Ramezanian M, Mahmoud-Hashemi H, Vaezi T, Beshkar M, Hasheminasab M. The pattern of maxillofacial fractures: a study of 302 patients and a discussion of fracture classification. J Craniomaxillofac Res. 2015; 1:95-102
Maloney PL, Lincoln RE, Coyne CP. A protocol for the management of compound mandibular fractures based on the time from injury to treatment. J Oral Maxillofac Surg. 2001; 59:879-884
Willis DH, Tong DC, Thomson WM, Love RM. Maxillofacial trauma and the GDP–specialty recognition and patterns of referral. NZ Dent J. 2010; 106:97-102
Marker P, Nielsen A, Bastian HL. Fractures of the mandibular condyle. Part 1: patterns of distribution of types and causes of fractures in 348 patients. Br J Oral Maxillofac Surg. 2000; 38:417-421
Kuijpers SC, van Roessel EW, Van Merkesteyn JR. Unusual case of a conservatively treated pathological fracture after sequestrectomy in a patient with long-term oral bisphosphonate use. J Cranio-Maxillofac Surg. 2011; 39:69-72
Marunick MT, Garcia-Gazaui S, Hildebrand JM. Mandibular pathological fracture during treatment with a dynamic mouth opening device: a clinical report. J Prosthet Dent. 2016; 116:488-491
Pires WR, Bonardi JP, Faverani LP, Momesso GA, Muñoz XM, Silva AF, Panzarini SR, Bassi AP, Ponzoni D. Late mandibular fracture occurring in the postoperative period after third molar removal: systematic review and analysis of 124 cases. Int J Oral Maxillofac Surg. 2016; 46:46-53
Wagner KW, Otten JE, Schoen R, Schmelzeisen R. Pathological mandibular fractures following third molar removal. Int J Oral Maxillofac Surg. 2005; 34:722-726
Marker P, Nielsen A, Bastian HL. Fractures of the mandibular condyle. Part 1: patterns of distribution of types and causes of fractures in 348 patients. Br J Oral Maxillofac Surg. 2000; 38:417-421
Ogundare BO, Bonnick A, Bayley N. Pattern of mandibular fractures in an urban major trauma center. J Oral Maxillofac Surg. 2003; 61:713-718
Gray RJ, Davies SJ. Emergency treatment of acute temporomandibular disorders: Part 1. Dent Update. 1997; 24:170-173
Whaites E., 2nd edn. London: Elsevier Ltd; 2009
Didcot: National Radiological Protection Board; 2001
Leeds: Public Health England: Radiation Protection Services; 2013
Tay AB, Lai JB, Lye KW Inferior alveolar nerve injury in trauma-induced mandible fractures. J Oral Maxillofac Surg. 2015; 73:1328-1340
Scott RA, Teo N, Perry M. Displacement of mandibular fractures: is there a correlation with sensory loss and recovery?. Int J Oral Maxillofac Surg. 2014; 43:555-558
Omeje KU, Adebola AR, Efunkoya AA Prospective study of the quality of life after treatment of mandibular fractures. Br J Oral Maxillofac Surg. 2015; 53:342-346
Béogo R, Bouletreau P, Konsem T, Traoré I, Coulibaly AT, Ouédraogo D. Wire internal fixation: an obsolete, yet valuable method for surgical management of facial fractures. Pan Afr Med J. 2014; 17
Koshy JC, Feldman EM, Chike-Obi CJ, Bullocks JM. Pearls of mandibular trauma management. Semin Plast Surg. 2010; 24:357-374
Goth S, Sawatari Y, Peleg M. Management of paediatric mandible fractures. J Craniofac Surg. 2012; 23:47-56
Andersson L, Andreasen JO, Day P International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dent Traumatol. 2012; 28:88-96
The Role of the General Dental Practitioner in the Management of Mandibular Fractures Gurdeep K Hans Surina Bhola Zahra Ahmad Dental Update 2024 47:5, 707-709.
Authors
Gurdeep KHans
BDS, MFDS RCPSG
Dental Core Trainee, Oral and Maxillofacial Surgery, Wexham Park Hospital, Wexham Street, Slough, SL2 4HL
Mandibular fractures are a common presentation to emergency departments in hospital. Although the majority of mandibular fractures are treated in secondary care, General Dental Practitioners (GDPs) should have the basic knowledge to be able to support fracture patients in practice, whether that is in an emergency situation, managing associated sequelae, or through post-operative recovery.
CPD/Clinical Relevance: This article highlights the importance of management of trauma in a primary care setting by GDPs, including pre- and post-operative care of mandibular fractures.
Article
Gurdeep K Hans
Fractures of the mandible are a common presentation in secondary care, usually to Accident and Emergency departments in hospital, with the most common cause being trauma.1
For acute severe trauma, most patients may present at hospital. However, in mild to moderate injuries, especially when the trauma to the dentition or the soft tissues may be the only presenting signs/symptoms, the patient may present to the General Dental Practitioner (GDP) in primary care.
It is imperative that GDPs have the basic knowledge to be able to manage acute injuries involving the mandible. Important aspects of patient care include:
Recognition of a patient who needs to be referred urgently;2
Identifying what can be treated acutely in dental practice;
In addition, after patients have been discharged from secondary care, for example, after an invasive surgical procedure, it is the responsibility of the GDP to monitor and manage patients through the remainder of their care, referring patients back to specialist departments should the need arise. Dentists in primary care must have at least a basic understanding of orofacial trauma, as this may also reduce the demand on already over-subscribed services.
Aetiology and sites of mandibular fractures
Common aetiologies of mandibular fractures include:
Assault – this may involve individuals under the influence of substances such as drugs and excessive alcohol;
Road traffic accidents – commonly involving drivers and cyclists;4
Abuse – the practitioner may have a safeguarding responsibility to the patient for which appropriate safeguarding protocols must be adhered to;
Pathological fracture – examples of this could be patients who have thin cortical bone in the mandible, such as edentulous individuals, or those post treatment of bony sequestrations, such as patients on long-term bisphosphonates.5 Long-standing head and neck cancer patients may also be more likely to suffer pathological fractures after radiotherapy and studies have demonstrated that even less invasive dental procedures in these patients may lead to fracture.6
Contact sports injuries;
Occupational injuries;
Falls;
Iatrogenic injury – although rare, this may occur due to impacted third molar surgery for example.7,8
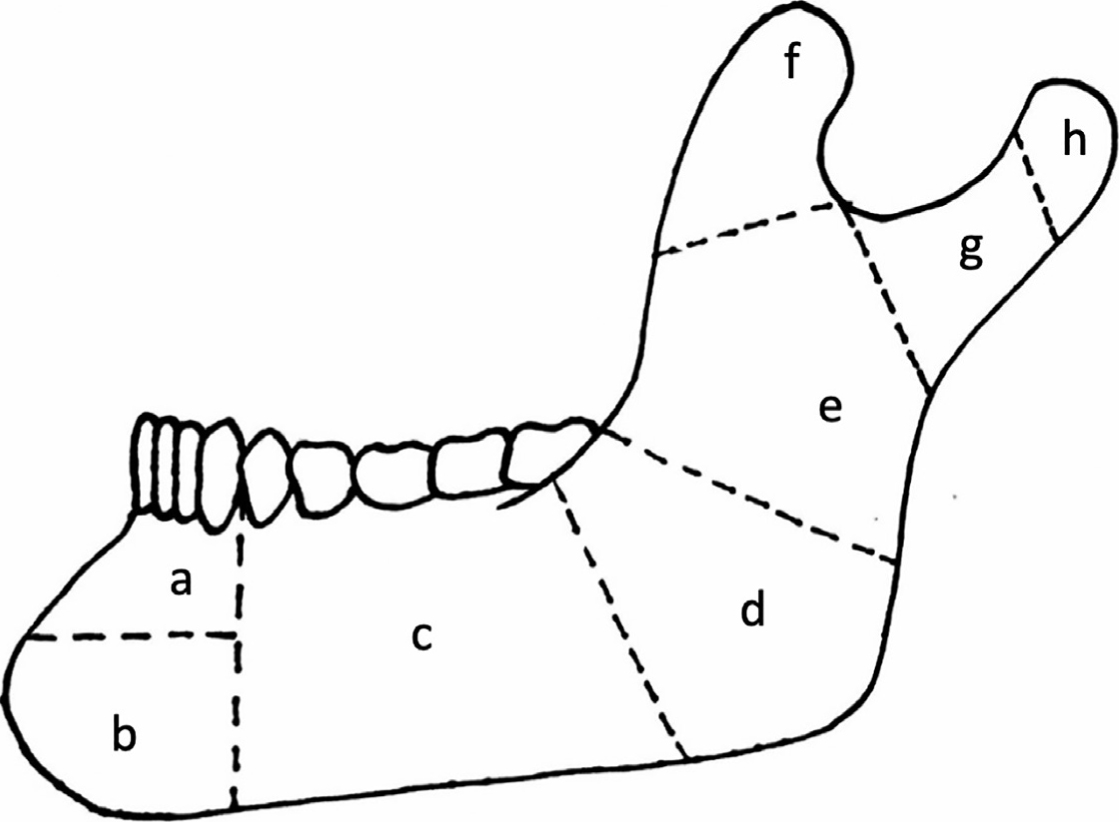
The most common sites of fracture are the angle, the condyle, and the parasymphyseal region of the mandible. However, evidence has shown that these figures vary internationally; therefore, no specific percentage can be assigned.9Figure 1 represents the sites where a fracture in the mandible may occur.10
Figure 1. Diagrammatic representation of fracture locations in the mandible: (a) dento-alveolar (b) symphysis (c) body (d) angle (e) ramus (f) coronoid (g) subcondylar (h) condylar.
What can you do as a GDP?
If presented with a patient who has sustained facial trauma and a suspected mandible fracture, as with any patient, a thorough history is imperative. The first priority involves checking that the patient does not have acute life or limb threatening conditions, for which immediate emergency treatment may be required. The ABCDE (Airway, Breathing, Circulation, Disability, Exposure) system can be used to assess this but, for a GDP, even the principles of Basic Life Support should be implemented. Should there be suspected head injury, the emergency services must be involved urgently, but it is unlikely that trauma this severe will present at the primary care setting.
The focus of this article will be on patients who have sustained mandibular fractures, and Table 1 highlights the types of questions GDPs should be asking to obtain a comprehensive history of the incident. These questions are imperative in ascertaining differential diagnoses and therefore guiding the future management and appropriate referral pathway for the patient. Clear, concise and contemporaneous record-keeping should be ensured at all times.
Question to Ask
Relevance
Time of injury
A delay in treatment could affect outcomes.
History of injury
This will enable a diagnosis to be made and allow a better understanding of treatment options available.
Loss of consciousness or vomiting, and for how long?
These may indicate a head injury, in which case the patient will need to go to hospital immediately for further investigation.
Was the patient under the influence of any substances when the injury occurred, eg alcohol or drugs
Intoxication may affect consent, as well as ease of treatment, and possible drug interactions.
Method of injury, and how many times if hit
Any objects used in assault could be embedded in soft tissues and pose an infection risk, so these may need to be explored, for example, chipped incisor fragments are often found in the lower lip.
Direction of injury
The direction of assault could give a clue as to the location of fracture, or possible other injuries.
Was the assault witnessed and by whom?
This may help to ascertain the complete history of the injury.
Are the police involved?
If the GDP is required to give a witness statement, this may be relevant.
Feeling of numbness or tingling in the lower lip, chin, or face
This may indicate nerve damage, or temporary paraesthesia of the trigeminal nerve or its branches.
Altered or loss of function of the mandible
Mandibular fracture may cause a change in occlusion, especially if displaced. Clinicians should assess movement, occlusion, speech, and swallowing.
Medical history
A thorough MH is required with allergy history. For example, diabetics may have poor healing, or those on intravenous infusions (bisphosphonates) may require referral.
Any missing or mobile teeth
This is something which may indicate fracture of the dento-alveolar segment, and may need acute management, eg splinting before referral. Remember with avulsed teeth, the extra-oral dry time (ideally <60 mins) affects the success rate of treatment (IADT Guidelines).
Pain history
Clinicians should gather a comprehensive pain history, including site, onset, duration, character, radiation, severity, exacerbating and relieving factors, and associated factors.
Following a comprehensive history, a clinical examination should be conducted, starting extra-orally and then intra-orally. Before emphasis is placed on the mandible, the GDP should have a basic understanding of general orofacial trauma, as most injuries are not isolated. Clinicians should check the eyes and the upper face. If there are any eye signs, eg diplopia, these will usually be referred to the local Ophthalmology and/or Oral and Maxillofacial (OMFS) department, but this is beyond the scope of this paper.
After mandibular trauma, GDPs may notice signs of fracture extra-orally and intra-orally
Extra-oral signs of fracture on examination
Limited mouth opening
Normal mouth opening is usually 38 mm for females, and 45 mm for males11 so, if this is markedly reduced, it may indicate either fracture, or soft tissue swelling causing marked trismus/pain.
Deviation on opening
A unilateral condylar fracture, due to the anatomy of the temporomandibular joint, may present as deviation on opening. If this is normal for the patient, the GDP may have this noted from previous examinations.
Rule out dislocation
Patients who have a history of temporomandibular joint dysfunction, or previous dislocation, may be aware of their condition. Dislocation without reduction usually presents as an inability either to open or close the mouth, presenting as a ‘closed’ or ‘open’ lock. This requires urgent relocation, as the muscles may spasm, after which the patient may require sedation to reduce the temporomandibular joint back into the fossa. This must be differentiated from fracture, which can also be deduced from radiographic examination of the position of the condyles in the glenoid fossa, but this is something which will usually be diagnosed in a hospital setting. If comfortable, GDPs can attempt relocation in surgery, but if there is any doubt, urgent referral should be made to the local OMFS department.
Numbness/paraesthesia
Mandibular fractures between the mental foramen and mandibular foramen may involve the inferior alveolar nerve and this may be damaged upon trauma, resulting in paraesthesia to the lip, chin, gums and teeth on the damaged side, either transient or permanent. Damage to the nerve may be caused by indirect injury to the nerve bundle, compression vs soft tissue oedema, or direct injury of the nerve if involved in the line of the fracture.
Intra-oral signs of fracture on examination
Dental trauma
This can include avulsion, luxation, intrusion or extrusion injuries, as well as concussion or subluxation. GDPs can refer to the International Association for Dental Traumatology (IADT) Guidelines for how to manage trauma acutely. The patient should always be warned about darkening/discoloration of teeth or loss of vitality and associated long-term prognosis. Long-term clinical and radiographic follow-up will be required for such patients.
Tears in the gingivae with bleeding
This may indicate mandible fracture and/or dento-alveolar fractures, which may need to be splinted for a period of weeks–months, depending on the type of fracture that has occurred.
Occlusion
Step deformities or open bites could indicate fracture. Clinicians should always enquire if the patient's ‘bite feels different’. However, this should be supplemented with clinical examination, as sometimes soft tissue swelling can cause the patient to posture, leading to misdiagnosis of fracture.
Haematomas
Bruising in the mouth could indicate underlying soft and/or hard tissue injuries. Following clinical examination, any investigations required should be done. This may include sensibility testing of teeth that have sustained trauma, and associated radiographs, eg long cone periapicals. For the suspected fracture itself however, the most appropriate investigations are radiographs. It is important to have more than one image, at differing angles, as a single view may mask fractures. However, this is something which would usually be done in secondary care, for example, a posterior-anterior view, with an orthopantomogram (OPT). For the GDP, an OPT is ideal, as it gives a general image of any fractures or teeth of poor prognosis. Again, for GDPs, these plain films must be justified, while following IRMER and IRR guidelines.12,13,14,15 The clinician may feel more comfortable referring the patient to secondary care for radiographic investigation, depending on the severity of the symptoms.
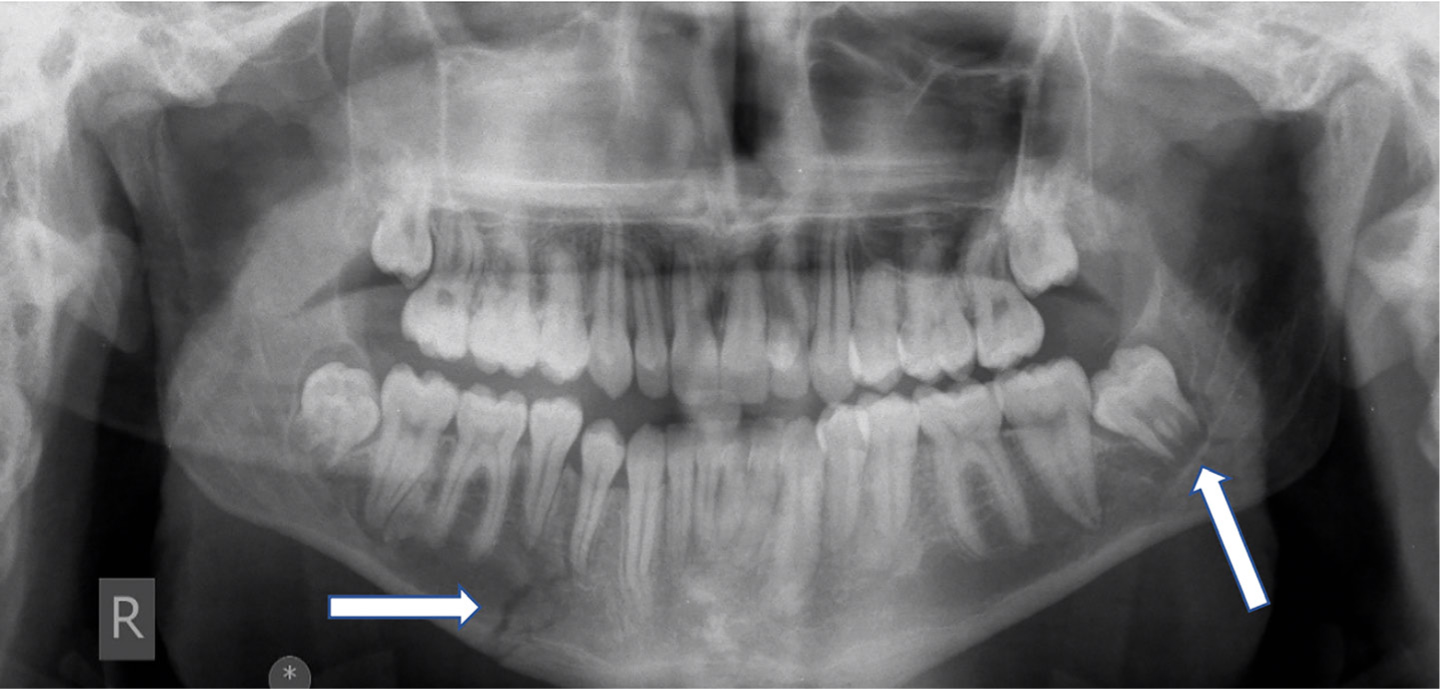
Figures 2 is an OPT taken at the time of injury, showing a left angle and right symphyseal fracture.
Figure 2. Left angle and right symphysis fracture before surgery.
When to refer?
When referring to A&E or a local OMFS department in hospital, it is helpful for the clinicians in secondary care to send the patient with a letter, with relevant good quality radiographs, and clinical investigations and findings. If unsure of the diagnosis, clinicians can contact the local OMFS department for advice. Generally, the following scenarios would warrant an OMFS referral:
Any sign of head injury, loss of consciousness or vomiting – these patients should be sent urgently to A&E;
Any evidence of fracture by radiographic or clinical examination;
Severe pain;
Nerve paraesthesia or altered sensation;
Any ‘eye signs’ – these patients will need to be seen in hospital as they may have other associated injuries. Eye signs can include diplopia, proptosis, and pain/restriction of eye movements;
Trismus and limited mouth opening.
Once referred, patients with mandibular fractures may have the following treatment in hospital:
Reassurance and analgesia;
Inter-maxillary fixation (IMF) – this involves splinting the patient's teeth into occlusion using brackets, buttons, or wires and elastics;
Open reduction and internal fixation (ORIF) – this is an invasive surgical procedure which involves using plates and screws to approximate and strengthen the fractured segments together, and may also require removal of teeth involved in the fracture line, eg lower third molars for angle fractures.
Post-operative care
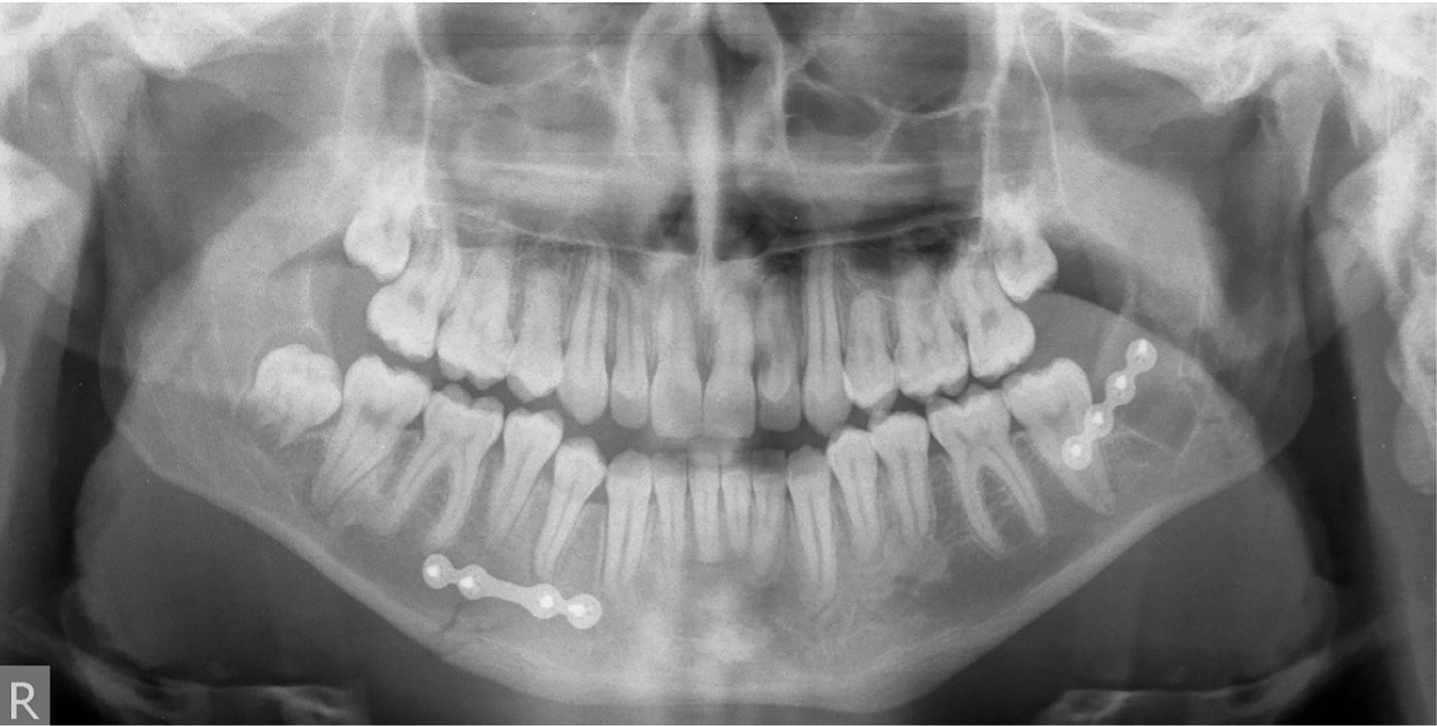
Following treatment of mandible fractures in hospital, the patient will be seen back in secondary care for review appointments but, ultimately, it will be a combination of the GDP and General Practitioner (GP) who follow up the patient long term. Therefore, it is imperative that the GDP understands what treatment, if any, has been carried out and what altered needs the patient now has. Post-operative imaging would usually be taken in secondary care post-surgery to assess the approximation of the fracture site, and the position of any plates and screws. The OPT in Figure 3 demonstrates the same fracture in Figure 2 after surgery. The GDP will also need to be vigilant of signs that may indicate new infection, mal-union, and non-or delayed-healing and should appropriately re-refer back to secondary care, as these may manifest long after the patient has been discharged from the OMFS department.
Figure 3. The same fracture in Figure 2 after surgery with open reduction and internal fixation (ORIF) of the fractures.
Many patients may suffer altered sensation or paraesthesia due to bruising and soft tissue injury. Persistent numbness (>12 months) may occur if the larger nerves, such as the inferior alveolar nerve (IAN), have been incorporated in the fracture line.16,17Figure 4 shows a displaced left angle fracture which resulted in prolonged IAN damage, and lip and chin numbness.
Figure 4. Displaced left angle fracture associated with vertical fracture of LL7. This patient had prolonged lip and chin numbness after trauma.
The quality of life of a patient after surgical treatment of a fractured mandible has been shown to decline straight after treatment, no matter what type of fixation was carried out. Nevertheless, patients' main complaints may include limitation of opening, difficulty eating, chewing and swallowing in the early post-operative period.18
When patients return to their GDP, they may have limited mouth opening, and short-term temporomandibular joint dysfunction, which may require conservative management and advice, eg soft diet. All patients who have had ORIF need a soft diet initially to reduce forces on the healing mandible. Patients will also need thorough oral hygiene advice, advised adjuncts such as a high fluoride toothpaste, chlorhexidine mouthwash, and diet advice.19
Patients need to be instructed regarding the risk of malnutrition during the healing phase, due to reduced mouth opening/pain, which may need caloric supplementation. The GDP can liaise with the patient's GP for this.
Typically, sutures used in the mouth during surgery are resorbable, taking between 10–14 days to dissolve. Sometimes the patient may need to see the dentist between appointments with the OMFS department, for example if there is a contaminated or infected suture which needs trimming or removal. Early loss of a suture may also cause bleeding, or a soft tissue defect, which could be managed locally by the GDP, either by re-suturing or, if appropriate, liaison with the local OMFS team.
Should the patient have plates in situ it is important to know as, occasionally, these can get infected and can cause patients distress and pain. This may present as pain and swelling around the area, pus exudate and sometimes even an exposed plate or screws in the mouth. This is a clear complication of surgery that can be picked up in primary care and will warrant referral to the OMFS unit for possible removal, with antibiotic cover. If the patient has had teeth removed in the process, then dry socket is also a possibility, as well as dental pathology from non-vital traumatized teeth.20
Paediatric fractures
Even though paediatric facial trauma accounts for <15% of all maxillofacial injuries, the clinician should still comprehensively assess the child patient, to obtain a thorough history. Additional issues with children may include safeguarding, long-term complications affecting craniofacial development, occlusion, the developing dentition and symmetry. This may require multidisciplinary care, and liaison with the local paediatric team, orthodontist and OMFS department.21
The GDP must be fully aware of dental traumatology guidelines as set by the International Association for Dental Traumatology (IADT) in terms of short-, medium- and long-term management of any teeth which have undergone injury. The GDP must ascertain if the child is up-to-date with his or her vaccinations, particularly tetanus.22
Regular review of the developing dentition, good radiographs and oral hygiene and prevention advice is the responsibility of the GDP to prevent any future manageable consequences of trauma, as with adult patients.
Conclusion
Mandibular fractures can be an unfamiliar emergency seen by GDPs. Most GDPs may not feel they have the confidence to deal with patients before, during and after surgical or non-surgical procedures. This article demonstrates that, if certain steps are followed, there is no reason why GDPs cannot be well integrated into patients' care, taking a multidisciplinary approach to patient treatment. This may help to reduce the pressure on emergency services in secondary care. Nevertheless, the GDP should be well aware that, if patients require specialist input, they should be referred without delay.