be of chronic fungal origin, a mycetoma.
When fungal infection, Aspergillosis or Mucormycosis occurs in the immune-compromised individual, it does so often in the absence of any dental material and can demonstrate invasive behaviour similar to that seen in invasive malignancy of the maxillary sinus.56 Urgent referral is essential should any clinical signs or symptoms suggestive of rhinosinal malignancy present to the Dental Team (Table 1).
Symptoms
Clinical Signs
Recurrent recent onset unilateral epistaxis
Unexplained buccal expansion of maxillary alveolus
Recent onset unexplained orofacial pain
Recent onset trismus
Diplopia
Loss of corticated outline of maxillary sinus floor or walls (radiographic sign)
Loss of sensation in maxillary division of trigeminal nerve
Mobility of teeth in absence of periodontal or periapical disease
Unilateral presence of soft tissue in anterior nares
Non-healing extraction site
Spontaneous formation of oro-antral fistula
Dull tone to percussion of multiple posterior maxillary teeth
Aspergillosis is relatively rare in developed societies with advanced healthcare systems. Invasive Aspergillosis of the paranasal sinuses is an increasing problem within immunocompromised patients, particularly with haematological malignancy.57 However, it is invasive pulmonary Aspergillosis in the immunocompromised patient that contributes most to morbidity and mortality.58
Dispelling the concept that zinc materials actively contribute to Aspergillosis of the maxillary sinus is the finding that there is no evidence of any influence on growth between individual Aspergillus species with differing concentrations of zinc cement.59 Therefore, rather than zinc-based endodontic materials contributing to Aspergillosis infection through a chemical route, it is more probably mediated through the route of a local irritant causing inflammation and stasis. This concept is further supported by the fact that Aspergillosis infection has been reported in the maxillary sinus when dental implants, which are zinc free, have perforated the sinus lining.60
Summary
In this paper the mechanisms of inflammatory changes within the maxillary sinus lining and how these present have been discussed. The role of acute and chronic apical periodontitis in maxillary sinus disease of endodontic origin has also been discussed. When using CBCT, caution has been urged in assuming that any thickening of the maxillary sinus lining in the presence of dental infection is dentally related: such thickening is also seen in the absence of dental infection, and should be regarded as a normal variation in the immunological response of the sinus lining to irritants.
The role of extruded endodontic materials in the maxillary sinus acting as chemical irritants, causing inflammation and stasis, and contributing to either bacterial or fungal infection, has been outlined. In the final paper in this series, the role of dental implantology in relation to maxillary sinus health and function will be discussed.